
Obesity during Adolescence and Feeding Practices during Infancy: Cross-Sectional Study

 , ,
, ,
Abstract
:1. Background
Objectives
2. Methods
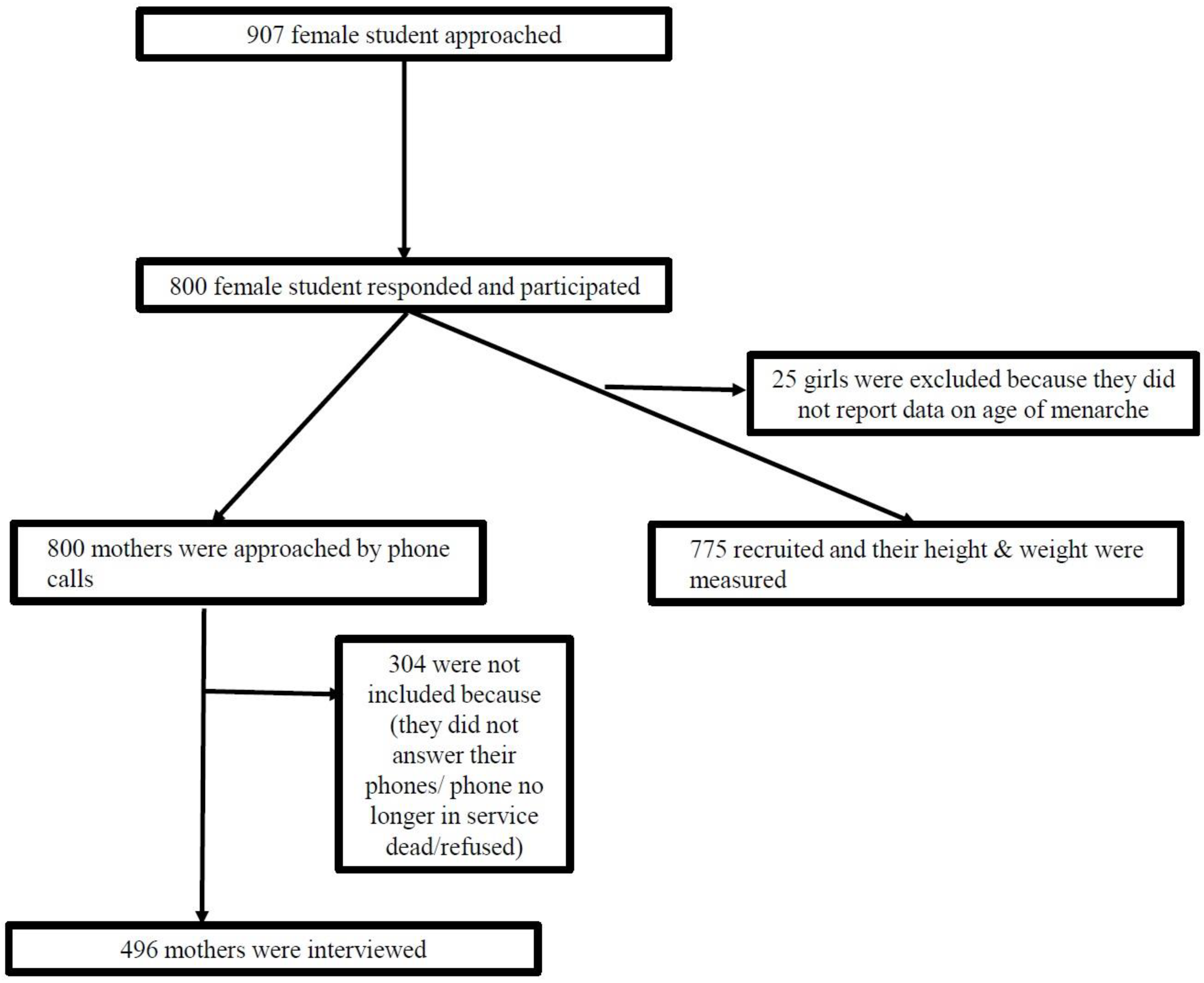
2.1. Study Design and Study Participants
2.2. Data Collection
2.3. Data Management and Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jedrychowski, W.; Perera, F.; Jankowski, J.; Butscher, M.; Mroz, E.; Flak, E.; Kaim, I.; Lisowska-Miszczyk, I.; Skarupa, A.; Sowa, A. Effect of exclusive breastfeeding on the development of children’s cognitive function in the Krakow prospective birth cohort study. Eur. J. Pediatr. 2012, 171, 151–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Størdal, K.; Lundeby, K.M.; Brantsæter, A.L.; Haugen, M.; Nakstad, B.; Lund-Blix, N.A.; Stene, L.C. Breast-feeding and Infant Hospitalization for Infections: Large Cohort and Sibling Analysis. J. Pediatr. Gastroenterol. Nutr. 2017, 65, 225–231. [Google Scholar] [CrossRef] [PubMed]
- UNICEF. Infant and Young Child Feeding. Available online: https://data.unicef.org/topic/nutrition/infant-and-young-child-feeding/ (accessed on 11 September 2019).
- Victora, C.G.; Bahl, R.; Barros, A.J.; Franca, G.V.; Horton, S.; Krasevec, J.; Murch, S.; Sankar, M.J.; Walker, N.; Rollins, N.C. Breastfeeding in the 21st century: Epidemiology, mechanisms, and lifelong effect. Lancet 2016, 387, 475–490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuwait Nutritional Surveillance System. The Kuwait Nutrition Surveillance System Annual Report; Food and Nutrition Administration, FNA: White Oak, MD, USA, 2017.
- World Health Orgnization WHO. Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 8 October 2020).
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- EMAN EMAfCoN-CD. Survey of Risk Factors for Chronic Non Communicable Diseases; MOH, WHO: Kuwait City, Kuwait, 2015; Volume 199, p. 199. [Google Scholar]
- Barker, D.J.; Martyn, C.N. The maternal and fetal origins of cardiovascular disease. J. Epidemiol. Community Health 1992, 46, 8–11. [Google Scholar] [CrossRef]
- Friedman, J.M.; Halaas, J.L. Leptin and the regulation of body weight in mammals. Nature 1998, 395, 763–770. [Google Scholar] [CrossRef]
- Picó, C.; Oliver, P.; Sánchez, J.; Miralles, O.; Caimari, A.; Priego, T.; Palou, A. The intake of physiological doses of leptin during lactation in rats prevents obesity in later life. Int. J. Obes. 2007, 31, 1199–1209. [Google Scholar] [CrossRef] [Green Version]
- Beyerlein, A.; von Kries, R. Breastfeeding and body composition in children: Will there ever be conclusive empirical evidence for a protective effect against overweight? Am. J. Clin. Nutr. 2011, 94 (Suppl. S6), 1772s–1775s. [Google Scholar] [CrossRef] [Green Version]
- Yan, J.; Liu, L.; Zhu, Y.; Huang, G.; Wang, P.P. The association between breastfeeding and childhood obesity: A meta-analysis. BMC Public Health 2014, 14, 1267. [Google Scholar] [CrossRef] [Green Version]
- Huus, K.; Ludvigsson, J.F.; Enskar, K.; Ludvigsson, J. Exclusive breastfeeding of Swedish children and its possible influence on the development of obesity: A prospective cohort study. BMC Pediatr. 2008, 8, 42. [Google Scholar] [CrossRef]
- Public Authority for Civil Information PACI. Statistical Report. Available online: http://stat.paci.gov.kw/englishreports/#DataTabPlace:ColumnBUseType (accessed on 24 October 2018).
- Al-Mathkoori, R.; Nur, U.; Al-Taiar, A. Is age of menarche among school girls related to academic performance? Int. J. Adolesc. Med. Health 2017, 31, 164. [Google Scholar] [CrossRef] [PubMed]
- Al-Mathkoori, R.; Albatineh, A.; Al-Shatti, M.; Al-Taiar, A. Is age of menarche among school girls related to breastfeeding during infancy? Am. J. Hum. Biol. 2018, 30, e23122. [Google Scholar] [CrossRef]
- Rasmussen, K.M.; Felice, J.P.; O’Sullivan, E.J.; Garner, C.D.; Geraghty, S.R. The Meaning of “Breastfeeding” Is Changing and So Must Our Language About It. Breastfeed Med. 2017, 12, 510–514. [Google Scholar] [CrossRef] [PubMed]
- WHO. BMI Calssification. Available online: https://apps.who.int/bmi/index.jsp?introPage=intro_3.html (accessed on 24 September 2019).
- Zhang, J.; Kai, F.Y. What’s the Relative Risk? A Method of Correcting the Odds Ratio in Cohort Studies of Common Outcomes. JAMA 1998, 280, 1690–1691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farrag, N.S.; Cheskin, L.J.; Farag, M.K. A systematic review of childhood obesity in the Middle East and North Africa (MENA) region: Prevalence and risk factors meta-analysis. Adv. Pediatr. Res. 2017, 4, 8. [Google Scholar] [CrossRef] [Green Version]
- Al-Thani, M.; Al-Thani, A.; Alyafei, S.; Al-Chetachi, W.; Khalifa, S.E.; Ahmed, A.; Ahmad, A.; Vinodson, B.; Akram, H. The prevalence and characteristics of overweight and obesity among students in Qatar. Public Health 2018, 160, 143–149. [Google Scholar] [CrossRef]
- Ng, S.W.; Zaghloul, S.; Ali, H.; Harrison, G.; Yeatts, K.; El Sadig, M.; Popkin, B.M. Nutrition transition in the United Arab Emirates. Eur. J. Clin. Nutr. 2011, 65, 1328–1337. [Google Scholar] [CrossRef] [Green Version]
- Al-Qaoud, N.; Prakash, P. Breastfeeding and obesity among Kuwaiti preschool children. Med. Princ. Pract. Int. J. Kuwait Univ. Health Sci. Cent. 2009, 18, 111–117. [Google Scholar] [CrossRef]
- Huang, J.; Zhang, Z.; Wu, Y.; Wang, Y.; Wang, J.; Zhou, L.; Ni, Z.; Hao, L.; Yang, N.; Yang, X. Early feeding of larger volumes of formula milk is associated with greater body weight or overweight in later infancy. Nutr. J. 2018, 17, 12. [Google Scholar] [CrossRef] [Green Version]
- Oddy, W.H.; Mori, T.A.; Huang, R.C.; Marsh, J.A.; Pennell, C.E.; Chivers, P.T.; Hands, B.P.; Jacoby, P.; Rzehak, P.; Koletzko, B.V.; et al. Early infant feeding and adiposity risk: From infancy to adulthood. Ann. Nutr. Metab. 2014, 64, 262–270. [Google Scholar] [CrossRef] [Green Version]
- Huh, S.Y.; Rifas-Shiman, S.L.; Taveras, E.M.; Oken, E.; Gillman, M.W. Timing of solid food introduction and risk of obesity in preschool-aged children. Pediatrics 2011, 127, e544–e551. [Google Scholar] [CrossRef] [PubMed]
- Pearce, J.; Taylor, M.A.; Langley-Evans, S.C. Timing of the introduction of complementary feeding and risk of childhood obesity: A systematic review. Int. J. Obes. 2013, 37, 1295–1306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tahir, M.J.; Michels, K.B.; Willett, W.C.; Forman, M.R. Age at Introduction of Solid Food and Obesity Throughout the Life Course. Obesity 2018, 26, 1611–1618. [Google Scholar] [CrossRef] [Green Version]
- Pearce, J.; Langley-Evans, S.C. The types of food introduced during complementary feeding and risk of childhood obesity: A systematic review. Int. J. Obes. 2013, 37, 477–485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vadiveloo, M.; Tovar, A.; Ostbye, T.; Benjamin-Neelon, S.E. Associations between timing and quality of solid food introduction with infant weight-for-length z-scores at 12 months: Findings from the Nurture cohort. Appetite 2019, 141, 104299. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Characteristics | Public (n = 603) | Private (n = 172) | Total (N = 775) | |||
|---|---|---|---|---|---|---|
| n | (%) | n | (%) | N | (%) | |
| Age in Years, Mean (SD) | 16.74 | (1.09) | 16.62 | (1.21) | 16.72 | (1.12) |
| Nationality 1 | ||||||
| Kuwaiti | 572 | (95.33) | 21 | (12.21) | 593 | (76.81) |
| Non-Kuwaiti | 28 | (4.67) | 151 | (87.79) | 179 | (23.19) |
| Father’s Education 2 | ||||||
| No formal education | 4 | (0.72) | 6 | (3.77) | 10 | (1.40) |
| Primary/Intermediate | 60 | (10.81) | 27 | (16.98) | 87 | (12.18) |
| Secondary (high school) | 143 | (25.77) | 34 | (21.38) | 177 | (24.79) |
| Diploma | 81 | (14.59) | 15 | (9.43) | 96 | (13.45) |
| University & above | 267 | (48.11) | 77 | (48.43) | 344 | (48.18) |
| Mother’s Education 3 | ||||||
| No formal education | 23 | (3.97) | 14 | (8.48) | 37 | (4.97) |
| Primary/Intermediate | 74 | (12.76) | 36 | (21.82) | 110 | (14.77) |
| Secondary (high school) | 141 | (24.31) | 33 | (20.00) | 174 | (23.36) |
| Diploma | 81 | (13.97) | 15 | (9.09) | 96 | (12.89) |
| University & above | 261 | (45.00) | 67 | (40.61) | 328 | (44.03) |
| Currently residing with 4: | ||||||
| Both parents | 520 | (86.52) | 156 | (91.23) | 676 | (87.56) |
| Mother alone | 67 | (11.15) | 9 | (5.26) | 76 | (9.84) |
| Father alone | 5 | (0.83) | 2 | (1.17) | 7 | (0.91) |
| Other family members | 9 | (1.50) | 4 | (2.34) | 13 | (1.68) |
| BMI Characteristics | Public (n = 603) | Private (n = 172) | Total (N = 775) | |||
|---|---|---|---|---|---|---|
| n | (%) | n | (%) | N | (%) | |
| Underweight | 9 | (1.49) | 3 | (1.74) | 12 | (1.55) |
| Normal weight | 314 | (52.07) | 94 | (54.65) | 408 | (52.65) |
| Overweight | 144 | (23.88) | 39 | (22.67) | 183 | (23.61) |
| Obese | 136 | (22.55) | 36 | (20.93) | 172 | (22.19) |
| Total | 593 | (100.0) | 179 | (100.0) | 772 | (100.0) |
| Characteristics | Total | Prevalence of Overweight/Obesity | PR | [95%CI] | p a | |
|---|---|---|---|---|---|---|
| N | (%) | |||||
| Sociodemographic factors | ||||||
| Age in years | ||||||
| 14–16 | 258 | 127 | (49.22) | [Reference] | 0.048 | |
| >16–17 | 257 | 125 | (48.64) | 0.99 | [0.80–1.18] | |
| >17 | 260 | 103 | (39.62) | 0.79 | [0.62–0.98] | |
| Currently residing with: | ||||||
| Both parents | 676 | 320 | (47.34) | 1 | [Reference] | 0.017 |
| Not with both parents b | 96 | 33 | (34.38) | 0.73 | [0.53–0.91] | |
| ‘Mothers’ highest level of education | ||||||
| University & above | 328 | 158 | (48.17) | 1 | [Reference] | 0.037 |
| Diploma | 96 | 45 | (46.88) | 0.97 | [0.73–1.22] | |
| Secondary (high school) | 174 | 86 | (49.43) | 1.03 | [0.83–1.23] | |
| Primary or intermediate school | 110 | 41 | (37.27) | 0.76 | [0.56–0.99] | |
| No formal education | 37 | 10 | (27.03) | 0.55 | [0.30–0.91] | |
| Age of menarche in years | ||||||
| 7–<12 years | 201 | 111 | (55.22) | 1 | [Reference] | 0.003 |
| 12–<13 years | 209 | 95 | (45.45) | 0.80 | [0.61–0.99] | |
| ≥13 years | 231 | 90 | (38.96) | 0.67 | [0.50–0.86] | |
| Number of children the mother has | ||||||
| 1–3 children | 83 | 43 | (51.81) | 1 | [Reference] | 0.003 |
| 4–5 children | 198 | 106 | (53.54) | 1.04 | [0.75–1.35] | |
| 6 children or more | 214 | 81 | (37.85) | 0.69 | [0.47–0.97] | |
| Nutritional habits | ||||||
| Weekly consumption of soft drinks | ||||||
| ≤3 times per week | 490 | 239 | (48.78) | 1 | [Reference] | 0.026 |
| >3 times per week | 277 | 112 | (40.43) | 0.83 | [0.69–0.98] | |
| Weekly consumption of fruits | ||||||
| ≤3 times per week | 509 | 215 | (42.24) | 1 | [Reference] | 0.008 |
| >3 times per week | 262 | 137 | (52.29) | 1.24 | [1.06–1.41] | |
| Weekly consumption of dairy products | ||||||
| ≤3 times per week | 341 | 130 | (38.12) | 1 | [Reference] | <0.001 |
| >3 times per week | 429 | 221 | (51.52) | 1.35 | [1.16–1.54] | |
| Weekly consumption of fries | ||||||
| ≤3 times per week | 490 | 239 | (48.78) | 1 | [Reference] | 0.026 |
| >3 times per week | 284 | 115 | (40.49) | 0.83 | [0.69–0.80] | |
| Characteristics | Total | Prevalence of Overweight/Obesity | Model I | Model II | |||||
|---|---|---|---|---|---|---|---|---|---|
| PR | [95%CI] | p a | PR | [95%CI] | p b | ||||
| N | (%) | ||||||||
| Have you ever breastfed your daughter? | |||||||||
| Yes | 476 | 220 | (46.22) | 1 | [Reference] | 0.214 | 1 | [Reference] | 0.813 |
| No | 18 | 11 | (61.11) | 1.32 | [0.81–1.74] | 1.07 | [0.52–1.65] | ||
| Type of ‘infants’ feeding in the first 4 months | |||||||||
| Breastfeeding only | 150 | 63 | (42.00) | 1 | [Reference] | 0.293 | 1 | [Reference] | 0.589 |
| Breastfeeding & formula milk | 313 | 151 | (48.24) | 1.14 | [0.92–1.36] | 1.14 | [0.85–1.42] | ||
| No Breastfeeding | 31 | 17 | (54.84) | 1.29 | [0.86–1.68] | 1.20 | [0.68–1.68] | ||
| The duration of breastfeeding exclusive/mixed feeding (>6 months) | |||||||||
| ≤6 months | 425 | 200 | (47.06) | 1 | [Reference] | 0.954 | 1 | [Reference] | 0.410 |
| >6 months | 59 | 28 | (47.46) | 1.01 | [0.73–1.29] | 0.84 | [0.52–1.22] | ||
| The duration of breastfeeding exclusive/mixed feeding (>4 months) | |||||||||
| ≤4 months of age | 330 | 158 | (47.88) | 1 | [Reference] | 0.619 | 1 | [Reference] | 0.381 |
| >4 months | 154 | 70 | (45.45) | 0.95 | [0.76–1.15] | 0.88 | [0.64–1.15] | ||
| Have you ever fed your daughter with formula milk? | |||||||||
| Yes | 425 | 202 | (47.53) | 1 | [Reference] | 0.410 | 1 | [Reference] | 0.758 |
| No | 71 | 30 | (42.25) | 0.89 | [0.64–1.15] | 1.06 | [0.70–1.43] | ||
| Age of introducing formula milk (in months) ^ | |||||||||
| ≤4 months of age | 335 | 163 | (48.66) | 1 | [Reference] | 0.702 | 1 | [Reference] | 0.214 |
| >4 months | 63 | 29 | (46.03) | 0.95 | [0.68–1.22] | 0.77 | [0.46–1.14] | ||
| Age of introducing solid food (≤4 vs. >4 months) | |||||||||
| ≤4 months of age | 147 | 70 | (47.62) | 1 | [Reference] | 0.948 | 1 | [Reference] | 0.643 |
| >4 months | 270 | 127 | (47.04) | 0.99 | [0.78–1.20] | 0.97 | [0.72–1.24] | ||
| ‘Don’t remember | 67 | 33 | (49.25) | 1.03 | [0.74–1.33] | 1.15 | [0.77–1.50] | ||
| Age of introducing solid food (≤6 vs. >6 months) | |||||||||
| ≤6 months of age | 354 | 157 | (44.35) | 1 | [Reference] | 0.019 | 1 | [Reference] | <0.001 |
| >6 months | 63 | 40 | (63.49) | 1.42 | [1.13–1.68] | 1.77 | [1.39–2.03] | ||
| ‘Don’t remember | 67 | 33 | (49.25) | 1.11 | [0.83–1.39] | 1.31 | [0.91–1.67] | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sharaf-Alddin, R.; Almathkoori, R.; Kostakis, H.; Albatineh, A.N.; Al-Taiar, A.; Akpinar-Elci, M. Obesity during Adolescence and Feeding Practices during Infancy: Cross-Sectional Study. Epidemiologia 2023, 4, 106-116. https://doi.org/10.3390/epidemiologia4010011
Sharaf-Alddin R, Almathkoori R, Kostakis H, Albatineh AN, Al-Taiar A, Akpinar-Elci M. Obesity during Adolescence and Feeding Practices during Infancy: Cross-Sectional Study. Epidemiologia. 2023; 4(1):106-116. https://doi.org/10.3390/epidemiologia4010011
Chicago/Turabian StyleSharaf-Alddin, Reem, Radhia Almathkoori, Hara Kostakis, Ahmed N. Albatineh, Abdullah Al-Taiar, and Muge Akpinar-Elci. 2023. "Obesity during Adolescence and Feeding Practices during Infancy: Cross-Sectional Study" Epidemiologia 4, no. 1: 106-116. https://doi.org/10.3390/epidemiologia4010011
APA StyleSharaf-Alddin, R., Almathkoori, R., Kostakis, H., Albatineh, A. N., Al-Taiar, A., & Akpinar-Elci, M. (2023). Obesity during Adolescence and Feeding Practices during Infancy: Cross-Sectional Study. Epidemiologia, 4(1), 106-116. https://doi.org/10.3390/epidemiologia4010011