
Review of Outcomes after Diagnosis of Malignancy in Kidney Transplant Patients: UNOS Database

 , ,
, ,
Abstract
:1. Introduction
2. Methods and Materials
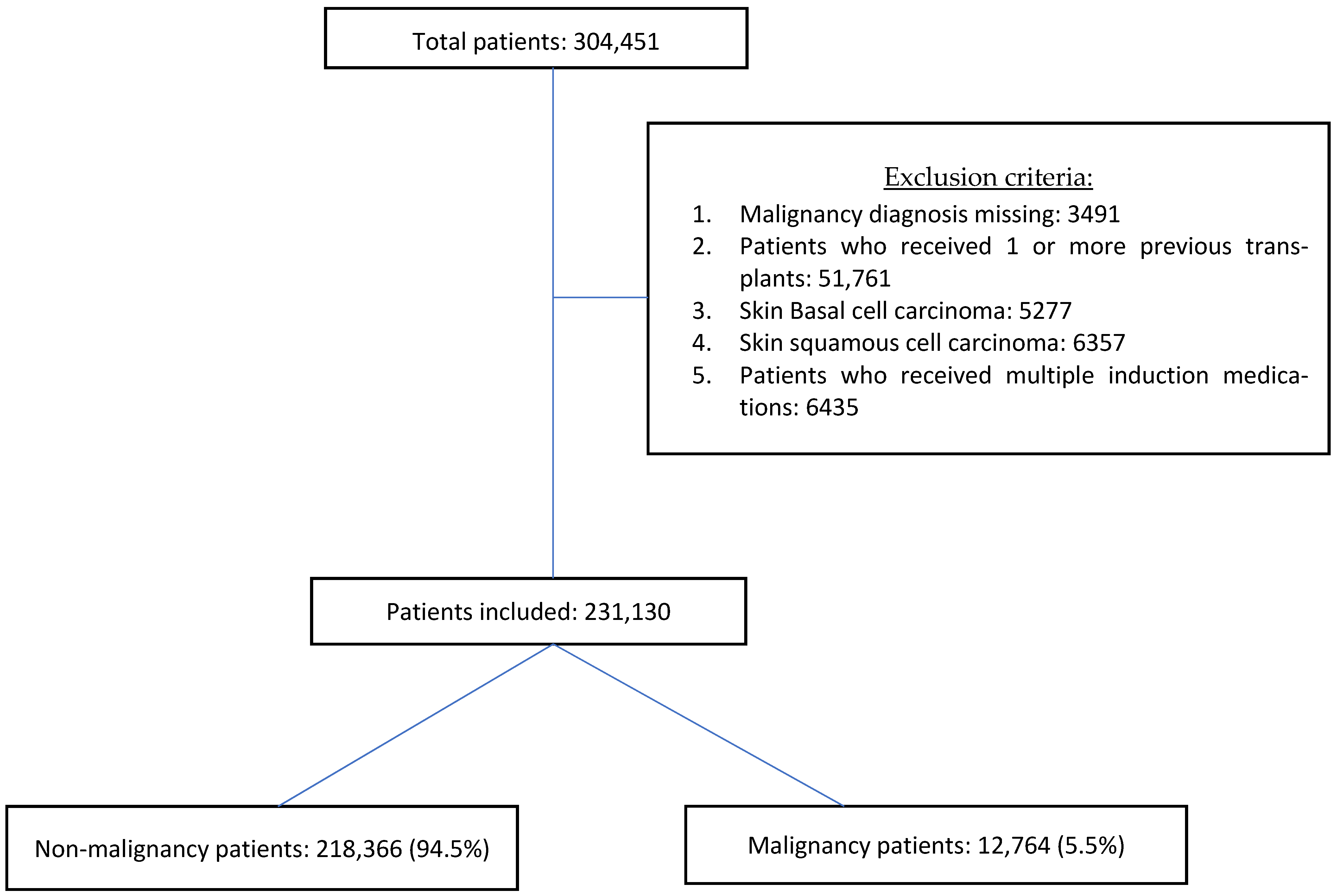
2.1. Data Source and Study Population
2.2. Descriptive Analysis of the Data
2.3. Statistical Analysis
3. Results
3.1. Malignancies of Interest and Their Incidence
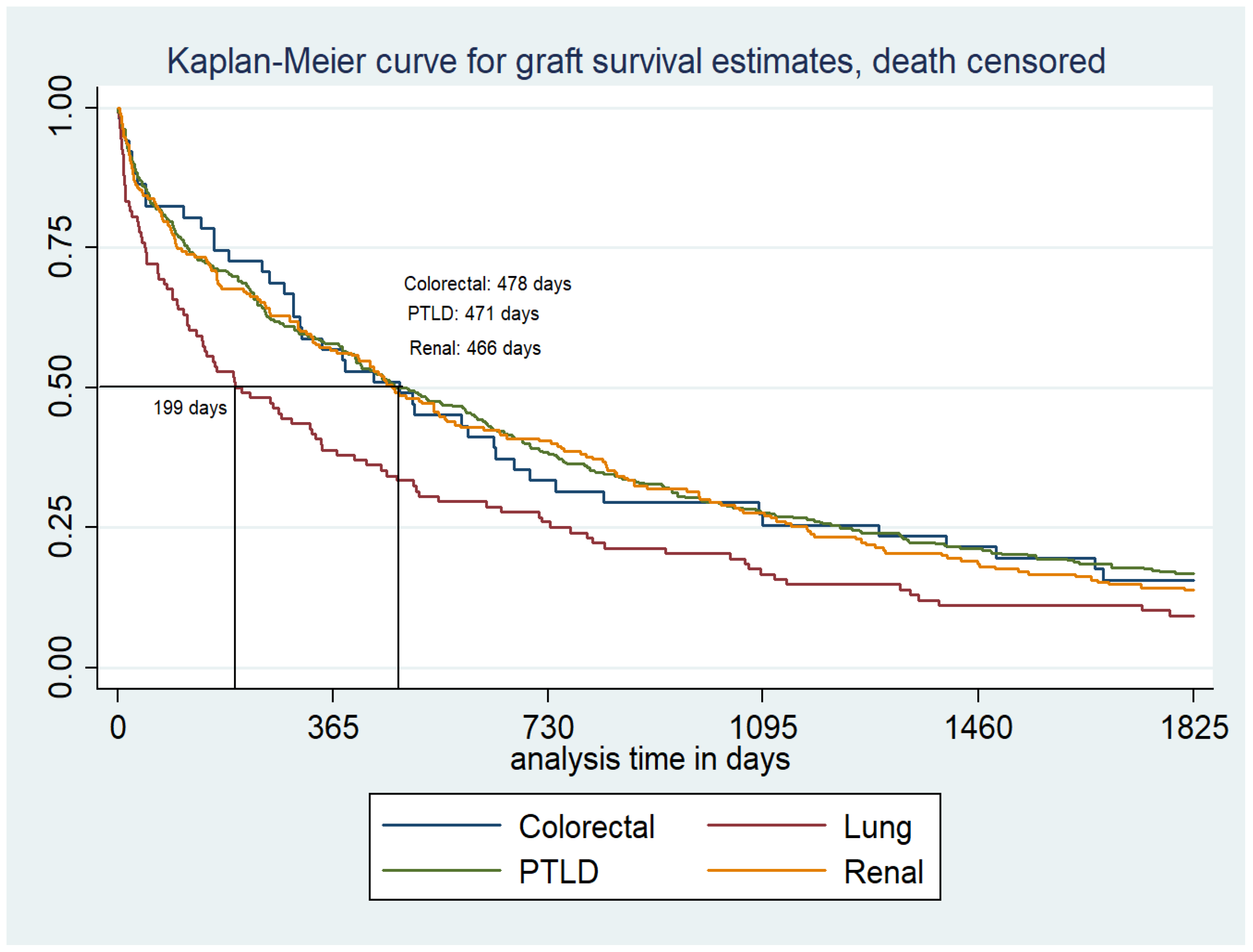
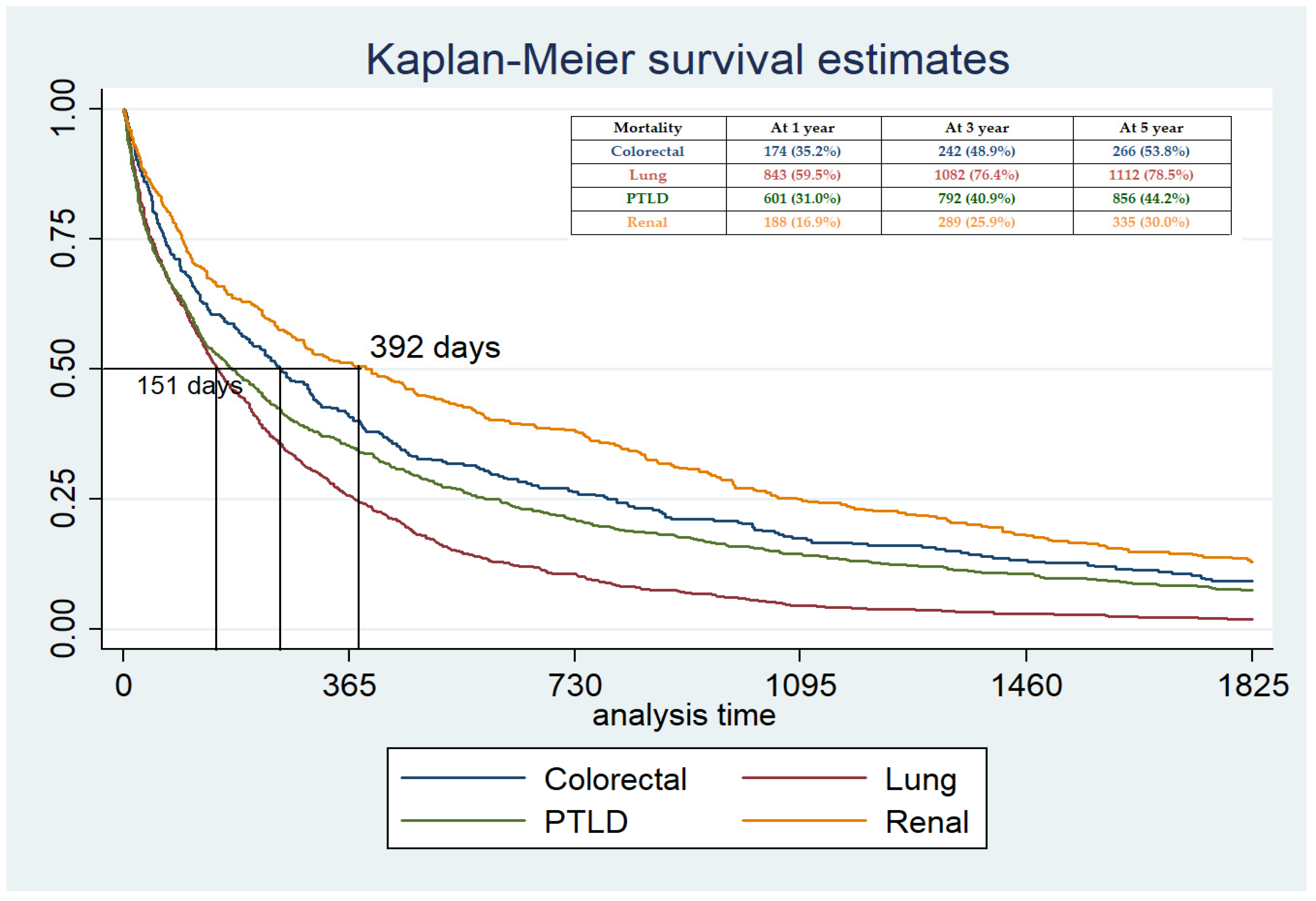
3.2. Graft Outcome and Patient Outcome (5-Year Follow-Up from Diagnosis)
3.2.1. Colorectal Malignancy
3.2.2. Lung Malignancy
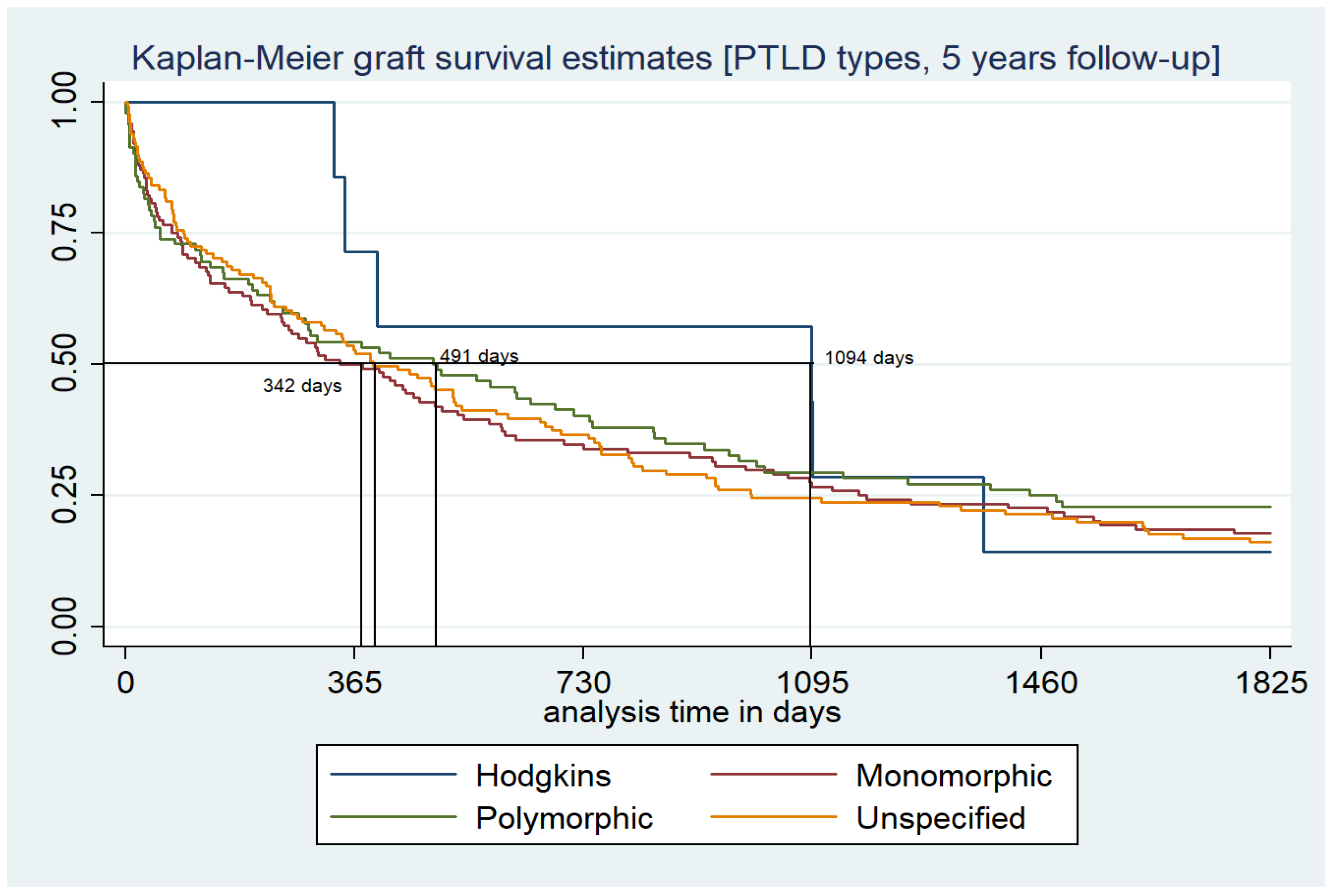
3.2.3. PTLD
3.2.4. Renal Malignancy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| UNOS/OPTN | United Network for Organs sharing/Organ procurement transplant network |
| PTLD | post-transplant lymphoproliferative disease |
| RCC | Renal cell carcinoma |
| SPK | Simultaneous pancreas and kidney transplant |
| EBV | Epstein–Barr virus |
| CMV | Cytomegalovirus |
References
- Vajdic, C.M.; van Leeuwen, M.T. Cancer incidence and risk factors after solid organ transplantation. Int. J. Cancer 2009, 125, 1747–1754. [Google Scholar] [CrossRef] [PubMed]
- Pilmore, H.; Dent, H.; Chang, S.; McDonald, S.P.; Chadban, S.J. Reduction in cardiovascular death after kidney transplantation. Transplantation 2010, 89, 851–857. [Google Scholar] [CrossRef]
- Farrugia, D.; Mahboob, S.; Cheshire, J.; Begaj, I.; Khosla, S.; Ray, D.; Sharif, A. Malignancy-related mortality following kidney transplantation is common. Kidney Int. 2014, 85, 1395–1403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collett, D.; Mumford, L.; Banner, N.R.; Neuberger, J.; Watson, C. Comparison of the incidence of malignancy in recipients of different types of organ: A UK Registry audit. Am. J. Transplant. 2010, 10, 1889–1896. [Google Scholar] [CrossRef] [PubMed]
- Kasiske, B.L.; Snyder, J.J.; Gilbertson, D.T.; Wang, C. Cancer after kidney transplantation in the United States. Am. J. Transplant. 2004, 4, 905–913. [Google Scholar] [CrossRef]
- Chapman, J.R.; Webster, A.C. Cancer after renal transplantation: The next challenge. Am. J. Transplant. 2004, 4, 841–842. [Google Scholar] [CrossRef]
- Stallone, G.; Infante, B.; Grandaliano, G. Management and prevention of post-transplant malignancies in kidney transplant recipients. Clin. Kidney J. 2015, 8, 637–644. [Google Scholar] [CrossRef] [Green Version]
- Robson, R.; Cecka, J.M.; Opelz, G.; Budde, M.; Sacks, S. Prospective registry-based observational cohort study of the long-term risk of malignancies in renal transplant patients treated with mycophenolate mofetil. Am. J. Transplant. 2005, 5, 2954–2960. [Google Scholar] [CrossRef]
- Sampaio, M.S.; Cho, Y.W.; Qazi, Y.; Bunnapradist, S.; Hutchinson, I.V.; Shah, T. Posttransplant malignancies in solid organ adult recipients: An analysis of the U.S. National Transplant Database. Transplantation 2012, 94, 990–998. [Google Scholar] [CrossRef]
- Engels, E.A.; Pfeiffer, R.M.; Fraumeni, J.F.; Kasiske, B.L.; Israni, A.K.; Snyder, J.J.; Wolfe, R.A.; Goodrich, N.P.; Bayakly, A.R.; Clarke, C.A.; et al. Spectrum of cancer risk among US solid organ transplant recipients. JAMA 2011, 306, 1891–1901. [Google Scholar] [CrossRef]
- van de Wetering, J.; Roodnat, J.I.; Hemke, A.C.; Hoitsma, A.J.; Weimar, W. Patient survival after the diagnosis of cancer in renal transplant recipients: A nested case-control study. Transplantation 2010, 90, 1542–1546. [Google Scholar] [CrossRef] [PubMed]
- Acuna, S.; Fernandes, K.A.; Daly, C.; Hicks, L.K.; Sutradhar, R.; Kim, S.J.; Baxter, N.N. Cancer Mortality Among Recipients of Solid-Organ Transplantation in Ontario, Canada. JAMA Oncol. 2016, 2, 463–469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pedotti, P.; Cardillo, M.; Rossini, G.; Arcuri, V.; Boschiero, L.; Caldara, R.; Cannella, G.; Dissegna, D.; Gotti, E.; Marchini, F.; et al. Incidence of cancer after kidney transplant: Results from the North Italy transplant program. Transplantation. 2003, 76, 1448–1451. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, F.; Fernandes, M.; Habbab, F.; de Edwardes, M.D.B.; Loertscher, R.; Meterissian, S. Malignancy after renal transplantation: Incidence and role of type of immunosuppression. Ann. Surg. Oncol. 2002, 9, 785–788. [Google Scholar] [CrossRef]
- Baccarani, U.; Adani, G.; Montanaro, D.; Risaliti, A.; Lorenzin, D.; Avellini, C.; Tulissi, P.; Groppuzzo, M.; Currò, G.; Luvisetto, F.; et al. De novo malignancies after kidney and liver transplantations: Experience on 582 consecutive cases. Transplant. Proc. 2006, 38, 1135–1137. [Google Scholar] [CrossRef]
- Webster, A.C.; Craig, J.C.; Simpson, J.M.; Jones, M.P.; Chapman, J.R. Identifying high risk groups and quantifying absolute risk of cancer after kidney transplantation: A cohort study of 15,183 recipients. Am. J. Transplant. 2007, 7, 2140–2151. [Google Scholar] [CrossRef]
- Na, R.; Grulich, A.E.; Meagher, N.S.; McCaughan, G.W.; Keogh, A.M.; Vajdic, C.M. Comparison of de novo cancer incidence in Australian liver, heart and lung transplant recipients. Am. J. Transplant. 2013, 13, 174–183. [Google Scholar] [CrossRef]
- Krynitz, B.; Edgren, G.; Lindelöf, B.; Baecklund, E.; Brattström, C.; Wilczek, H.; Smedby, K.E. Risk of skin cancer and other malignancies in kidney, liver, heart and lung transplant recipients 1970 to 2008--a Swedish population-based study. Int. J. Cancer. 2013, 132, 1429–1438. [Google Scholar] [CrossRef]
- Collins, M.G.; Teo, E.; Cole, S.R.; Chan, C.Y.; McDonald, S.P.; Russ, G.R.; Young, G.P.; Bampton, P.A.; Coates, P.T. Screening for colorectal cancer and advanced colorectal neoplasia in kidney transplant recipients: Cross sectional prevalence and diagnostic accuracy study of faecal immunochemical testing for haemoglobin and colonoscopy. BMJ 2012, 345, e4657. [Google Scholar] [CrossRef] [Green Version]
- Rawla, P.; Sunkara, T.; Barsouk, A. Epidemiology of colorectal cancer: Incidence, mortality, survival, and risk factors. Gastroenterol. Rev. 2019, 14, 89–103. [Google Scholar] [CrossRef]
- Merchea, A.; Shahjehan, F.; Croome, K.P.; Cochuyt, J.J.; Li, Z.; Colibaseanu, D.T.; Kasi, P.M. Colorectal Cancer Characteristics and Outcomes after Solid Organ Transplantation. J. Oncol. 2019, 5796108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, G.; Howard, K.; Craig, J.C.; Chapman, J.R. Cost-effectiveness of colorectal cancer screening in renal transplant recipients. Transplantation 2008, 85, 532–541. [Google Scholar] [CrossRef] [PubMed]
- Piselli, P.; Serraino, D.; Segoloni, G.P.; Sandrini, S.; Piredda, G.B.; Scolari, M.P.; Rigotti, P.; Busnach, G.; Messa, P.; Donati, D.; et al. Risk of de novo cancers after transplantation: Results from a cohort of 7217 kidney transplant recipients, Italy 1997–2009. Eur. J. Cancer 2013, 49, 336–344. [Google Scholar] [CrossRef] [PubMed]
- Sigel, K.; Veluswamy, R.; Krauskopf, K.; Mehrotra, A.; Mhango, G.; Sigel, C.; Wisnivesky, J. Lung cancer prognosis in elderly solid organ transplant recipients. Transplantation 2015, 99, 2181–2189. [Google Scholar] [CrossRef]
- Opelz, G.; Döhler, B. Lymphomas after solid organ transplantation: A collaborative transplant study report. Am. J. Transplant. 2004, 4, 222–230. [Google Scholar] [CrossRef] [PubMed]
- Taylor, A.L.; Marcus, R.; Bradley, J.A. Post-transplant lymphoproliferative disorders (PTLD) after solid organ transplantation. Crit. Rev. Oncol. Hematol. 2005, 56, 155–167. [Google Scholar] [CrossRef]
- Francis, A.; Johnson, D.W.; Craig, J.; Teixeira-Pinto, A.; Wong, G. Post-transplant lymphoproliferative disease may be an adverse risk factor for patient survival but not graft loss in kidney transplant recipients. Kidney Int. 2018, 94, 809–817. [Google Scholar] [CrossRef]
- Hiesse, C.; Rieu, P.; Kriaa, F.; Larue, J.R.; Neyrat, C.G.N.; Charpentier, B. Malignancy after renal transplantation: Analysis of incidence and risk factors in 1700 patients followed during a 25-year period. Transplant. Proc. 1997, 29, 831–833. [Google Scholar] [CrossRef]
- Hurst, F.P.; Jindal, R.M.; Graham, L.J.; Falta, E.M.; Elster, E.A.; Stackhouse, G.B.; Agodoa, L.Y.; Lentine, K.L.; Salifu, M.O.; Abbott, K. Incidence, predictors, costs, and outcome of renal cell carcinoma after kidney transplantation: USRDS experience. Transplantation 2010, 90, 898–904. [Google Scholar] [CrossRef]
- Tsaur, I.; Obermüller, N.; Jonas, D.; Blaheta, R.; Juengel, E.; Scheuermann, E.H.; Kachel, H.G.; Karalis, A.; Probst, M. De novo renal cell carcinoma of native and graft kidneys in renal transplant recipients. BJU Int. 2011, 108, 229–234. [Google Scholar] [CrossRef] [PubMed]
- Kidney Disease: Improving Global Outcomes (KDIGO) Transplant Work Group. KDIGO clinical practice guideline for the care of kidney transplant recipients. Am. J. Transplant. 2009, 3 (Suppl. 9), S1–S155. [Google Scholar]
- Wong, G.; Chapman, J.R.; Craig, J.C. Cancer screening in renal transplant recipients: What is the evidence? Clin. J. Am. Soc. Nephrol. 2008, 3 (Suppl. 2), S87–S100. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No Malignancy (218,366) | Malignancy (12,764) | p-Value | |
|---|---|---|---|
| Age (Median, IQR) | 51 (39–61) | 58 (50–65) | 0.0001 |
| Gender (male) | 60.3% | 64.4% | <0.001 |
| Caucasian | 48.1% | 63.5% | <0.001 |
| African American | 27.3% | 21.7% | <0.001 |
| Type of transplant | |||
| Kidney transplant | 209,294 (95.9%) | 12,241 (95.9%) | |
| SPK # | 2063 (0.94%) | 14 (0.11%) | <0.001 |
| Heart and kidney | 1059 (0.48%) | 92 (0.72%) | <0.001 |
| Liver and kidney | 5897 (2.7%) | 415 (3.2%) | <0.001 |
| Intestine and kidney | 41 (0.00%) | 2 (0.00%) | |
| Lung and kidney | 43 (0.00%) | 3 (0.00%) | |
| Some risk factors | |||
| EBV @ high risk (D+ve, R-ve) | 6.8% | 7.2% | 0.052 |
| CMV $ high risk (D+ve, R-ve) | 17.9% | 17.4% | 0.15 |
| Preemptive transplant | 17.7% | 20.4% | <0.001 |
| Dialysis vintage time | 1024 (470–1806) | 900 (423–1560) | <0.001 |
| Deceased donor | 68.2% | 68.5% | 0.44 |
| Induction | |||
| Thymoglobulin | 41.6% | 40.6% | 0.03 |
| Campath | 11.5% | 9.04% | <0.001 |
| Simulect | 20.3% | 21.3% | 0.005 |
| Multiple maintenance | |||
| Tacro 1 + mmf 2 (180,009) | 170,421 (78.0%) | 9588 (75.1%) | <0.001 |
| Rapa 3 + Tacro (4010) | 3743 (1.71%) | 267 (2.09%) | 0.005 |
| Rapa + Tacro + mmf (1578) | 1472 (0.67%) | 106 (0.83%) | 0.01 |
| Cyclo 4 + Aza 5 (682) | 635 (0.29%) | 47 (0.37%) | 0.84 |
| Outcome | |||
| Death-censored graft failure | 17.6% | 13.7% | <0.001 |
| Death rate | 22.0% | 52.7% | <0.001 |
| Type of Malignancy (Total Number of Patients) | Incidence (95% CI) 0–5 Year Follow-Up Period | Incidence (95% CI) 5–10 Year Follow-Up Period |
|---|---|---|
| Colorectal (494) | 2.99 (2.64–3.39) | 5.47 (4.72–6.34) |
| Lung (1416) | 9.21 (8.57–9.89) | 15.68 (14.38–17.11) |
| PTLD # (1936) | 15.61 (14.77–16.5) | 14.58 (13.32–15.96) |
| Renal (1115) | 8.55 (7.94–9.20) | 9.46 (8.46–10.59) |
| Graft Survival | ||
| Malignancy | Death-censored graft failure | Diagnosis to graft survival time (days) |
| Colorectal | 51 (10.3%) | 478 (163–1292) |
| Lung | 108 (7.6%) | 199 (45–733) |
| PTLD # | 386 (19.9%) | 471 (118–1226) |
| Renal | 210 (18.8%) | 466 (100–1169) |
| Patient Survival | ||
| Malignancy | Total number of deaths | Time from Diagnosis to death (days) |
| Colorectal | 304/494 (61.5%) | 254 (68–781) |
| Lung | 1190/1416 (84%) | 151 (45–373) |
| PTLD | 950/1936 (49.1%) | 175 (41–585) |
| Renal | 396/1115 (35.5%) | 392 (95–1089) |
| Graft Survival for PTLD types | ||
| PTLD types | Death-censored graft failure | Graft survival time |
| Hodgkin’s (n = 49) | 8 (16.3%) | 1094 (349–1368) |
| Monomorphic (n = 666) | 124 (18.6%) | 342 (73–1168) |
| Polymorphic (n = 421) | 91 (21.6%) | 491 (55–1441) |
| Unspecified (n = 800) | 158 (19.8%) | 395 (93–998) |
| Graft Failure Cause | Colorectal (51) | Lung (115) | PTLD # (381) | Renal (215) |
| Acute rejection | 3 (5.9%) | 12 (10.4%) | 66 (17.3%) | 20 (9.3%) |
| Infection | 3 (5.9%) | 4 (3.5%) | 23 (6.0%) | 6 (2.8%) |
| Chronic rejection | 25 (49%) | 38 (33%) | 112 (29.4%) | 81(37.6%) |
| Cancer Complications | 2 (3.9%) | 16 (13.9%) | 64 (16.8%) | 34(15.8%) |
| BK | -- | 3 (2.6%) | 11 (2.9%) | 6 (2.8%) |
| Others | 18 (35.3%) | 36 (31.3%) | 88 (23.1%) | 53 (24.6%) |
| 6 transplant nephrectomy | ||||
| Missing cause of graft failure | -- | 6 (5.2%) | 17 (4.4%) | 9 (4.2%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patel, H.; Agrawal, N.; Nissaisorakarn, V.; Gupta, R.; Cardarelli, F. Review of Outcomes after Diagnosis of Malignancy in Kidney Transplant Patients: UNOS Database. Transplantology 2021, 2, 253-263. https://doi.org/10.3390/transplantology2030024
Patel H, Agrawal N, Nissaisorakarn V, Gupta R, Cardarelli F. Review of Outcomes after Diagnosis of Malignancy in Kidney Transplant Patients: UNOS Database. Transplantology. 2021; 2(3):253-263. https://doi.org/10.3390/transplantology2030024
Chicago/Turabian StylePatel, Het, Nikhil Agrawal, Voravech Nissaisorakarn, Ridhi Gupta, and Francesca Cardarelli. 2021. "Review of Outcomes after Diagnosis of Malignancy in Kidney Transplant Patients: UNOS Database" Transplantology 2, no. 3: 253-263. https://doi.org/10.3390/transplantology2030024
APA StylePatel, H., Agrawal, N., Nissaisorakarn, V., Gupta, R., & Cardarelli, F. (2021). Review of Outcomes after Diagnosis of Malignancy in Kidney Transplant Patients: UNOS Database. Transplantology, 2(3), 253-263. https://doi.org/10.3390/transplantology2030024