
Trends in the Use of Complementary and Alternative Therapies among US Adults with Current Asthma

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.1.1. Complementary and Alternative Therapy Use Ascertainment
2.1.2. Covariates Ascertainment
2.2. Statistical Analysis
3. Results
3.1. Use of any CAM among US Adults with Current Asthma in 2019
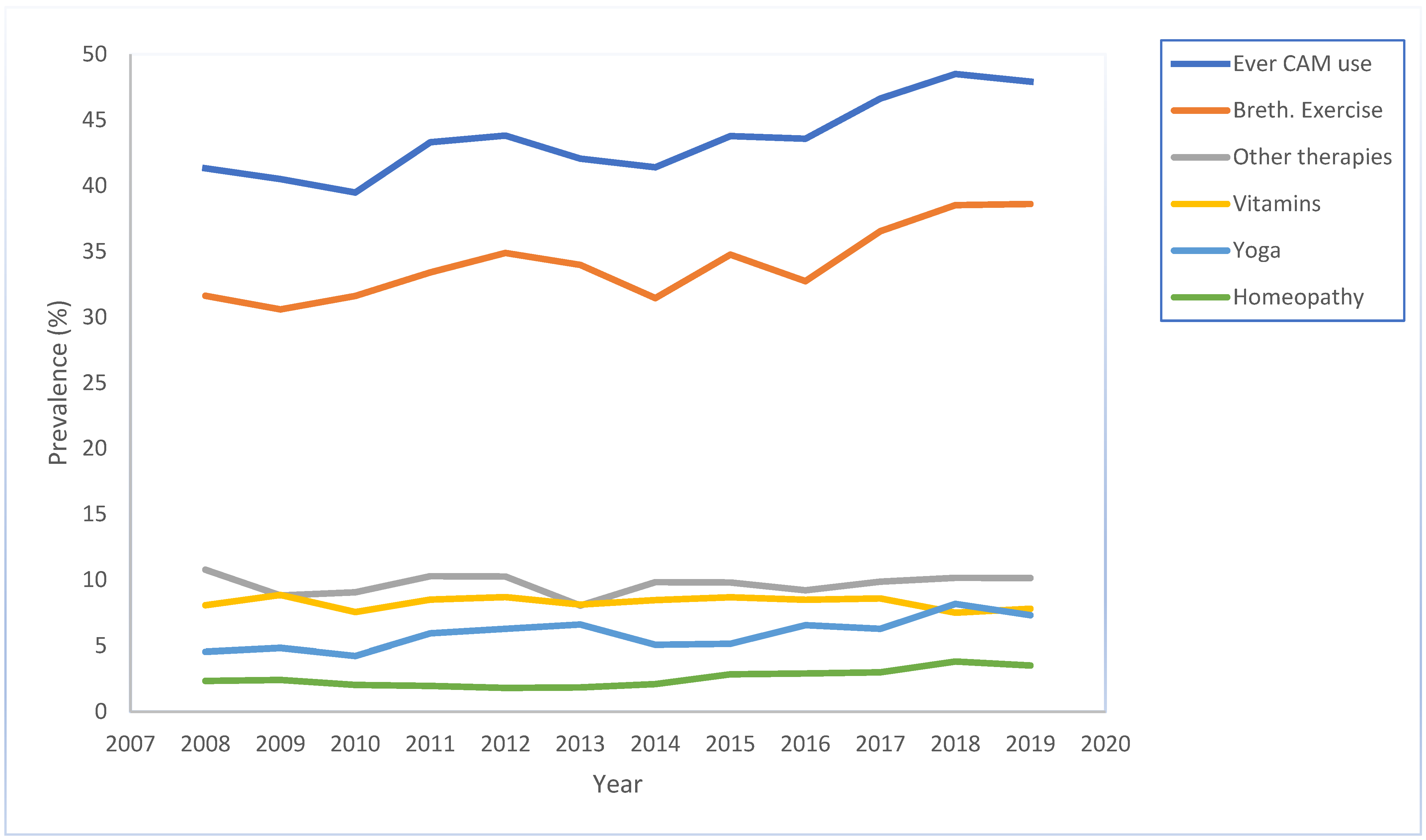
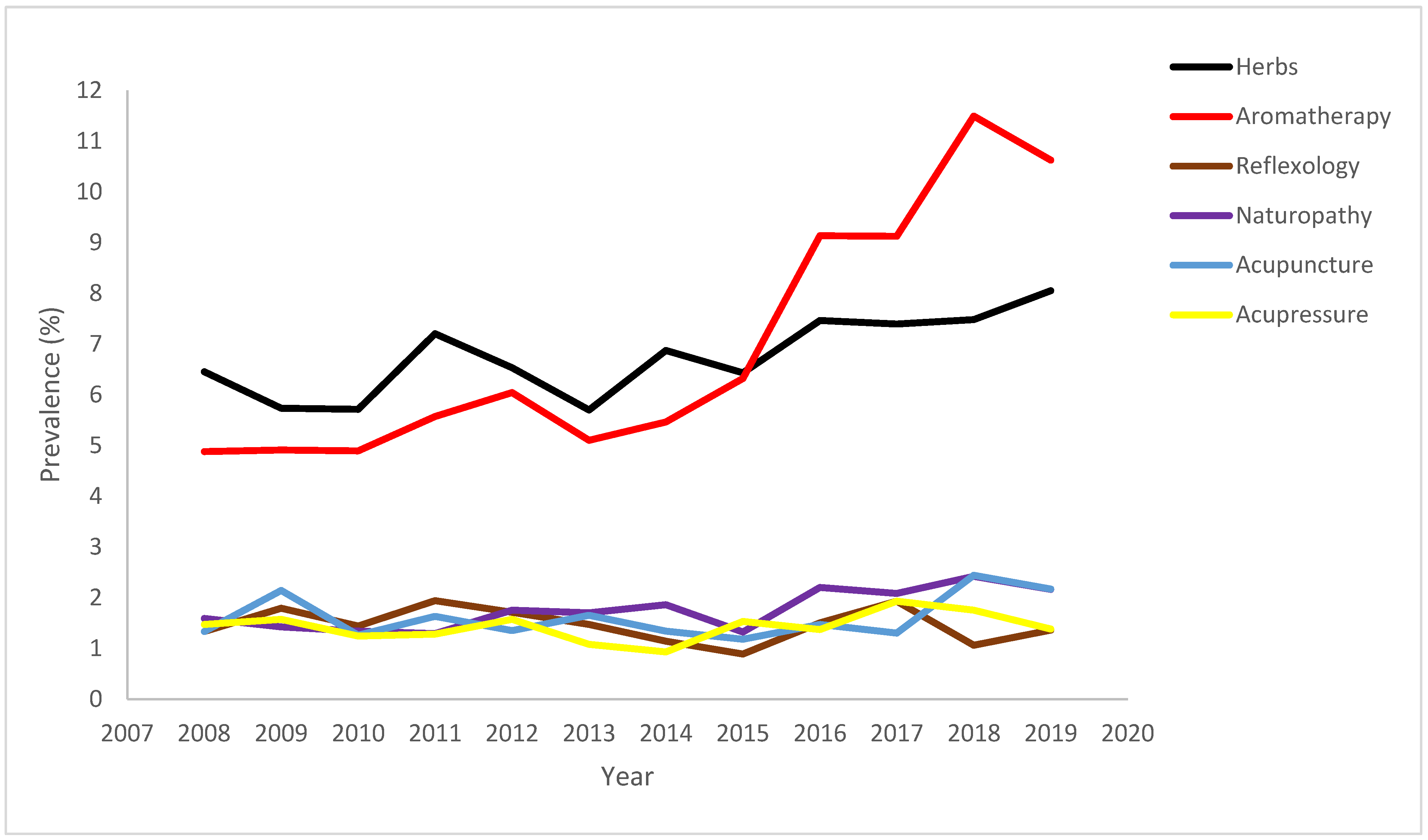
3.2. CAM Trend across Years
3.3. Trend by Subgroups
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Reddel, H.K.; Bacharier, L.B.; Bateman, E.D.; Brightling, C.E.; Brusselle, G.G.; Buhl, R.; Cruz, A.A.; Duijts, L.; Drazen, J.M.; FitzGerald, J.M. Global Initiative for Asthma Strategy 2021: Executive summary and rationale for key changes. Am. J. Respir. Crit. Care Med. 2022, 205, 17–35. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Most Recent National Asthma Data. 2020. Available online: https://www.cdc.gov/asthma/most_recent_national_asthma_data.htm (accessed on 3 January 2023).
- Chen, W.; FitzGerald, J.M.; Rousseau, R.; Lynd, L.D.; Tan, W.C.; Sadatsafavi, M. Complementary and alternative asthma treatments and their association with asthma control: A population-based study. BMJ Open 2013, 3, e003360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robinson, A.; McGrail, M.R. Disclosure of CAM use to medical practitioners: A review of qualitative and quantitative studies. Complement. Ther. Med. 2004, 12, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Zollman, C.; Vickers, A. What is complementary medicine? BMJ 1999, 319, 693–696. [Google Scholar] [CrossRef]
- Kim, E.J.; Simonson, J.; Jacome, S.; Conigliaro, J.; Hanchate, A.D.; Hajizadeh, N. Disparities in complementary alternative medicine use and asthma exacerbation in the United States. J. Asthma 2020, 57, 866–874. [Google Scholar] [CrossRef]
- Shaw, A.; Noble, A.; Salisbury, C.; Sharp, D.; Thompson, E.; Peters, T.J. Predictors of complementary therapy use among asthma patients: Results of a primary care survey. Health Soc. Care Community 2008, 16, 155–164. [Google Scholar] [CrossRef]
- Vincent, C.; Furnham, A. Why do patients turn to complementary medicine? An empirical study. Br. J. Clin. Psychol. 1996, 35, 37–48. [Google Scholar] [CrossRef]
- Mainardi, T.; Kapoor, S.; Bielory, L. Complementary and alternative medicine: Herbs, phytochemicals and vitamins and their immunologic effects. J. Allergy Clin. Immunol. 2009, 123, 283–294.e10. [Google Scholar] [CrossRef]
- Slader, C.A.; Reddel, H.K.; Jenkins, C.R.; Armour, C.L.; Bosnic-Anticevich, S.Z. Complementary and alternative medicine use in asthma: Who is using what? Respirology 2006, 11, 373–387. [Google Scholar] [CrossRef]
- Clarke, R.; Lundy, F.T.; McGarvey, L. Herbal treatment in asthma and COPD–current evidence. Clin. Phytosci. 2015, 1, 4. [Google Scholar] [CrossRef]
- Singh, B.B.; Khorsan, R.; Vinjamury, S.P.; Der-Martirosian, C.; Kizhakkeveettil, A.; Anderson, T.M. Herbal treatments of asthma: A systematic review. J. Asthma 2007, 44, 685–698. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Xuan, N.-X.; Ying, S.-M.; Li, W.; Chen, Z.-H.; Shen, H.-H. Herbal medicines for asthmatic inflammation: From basic researches to clinical applications. Mediat. Inflamm. 2016, 2016, 6943135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCarney, R.W.; Linde, K.; Lasserson, T.J. Homeopathy for chronic asthma. Cochrane Database Syst. Rev. 2004, 2004, CD000353. [Google Scholar] [CrossRef]
- Li, M.; Zhang, X.; Bao, H.; Li, C.; Zhang, P. Acupuncture for asthma: Protocol for a systematic review. Medicine 2017, 96, e7296. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-M.; Xie, X.-L.; Xiao, P.-Y.; Wang, Q.-H.; Wang, J.-S.; Yu, X.-D.; Deng, S. Acupuncture on treating asthma: A protocol for systematic review and meta analysis. Medicine 2020, 99, e18457. [Google Scholar] [CrossRef]
- Cramer, H.; Posadzki, P.; Dobos, G.; Langhorst, J. Yoga for asthma: A systematic review and meta-analysis. Ann. Allergy Asthma Immunol. 2014, 112, 503–510.e5. [Google Scholar] [CrossRef]
- O’Connor, E.; Patnode, C.D.; Burda, B.U.; Buckley, D.I.; Whitlock, E.P. Breathing Exercises and/or Retraining Techniques in the Treatment of Asthma: Comparative Effectiveness; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2012.
- Santino, T.A.; Chaves, G.S.; Freitas, D.A.; Fregonezi, G.A.; Mendonca, K.M. Breathing exercises for adults with asthma. Cochrane Database Syst. Rev. 2020, 3, CD001277. [Google Scholar] [CrossRef]
- Brygge, T.; Heinig, J.; Collins, P.; Ronborg, S.; Gehrchen, P.; Hilden, J.; Heegaard, S.; Poulsen, L. Reflexology and bronchial asthma. Respir. Med. 2001, 95, 173–179. [Google Scholar] [CrossRef] [Green Version]
- Ng, T.; Wong, M.; Hong, C.; Koh, K.; Goh, L. The use of complementary and alternative medicine by asthma patients. QJM 2003, 96, 747–754. [Google Scholar] [CrossRef] [Green Version]
- Liang, Y.; Lenon, G.B.; Yang, A.W.H. Acupressure for respiratory allergic diseases: A systematic review of randomised controlled trials. Acupunct. Med. 2017, 35, 413–420. [Google Scholar] [CrossRef]
- 2016 BRFSS Survey Data and Documentation. Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/brfss/annual_data/annual_2016.html (accessed on 3 January 2022).
- 2016 BRFSS Asthma Call-Back Survey (ACBS). Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/brfss/acbs/2016_documentation.html (accessed on 3 January 2022).
- Education, N.A.; Program, P. Expert panel report 3 (EPR-3): Guidelines for the diagnosis and management of asthma-summary report 2007. J. Allergy Clin. Immunol. 2007, 120 (Suppl. S5), S94–S138. [Google Scholar]
- Zahran, H.S.; Person, C.J.; Bailey, C.; Moorman, J.E. Predictors of asthma self-management education among children and adults—2006–2007 behavioral risk factor surveillance system asthma call-back survey. J. Asthma 2012, 49, 98–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zahran, H.S.; Bailey, C.M.; Qin, X.; Moorman, J.E. Assessing asthma control and associated risk factors among persons with current asthma–findings from the child and adult Asthma Call-back Survey. J. Asthma 2015, 52, 318–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.J.; Fay, M.P.; Feuer, E.J.; Midthune, D.N. Permutation tests for joinpoint regression with applications to cancer rates. Stat. Med. 2000, 19, 335–351. [Google Scholar] [CrossRef]
- Ernst, E. Complementary therapies for asthma: What patients use. J. Asthma 1998, 35, 667–671. [Google Scholar] [CrossRef] [PubMed]
- Guallar, E.; Stranges, S.; Mulrow, C.; Appel, L.J.; Miller III, E.R. Enough is enough: Stop wasting money on vitamin and mineral supplements. Ann. Intern. Med. 2013, 159, 850–851. [Google Scholar] [CrossRef]
- Huang, H.-Y.; Caballero, B.; Chang, S.; Alberg, A.J.; Semba, R.D.; Schneyer, C.R.; Wilson, R.F.; Cheng, T.-Y.; Vassy, J.; Prokopowicz, G. The efficacy and safety of multivitamin and mineral supplement use to prevent cancer and chronic disease in adults: A systematic review for a National Institutes of Health state-of-the-science conference. Ann. Intern. Med. 2006, 145, 372–385. [Google Scholar] [CrossRef] [Green Version]
- Marra, M.V.; Boyar, A.P. Position of the American Dietetic Association: Nutrient supplementation. J. Am. Diet. Assoc. 2009, 109, 2073–2085. [Google Scholar] [CrossRef]
- Barnes, P.M.; Bloom, B.; Nahin, R.L. Complementary and alternative medicine use among adults and children: United States, 2007. Natl. Health Stat. Rep. 2008, 12, 1–23. [Google Scholar]
- Ramsey, S.D.; Zeliadt, S.B.; Blough, D.K.; Fedorenko, C.R.; Fairweather, M.E.; McDermott, C.L.; Penson, D.F.; Van Den Eeden, S.K.; Hamilton, A.S.; Arora, N.K. Complementary and alternative medicine use, patient-reported outcomes, and treatment satisfaction among men with localized prostate cancer. Urology 2012, 79, 1034–1041. [Google Scholar] [CrossRef] [Green Version]
- Bishop, F.; Rea, A.; Lewith, H.; Chan, Y.; Saville, J.; Prescott, P.; Von Elm, E.; Lewith, G. Complementary medicine use by men with prostate cancer: A systematic review of prevalence studies. Prostate Cancer Prostatic Dis. 2011, 14, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Bishop, F.L.; Lewith, G.T. Who uses CAM? A narrative review of demographic characteristics and health factors associated with CAM use. Evid-Based Complement. Altern. Med. 2010, 7, 11–28. [Google Scholar] [CrossRef] [Green Version]
- Barnes, P.M.; Powell-Griner, E.; McFann, K.; Nahin, R.L. Complementary and Alternative Medicine Use among Adults: United States, 2002. In Seminars in Integrative Medicine; Elsevier: Amsterdam, The Netherlands, 2004; pp. 54–71. [Google Scholar] [CrossRef]
- Goldstein, M.S.; Brown, E.R.; Ballard-Barbash, R.; Morgenstern, H.; Bastani, R.; Lee, J.; Gatto, N.; Ambs, A. The use of complementary and alternative medicine among California adults with and without cancer. Evid-Based Complement. Altern. Med. 2005, 2, 557–565. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.; Braunack-Mayer, A.; Wittert, G. What do we know about men’s help-seeking and health service use? Med. J. Aust. 2006, 184, 81–83. [Google Scholar] [CrossRef] [Green Version]
- Nathanson, C.A. Illness and the feminine role: A theoretical review. Soc. Sci. Med. 1975, 9, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Jones, E.; Nissen, L.; McCarthy, A.; Steadman, K.; Windsor, C. Exploring the use of complementary and alternative medicine in cancer patients. Integr. Cancer Ther. 2019, 18, 1534735419846986. [Google Scholar] [CrossRef] [Green Version]
- Su, D.; Li, L. Trends in the use of complementary and alternative medicine in the United States: 2002–2007. J. Health Care Poor Underserved 2011, 22, 296–310. [Google Scholar] [CrossRef]
- Rhee, T.G.; Evans, R.L.; McAlpine, D.D.; Johnson, P.J. Racial/ethnic differences in the use of complementary and alternative medicine in US adults with moderate mental distress: Results from the 2012 National Health Interview Survey. J. Prim. Care Community Health 2017, 8, 43–54. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Use of any CAM 2019 | ||||
|---|---|---|---|---|
| No. of Participants | No. of Participants | Weighted% (95% CI) a | p-Value | |
| Use of at least one CAM | 8928 | 3946 | 47.92 (45.59–50.24) | |
| Age | <0.0001 | |||
| 18–55 years | 3433 | 1702 | 51.75 (48.51–54.99) | |
| >55 years | 5495 | 2244 | 41.64 (38.89–44.39) | |
| Sex | <0.0001 | |||
| Women | 5967 | 2808 | 52.58 (49.69–55.47) | |
| Men | 2961 | 1138 | 40.03 (36.28–43.78) | |
| Race | 0.16 | |||
| White Non-Hispanic | 7161 | 3057 | 46.04 (43.57–48.50) | |
| Black Non-Hispanic | 417 | 188 | 48.88 (39.10–58.67) | |
| Multiracial/other race Non-Hispanic | 623 | 326 | 55.32 (45.87–64.77) | |
| Hispanic | 601 | 314 | 52.79 (45.02–60.56) | |
| Income | 0.02 | |||
| ≥$25,000 | 5277 | 2228 | 44.93 (41.93–47.92) | |
| <$25,000 | 1096 | 573 | 53.51 (47.19–59.83) | |
| Daytime Symptoms | <0.0001 | |||
| ≤2 days/week | 5532 | 2184 | 58.2 (50.96–65.43) | |
| >2 days/week | 2305 | 1207 | 59.09 (54.95–63.22) | |
| Throughout the day | 880 | 487 | 42.75 (39.78–45.71) | |
| Night symptoms | <0.0001 | |||
| ≤2 times a month | 6917 | 2790 | 59.19 (50.70–67.68) | |
| 1–3 times a week | 1175 | 697 | 65.46 (60.15–70.77) | |
| ≥4 times a week | 578 | 344 | 43.94 (41.27–46.60) | |
| 12-Month Prevalence of Use, Weighted% | 2019 vs. 2008 | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | PR (95% CI) | PD (95% CI) | |
| Increased CAM use a | ||||||||||||||
| Ever using CAM | 41.3 | 40.5 | 39.5 | 43.3 | 43.8 | 42.1 | 41.4 | 43.8 | 43.6 | 46.6 | 48.5 | 47.9 | 1.3 (1.2, 1.5) | 6.6 (3.5, 9.7) |
| Herbs | 6.5 | 5.7 | 5.7 | 7.2 | 6.5 | 5.7 | 6.9 | 6.4 | 7.5 | 7.4 | 7.5 | 8.1 | 1.3 (1.0, 1.6) | 1.6 (−0.1, 3.3) |
| Aromatherapy | 4.9 | 4.9 | 4.9 | 5.6 | 6.0 | 5.1 | 5.5 | 6.3 | 9.1 | 9.1 | 11.5 | 10.6 | 2.3 (1.7, 3.1) | 5.7 (3.8, 7.6) |
| Homeopathy | 2.3 | 2.4 | 2.0 | 2.0 | 1.8 | 1.9 | 2.1 | 2.9 | 2.9 | 3.0 | 3.8 | 3.5 | 1.5 (1.1, 2.2) | 1.2 (0.2, 2.2) |
| Yoga | 4.6 | 4.9 | 4.2 | 6.0 | 6.3 | 6.6 | 5.1 | 5.2 | 6.6 | 6.3 | 8.2 | 7.3 | 1.7 (1.2, 2.2) | 2.8 (0.1, 4.5) |
| Breath. Exercises | 31.6 | 30.6 | 31.6 | 33.4 | 34.9 | 34.0 | 31.5 | 34.8 | 32.7 | 36.5 | 38.5 | 38.6 | 1.4 (1.2, 1.6) | 7.0 (3.9, 10.1) |
| Naturopathy | 1.6 | 1.4 | 1.3 | 1.3 | 1.8 | 1.7 | 1.9 | 1.3 | 2.2 | 2.1 | 2.4 | 2.2 | 1.4 (0.9, 2.1) | 0.6 (−0.2, 1.4) |
| Stable CAM use b | ||||||||||||||
| Vitamins | 8.1 | 8.9 | 7.6 | 8.5 | 8.7 | 8.1 | 8.5 | 8.7 | 8.5 | 8.6 | 7.5 | 7.8 | 1.0 (0.8, 1.2) | −0.3 (−2.0, 1.5) |
| Acupuncture | 1.3 | 2.1 | 1.3 | 1.6 | 1.4 | 1.7 | 1.3 | 1.2 | 1.5 | 1.3 | 2.4 | 2.2 | 1.6 (1.0, 2.8) | 0.9 (−0.2, 0.1) |
| Acupressure | 1.5 | 1.6 | 1.2 | 1.3 | 1.6 | 1.1 | 0.9 | 1.5 | 1.4 | 1.9 | 1.8 | 1.4 | 0.9 (0.6, 1.5) | −0.1 (−0.8, 0.6) |
| Reflexology | 1.3 | 1.8 | 1.4 | 1.9 | 1.7 | 1.5 | 1.1 | 0.9 | 1.5 | 1.9 | 1.1 | 1.4 | 1.0 (0.7, 1.6) | 0.02 (−0.6, 0.6) |
| Other therapies | 10.8 | 8.8 | 9.1 | 10.3 | 10.3 | 8.1 | 9.8 | 9.8 | 9.2 | 9.9 | 10.2 | 10.2 | 0.9 (0.8, 1.1) | −0.6 (−2.4, 1.1) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ogbu, C.E.; Oparanma, C.; Ogbu, S.C.; Ujah, O.I.; Okoli, M.L.; Kirby, R.S. Trends in the Use of Complementary and Alternative Therapies among US Adults with Current Asthma. Epidemiologia 2023, 4, 94-105. https://doi.org/10.3390/epidemiologia4010010
Ogbu CE, Oparanma C, Ogbu SC, Ujah OI, Okoli ML, Kirby RS. Trends in the Use of Complementary and Alternative Therapies among US Adults with Current Asthma. Epidemiologia. 2023; 4(1):94-105. https://doi.org/10.3390/epidemiologia4010010
Chicago/Turabian StyleOgbu, Chukwuemeka E., Chisa Oparanma, Stella C. Ogbu, Otobo I. Ujah, Menkeoma L. Okoli, and Russell S. Kirby. 2023. "Trends in the Use of Complementary and Alternative Therapies among US Adults with Current Asthma" Epidemiologia 4, no. 1: 94-105. https://doi.org/10.3390/epidemiologia4010010
APA StyleOgbu, C. E., Oparanma, C., Ogbu, S. C., Ujah, O. I., Okoli, M. L., & Kirby, R. S. (2023). Trends in the Use of Complementary and Alternative Therapies among US Adults with Current Asthma. Epidemiologia, 4(1), 94-105. https://doi.org/10.3390/epidemiologia4010010