1. Introduction
Unless diagnosed and treated promptly, bone and joint infections in children are devastating and even fatal diseases that especially in resource-poor settings cause serious and long-lasting sequelae [
1]. In children, osteomyelitis (OM) and septic arthritis (SA) are most often hematogenous [
2]. Common causative agents in tropical regions include
S.aureus, respiratory pathogens, and Salmonella s.p.p. [
2,
3]. The prognosis is generally favorable in acute cases if the antibiotic treatment is started promptly [
1]. Potential sequelae include chronic osteomyelitis, pathological fracture, sequestra, and growth disturbance [
1,
2].
The global disease burden of sickle cell disease (SCD) is highest in sub-Saharan Africa. The birth prevalence of SCD is 1125 per 100,000 compared with 43 per 100,000 in Europe [
4,
5]. Children with SCD are prone to osteomyelitis [
1,
2]. A special problem is to distinguish osteomyelitis from a vaso-occlusive crisis [
6,
7]. Bone and joint infections are the most common musculoskeletal complication in children under 10 years old with SCD, surpassed in adolescence only by malleolar ulcers [
8]. SCD patients with hematogenous bone or joint infection are traditionally deemed to require surgery more frequently and are believed to experience complications such as epiphysiodesis or joint destruction more often than patients without SCD. Few trials have studied the efficacy and safety of antibiotic treatment among patients with SCD [
9]. Besides bone and joint infections, patients with SCD suffer from osteonecrosis and bone infarction [
10]. Bone infarction among SCD patients is significantly more common that osteomyelitis, which only covers 1–2% of musculoskeletal complaints of SCD patients [
11]. Unfortunately, the differential diagnosis between osteomyelitis and bone infarction in SCD is challenging [
10,
11].
Distinguishing osteomyelitis from bone infarction in patients with SCD is a challenge even for a multidisciplinary team of pediatric infectious disease specialists, hematologists, and orthopedic surgeons. Body temperature (>38°/100.4°F for infection and <38°/100.4°F for infarction), leukocytosis, and C-reactive protein levels may be used in the differential diagnosis. Fever is rare in infarction, but mildly elevated inflammatory markers may cause confusion [
10]. X-rays are often normal. Bone scan and MRI are specific [
10,
12], but poor availability limits their use in resource-poor settings. Pain at multiple sites has been thought to be more characteristic of bone infarction than osteomyelitis.
The treatment of bone infarction in patients with SCD is supportive with hydration and analgesics whereas prompt antibiotic management and possibly invasive procedures are required in osteomyelitis. Every effort should be undertaken in the differential diagnosis. Knowledge of the pattern of disease of osteomyelitis is useful in this respect, but still very few publications have reported the characteristics of osteomyelitis in resource- poor settings.
The aim of this study is to characterize the features of osteomyelitis in Luanda, Angola, with special emphasis on the special challenges that the clinicians face in a sub-Saharan African setting, such as severe cases of osteomyelitis in patients without SCD, osteomyelitis in SCD patients, and difficulties in distinguishing osteomyelitis from vaso-occlusive crisis or osteonecrosis in patients with SCD.
2. Materials and Methods
In this retrospective chart review, the case records of all patients at age 0 to 15 years admitted to the Department of Surgery in David Bernandino Children´s Hospital, Luanda, Angola were systematically searched from January 1st to December 31st 2014 to identify patients diagnosed with bone and joint infections (the main disease entity was osteomyelitis or septic arthritis). We collected demographic, laboratory, and radiographic data regarding the treatment and outcome. No universal screening for SCD could be applied during this period. Only if sickle-cell anemia was suspected by the attending clinician was hemoglobin electrophoresis used to identify cases of sickle-cell anemia. A total of 45 bone and joint infections (the main disease entity was osteomyelitis in 40 cases and septic arthritis in 5 cases) were identified. Of the patients, 26 (58%) were males and 19 (42%) females. The mean and median age was 6 years and the age of patients included in the study varied from 1 month to 13 years. Median age of patients with and without sickle-cell disease were 6 years (range 1 month to 13 years) and 3 years (range 1 year to 13 years) Malnutrition was defined as weight for age z-score < 2. Children with and without SCD were compared to identify potential difference in clinical findings, blood analysis, duration of fever, number of surgical procedures, and prognosis. Skin traction was used in small children, and skeletal traction was used in older children and adolescents. Statview® (version 5.0.1., Abacus Corporation, Baltimore, MD, USA) was used in the data analysis. An unpaired T-test was used to calculate p-values and p < 0.05 was considered significant. We were not able to perform preset follow-up for the patients, so the data analysis consists of inpatient data.
3. Results
Some cases were multifocal; in all, 61 bones and joints were involved. Mean and median duration of illness (identified in 31/45 patients) were 39 and 14 days, respectively (range 7 days to 1 year). No patient went to the hospital in under 7 days from the onset of symptoms and signs. Of them, 42% (19/45) presented within 2 weeks. A total of 13% (6/45) of the patients were malnourished.
Of them, 7% (3/45) of the patients arrived to hospital with an altered level of consciousness, and 18% (8/45) were dyspneic. None of the patients had convulsions on admission. The rough assessment of the attending clinician regarding the general condition was that it was poor in 13% (6/45). Three patients (6%) had edema at the ward. Median (interquartile range, IQR) blood hemoglobin, erythrocyte sedimentation rate (ESR), and white blood cell count (WBC) were 5.7 g/dL (5.0), 115 mm/h (61), and 15,400/mm3 (10,600), respectively. A total of 87% (39/45) of the patients had changes in X-ray. Potential discharge from the focus was cultured in only five cases, the yield being 2 cases of Staphylococcus aureus and isolated cases of Klebsiella, Enterobacter, and Citrobacter spp. A total of 25 patients were tested for HIV, but all had negative serology.
A total of 71% (30/42) of patients were febrile and in 54% (20/37) of patients the fever lasted longer than one week. Blood transfusion and supplemental oxygen were given to 38% (17/45) and to 18% (8/45) of patients. A pathologic fracture developed in 31% (14/45) of the patients, of whom 64% (29/45) underwent surgery, traction being used in 4 cases (9%). Median (IQR) duration of antibiotics was 28 days (40). Antimalarials were given to 6 children (13%). Median length of stay in hospital was 31 days (IQR 47).
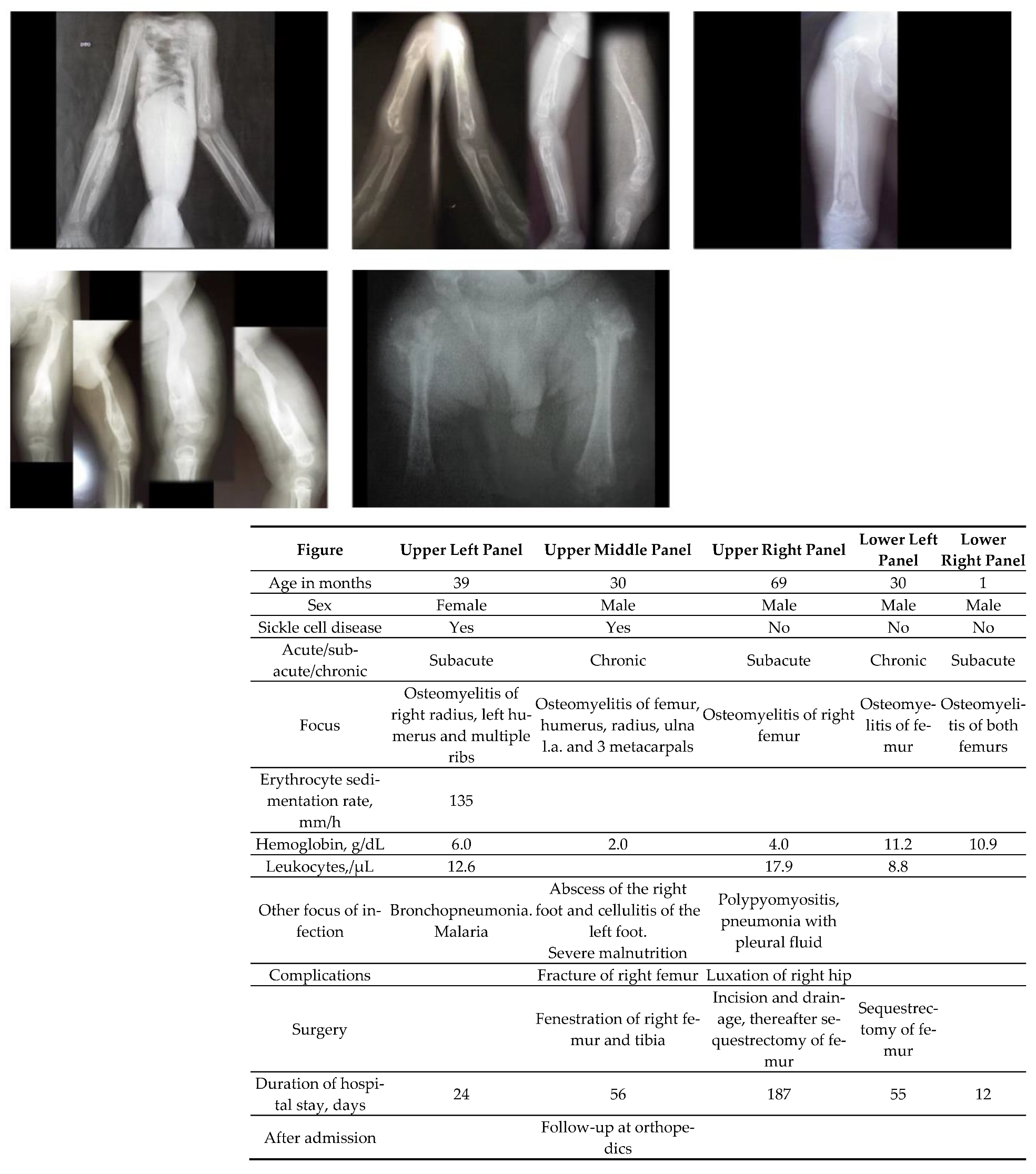
Figure 1 shows severe osteomyelitis in 5 children.
SCD was screened in 60% (27/45) of patients and the disease was found in 85% of the screened patients (23 patients). A comparison of the SCD patients versus those without SCD found is given in
Table 1. There was no significant difference between groups, except that the patients with SCD presented with significantly lower hemoglobin (
p < 0.05), and significantly more likely required blood transfusion (
p < 0.05). Furthermore, 74% (14/19) of the children who attended with a history of less than 2 weeks had SCD.
4. Discussion
This report highlights the severity of bone and joint infections in children in a sub-Saharan setting. Recent studies have shown that acute osteomyelitis in previously healthy non-neonatal children in a high-income setting can be treated with a short antibiotic treatment (a total course of 3 weeks in osteomyelitis, 2 weeks in septic arthritis) [
13,
14]. The recovery is fastest if the patient presents within 5 days of the onset of symptoms, this window obviously being the “golden period” of the treatment of osteomyelitis [
14]. Unfortunately, none of the patients in this series presented within 7 days from the disease onset, and we assume that at least in part because of this reason, the recovery was rather slow, as over 80% of patients were still febrile after one week of treatment.
Empirical antibiotic treatment is commonly given to children with SCD suffering from bone pain of unknown cause [
15]. Understanding the pattern of symptoms in osteomyelitis may help to better target the treatment. The clinical features and findings used to differentiate osteomyelitis from a vaso-occlusive crisis in SCD patients are fever (> 38.0°C) and pain in a single area in the diaphysis of a long bone [
16]. In our series, fever was present in 8–9 out of 10 patients. Multiple bone involvement was however not that uncommon a finding, as seen in
Figure 1.
Patients with SCD probably presented with low hemoglobin and thus needed blood transfusion more often. In patients with major sickling hemoglobinopathies, Salmonella is the most common pathogen, causing osteoarticular infections in the USA and Europe, whereas
S.aureus is the leading pathogen in sub-Saharan Africa and the Middle East [
17]. However, the prevalence of different pathogens and their sensitivity pattern to antibiotics are not well known in sub-Saharan Africa. Our study did not much illuminate this problem, as only 5 cases were appropriately analyzed bacteriologically. Moreover, without bacterial cultures an aseptic osteonecrosis may be mistaken for an active infection, and this was a clear limitation when interpreting the results. Because of this we have started using PCR technique for the bone and joint samples. We also have used this method to identify the agents causing bacterial meningitis from cerebrospinal fluid impregnated in the filter paper strips which were mailed to Finland for bacteriology [
18].
If acute osteomyelitis is treated early, fractures are extremely rare, because they usually associate with delayed diagnosis or resistant pathogens, such as methicillin-resistant
S. aureus [
1,
18]. Approximately one third of our patients had a fracture, and in other settings in Africa pathological fractures are also known to be commonly found in chronic osteomyelitis [
19].
Our study has limitations. PCR was not used to identify the causative agent. The analysis was retrospective, and the diagnostic criteria for osteomyelitis and septic arthritis could not be pinpointed; we had to rely on the clinical symptoms, laboratory analysis, and X-rays. Our study compared children from a diverse age range that differ significantly in terms of bone structure and stage of cognitive development. The pathogenesis of osteomyelitis changes as the prevalence of hematogenous etiology declines after growth plate closure [
1]. Thus, we chose to include all under 15-year-olds, realizing the developmental diversity of this group.
The patients already had a long duration of illness on admission. This reflects the reality in a sub-Saharan Africa with a significant delay in patient presentation. Moreover, the duration of symptoms was recorded as reported by the parents, which may lead to underestimation. All patients were not systematically evaluated for sickle cell disease, but targeted diagnostic assessment such as electrophoresis was available if hemoglobinopathy was suspected. Systematic screening for SCD might have increased detection, so the prevalence of SCD reported in this series should be considered as the lower margin. Unfortunately, we were not able to arrange a prescheduled follow-up. Thus, we are unable to formulate guidelines regarding the optimal diagnostic method or treatment.
In conclusion, we noted that in a significant minority of osteomyelitis, there is absence of fever or multifocal symptoms, making the differential diagnosis of osteomyelitis and bone infarction in patients with SCD difficult. It is unsurprising that a large proportion of patients suffering from SCD require blood transfusion during hospitalization, as patients with SCD present with low hemoglobin. Treatment guidelines cannot be formulated due to the lack of routine long-term follow-up. More research regarding the diagnosis and treatment of osteomyelitis in resource-scarce settings is urgently needed.
Author Contributions
Conceptualization, M.P., T.P. (Tuula Pelkonen), G.J., L.B.; T.P. (Tiina Pöyhiä), I.R. and H.P.; investigation, T.P. (Tuula Pelkonen); writing—original draft preparation, writing and editing, M.P.; project administration, T.P. (Tuula Pelkonen), G.J., L.B., T.P. (Tiina Pöyhiä), I.R., H.P. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the Foundation for Pediatric Research, Finland.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board of David Bernandino Children´s Hospital, Luanda.
Informed Consent Statement
Informed consent was obtained from subjects involved in the study.
Acknowledgments
Open access funding provided by University of Helsinki.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Peltola, H.; Pääkkönen, M. Acute osteomyelitis in children. N. Engl. J. Med. 2014, 370, 352–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pääkkönen, M.; Peltola, H. Bone and joint infections. Pediatr. Clin. N. Am. 2013, 60, 425–436. [Google Scholar] [CrossRef] [PubMed]
- Alsaif, M.A.; Abdulbaqi, M.; Noaim, K.A.; Aghbari, M.; Al Abdulqader, M.; Robinson, J. Prevalence of serious bacterial infections in children with sickle cell disease at King Abdulaziz Hospital, Al Ahsa. Mediterr. J. Hematol. Infect. Dis. 2021, 13, e2021002. [Google Scholar] [CrossRef] [PubMed]
- GBD 2015 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence and years lived with disability for 310 diseases and injuries, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1545–1602. [Google Scholar] [CrossRef] [Green Version]
- Wastnedge, E.; Waters, D.; Patel, S.; Morrison, K.; Goh, M.Y.; Adeloye, D.; Rudan, I. The global burden of sickle cell disease in children under five years of age: A systematic review and meta-analysis. J. Glob. Health 2018, 8, 021103. [Google Scholar] [CrossRef] [PubMed]
- Ambe, J.P.; Mava, Y.; Chama, R.; Farouq, G.; Machoko, Y. Clinical features of sickle cell anaemia in northern Nigerian children. West Afr. J. Med. 2012, 31, 81–85. [Google Scholar] [PubMed]
- Berger, E.; Saunders, N.; Wnag, L.; Friedman, J.N. Sickle cell disease in children: Differentiating osteomyelitis from vaso-occlusive crisis. Arch. Pediatr. Adolesc. Med. 2009, 163, 251–255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Onyemaechi, N.O.; Enweani, U.N.; Maduka, C.O. Musculoskeletal complications of sickle cell disease in Enugu, Nigeria. Niger. J. Med. 2011, 20, 456–461. [Google Scholar] [PubMed]
- Martí-Carvajal, A.J.; Agreda-Pérez, L.H. Antibiotics for treating osteomyelitis in people with sickle cell disease. Cochrane Database Syst. Rev. 2012, 12, CD007175. [Google Scholar] [PubMed]
- Vanderhave, K.L.; Perkins, C.A.; Scannel, B.; Brighton, B.K. Orthopaedic manifestations of sickle cell disease. J. Am. Acad. Orthop. Surg. 2018, 26, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Dalton, G.P.; Drummond, D.S.; Davidson, R.S.; Robertson, W.W., Jr. Bone infraction versus infection in sickle cell disease in children. J. Pediatr. Orthop. 1996, 16, 540–544. [Google Scholar] [CrossRef] [PubMed]
- Kao, C.M.; Yee, M.E.; Maillis, A.; Lai, K.; Bakshi, N.; Rostad, B.S.; Jerris, R.C.; Lane, P.A.; Yildirim, I. Microbiology and radiographic features of osteomyelitis in children and adolescents with sickle cell disease. Pediatr. Blood Cancer 2020, 67, e28517. [Google Scholar] [CrossRef] [PubMed]
- Peltola, H.; Pääkkönen, M.; Kallio, P.; Kallio, M.J. Prospective, randomized trial of 10 versus 30 days of antimicrobial treatment, including a short-term course of parenteral therapy, for childhood septic arthritis. Clin. Infect. Dis. 2009, 48, 1201–1210. [Google Scholar] [CrossRef] [PubMed]
- Peltola, H.; Pääkkönen, M.; Kallio, P.; Kallio, M.J. Short- versus long term antimicrobial treatment for acute hematogenous osteomyelitis of childhood: Prospective, randomized trial on 131 culture-positive cases. Pediatr. Infect. Dis. J. 2010, 29, 1123–1128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fontalis, A.; Hughes, K.; Nguyen, M.P.; Williamson, M.; Yeo, A.; Lui, D.; Gelfer, Y. The challenge of differentiation vaso-occlusive crises from osteomyelitis in children with sickle cell disease and bone pain: A 15-year retrospective review. J. Child Orthop. 2019, 13, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Af Farii, H.; Zhou, S.; Albers, A. Management of osteomyelitis in sickle cell disease: Review article. J. Am. Acad. Orthop. Surg. Glob. Res. Rev. 2020, 4, e2000002-10. [Google Scholar] [CrossRef] [PubMed]
- Thanni, L.O. Bacterial osteomyelitis in major sickling haemonoglobinopathies: Geographic difference in pathogen prevalence. Afr. Health Sci. 2006, 6, 236–239. [Google Scholar] [PubMed]
- Peltola, H.; Roine, I.; Leinonen, M.; Kuisma, L.; Mata, A.; Arbo, A.; Goyo, J.; Saukkoriipi, A. Diagnosis of Streptococcus pneumoniae and Haemophilus influenzae type b meningitis by identifying DNA from cerebrospinal fluid-impregnated filter paper strips. Pediatr. Infect. Dis. J. 2010, 29, 111–114. [Google Scholar] [CrossRef] [Green Version]
- Akinyoola, A.L.; Orimolade, E.A.; Yusuf, M.G. Pathologic fractures of long bones in Nigerian children. J. Child Orthop. 2008, 2, 475–479. [Google Scholar] [CrossRef] [Green Version]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 

{kind=link}