
The Safety of Topical and Intravenous Tranexamic Acid in Endoscopic Sinus Surgery



Abstract
:1. Introduction
2. Materials and Methods
2.1. Scoping Review
2.1.1. Databases Used
2.1.2. Eligibility Screening Criteria
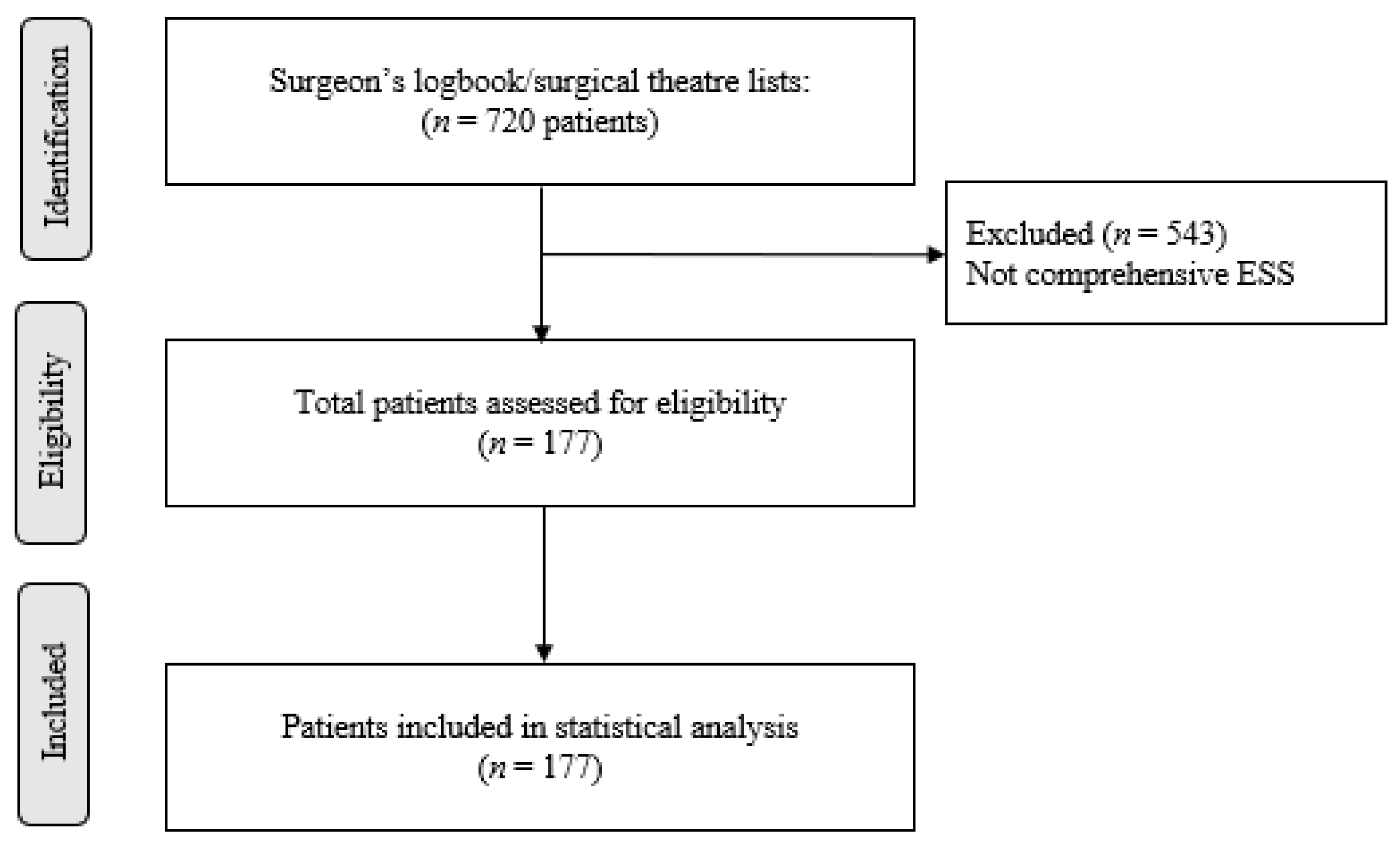
2.2. Retrospective Clinical Study
2.3. Statistical Analysis
3. Results
3.1. Scoping Review
3.1.1. Cytotoxicity
3.1.2. Wound Healing Effects
3.1.3. Anti-Inflammatory Effects
3.2. Retrospective Clinical Study
3.2.1. Patient Characteristics
3.2.2. Surgical Characteristics
3.2.3. Use of TXA
3.2.4. Post-Operative Course
3.2.5. Safety
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Georgalas, C.; Obholzer, R.; Martinez-Devesa, P.; Sandhu, G. Day-case septoplasty and unexpected re-admissions at a dedicated day-case unit: A 4-year audit. Ann. R. Coll. Surg. Engl. 2006, 88, 202–206. [Google Scholar] [CrossRef] [PubMed]
- Duignan, M.; Lao, C.; Lawrenson, R.; Wood, A.J. A policy of day-case sinonasal surgery is safe, well tolerated and cost-effective. J. Laryngol. Otol. 2021, 135, 341–343. [Google Scholar] [CrossRef] [PubMed]
- Alsaleh, S.; Manji, J.; Javer, A. Optimization of the Surgical Field in Endoscopic Sinus Surgery: An Evidence-Based Approach. Curr. Allergy Asthma Rep. 2019, 19, 8. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, A.V.; Roldan, A.F.; Laguna, D.O. Bleeding control in endoscopic sinus surgery: A systematic review of the literature. Rhinology 2013, 51, 298–305. [Google Scholar] [CrossRef]
- Valentine, R.; Wormald, P.-J. Nasal dressings after endoscopic sinus surgery: What and why? Curr. Opin. Otolaryngol. Head Neck Surg. 2010, 18, 44–48. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Kim, S.; Kang, H.; Jin, H.J.; Hwang, S.H. Efficacy of tranexamic acid on operative bleeding in endoscopic sinus surgery: A meta-analysis and systematic review. Laryngoscope 2019, 129, 800–807. [Google Scholar] [CrossRef]
- Athanasiadis, T.; Beule, A.G.; Wormald, P.J. Effects of topical antifibrinolytics in endoscopic sinus surgery: A pilot randomized controlled trial. Am. J. Rhinol. 2007, 21, 737–742. [Google Scholar] [CrossRef]
- Baradaranfar, M.H.; Dadgarnia, M.H.; Mahmoudi, H.; Behniafard, N.; Atighechi, S.; Zand, V.; Baradaranfar, A.; Vaziribozorg, S. The Effect of Topical Tranexamic Acid on Bleeding Reduction during Functional Endoscopic Sinus Surgery. Iran. J. Otorhinolaryngol. 2017, 29, 69–74. [Google Scholar]
- Jahanshahi, J.; Hashemian, F.; Pazira, S.; Bakhshaei, M.H.; Farahani, F.; Abasi, R.; Poorolajal, J. Effect of topical tranexamic acid on bleeding and quality of surgical field during functional endoscopic sinus surgery in patients with chronic rhinosinusitis: A triple blind randomized clinical trial. PLoS ONE 2014, 9, e104477. [Google Scholar] [CrossRef]
- Shehata, A.; Ibrahim, M.; Abd-El-Fattah, M. Topical tranexamic acid versus hot saline for field quality during endoscopic sinus surgery. Egypt. J. Otolaryngol. 2014, 30, 327–331. [Google Scholar] [CrossRef] [Green Version]
- Standring, S.; Anand, N.; Birch, R.; Collins, P.; Crossman, A.R.; Gleeson, M.; Jawaheer, G.; Smith, A.L.; Spratt, J.D.; Stringer, M.D.; et al. Gray’s Anatomy: The Anatomical Basis of Clinical Practic, 41st ed.; Elsevier Limited: New York, NY, USA, 2016; p. 2016. [Google Scholar]
- Gayet-Ageron, A.; Prieto-Merino, D.; Ker, K.; Shakur, H.; Ageron, F.-X.; Roberts, I.; Kayani, A.; Geer, A.; Ndungu, B.; Fawole, B.; et al. Effect of treatment delay on the effectiveness and safety of antifibrinolytics in acute severe haemorrhage: A meta-analysis of individual patient-level data from 40,138 bleeding patients. Lancet 2018, 391, 125–132. [Google Scholar] [CrossRef]
- Peedicayil, A.; Weaver, A.; Li, X.; Carey, E.; Cliby, W.; Mariani, A. Incidence and timing of venous thromboembolism after surgery for gynecological cancer. Gynecol. Oncol. 2011, 121, 64–69. [Google Scholar] [CrossRef] [PubMed]
- Bjørnarå, B.; Gudmundsen, T.; Dahl, O. Frequency and timing of clinical venous thromboembolism after major joint surgery. J. Bone Jt. Surgery. Br. Vol. 2006, 88, 386–391. [Google Scholar] [CrossRef] [Green Version]
- Expósito-Ruiz, M.; Arcelus, J.I.; Caprini, J.A.; López-Espada, C.; Bura-Riviere, A.; Amado, C.; Loring, M.; Mastroiacovo, D.; Monrea, M.; RIETE Investigators. Timing and impact of venous thromboembolism after non-cancer surgery. J. Vasc. Surg. 2020, 9, 859–867.e2. [Google Scholar] [PubMed]
- Fokkens, W.J.; Lund, V.J.; Hopkins, C.; Hellings, P.W.; Kern, R.; Reitsma, S.; Bernal-Sprekelsen, M.; Mullol, J.; Alobid, I.; Anselmo-Lima, W.T.; et al. European position paper on rhinosinusitis and nasal polyps. Rhinology 2020, 58 (Suppl. S29), 1–464. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- Dos Reis, L.G.; Ghadiri, M.; Young, P.; Traini, D. Nasal Powder Formulation of Tranexamic Acid and Hyaluronic Acid for the Treatment of Epistaxis. Pharm. Res. 2020, 37, 186. [Google Scholar] [CrossRef]
- Gholizadeh, H.; Messerotti, E.; Pozzoli, M.; Cheng, S.; Traini, D.; Young, P.; Kourmatzis, A.; Caramella, C.; Ong, H.X. Application of a Thermosensitive In Situ Gel of Chitosan-Based Nasal Spray Loaded with Tranexamic Acid for Localised Treatment of Nasal Wounds. AAPS PharmSciTech 2019, 20, 299. [Google Scholar] [CrossRef]
- Haghi, M.; van den Oetelaar, W.; Moir, L.M.; Zhu, B.; Phillips, G.; Crapper, J.; Young, P.M.; Traini, D. Inhalable tranexamic acid for haemoptysis treatment. Eur. J Pharm. Biopharm. 2015, 93, 311–319. [Google Scholar] [CrossRef]
- Wyrwa, R.; Otto, K.; Voigt, S.; Enkelmann, A.; Schnabelrauch, M.; Neubert, T.; Schneider, G. Electrospun mucosal wound dressings containing styptics for bleeding control. Mater. Sci. Eng. C 2018, 93, 419–428. [Google Scholar] [CrossRef]
- Baylis, J.R.; Finkelstein-Kulka, A.; Macias-Valle, L.; Manji, J.; Lee, M.; Levchenko, E.; Okpaleke, C.; Al-Salihi, S.; Javer, A.; Kastrup, C.J. Rapid hemostasis in a sheep model using particles that propel thrombin and tranexamic acid. Laryngoscope 2017, 127, 787–793. [Google Scholar] [CrossRef] [PubMed]
- Yee, B.E.; Wissler, R.N.; Zanghi, C.N.; Feng, C.; Eaton, M.P. The effective concentration of tranexamic acid for inhibition of fibrinolysis in neonatal plasma in vitro. Anesth. Analg. 2013, 117, 767–772. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, D.J.; Blackstock, K.J.; Epstein, K.; Brainard, B.M. Evaluation of tranexamic acid and ε-aminocaproic acid concentrations required to inhibit fibrinolysis in plasma of dogs and humans. Am. J. Vet. Res. 2014, 75, 731–738. [Google Scholar] [CrossRef] [PubMed]
- Eikebrokk, T.A.; Vassmyr, B.S.; Ausen, K.; Gravastrand, C.; Spigset, O.; Pukstad, B. Cytotoxicity and effect on wound re-epithelialization after topical administration of tranexamic acid. BJS Open 2019, 3, 840–851. [Google Scholar] [CrossRef]
- Yuan, C.; Wang, X.-M.; Yang, L.-J.; Wu, P.-L. Tranexamic acid accelerates skin barrier recovery and upregulates occludin in damaged skin. Int. J. Dermatol. 2014, 53, 959–965. [Google Scholar] [CrossRef]
- Çevik, H.B.; Eceviz, E.; Kaya, Ö.T.Ç.; Ercan, F.; Çeçen, G.S. The effect of topical and systemic tranexamic acid on fracture healing in rats. Acta Orthop. Traumatol. Turc. 2020, 54, 207. [Google Scholar] [CrossRef]
- Diebel, M.E.; Diebel, L.N.; Liberati, D.M. Tranexamic acid and the gut barrier: Protection by inhibition of trypsin uptake and activation of downstream intestinal proteases. Am. J. Surg. 2017, 213, 489–493. [Google Scholar] [CrossRef]
- Li, Y.; Xie, H.; Deng, Z.; Wang, B.; Tang, Y.; Zhao, Z.; Yuan, X.; Zuo, Z.; Xu, S.; Zhang, Y.; et al. Tranexamic acid ameliorates rosacea symptoms through regulating immune response and angiogenesis. Int. Immunopharmacol. 2019, 67, 326–334. [Google Scholar] [CrossRef]
- Sun, Q.; Li, J.; Chen, J.; Zheng, C.; Liu, C.; Jia, Y. Comparison of intravenous, topical or combined routes of tranexamic acid administration in patients undergoing total knee and hip arthroplasty: A meta-analysis of randomised controlled trials. BMJ Open 2019, 9, e024350. [Google Scholar] [CrossRef]
- Wang, Z.; Shen, X. The efficacy of combined intra-articular and intravenous tranexamic acid for blood loss in primary total knee arthroplasty: A meta-analysis. Medicine 2017, 96, e8123. [Google Scholar] [CrossRef]
- Zhang, M.P.; Li, M.J.; Wang, M.X. Combined versus single application of tranexamic acid in total knee and hip arthroplasty: A meta-analysis of randomized controlled trials. Int. J. Surg. 2017, 43, 171–180. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Jiang, C.; Li, Q. A systematic review and meta-analysis comparing combined intravenous and topical tranexamic acid with intravenous administration alone in THA. PLoS ONE 2017, 12, e0186174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiong, H.; Liu, Y.; Zeng, Y.; Wu, Y.; Shen, B. The efficacy and safety of combined administration of intravenous and topical tranexamic acid in primary total knee arthroplasty: A meta-analysis of randomized controlled trials. BMC Musculoskelet. Disord. 2018, 19, 321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taeuber, I.; Weibel, S.; Herrmann, E.; Neef, V.; Schlesinger, T.; Kranke, P.; Messroghli, L.; Zacharowski, K.; Choorapoikayil, S.; Meybohm, P. Association of Intravenous Tranexamic Acid with Thromboembolic Events and Mortality: A Systematic Review, Meta-analysis, and Meta-regression. JAMA Surg. 2021, 156, e210884. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.R.; Wood, A.J. A double-blind randomised controlled trial of topical tranexamic acid after sinus surgery. Rhinol. Online 2022, 5, 120–127. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study | Objective | Study Design | Cell Lineage Used | TXA Strength and Formulation | Main Finding |
|---|---|---|---|---|---|
| Dos Reis et al. [18] | Develop a novel nasal powder formulation combining TXA with hyaluronic acid (HA) as a wound healing agent to repair the nasal mucosa. | In vitro | RPMI 2650 nasal cells | 40 mg/mL TXA vs. TXA + 0.1, 0.3 and 0.5% hyaluronic acid (TXA + HA) | No cytotoxicity at 0–40 mg/mL concentrations of TXA. Significant increase in cell proliferation above 40 mg/mL but no cytotoxicity. Use of TXA reduced the wound size to 90.5 ± 5.6% (p < 0.05) of the initial size. Addition of HA further improved healing properties Significant decrease in IL-8 but not IL-6 cytokines. |
| Gholizadeh et al. [19] | Investigate the application of a thermosensitive Chitosan-based formulation loaded with TXA for nasal epithelial wound healing. | In vitro | RPMI 2650 nasal cells | Chitosan (biodegradable polymer) containing TXA (1%) formulation vs. TXA 1% (w/v) aqueous solution | 89.32% cells still viable at 1 × 107 nM concentration of aqueous TXA 55.12% of cells still viable at 1 × 107 nM concentration of CS-TXA formulation Rate of wound healing in CS+TXA faster but after 6 h showed no statistical difference to aqueous-TXA alone |
| Haghi et al. [20] | Investigate a novel anti hemorrhagic drug delivery technology, containing TXA as a fine aerosol for delivery directly to the lung. | In vitro | Calu-3 air interface model (sub-bronchial human epithelial line) | Aqueous TXA solution (20 mg/mL) spray dried (2% w/v) vs. no treatment | Histological examination after 4 weeks of exposure to poly-TXA revealed absence of inflammatory effects and no changes in cellular morphology of the cartilage tissue, mucosal membrane and epithelial cells in the rat. |
| Wyrwa et al. [21] | Evaluate a novel electrospun material based on poly (L-lactide-co-D/L-lactide) (PLA) loaded with hemostatic agents in in vitro and in vivo experiments. | In vivo | New Zealand white rabbits | PLA (electrospun polymer dressing made of Poly) containing TXA 20% (w/w) | No significant differences in pathologist scores for inflammation between SPTT sites and control sites. Treatment of turbinate injuries with SPTT did not cause any more local tissue damage than plain gauze D-dimer levels did not differ significantly between any time points or between sheep that received SPTT or Floseal to their carotid injuries (p > 0.05). |
| R Baylis et al. [22] | Investigate a self-propelling formulation of thrombin and TXA (SPTT) in stopping bleeding in paranasal sinus injury in sheep. | Interventional animal study | Dorset cross sheep | 0.34 mg human thrombin + protonated 375 µL TXA (SPTT) on a gauze vs. Floseal (dressing containing human thrombin) OR Plain gauze | 82.2% (±22.13%) of cells still viable at 1 × 105 nM. Wound closure greater in TXA treated wounds 24 h after wound induction Significant decrease in secretion of IL-1β, IL-8 and INF- γ cytokines where TXA was used. |
| n (%) | ||
|---|---|---|
| Form of TXA given | Both IV and topical | 159 (89.9) |
| One form only | 15 (8.5) | |
| Neither form | 3 (1.7) | |
| Indication for surgery | Primary diffuse CRS | 150 (84.7) |
| Primary localized CRS | 3 (1.7) | |
| Secondary diffuse CRS | 7 (4.0) | |
| Secondary localized CRS | 10 (5.6) | |
| Other | 7 (4.0) | |
| Type of surgery | Bilateral primary comprehensive ESS | 123 (69.5) |
| Revision bilateral ESS | 36 (10.3) | |
| Primary unilateral comprehensive ESS | 18 (10.2) | |
| Adjunctive surgical procedures | 112 (63.3) | |
| Post-operative imaging | Planned/undergone revision surgery | 5 (2.8) |
| Under follow-up | 12 (6.8) | |
| Discharged from clinic | 126 (71.2) | |
| Lost to follow-up | 22 (12.4) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ratnayake Kumar, A.; Wood, A.J. The Safety of Topical and Intravenous Tranexamic Acid in Endoscopic Sinus Surgery. Sinusitis 2022, 6, 56-65. https://doi.org/10.3390/sinusitis6020008
Ratnayake Kumar A, Wood AJ. The Safety of Topical and Intravenous Tranexamic Acid in Endoscopic Sinus Surgery. Sinusitis. 2022; 6(2):56-65. https://doi.org/10.3390/sinusitis6020008
Chicago/Turabian StyleRatnayake Kumar, Agrani, and Andrew James Wood. 2022. "The Safety of Topical and Intravenous Tranexamic Acid in Endoscopic Sinus Surgery" Sinusitis 6, no. 2: 56-65. https://doi.org/10.3390/sinusitis6020008
APA StyleRatnayake Kumar, A., & Wood, A. J. (2022). The Safety of Topical and Intravenous Tranexamic Acid in Endoscopic Sinus Surgery. Sinusitis, 6(2), 56-65. https://doi.org/10.3390/sinusitis6020008