
Implantation of a Vascular Access Button for Chronic Blood Sampling and Drug Administration in the Rabbit


Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals
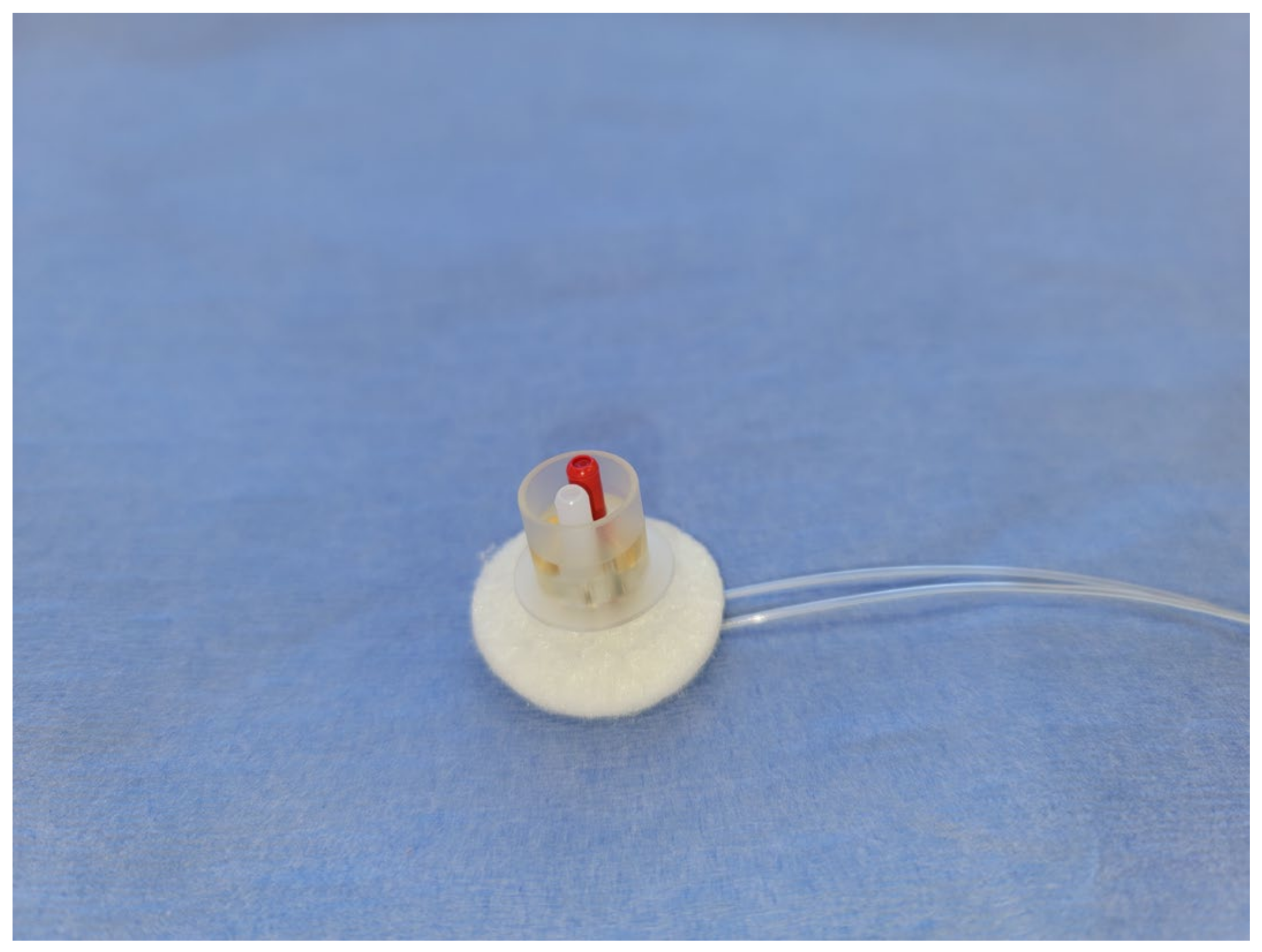
2.2. Implant
2.3. Pre-Operative Preparation
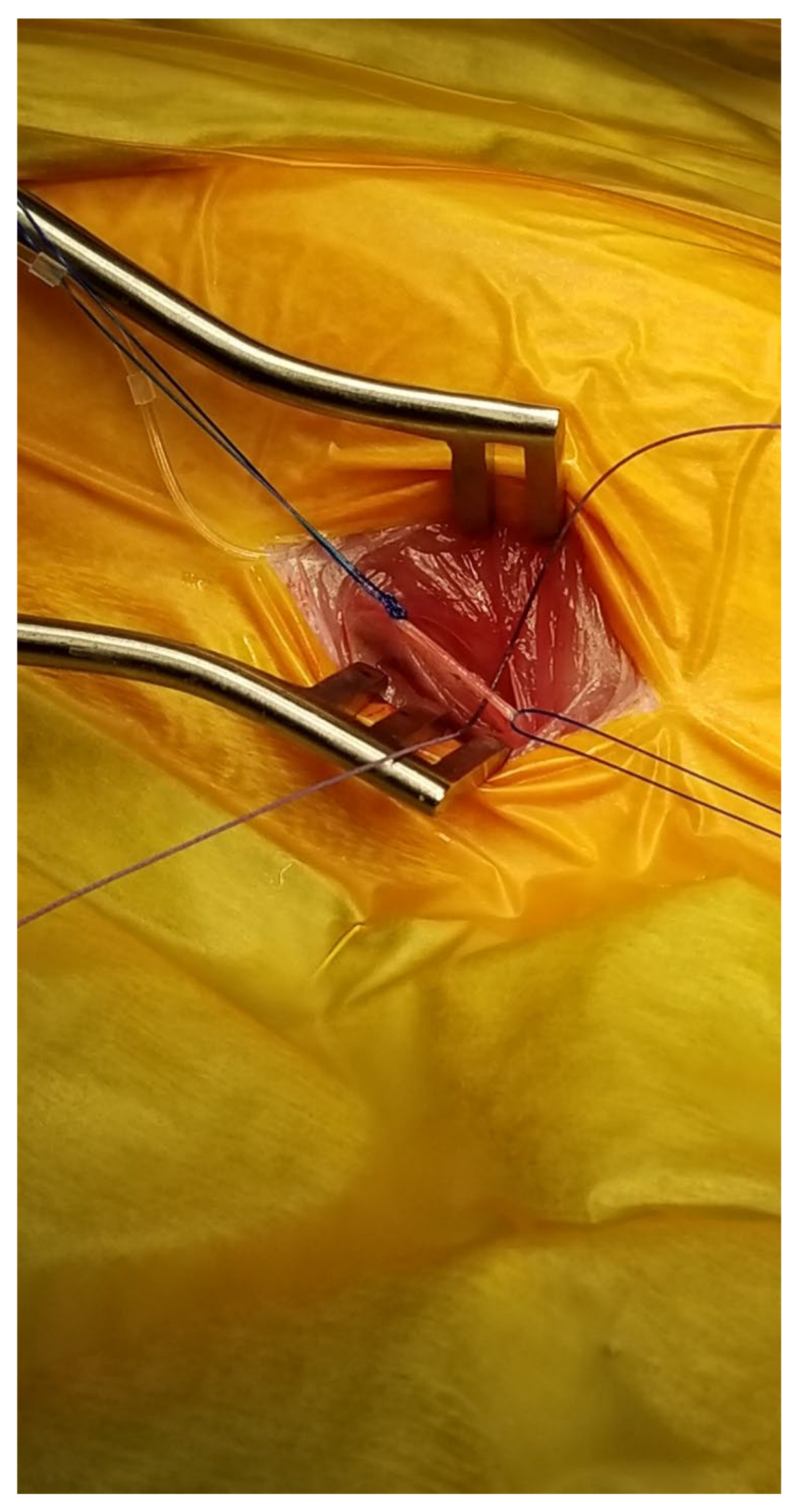
2.4. Surgical Procedure
2.5. Post-Operative Care
2.6. Catheter Maintenance
3. Results
3.1. Patency
3.2. Surgical Complications
3.3. Post-Operative Complications
4. Discussion
4.1. Pharmacokinetic Studies
4.2. Refinements
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Perry-Clark, L.M.; Meunier, L.D. Vascular access ports for chronic serial infusion and blood sampling in New Zealand rabbits. Lab. Anim. Sci. 1991, 41, 495–497. [Google Scholar]
- Griswold, D.E.; Martin, L.; Ventre, J.; Meunier, L.; Perry, L. Technique for quantification of LTB4-Induced changes in peripheral granulocyte counts in vivo in the rabbit. J. Pharmacol. Methods 1991, 25, 319–328. [Google Scholar] [CrossRef]
- Marongiu, M.L.; Gulinati, A.; Floris, B. A procedure for rabbit blood serial collection. Ital. J. Anim. Sci. 2007, 6 (Suppl. S1), 773. [Google Scholar] [CrossRef]
- Cleva, G.M.; Stone, G.M.; Evans, D.L.; Dickens, R.K. Chronic vascular catheterization of the koala and the rabbit. Aust. Vet. J. 1995, 72, 50–52. [Google Scholar] [CrossRef] [PubMed]
- Kunta, J.R.; Perry, B.A.; Sutyak, J.P. Development of a novel intestinal and vascular access port (IAVP) rabbit model to study regiospecific oral absorption pharmacokinetics. Comp. Med. 2001, 51, 349–356. [Google Scholar] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Animal ID | Age (Months) | Weight (Kg) | Model | Surgical Outcome | Patency (Days) | Comments |
|---|---|---|---|---|---|---|
| 1 | 14 | 4 | Arterial | Successful | 253 | |
| 2 | 12 | 3.8 | Arterial | Successful | 250 | |
| 3 | 15 | 3.9 | Arterial | Successful | 253 | |
| 4 | 14 | 4.5 | Arterial | Successful | 252 | |
| 5 | 14 | 4.1 | Arterial | Successful | 112 | |
| 6 | 14 | 4.6 | Arterial | Successful | 251 | |
| 7 | 6 | 3.4 | Arterial and venous | Successful, arterial catheter only advanced 8 cm | 617+ | Arterial catheter is infusion only |
| 8 | 6 | 3.3 | Arterial and venous | Successful, arterial catheter only advanced 10 cm | 616+ | Arterial catheter is infusion only |
| 9 | 6 | 3.4 | Arterial and venous | Successful | 608+ | |
| 10 | 6 | 3.4 | Arterial and venous | Successful | 329 | |
| 11 | 14 | 3.8 | Arterial and venous | Successful | 322+ | |
| 12 | 9 | 4 | Arterial and venous | Successful | 314+ | |
| 13 | 12 | 3.4 | Arterial and venous | Successful | 59 | Removed from the colony at day 59 |
| 14 | 12 | 4 | Arterial and venous | Successful | 76 | Removed from the colony at day 76 |
| 15 | 16 | 3.8 | Arterial and venous | Successful | 196+ | |
| 16 | 16 | 3.6 | Arterial and venous | Successful | 195+ | |
| 17 | 16 | 3.5 | Arterial and venous | Successful | 182+ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ehrmann, J.; Johnson, W.; de Castro, A.; Donnelly, M. Implantation of a Vascular Access Button for Chronic Blood Sampling and Drug Administration in the Rabbit. Surgeries 2023, 4, 141-151. https://doi.org/10.3390/surgeries4020016
Ehrmann J, Johnson W, de Castro A, Donnelly M. Implantation of a Vascular Access Button for Chronic Blood Sampling and Drug Administration in the Rabbit. Surgeries. 2023; 4(2):141-151. https://doi.org/10.3390/surgeries4020016
Chicago/Turabian StyleEhrmann, Jon, Wendy Johnson, Arlene de Castro, and Marcie Donnelly. 2023. "Implantation of a Vascular Access Button for Chronic Blood Sampling and Drug Administration in the Rabbit" Surgeries 4, no. 2: 141-151. https://doi.org/10.3390/surgeries4020016
APA StyleEhrmann, J., Johnson, W., de Castro, A., & Donnelly, M. (2023). Implantation of a Vascular Access Button for Chronic Blood Sampling and Drug Administration in the Rabbit. Surgeries, 4(2), 141-151. https://doi.org/10.3390/surgeries4020016