
Pregnancy-Related Decision-Making and Perceptions of Risk among Reproductive-Age Females Undergoing Hip Arthroscopy for Femoroacetabular Impingement Syndrome: A Single-Surgeon Cross-Sectional Study

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Ethical Approval
2.3. Patient Population and Eligibility Criteria
2.4. Diagnostic Protocol and Surgical Indications
2.5. Surgical Technique and Postoperative Protocol
2.6. Demographic and Operative Information
2.7. Survey Description
2.7.1. Obstetric and Gynecologic (OB/GYN) History
2.7.2. Surgical and Pregnancy Planning
2.7.3. Perception of Risks to Pregnancy from Hip Pain and Hip Surgery
2.8. Statistical Analysis
3. Results
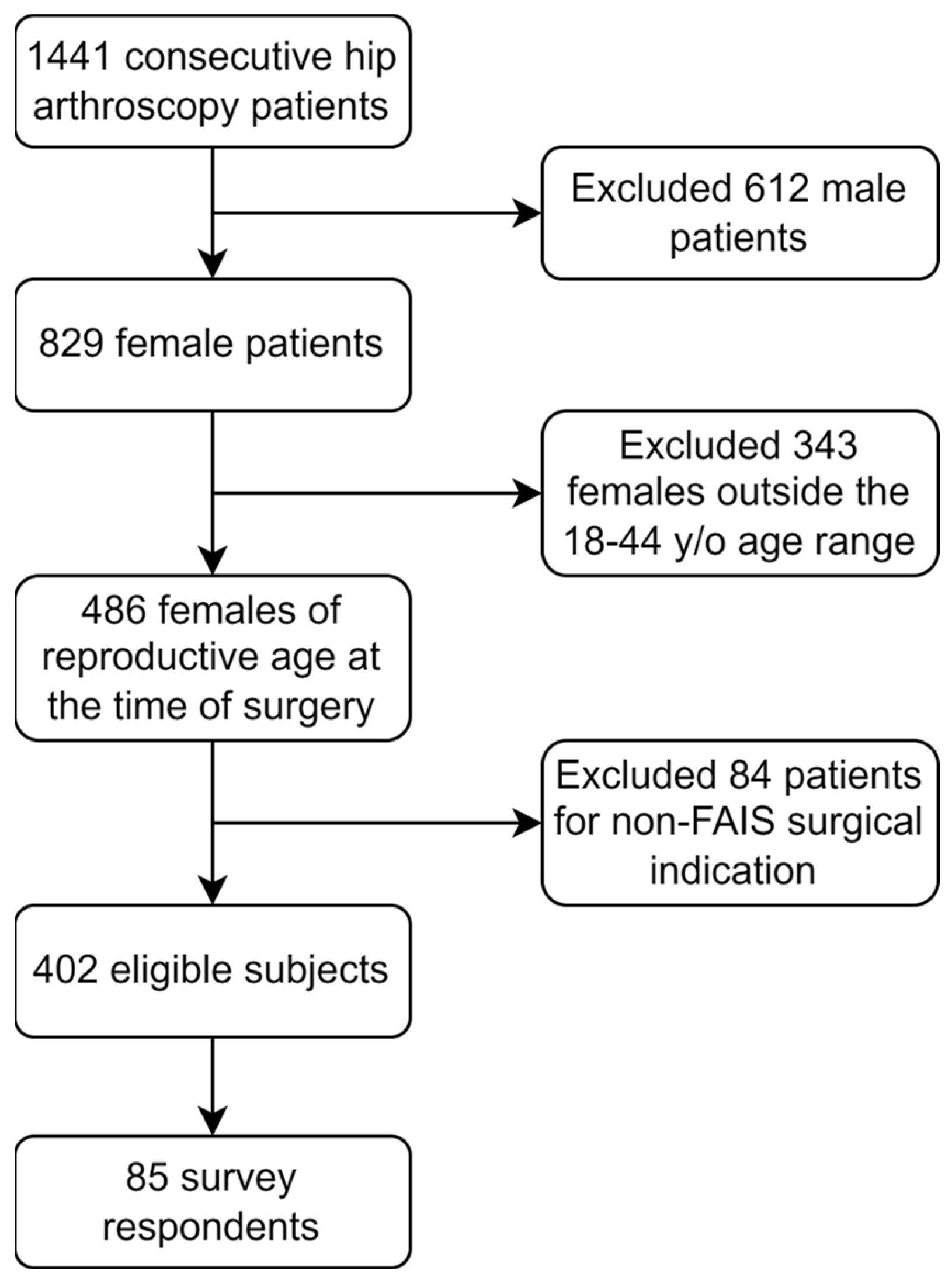
3.1. Patient Flow
3.2. Subject Demographics
3.3. OB/GYN History
3.4. Pregnancy Decision-Making among Group 1 Subjects (Nulligravidae)
3.5. Pregnancy Decision-Making among Group 3 Subjects
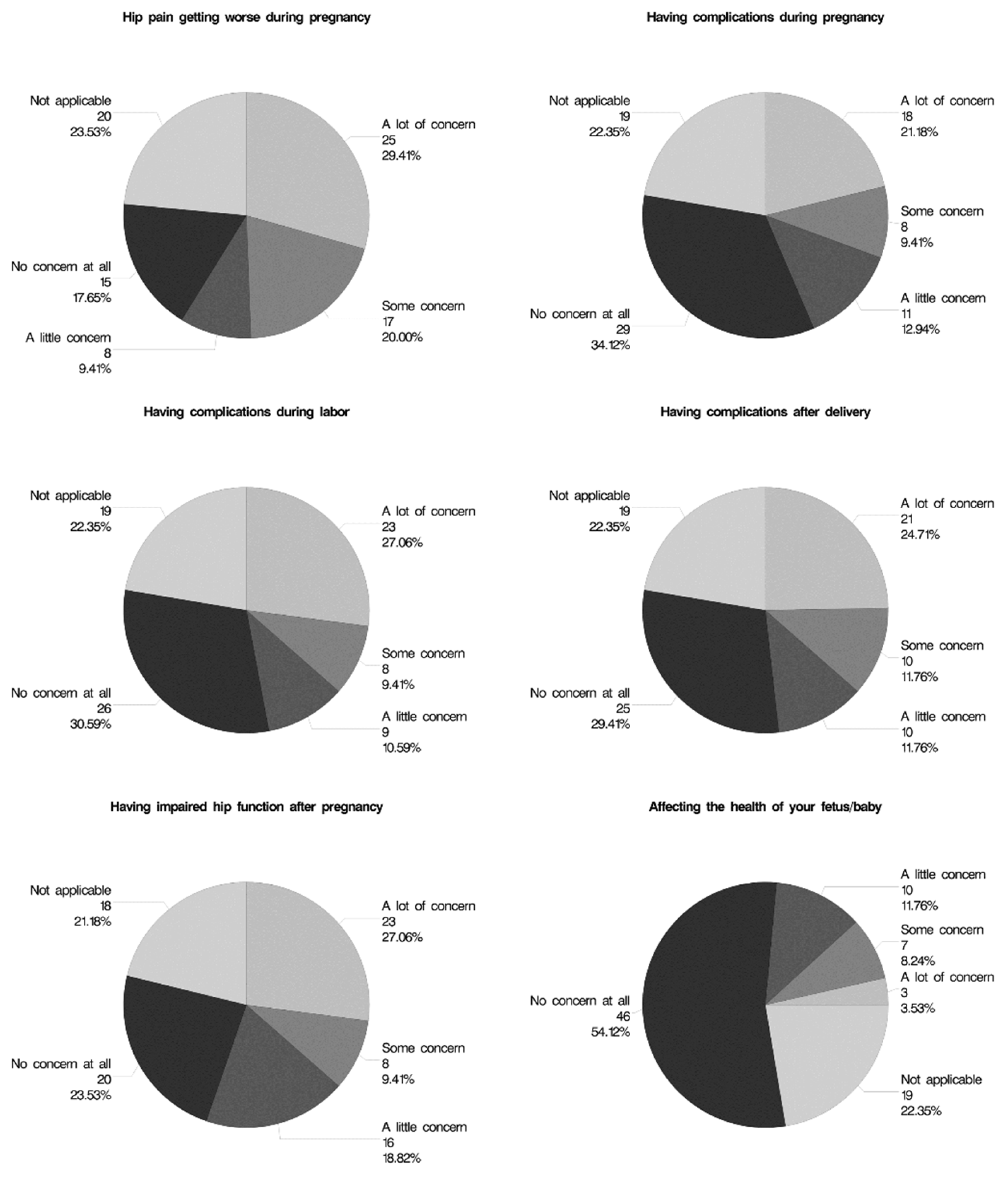
3.6. Hip Pain and Perceived Risks to Pregnancy
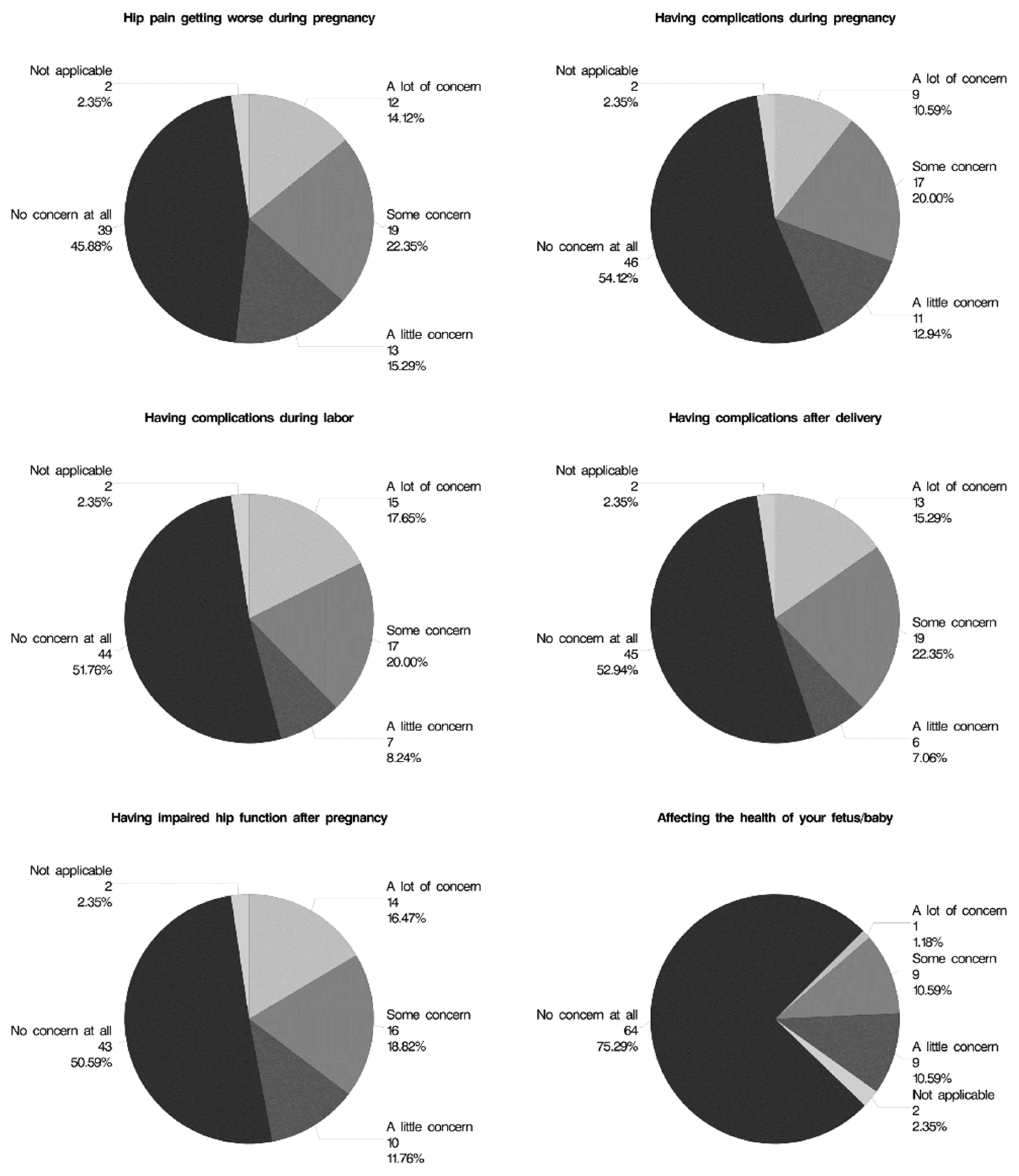
3.7. Hip Surgery and Perceived Risks to Pregnancy
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zusmanovich, M.; Haselman, W.; Serrano, B.; Banffy, M. The incidence of hip arthroscopy in patients with femoroacetabular impingement syndrome and labral pathology increased by 85% between 2011 and 2018 in the United States. Arthroscopy 2022, 38, 82–87. [Google Scholar] [CrossRef]
- Minkara, A.A.; Westermann, R.W.; Rosneck, J.; Lynch, T.S. Systematic review and meta-analysis of outcomes after hip arthroscopy in femoroacetabular impingement. Am. J. Sports Med. 2019, 47, 488–500. [Google Scholar] [CrossRef] [PubMed]
- Jan, K.; Fenn, T.W.; Kaplan, D.J.; Nho, S.J. Patients maintain clinically significant outcomes at 5-year follow-up after hip arthroscopy for femoroacetabular impingement syndrome: A systematic review. Arthroscopy 2023, 39, 1869–1881.e1861. [Google Scholar] [CrossRef] [PubMed]
- Hoffer, A.J.; Kingwell, D.; Leith, J.; McConkey, M.; Ayeni, O.R.; Lodhia, P. Intra-articular soft tissue pathology of the postpartum hip: A systematic review. Curr. Rev. Musculoskelet. Med. 2022, 15, 659–666. [Google Scholar] [CrossRef] [PubMed]
- McDowell, C.M.; Lachiewicz, P.F. Pregnancy after total hip arthroplasty. J. Bone Joint Surg. Am. 2001, 83, 1490–1494. [Google Scholar] [CrossRef] [PubMed]
- Yazici, Y.; Erkan, D.; Zuniga, R.; Bateman, H.; Salvati, E.A.; Magid, S.K. Pregnancy outcomes following total hip arthroplasty: A preliminary study and review of the literature. Orthopedics 2003, 26, 75–76. [Google Scholar] [CrossRef] [PubMed]
- Stea, S.; Bordini, B.; De Clerico, M.; Traina, F.; Toni, A. Safety of pregnancy and delivery after total hip arthroplasty. J. Womens Health 2007, 16, 1300–1304. [Google Scholar] [CrossRef] [PubMed]
- Sierra, R.J.; Trousdale, R.T.; Cabanela, M.E. Pregnancy and childbirth after total hip arthroplasty. J. Bone Joint Surg. Br. 2005, 87, 21–24. [Google Scholar] [CrossRef] [PubMed]
- Ellington, S.; Strid, P.; Tong, V.T.; Woodworth, K.; Galang, R.R.; Zambrano, L.D.; Nahabedian, J.; Anderson, K.; Gilboa, S.M. Characteristics of women of reproductive age with laboratory-confirmed SARS-CoV-2 infection by pregnancy status—United States, January 22–June 7, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 769–775. [Google Scholar] [CrossRef]
- Shankar, D.S.; Bi, A.S.; Buldo-Licciardi, M.; Rynecki, N.D.; Akpinar, B.; Youm, T. Five-year outcomes of primary hip arthroscopy for femoroacetabular impingement syndrome among female patients: Higher body mass index is associated with reduced clinically significant outcomes. Arthroscopy 2023, 40, 732–741. [Google Scholar] [CrossRef]
- Shankar, D.S.; Wingo, T.; Akpinar, B.; Rynecki, N.D.; Youm, T. Patient-reported outcomes and survivorship are not different for primary hip arthroscopy patients of age 50 years and older compared to a 20 to 35 years old matched cohort at minimum five-year follow-up. Arthroscopy 2023, 39, 1651–1659. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Conder, R.; Zamani, R.; Akrami, M. The biomechanics of pregnancy: A systematic review. J. Funct. Morphol. Kinesiol. 2019, 4, 72. [Google Scholar] [CrossRef] [PubMed]
- Saltzman, B.M. Editorial commentary: Obesity is associated with lower hip function pre- and postoperatively and increased time to patient acceptable symptom state after hip arthroscopy. Arthroscopy 2023, 39, 1980–1982. [Google Scholar] [CrossRef] [PubMed]
- Marnach, M.L.; Ramin, K.D.; Ramsey, P.S.; Song, S.W.; Stensland, J.J.; An, K.N. Characterization of the relationship between joint laxity and maternal hormones in pregnancy. Obstet. Gynecol. 2003, 101, 331–335. [Google Scholar] [CrossRef] [PubMed]
- Brooks, A.G.; Domb, B.G. Acetabular labral tear and postpartum hip pain. Obstet. Gynecol. 2012, 120, 1093–1098. [Google Scholar] [CrossRef] [PubMed]
- Palsson, T.S.; Beales, D.; Slater, H.; O’Sullivan, P.; Graven-Nielsen, T. Pregnancy is characterized by widespread deep-tissue hypersensitivity independent of lumbopelvic pain intensity, a facilitated response to manual orthopedic tests, and poorer self-reported health. J. Pain 2015, 16, 270–282. [Google Scholar] [CrossRef]
- ACOG Committee. Opinion No. 775: Nonobstetric surgery during pregnancy. Obstet. Gynecol. 2019, 133, e285–e286. [CrossRef]
- Filan, D.; Mullins, K.; Carton, P. Hip range of motion is increased after hip arthroscopy for femoroacetabular impingement: A systematic review. Arthrosc. Sports Med. Rehabil. 2022, 4, e797–e822. [Google Scholar] [CrossRef]
- Alkan, H.; Erdogan, Y.; Veizi, E.; Sezgin, B.S.; Cepni, S.; Mert, H.C.; Firat, A. Better sex after hip arthroscopy: Sexual dysfunction in patients with femoro-acetabular impingement syndrome. Orthop. Traumatol. Surg. Res. 2023, 103693. [Google Scholar] [CrossRef] [PubMed]
- Rynecki, N.D.; Kingery, M.T.; DeClouette, B.; Buldo-Licciardi, M.; Jazrawi, T.; Eskenazi, J.; Lan, R.; Youm, T. Hip Arthroscopy Improves Sexual Function in Receptive Partners with Femoroacetabular Impingement Syndrome. Clin. Orthop. Relat. Res. 2024. [Google Scholar] [CrossRef] [PubMed]
- Beck, E.C.; Drager, J.; Nwachukwu, B.U.; Jan, K.; Rasio, J.; Nho, S.J. Gender and age-specific differences observed in rates of achieving meaningful clinical outcomes 5-years after hip arthroscopy for femoroacetabular impingement syndrome. Arthroscopy 2021, 37, 2488–2496.e1. [Google Scholar] [CrossRef] [PubMed]
- Jones, D.L.; Philippi, M.T.; Maak, T.G.; Aoki, S.K. Progressive osteoarthritis during pregnancy several years following hip arthroscopy for femoroacetabular impingement. J. Orthop. 2018, 15, 475–479. [Google Scholar] [CrossRef] [PubMed]
- Matsuda, D.K.; Khatod, M. Rapidly progressive osteoarthritis after arthroscopic labral repair in patients with hip dysplasia. Arthroscopy 2012, 28, 1738–1743. [Google Scholar] [CrossRef] [PubMed]
- Kuitunen, I.; Eskelinen, A.; Skytta, E.T.; Huhtala, H.; Artama, M. Congenital anomalies in the offspring of women with total hip replacement: A nationwide register study in Finland. Hip. Int. 2021, 31, 348–353. [Google Scholar] [CrossRef] [PubMed]
- Meldrum, R.; Feinberg, J.R.; Capello, W.N.; Detterline, A.J. Clinical outcome and incidence of pregnancy after bipolar and total hip arthroplasty in young women. J. Arthroplast. 2003, 18, 879–885. [Google Scholar] [CrossRef]
- Smith, M.W.; Marcus, P.S.; Wurtz, L.D. Orthopedic issues in pregnancy. Obstet. Gynecol. Surv. 2008, 63, 103–111. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable a | All subjects (n = 85) | Group 1 b (n = 39) | Group 2 b (n = 20) | Group 3 b (n = 26) | p-Value c |
|---|---|---|---|---|---|
| Number of subjects | 85 | 39 | 20 | 26 | - |
| Age at the time of surgery (years) | 32.3 ± 6.5 | 29.6 ± 6.6 | 36.6 ± 5.4 | 33.2 ± 5.1 | 0.002 * |
| 1 < 3 | |||||
| 2 < 3 | |||||
| BMI at the time of surgery | 24.5 ± 4.7 | 24.2 ± 4.2 | 26.5 ± 6.8 | 23.2 ± 2.6 | 0.62 |
| Prior surgery on the index hip | 8 (9.4%) | 6 (15.4%) | 1 (5.0%) | 1 (3.9%) | 0.31 |
| Gravidity | n/a | G0: 39 (100.0%) | G1: 5 (25.0%) | G1: 11 (42.3%) | n/a |
| G2: 6 (30.0%) | G2: 10 (38.5%) | ||||
| G3: 1 (5.0%) | G3: 4 (15.4%) | ||||
| G4: 4 (20.0%) | G4: 0 (0.0%) | ||||
| G5: 3 (15.0%) | G5: 1 (3.9%) | ||||
| G6: 1 (5.0%) | G6: 0 (0.0%) | ||||
| Parity | n/a | P0: 39 (100.0%) | P0: 4 (20.0%) | P0: 1 (3.9%) | n/a |
| P1: 2 (10.0%) | P1: 12 (46.2%) | ||||
| P2: 8 (40.0%) | P2: 12 (46.2%) | ||||
| P3: 4 (20.0%) | P3: 1 (3.9%) | ||||
| P4: 2 (10.0%) | P4: 0 (0.0%) | ||||
| Time from surgery to subsequent pregnancy (months) | 51.9 ± 34.5 | 46.8 ± 33.6 | 48.1 ± 31.3 | 62.6 ± 36.8 | 0.23 |
| Considering future pregnancy | 43 (50.6%) | 28 (71.8%) | 2 (10.0%) | 13 (50.0%) | <0.001 * |
| Time elapsed from surgery to survey response (months) | 51.9 ± 34.5 | 46.8 ± 33.6 | 48.1 ± 31.3 | 62.6 ± 36.8 | 0.23 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shankar, D.S.; Li, Z.I.; Triana, J.; Eskenazi, J.A.; Lan, R.; Hughes, A.J.; Youm, T. Pregnancy-Related Decision-Making and Perceptions of Risk among Reproductive-Age Females Undergoing Hip Arthroscopy for Femoroacetabular Impingement Syndrome: A Single-Surgeon Cross-Sectional Study. Surgeries 2024, 5, 194-205. https://doi.org/10.3390/surgeries5020019
Shankar DS, Li ZI, Triana J, Eskenazi JA, Lan R, Hughes AJ, Youm T. Pregnancy-Related Decision-Making and Perceptions of Risk among Reproductive-Age Females Undergoing Hip Arthroscopy for Femoroacetabular Impingement Syndrome: A Single-Surgeon Cross-Sectional Study. Surgeries. 2024; 5(2):194-205. https://doi.org/10.3390/surgeries5020019
Chicago/Turabian StyleShankar, Dhruv S., Zachary I. Li, Jairo Triana, Jordan A. Eskenazi, Rae Lan, Andrew J. Hughes, and Thomas Youm. 2024. "Pregnancy-Related Decision-Making and Perceptions of Risk among Reproductive-Age Females Undergoing Hip Arthroscopy for Femoroacetabular Impingement Syndrome: A Single-Surgeon Cross-Sectional Study" Surgeries 5, no. 2: 194-205. https://doi.org/10.3390/surgeries5020019
APA StyleShankar, D. S., Li, Z. I., Triana, J., Eskenazi, J. A., Lan, R., Hughes, A. J., & Youm, T. (2024). Pregnancy-Related Decision-Making and Perceptions of Risk among Reproductive-Age Females Undergoing Hip Arthroscopy for Femoroacetabular Impingement Syndrome: A Single-Surgeon Cross-Sectional Study. Surgeries, 5(2), 194-205. https://doi.org/10.3390/surgeries5020019