1. Introduction
Worldwide cervical cancer is the fourth most common cancer and is also the fourth leading cause of death among women, after breast cancer, colorectal cancer, and lung cancer [
1].
Laparoscopy is today the gold standard treatment for cervical cancer. Many randomized studies have recently shown that laparoscopic treatment is related to better preoperative outcomes and a better quality of life than open surgery, without any effects on patient safety [
2,
3,
4]. Meta-analyses comparing retrospective data on radical laparoscopic hysterectomy and open technique did not show differences in oncological and survival outcomes (disease-free survival 85–95%; overall survival 93–97%), with better postoperative outcomes [
5,
6,
7].
For this reason, laparoscopic surgery for the treatment of cervical cancer has been defined in the main guidelines, NCCN [
8] and ESGO [
9], as a better choice than open surgery. However, the role of the uterine manipulator in laparoscopic uterine surgery is still controversial. Most surgeons state that using a manipulator in laparoscopic hysterectomy allows a better dissection of the spaces and, therefore, a faster and safer procedure [
10]. However, doubts arise about the spreading of malignant cells by use of uterine manipulator, especially on the vaginal apex and peritoneum [
11].
In the main trial [
12] on the laparoscopic treatment of cervical cancer performed in the last five years (LLAC study), minimally invasive radical hysterectomy was associated with lower rates of disease-free survival and overall survival than open abdominal radical hysterectomy among women with early stage cervical cancer. In this study, 319 patients with early cervical cancer with laparoscopic or robotic radical hysterectomy were treated, of which 27 had cancer recurrence or death (66% loco-regional recurrences with a median follow-up of 2.5 years). The study was terminated early by the safety monitoring committee due to the significant inferiority of the minimally invasive arm.
The unexpected results of the LLAC study have been discussed in many editorials, focusing on different aspects of radical hysterectomy such as the learning curve, the length of the vaginal border, the radicality of the parametric section, the ethnic differences, the extension of the lymphadenectomy, and the standardization of the surgical technique.
For this reason, the aim of this study is to investigate the long-term oncological safety of laparoscopic treatment without the use of a uterine manipulator for patients with early stage cervical cancer. It is a retrospective observational study where we want to evaluate if not using the uterine manipulator could avoid the spreading of malignant cells in the vaginal apex and peritoneum.
2. Materials and Methods
2.1. Study Design
This is a retrospective cohort study led by the Department of Obstetrics and Gynecology of ARNAS Garibaldi Nesima in Catania. For this study, patients affected by cervical cancer, treated in the period between 1 January 2014 and 31 December 2017, were considered.
The study is conformed to the standards contained in the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement, available through the Enhancing the Quality and Transparency of Health Research (EQUATOR) Network. In addition, all stages of the study respected the guidelines provided by the Helsinki Declaration. Each woman received appropriate counseling about the purpose of the research and the guarantee of anonymous treatment of personal data, according to Italian law guaranteeing privacy, and signed an informed consent form for data collection. The study was approved by Ethics Committee Catania 2 (N° Prot. 262/C.E) (Report n° 68/2020/CECT2).
2.2. Study Population
Women aged ≥18 years with surgical treatment for cervical cancer.
2.3. Methods
All women who were referred to the Gynecological Unit for surgical treatment of cervical cancer were clinically evaluated by a gynecological exam. The inclusion and exclusion criteria were described in
Table 1. Demographic data, past medical history, obstetrical history, and clinical data were collected. An ultrasound examination was performed before surgery. The patients were divided into two groups: treatment with and without an intra-uterine manipulator. Only two surgeons, with over ten years of experience in oncological surgery, treated the patients. After surgery, a careful follow-up was performed through gynecological examination and ultrasound evaluation every three months for the first two years, and then every six months for three years, for a total of five years, to investigate the long-term oncological safety of laparoscopic treatment, with or without the use of a uterine manipulator (Clermont–Ferrand model).
3. Results
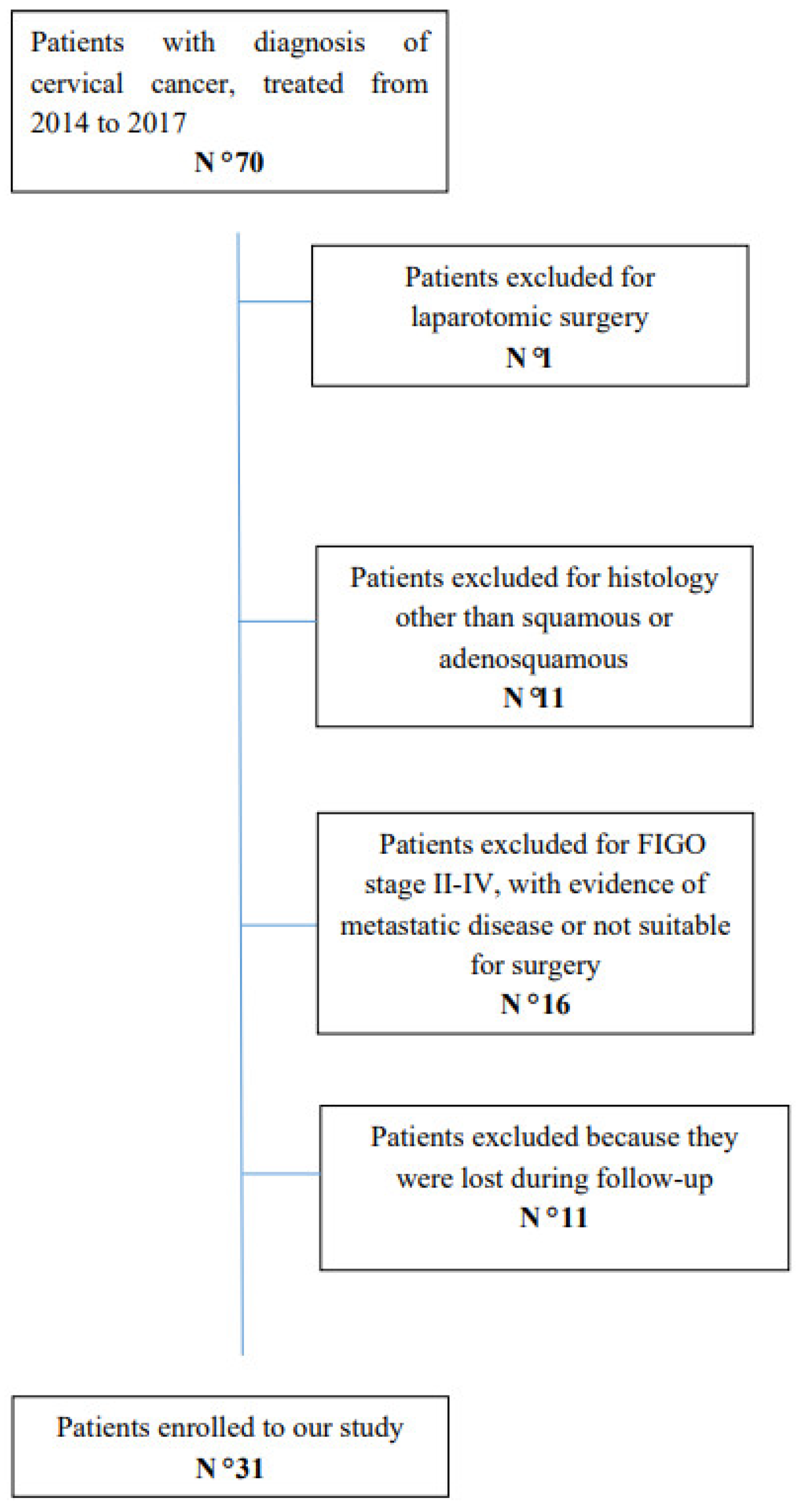
From 2014 to 2017, seventy women underwent surgery for the preoperative diagnosis of cervical cancer. Amongst these patients, eleven were excluded for different histology than squamous or adenosquamous carcinoma; fifteen patients were excluded for an advanced stage of pathology, FIGO stage II–IV, evidence of metastatic disease or not suitable for surgery. One woman was excluded because a laparotomic surgery was performed; finally, eleven patients were excluded because they were lost during follow-up. In the end, thirty-one patients with early stage cervical cancer, with a histological exam of squamous or adenosquamous carcinoma, were considered eligible for our study (
Figure 1).
Among the thirty-one patients enrolled, twelve women had cancer in situ (IA1), nineteen had an early stage cervical cancer, in particular two cases of cervical cancer stage IA2, ten cases of cervical cancer stage IB1, and seven cases of cervical cancer stage IB2, according to the FIGO classification. Among patients with cancer in situ, nine women underwent a radical hysterectomy type A according to Querleu–Morrow classification, two women a type B radical hysterectomy, and only one woman a type C radical hysterectomy. Among these patients, the uterine manipulator was used in only one case, and no recurrence occurred in five years. Among patients with early cervical cancer, two women underwent a radical hysterectomy type B according to Querleu–Morrow classification, fourteen women a type C1 radical hysterectomy, one woman a type C2, and two women underwent a fertility-sparing treatment for cervical cancer. Among these, the uterine manipulator was used in only two cases, and no recurrence occurred among these in five years. In two cases adjuvant chemotherapy was performed.
Finally, amongst thirty-one women treated for cervical cancer and enrolled in this study, at follow-up three cases of recurrence occurred, but the uterine manipulator was not used. The first patient had abdominal wall recurrence one year after treatment. She had a poorly differentiated squamous carcinoma, stage FIGO IB1, and was treated with C1 radical hysterectomy, according to Querleu–Morrow classification, with salpingectomy and pelvic lymphadenectomy one year before. The second patient had centro-pelvic recurrence one year after treatment. She had moderately differentiated squamous carcinoma, stage FIGO IB1, and was and was treated with C1 radical hysterectomy with salpingo-oophorectomy and pelvic lymphadenectomy one year before. The last patient had nodal recurrence two years after treatment. She had squamous carcinoma, stage FIGO IB1, and was treated with fertility-sparing surgery, B1 radical trachelectomy with left salpingo-oophorectomy and pelvic lymphadenectomy (
Table 2).
4. Discussion
The LLAC study is the leading study on laparoscopic treatment of cervical cancer. The unexpected results of this study, however, have raised many questions. On the one hand, laparoscopic treatment has a better postoperative outcome and a better quality of life for women than open surgery in a short-term period; on the other hand, according to this study, it could determine a higher risk of cancer recurrence or death. In agreement with the LLAC study, the systematic review and meta-analysis of observational studies by Nitecki et al. confirmed that women who underwent radical laparoscopic hysterectomy for early stage cervical cancer have an increased risk of recurrence and death in comparison to open surgery [
13].
As mentioned above, many editorials evaluated the different features of laparoscopic radical hysterectomy, which could determine so high recurrence rates, among these: the learning curve, the length of the vaginal border, the radicality of the parametric section, the ethnic differences, the extension of the lymphadenectomy, and the standardization of surgical technique.
In our study, we have considered the possible role of the uterine manipulator, considering if it could increase the recurrence rates. The uterine manipulator is an instrument widely used in laparoscopic hysterectomy that helps expose the anatomy during surgical procedures. It allows, in fact, a perpendicular dissection of the uterine arteries, through the lateralization of the uterus, increases the distance between the uterine cervix and the ureters, reducing the risk of ureter lesion, allows us to elevate the uterus, and allows us to delineate the vaginal fornices to facilitate the colpotomy, maintaining the pneumoperitoneum after the vaginal incision [
14]. The role of the uterine manipulator in gynecological malignancies may be controversial.
Nica et al. compared 115 women with early stage cervical cancer that had surgery with the use of an intrauterine manipulator and 109 women without it. They concluded that patients with low-risk features had good long-term oncology outcomes and that a significant predictor of disease recurrence is tumor size, through the dissemination of malignant cells during minimally invasive colpotomy [
15].
Yinxia Liu et al. investigated the relationship between LVSI and surgical approach in early stage cervical cancer. As mentioned above, in fact, the LLAC trial had a worldwide implication. Many hypotheses were advanced, one of which was the possibility that uterine manipulators may spread malignant cells through the LVSI. In particular, 735 patients with early stage cervical cancer were enrolled in this study. Among these, 375 underwent radical laparoscopic hysterectomy and pelvic lymphadenectomy, and 378 underwent open surgery. They concluded that uterine manipulators are not associated with LVSI in surgery for early stage of cervical cancer. Conversely, these could be related to lymph node metastasis and deep stromal invasion [
16].
The SUCCOR study, a retrospective study, in line with data described in the literature, showed a worse disease-free survival in women who underwent a minimally invasive treatment than open surgery. Avoiding the use of a uterine manipulator or closing the vagina over the tumor could improve these results [
17].
Appropriate counselling should be performed on all women, particularly elder women, to choose the best surgical option to treat a patient affected by a gynecological cancer [
18,
19,
20]. Some previous studies demonstrated that minimally invasive surgery (laparoscopy or robotics) was as adequate and effective as abdominal surgery in terms of surgical and oncological outcomes in the surgical treatment of early stage cervical cancer FIGO stage IB1 [
21,
22,
23].
Our study showed that the five-year rates of recurrence in patients treated with minimally invasive surgery are not low, about 10%, similar to the data in the literature [
13] and LLAC study [
12]. However, these recurrence rates do not seem to be related to the use of the intrauterine manipulator, confirming the results of the SUCCOR study [
17]. The strength of the work is represented by the fact that all the surgical operations were performed by only two surgeons and in the same hospital. However, we need to underline that our study has numerous limitations: it is a retrospective study, has a small number of cases, and the follow-up of the patients is only five years.
5. Conclusions
Our study demonstrated that the five-year rates of recurrence in patients treated with minimally invasive surgery are not low, about 10%, similar to the data in the literature [
13] and the LLAC study [
12]. The use of the intrauterine manipulator is not related to a higher level of recurrence rates, but further prospective studies will be needed to clarify the factors related to high relapse rates in minimally invasive cervical cancer treatment.
Author Contributions
Conceptualization, M.D and F.A.G.; methodology, C.E.; validation, G.E.; formal analysis, G.B.; investigation, F.C.; data curation, G.B.; writing—original draft preparation, F.A.G.; writing—review and editing, C.E.; visualization, M.D.; supervision, G.E.; project administration, G.E. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of Azienda di Rilievo Nazionale e di Alta Specializzazione (ARNAS) Garibaldi, Catania (N° Prot. 262/C.E approved on 11-05-2020) (Report n° 68/2020/CECT2).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data is contained within the article.
Acknowledgments
The authors acknowledge the mentorship provided by Giuseppe Ettore, Department of Obstetrics and Gynaecology, Azienda di Rilievo Nazionale e di Alta Specializzazione (ARNAS) Garibaldi, Catania, ITALY, throughout the preparation of this manuscript.
Conflicts of Interest
The authors declare that they have no conflict of interest.
References
- Arbyn, M.; Weiderpass, E.; Bruni, L.; de Sanjosé, S.; Saraiya, M.; Ferlay, J.; Bray, F. Estimates of incidence and mortality of cervical cancer in 2018: A worldwide analysis. Lancet Glob. Health 2020, 8, e191–e203. [Google Scholar] [CrossRef]
- Possover, M.; Krause, N.; Kühne-Heid, R.; Schneider, A. Laparoscopic assistance for extended radicality of radical vaginal hysterectomy: Description of a technique. Gynecol. Oncol. 1998, 70, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Boggess, J.F.; Gehrig, P.A.; Cantrell, L.; Shafer, A.; Ridgway, M.; Skinner, E.N.; Fowler, W.C. A case-control study of robot-assisted type III radical hysterectomy with pelvic lymph node dissection compared with open radical hysterectomy. Am. J. Obstet. Gynecol. 2008, 199, 357.e1–357.e7. [Google Scholar] [CrossRef] [PubMed]
- Canton-Romero, J.C.; Anaya-Prado, R.; Rodriguez-Garcia, H.A.; Mejia-Romo, F.; De-Los-Rios, P.E.; Cortez-Martinez, G.; Delgado-Ramirez, R.; Quijano, F. Laparoscopic radical hysterectomy with the use of a modified uterine manipulator for the management of stage IB1 cervix cancer. J. Obstet. Gynaecol. 2010, 30, 49–52. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.Z.; Deng, L.; Xu, H.C.; Zhang, Y.; Liang, Z.Q. Laparoscopy versus laparotomy for the management of early stage cervical cancer. BMC Cancer 2015, 15, 928. [Google Scholar] [CrossRef]
- Sert, B.M.; Boggess, J.F.; Ahmad, S.; Jackson, A.L.; Stavitzski, N.M.; Dahl, A.A.; Holloway, R.W. Robot-assisted versus open radical hysterectomy: A multi-institutional experience for early-stage cervical cancer. Eur. J. Surg. Oncol. 2016, 42, 513–522. [Google Scholar] [CrossRef]
- Shazly, S.A.; Murad, M.H.; Dowdy, S.C.; Gostout, B.S.; Famuyide, A.O. Robotic radical hysterectomy in early stage cervical cancer: A systematic review and meta-analysis. Gynecol. Oncol. 2015, 138, 457–471. [Google Scholar] [CrossRef] [PubMed]
- Reid, E.; Suneja, G.; Ambinder, R.F.; Ard, K.; Baiocchi, R.; Barta, S.K.; Carchman, E.; Cohen, A.; Gupta, N.; Johung, K.L.; et al. Cancer in People Living With HIV, Version 1.2018, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2018, 16, 986–1017. [Google Scholar] [CrossRef]
- Cibula, D.; Pötter, R.; Planchamp, F.; Avall-Lundqvist, E.; Fischerova, D.; Haie Meder, C.; Köhler, C.; Landoni, F.; Lax, S.; Lindegaard, J.C.; et al. The European Society of Gynaecological Oncology/European Society for Radiotherapy and Oncology/European Society of Pathology Guidelines for the Management of Patients With Cervical Cancer. Int. J. Gynecol. Cancer 2018, 28, 641–655. [Google Scholar] [CrossRef]
- Spirtos, N.M.; Eisenkop, S.M.; Schlaerth, J.B.; Ballon, S.C. Laparoscopic radical hysterectomy (type III) with aortic and pelvic lymphadenectomy in patients with stage I cervical cancer: Surgical morbidity and intermediate follow-up. Am. J. Obstet. Gynecol. 2002, 187, 340–348. [Google Scholar] [CrossRef]
- Krizova, A.; Clarke, B.A.; Bernardini, M.Q.; James, S.; Kalloger, S.E.; Boerner, S.L.; Mulligan, A.M. Histologic artifacts in abdominal, vaginal, laparoscopic, and robotic hysterectomy specimens: A blinded, retrospective review. Am. J. Surg. Pathol. 2011, 35, 115–126. [Google Scholar] [CrossRef]
- Ramirez, P.T.; Frumovitz, M.; Pareja, R.; Lopez, A.; Vieira, M.; Ribeiro, R.; Buda, A.; Yan, X.; Shuzhong, Y.; Chetty, N.; et al. Minimally Invasive versus Abdominal Radical Hysterectomy for Cervical Cancer. N. Engl. J. Med. 2018, 379, 1895–1904. [Google Scholar] [CrossRef]
- Nitecki, R.; Ramirez, P.T.; Frumovitz, M.; Krause, K.J.; Tergas, A.I.; Wright, J.D.; Rauh-Hain, J.A.; Melamed, A. Survival After Minimally Invasive vs Open Radical Hysterectomy for Early-Stage Cervical Cancer: A Systematic Review and Meta-analysis. JAMA Oncol. 2020, 6, 1019–1027. [Google Scholar] [CrossRef]
- van den Haak, L.; Alleblas, C.; Nieboer, T.E.; Rhemrev, J.P.; Jansen, F.W. Efficacy and safety of uterine manipulators in laparoscopic surgery: A review. Arch. Gynecol. Obstet. 2015, 292, 1003–1011. [Google Scholar] [CrossRef]
- Nica, A.; Kim, S.R.; Gien, L.T.; Covens, A.; Bernardini, M.Q.; Bouchard-Fortier, G.; Kupets, R.; May, T.; Vicus, D.; Laframboise, S.; et al. Survival after minimally invasive surgery in early cervical cancer: Is the intra-uterine manipulator to blame? Int. J. Gynecol. Cancer 2020, 30, 1864–1870. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Huang, S.; Ming, X.; Jing, H.; Li, Z. Surgical Approach and Use of Uterine Manipulator Are Not Associated with LVSI in Surgery for Early-stage Cervical Cancer. J. Minim. Invasive Gynecol. 2021, 28, 1573–1578. [Google Scholar] [CrossRef] [PubMed]
- Chiva, L.; Zanagnolo, V.; Querleu, D.; Martin-Calvo, N.; Arévalo-Serrano, J.; Căpîlna, M.E.; Fagotti, A.; Kucukmetin, A.; Mom, C.; Chakalova, G.; et al. SUCCOR study: An international European cohort observational study comparing minimally invasive surgery versus open abdominal radical hysterectomy in patients with stage IB1 cervical cancer. Int. J. Gynecol. Cancer 2020, 30, 1269–1277. [Google Scholar] [CrossRef]
- Genovese, F.; Siringo, S.; Tuscano, A.; Gulino, F.A.; Cannone, F.; Leanza, V.; Cosentino, F.; Palomba, S.; Palumbo, M.A. Understanding the limits of parametrial resection in radical hysterectomy: A randomized controlled trial. Prz. Menopauzalny 2022, 21, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Vitale, S.G.; Capriglione, S.; Zito, G.; Lopez, S.; Gulino, F.A.; Di Guardo, F.; Vitagliano, A.; Noventa, M.; La Rosa, V.L.; Sapia, F.; et al. Management of endometrial, ovarian and cervical cancer in the elderly: Current approach to a challenging condition. Arch. Gynecol. Obstet. 2019, 299, 299–315. [Google Scholar] [CrossRef] [PubMed]
- Vitale, S.G.; Valenti, G.; Gulino, F.A.; Cignini, P.; Biondi, A. Surgical treatment of high stage endometrial cancer: Current perspectives. Updates Surg. 2016, 68, 149–154. [Google Scholar] [CrossRef] [PubMed]
- D’Oria, O.; Corrado, G.; Laganà, A.S.; Chiantera, V.; Vizza, E.; Giannini, A. New Advances in Cervical Cancer: From Bench to Bedside. Int. J. Environ. Res. Public Health 2022, 19, 7094. [Google Scholar] [CrossRef] [PubMed]
- Ferrandina, G.; Corrado, G.; Scambia, G. Minimally invasive surgery and quality of life in cervical cancer. Lancet Oncol. 2020, 21, 746–748. [Google Scholar] [CrossRef]
- Corrado, G.; Vizza, E.; Legge, F.; Pedone Anchora, L.; Sperduti, I.; Fagotti, A.; Mancini, E.; Gallotta, V.; Zampa, A.; Chiofalo, B.; et al. Comparison of Different Surgical Approaches for Stage IB1 Cervical Cancer Patients: A Multi-institution Study and a Review of the Literature. Int. J. Gynecol. Cancer 2018, 28, 1020–1028. [Google Scholar] [CrossRef] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).



 ,
, 

{kind=link}