

Management of Large Subcardial Diverticula in Sleeve Gastrectomy: Technical Tips


 , and
, and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
1.1. Gastric Diverticula and Sleeve Gastrectomy
1.2. Technical Considerations
- −
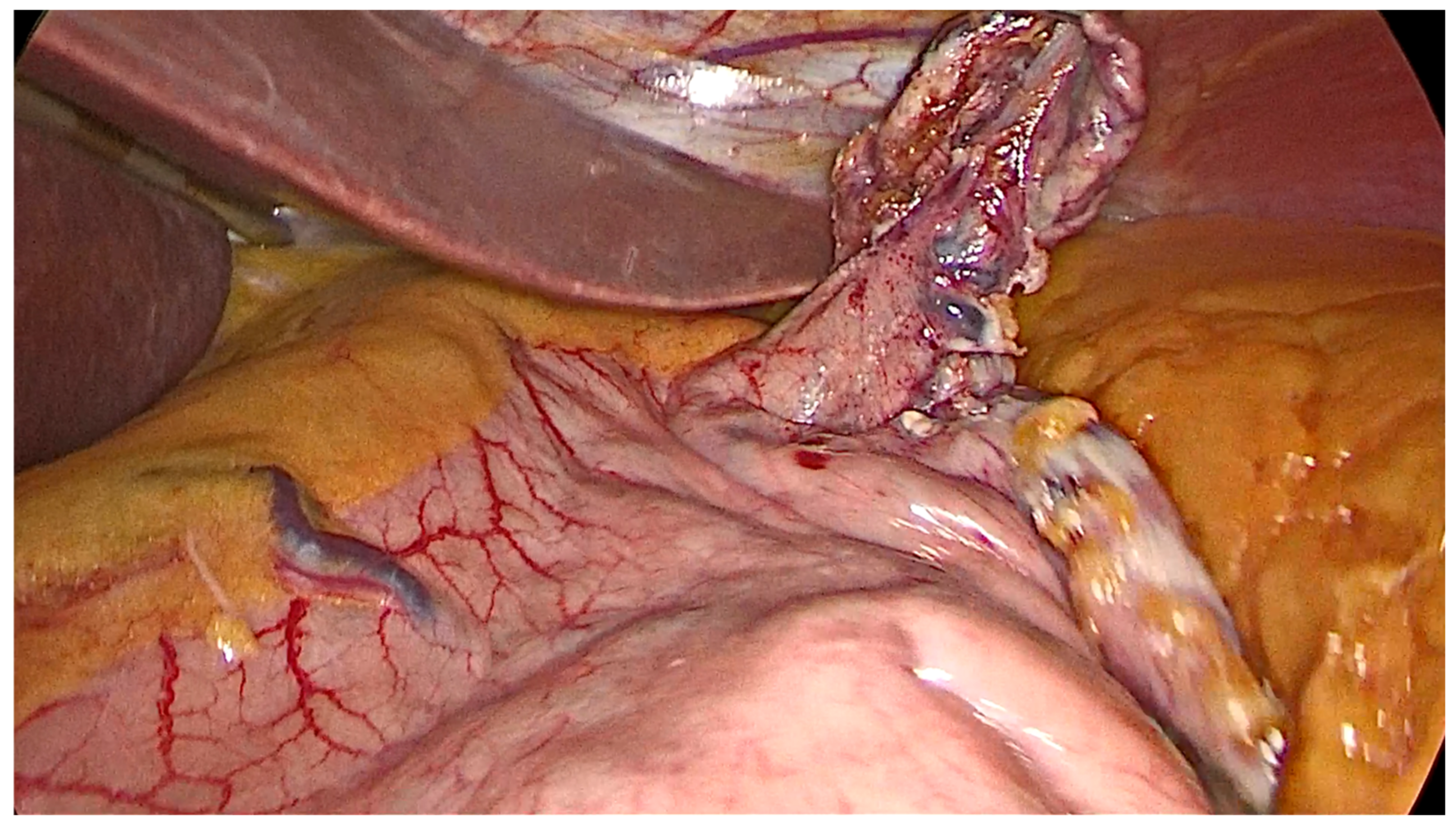
- Opening a window in the gastro-colic ligament using an energy device from the antrum and proceeding up to the angle of His, along the greater curvature, until the left diaphragmatic pillar was fully exposed.
- −
- The gastric fundus must be entirely mobilized with coagulation and section of the short gastric vessels and the opening of the gastro-splenic ligament.
- −
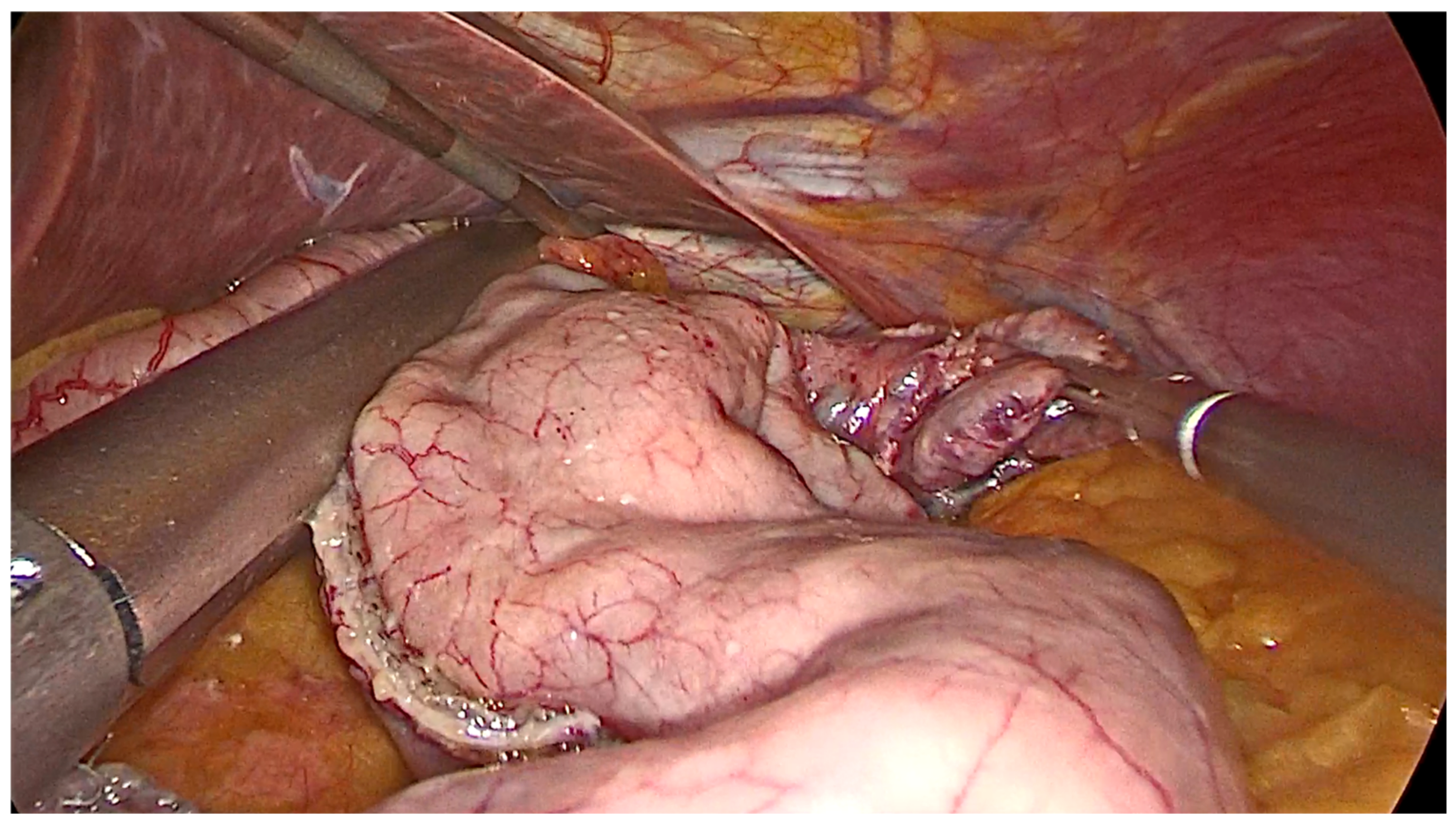
- After the transoral position of a bougie (of diameter ranging 36–40 Fr), sleeve gastrectomy is performed with the use of a stapler, beginning from the distance of 4–6 cm from the pylorus up to the angle of His.
- −
- Care must be taken in the first two uses of the stapler to prevent narrowing the gastric sleeve at the incisura.
- −
- Symmetric traction on the anterior and posterior stomach wall must be undertaken during stapling.
- −
- The staple line should be regular and straight from the antrum to the angle of His.
- −
- Each reload of the stapler must be calibrated based on the thickness of the gastric wall, as well documented in the work of Elariny et al. [13], providing the right compression and hemostasis of the tissue.
- −
- The staple line should stay at least 1 cm away from the esophago-gastric junction.
2. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rashid, F.; Aber, A.; Iftikhar, S.Y. A review on gastric diverticulum. World J. Emerg. Surg. 2012, 7, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palmer, E.D. Collective review: Gastric diverticulum. Int. Abstr. Surg. 1951, 92, 417–428. [Google Scholar] [PubMed]
- Gockel, I.; Thomschke, D.; Lorenz, D. Gastrointestinal: Gastric diverticula. J. Gastroenterol. Hepatol. 2004, 19, 227. [Google Scholar] [CrossRef] [PubMed]
- Cotea, E.; Vasilescu, A.; Dimiftoe, G. Gastric diverticula on the greater curvature. J. Chir. 2007, 3, 269–273. [Google Scholar]
- Marano, L.; Reda, G.; Porfidia, R.; Grassia, M.; Petrillo, M.; Esposito, G.; Torelli, F.; Cosenza, A.; Izzo, G.; Di Martino., N. Large symptomatic gastric diverticula: Two case reports and a brief review of literature. World J. Gastroenterol. 2013, 19, 6114–6117. [Google Scholar] [CrossRef] [PubMed]
- Donkervoort, S.C.; Baak, L.C.; Blaauwgeer, J.L. Laparoscopic resection of a symptomatic gastric diverticulum. JSLS J. Soc. Laparosc. Robot. Surg. 2006, 10, 525–527. [Google Scholar]
- Pietrzak, C.; Leya, J.; Abood, G.; Yonick, D.; Gupta, N. Recurrent intrabdominal abscess formation due to a gastric diverticulum. Endoscopy 2013, 45, E345–E346. [Google Scholar] [PubMed] [Green Version]
- Ho, M.F.; Teoh, A.Y.; Liu, S.Y.; Chiu, P.W.; Wong, S.K.; Ng, E.K.W. Perforated gastric diverticulum with bleeding. Endoscopy 2013, 45, E422–E423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castelli, A.A.; Lutfi, R.E. Strategies for diagnosing and managing gastric diverticulum in sleeve gastrectomy. Surg. Obes. Relat. Dis. 2019, 15, 126–127. [Google Scholar] [CrossRef] [PubMed]
- Wylie, L.E.; Villalvazo, Y.; Jensen, C. A Strong Approach to a Weak Gastric Wall in Bariatric Surgery: Concurrent Diverticulectomy and Sleeve Gastrectomy. Cureus 2020, 12, e6545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gagner, M.; Hutchinson, C.; Rosenthal, R. Fifth International Consensus Conference: Current status of sleeve gastrectomy. Surg. Obes. Relat. Dis. 2016, 12, 750–756. [Google Scholar] [CrossRef] [PubMed]
- Mahawar, K.K.; Omar, I.; Singhal, R.; Aggarwal, S.; Allouch, M.I.; Alsabah, S.K.; Angrisani, L.; Badiuddin, F.M.; Balibrea, J.M.; Bashir, A.; et al. The first modified Delphi consensus statement on sleeve gastrectomy. Surg. Endosc. 2021, 35, 7027–7033. [Google Scholar] [CrossRef] [PubMed]
- Elariny, H.; Gonzalez, H.; Wang, B. Tissue thickness of human stomach measured on excised gastric specimens from obese patients. Surg. Technol. Int. 2005, 14, 119–124. [Google Scholar] [PubMed]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frattini, F.; Pino, A.; Cordaro, G.; Lianos, G.; Bertoli, S.; Dionigi, G. Management of Large Subcardial Diverticula in Sleeve Gastrectomy: Technical Tips. Surgeries 2023, 4, 134-140. https://doi.org/10.3390/surgeries4010015
Frattini F, Pino A, Cordaro G, Lianos G, Bertoli S, Dionigi G. Management of Large Subcardial Diverticula in Sleeve Gastrectomy: Technical Tips. Surgeries. 2023; 4(1):134-140. https://doi.org/10.3390/surgeries4010015
Chicago/Turabian StyleFrattini, Francesco, Antonella Pino, Giuseppe Cordaro, Georgios Lianos, Simona Bertoli, and Gianlorenzo Dionigi. 2023. "Management of Large Subcardial Diverticula in Sleeve Gastrectomy: Technical Tips" Surgeries 4, no. 1: 134-140. https://doi.org/10.3390/surgeries4010015
APA StyleFrattini, F., Pino, A., Cordaro, G., Lianos, G., Bertoli, S., & Dionigi, G. (2023). Management of Large Subcardial Diverticula in Sleeve Gastrectomy: Technical Tips. Surgeries, 4(1), 134-140. https://doi.org/10.3390/surgeries4010015