1. Introduction
Spinal cord injury (SCI) is a highly disabling condition that can result in severe impairment of sensory, motor, and autonomic functions. This can lead to several complications that can make it difficult for patients to perform basic activities of daily living, such as sexual and bladder dysfunction, gastrointestinal and respiratory problems, and urinary tract infections [
1,
2].
In these cases, specific therapies that aim to stimulate or not stimulate neuroplasticity to promote axonal growth have been utilized. While this process is time-consuming, it can increase pre-existing connections and promote the formation of new neuronal circuits [
2]. In the presence of a compromised pathway, one form of intervention is through functional neurorecovery, in which training capitalizes on the intrinsic mechanisms of the nervous system (NS) to generate rhythmic movements through sensorimotor pathways [
3]. According to Musselman and colleagues [
4], this pattern currently used in neurorehabilitation is performed through assistive technologies (AT).
An example of AT in evidence is brain–machine interfaces (BCIs) which link cortical control and electrical stimulation of muscles. Through this mechanism, these interfaces engage part of the spinal cord function, making it possible to restore basic functions such as gripping or muscle stretching [
5]. According to Yang et al. [
2], such BCIs must contain a mechanism to record the neuroelectric signal (NES
), such as electroencephalography (EEG), to send signals to a computer, which in turn decodes the expected movement and activates auxiliary devices to perform the expected movement. This stimulus can be performed through functional electrical stimulation devices (FES
) [
6].
In order for the NES from the EEG to be more consistent with the desired task, it is extremely important to use motor imagery (MI) for the desired action, which causes oscillations in sensorimotor rhythms in the motor regions of the brain [
7]. In addition, according to Bobrova et al. [
8], it has been suggested that BCI systems based on FES
operate on the Hebbian learning principle, where the simultaneous excitation of the motor zones of the cortex during MI and the spinal cord structure stimulated by FES
leads to an improvement in the ability to control the movements of the paralyzed limb. With this association between the computer and the effector systems, better secondary functions are observed in intestinal, urinary, and sexual functions in addition to improvements in flexibility and control of fine motor skills using the limbs [
2].
However, as BCIs depend on full concentration to perform activities correctly, they can be influenced by situations of anxiety, fatigue, or frustration. Therefore, strategies have emerged to try to mitigate these limitations, which include mindfulness meditation and music training. Of these, there has been greater emphasis on mindfulness for stimulating self-regulation of cognitive and emotional processes [
9].
In the use of BCIs, a point of extreme relevance is the learning curve that the user goes through to adapt to the use of the interface and eventually enhance its performance. There is a trend towards gradual improvement in the results as relevant therapies are maintained. However, direct or indirect factors in the execution of neurorehabilitation, alternating between user-specific elements and ways of implementing the methodologies and functioning of the BCI, hinder the development of learning [
3,
10,
11]. This pilot study aims to investigate the learning curves of two people with complete spinal cord injury using the NES
-FES
interface in the sitting position. As a hypothesis, it is expected that throughout the interventions the users of the NES
-FES
interface will increase the accuracy of the NES
classifier and reduce the false positive rate during the motor imagery to FES
activation process.
2. Materials and Methods
This was an uncontrolled longitudinal pilot study with a convenience sample composed of people with motor deficits resulting from spinal cord injury. The research was approved by the Ethics Committee in Research Involving Human Beings of the State University of Londrina (CEP-UEL), with opinion n 4,060,700. Participants/users were recruited through advertising in physiotherapy clinics in Londrina. The initial contact with the participants took place through a brief interview via a telephone call to collect information about the injury. In addition, the objectives of the project and how the interventions are carried out were briefly explained. Subsequently, the participants were invited to visit the Laboratório de Engenharia Neural e de Reabilitação (LENeR) and sign the form indicating free and informed consent, allowing initiation of the research protocols. The research lasted sixteen weeks for each participant, with one intervention per week (sixteen in total). The transport costs of the participants were paid for by the laboratory’s administration section.
2.1. Inclusion Criteria
Eighteen years of age or older;
A spinal cord injury between the C and T levels;
An injury time greater than twelve months.
2.2. Exclusion Criteria
Intolerance to discomfort caused by electrical stimulation;
Presence of neoplastic tissue near or in the lower limbs (electrically stimulated area);
Metallic implant in regions close to or between electrical stimulation electrodes;
Any cognitive alteration that might prevent experimental intervention;
Presence of other neurological or orthopedic disorders that might preclude experimental intervention;
Presence of infectious disease;
Presence of a cardiac pacemaker;
Three consecutive absences without prior warning.
2.3. NES
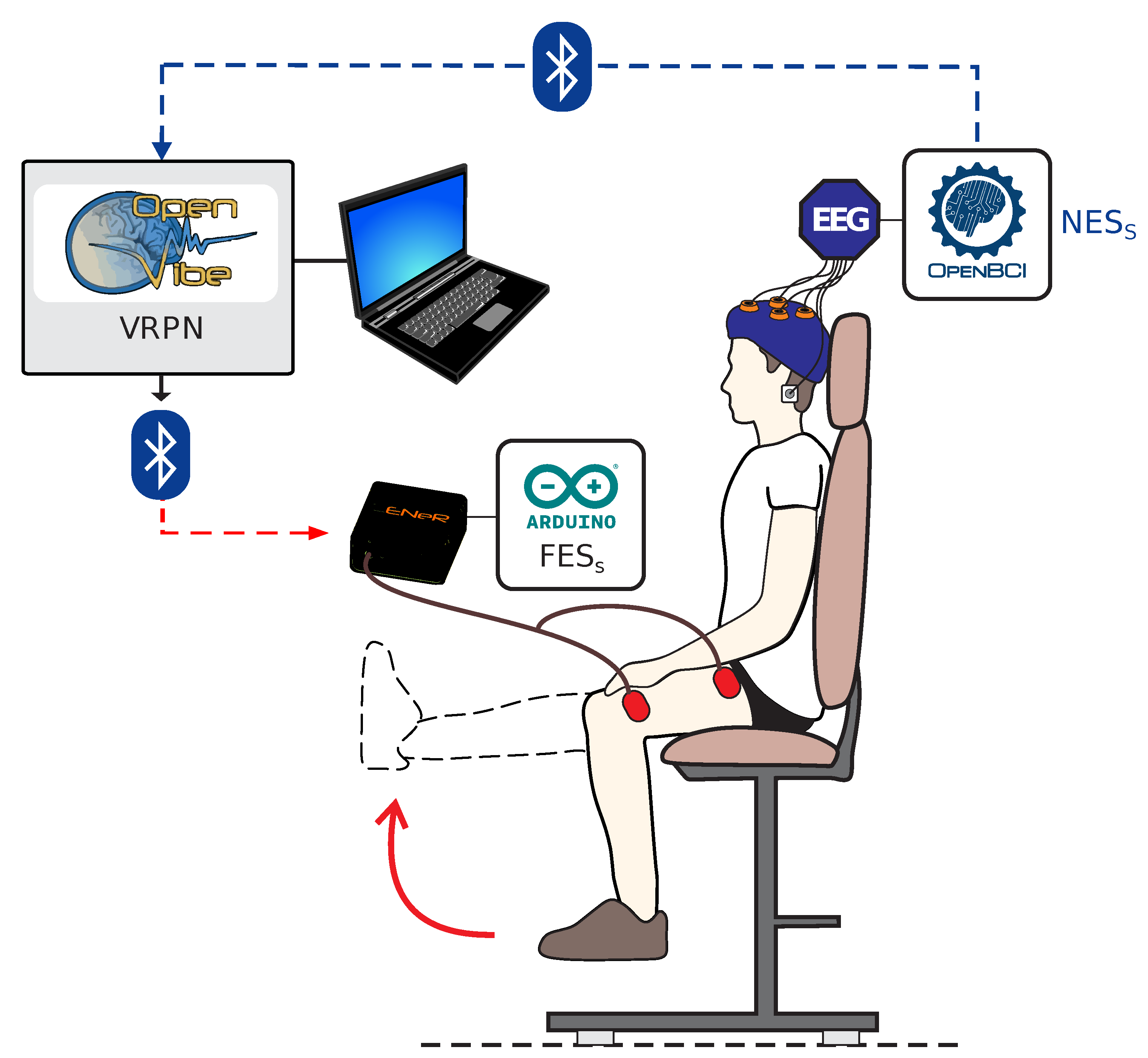
The participant was positioned seated in their wheelchair or an adapted chair in the LENeR facilities. In the interventions, non-woven fabric meshes were used to cover the chair and hide the lower limbs (LL), preventing their visualization by the participant during the BCI calibration. During installation of the equipment care was taken to respect the integrity of the participant in order to ensure their greater comfort.
2.3.1. NES Acquisition
EEG data were acquired using commercial equipment (Cyton OpenBCI Board®, Brooklyn, NY, USA ). OpenVibe® (version 3.0) software was used to acquire the signals; this software is an open-source C tool that can be customized for different purposes. The acquisition frequency of the NES was 250 Hz.
EEG Channels
In all sessions, brain activity was recorded using gold electrodes (Maxxi Gold®, Rome, Italy) distributed in a 10–10 system pattern over the scalp with conductive paste (Carbofix®, Herzliya, Israel) and conductive gel (Ultra-gel Eletro®). The channels (unipolar) were positioned in the Cz, C1 (or C2), FCz, and CPz regions and fixed with the aid of a customized EEG cap. Reference channels A1 and A2 were fixed bilaterally using Ag/AgCl electrodes on the mastoid processes of the temporal bones.
NES Preprocessing
The NES
was preprocessed using a 5th-order bandpass digital Butterworth filter (8–25 Hz) with an analysis window duration of 500 ms and a passband ripple equal to 1 dB. These settings were necessary to ensure the integrity of events related to desynchronization and synchronization (ERD/ERS) during MI related to the lower limbs [
12].
2.3.2. Step I—NES Check
In the NES checking phase, the feasibility of the signals recorded by the EEG electrodes was investigated. Such signals are composed of a set of local and noise field potentials. In the case of local field potentials, their measurement occurs from the depolarization of a population of superficial neurons. Because it is very weak, this signal is subject to noise, such as the noise caused by the electrical network.
After the signals were obtained, their demonstration was performed graphically under the temporal domain. Afterwards, the data were subjected to Fourier transform in order to decompose the deterministic signals into the frequency components [
13] in order to permit graphic demonstration within the spectral domain. This allowed for analysis of noise that might interfere with the signal and the frequency bands that were present according to the brain activity. The absence of wave patterns or cases of recording in rhythmic form indicate errors in capturing the signals in the region by the corresponding channel which need to be corrected before proceeding.
2.3.3. Step II—Calibration of Motor Imagery
The assay methodology was adapted from Yusoff [
12], in which participants looked at a reference while simultaneously receiving instruction to perform the MI. An instructor used mirrored and verbal movement to reproduce to the participant the instructions (classes) that were indicated on the monitor, namely, (i) motor imagery and (ii) rest. At these moments, the participant (1) imagined the knee extension movement, or (2) remained inactive. Between 5 and 10 trials were performed, with an average duration of 8 s for the two classes. The sequence of IM classes presented to the individual was random, and the NES
was recorded by the system. The LL in which the classes started was random in all interventions. MI training was performed at the beginning of every session, and was performed individually for the left leg and right leg. Step II was performed up to three times (lasting approximately 5–7 min in this Step) to achieve a better response before proceeding to Step III.
2.3.4. Step III—Spatial Filtering
Feature extraction was performed using the Common Spatial Pattern (CSP) filter. The equation of this filter is based on the work of Broniera-Junior et al. [
14], where the CSP maximizes the variance of the spatially filtered NES
under one condition (MI) while minimizing it for the other condition (rest). The seventh-order spatial filter was considered ideal for the present work.
2.3.5. Step IV—Motor Imagery Classifier
In this step, the Linear Discriminant Analysis (LDA) classifier was used to classify the results obtained by the CSP filter by reducing the resources to a space of lower dimension and maximizing the separation between the classes (MI and rest) [
15]. The result of the (Ac
) classifier accuracy is expressed in percentage units (%). The choice of the number of EEG channels and selection of the classifier were based on our previous study [
16], which indicated that for LDA four EEG channels presents more satisfactory results compared to multi-layer perceptron and support vector machine approaches.
2.3.6. Step V—Application of the NES-FES Interface
In this step, the participant was again instructed to imagine the movement indicated by the instructor. When MI activity was requested, the Ac
value was automatically calculated at 1 s. After calculation, if the Ac
value was equal to or above 72% a computational instruction was transferred from the OpenVibe
® software to the Virtual-Reality Peripheral Network (VRPN)-based interface developed in C
in the Microsoft Visual Studio
® [
17] environment. The signal received by the VRPN was then processed and sent in binary form to the electrical stimulator via Bluetooth to activate it.
FES
For artificial nerve activation [
18], an electrical stimulator was customized exclusively for this work following the criteria proposed in the IEC standard 60601-2-10 [
19]. Two self-adhesive electrodes were positioned in the anterior region of the volunteer’s thigh according to the methodology of Krueger et al. [
20], measuring 5 × 9 cm. One of the electrodes was positioned with the lower edge 3 cm from the base of the patella and the other over the femoral triangle [
21] to stimulate the quadriceps muscle through the femoral nerve [
22]. According to Krueger et al. [
20], after fixing the electrodes, an interval of 10 min is respected to stabilize the electrode–skin impedance. The biphasic electrical stimulation frequency parameters were: carrier frequency of 1 kHz (positive: 200
+ negative: 200
+ off: 600
, negative: 200
+ positive: 200
+ off: 600
). The modulated frequency was 20–40 Hz (active period of 24 ms) to increase and decrease the pulse trains. The amplitude was modulated according to the instant of maximum electrically stimulated extension [
20]. During step V, the activation condition of FES
occurred when the probability of similarity of the classifier output signal is equal to or greater than 72%. The assembly of the equipment on the participant is illustrated in
Figure 1.
2.3.7. Mindfulness Training
The audio used was developed by instructor Katya Stübing. It was suggested to both participants that they listen to the audio daily at the period of the day that they felt the most comfortable. Each mindfulness training session lasted 149 s. According to Linehan [
23], this training has been shown to improve emotional regulation. This daily task aimed to improve the performance of the participant during the sessions when carrying out the training and interventions.
2.4. Learning Curve Assessment
The participants’ assessment of the NES-FES interface learning curve included the following items:
2.5. Data Analysis, Presentation, and Statistics
The present study analyzed the learning curves in the application of the NES-FES interface in two people with complete spinal cord injuries. The participants were , with lesion level for eight years, and , with lesion level for fourteen years. The graphics were developed in a customized routine through the Plotly Open Source Graphing Library for Python®. (version 3.8.2-0ubuntu2) The image’s final editing was performed in Inkscape® version 1.2.2. A customized routine of the open-source software Octave® version 5.2.0 was used for statistical tests. Due to the small sample, we assumed that our data were non-parametric and performed the Spearman’s correlation (and p-value) test for the sixteen sessions with Ac and the success percentage of FES activation for each participant and each leg.
3. Results and Discussion
3.1. Learning Curve
As the sessions were carried out, an increase in the efficiency of the interventions was observed, with the participants gradually adapting to the interface and the indexes presenting the number of training repetitions (Ac and success percentage for FES activation) improving.
3.1.1. User’s Repetition of MI Training
The repetition of user MI training was performed in different situations, such as changes in FES
or when Ac
values were insufficient for a correct intervention. These repetitions proved to be efficient when the calibration was performed improperly, allowing for better Ac
values for the application of the NES
-FES
interface. However, as mentioned by Apicella et al. [
11], when the calibrations are performed properly the participants reported mental fatigue despite the benefits of repeating the exercise, which may have reduced their performance.
Therefore, it was essential to look for ways to enhance the performance of the participants in order to minimize repetitions. Removing distractions may have positively affected the learning curve with the interface, as it provided greater comfort for participants during the interventions. Any individuals from the laboratory except the researcher and participant were removed during MI calibration, and any sound sources that could compromise concentration were minimized. These actions are supported by the work of Tianhang Liu [
6], who has addressed the importance of mindfulness during such interventions.
However, several factors that interfered with the results persisted, such as the participant’s mood and self-reported mental fatigue before and during the calibrations [
3,
6,
11]. Hernandez-Rojas et al. [
10] have pointed out that this interference occurs due to the implementation of a two-class classification paradigm in which the classifier aims to discriminate between two highly related and antagonistic conditions, such as “stretch the leg” and “relax the leg”. For this reason, interfaces such as the one used in this research require broad user engagement in the completion of the requested tasks, as other cognitive tasks can be potentially interpreted within the pre-established paradigms even if they are not related to movement, ultimately affecting the activation of the NES
-FES
interface.
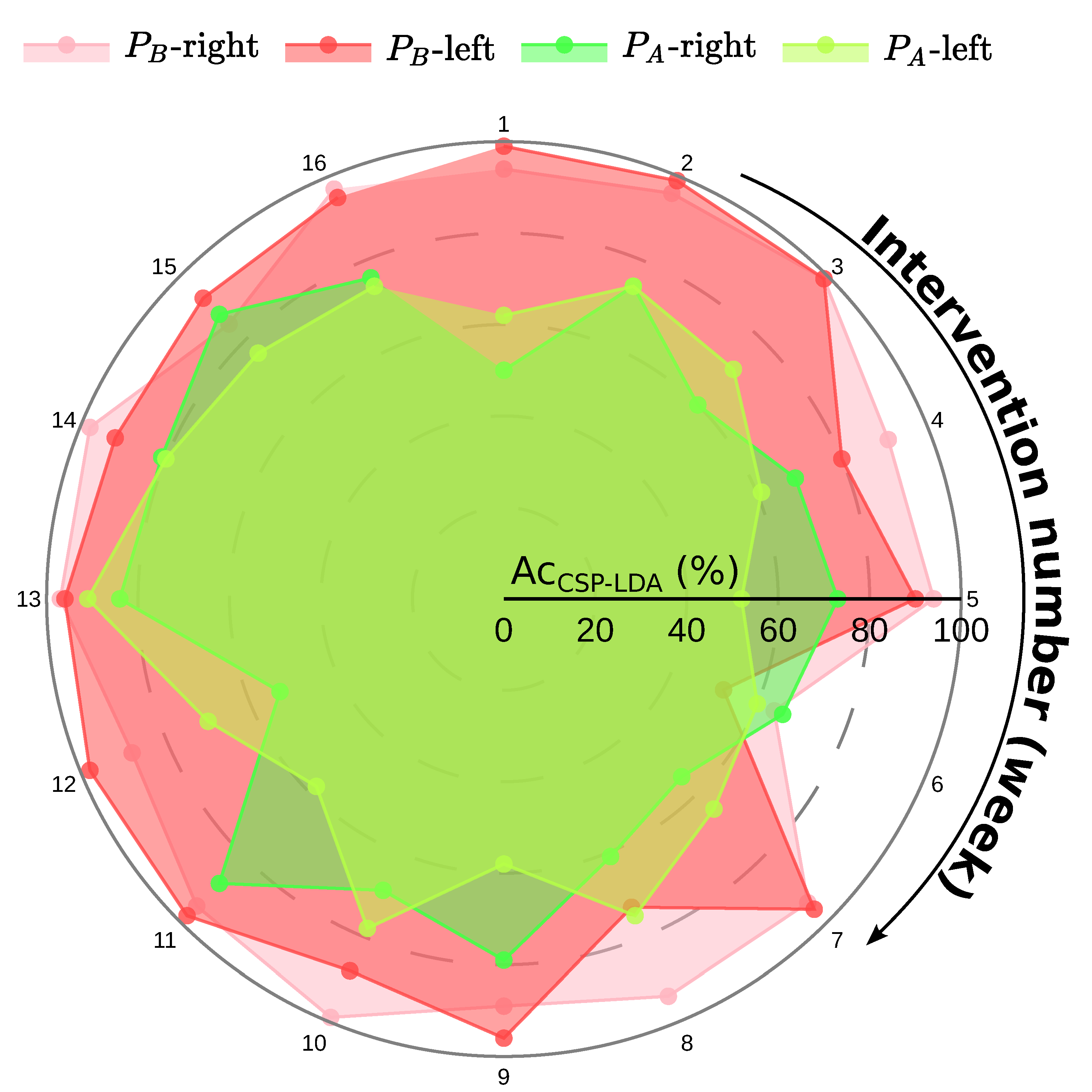
3.1.2. Classifier Accuracy
The
Figure 2 shows the Ac
values (0–100%) of both participants during the sixteen-week period, including the left lower limb (LLL) and right lower limb (RLL). A trend towards improvement in Ac
values was observed during the study period; it can be seen in
Figure 2 that as better values are obtained, more accurate activation signals are sent to the NES
-FES
interface. Nonetheless, high values do not entirely avoid the occurrence of errors during the activation of the FES
, and may not necessarily represent better performance during the intervention.
showed gradual development in the ease of obtaining Ac values. At first, the best Ac results obtained in the first intervention were 61.5% in the LLL and 50% in the RLL. Comparatively, their best results consisted of Ac values of 91% in LLL and 88% in RLL. However, the Ac correlation tests for among all interventions were RLL = = 0.59 (p = 0.02) and LLL = = 0.47 (p = 0.07). The significant moderated correlation output to RLL indicates a learning curve along the interventions that does not statistically occur with LLL.
presented high results from the first intervention that remained high and close for the remainder of the study. He showed an initial Ac of 99% in LLL and 94% in RLL. The best values obtained during the interventions were an Ac of 99% in both lower limbs. However, the Ac correlation tests for among all interventions were RLL = [ = 0.06 (p = 0.80) and LLL = = −0.21 (p = 0.40). These insignificant correlation outputs indicate that the learning curve for did not increase over the interventions. This may be due to the presenting high Ac values beginning with the first intervention.
In the work of Hernandez-Rojas et al. [
10], it was established through several studies on BCIs that Ac
in the range of 60% to 70% represents acceptable performance. Based on these parameters, it is possible to analyze the development presented by the users of the NES
-FES
interface more efficiently by comparing the performance of
and
throughout the course of this study.
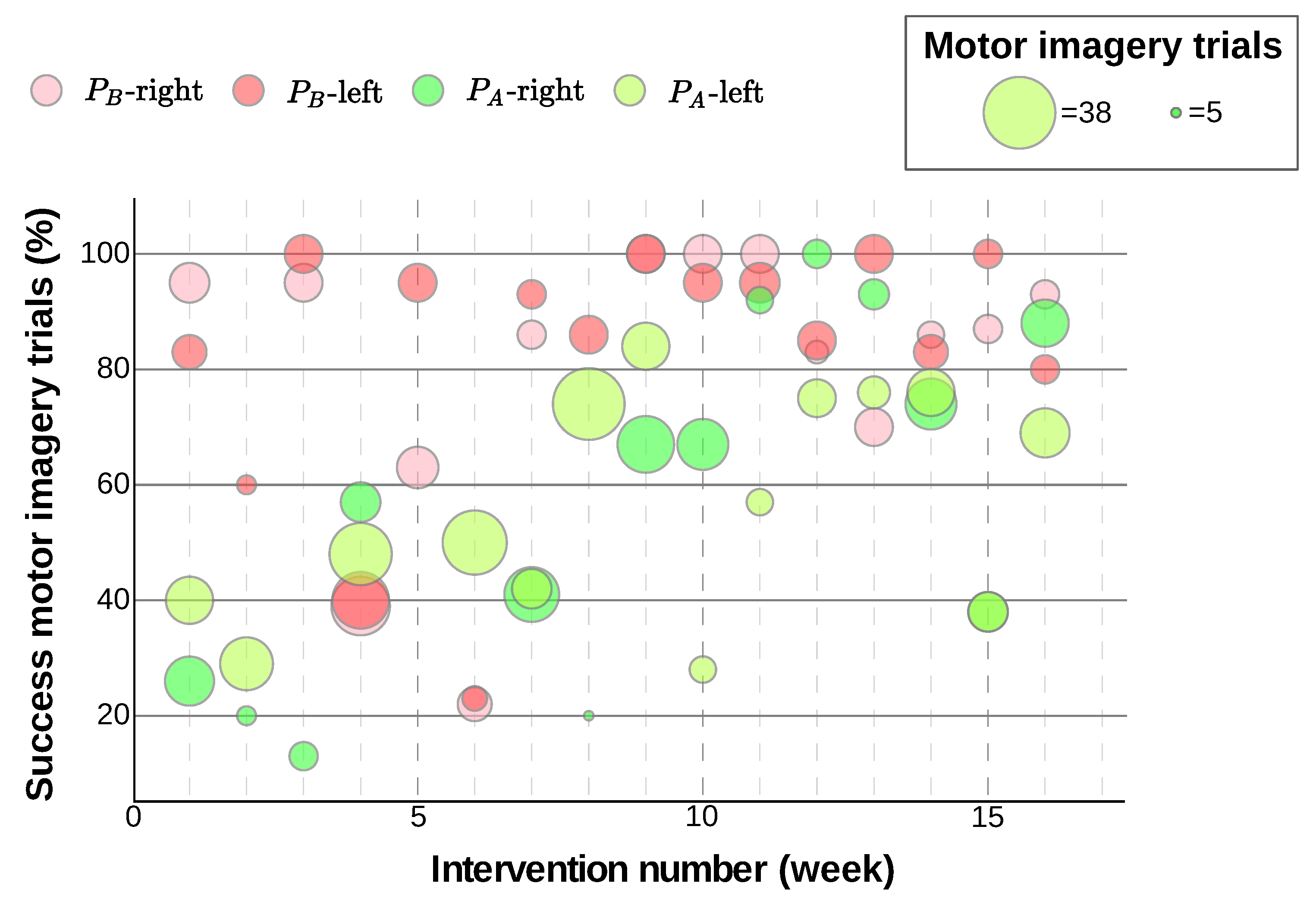
3.1.3. Success Percentage of FES Activation
Figure 3 shows the success percentage of FES
activation throughout the interventions, with larger circles indicating a greater number of attempts. The image shows the improved adaptation of the participants to the methodology with each new session held. In the first interventions, when the participants were adapting to the routine and the instructions, there was a tendency for lower Ac
values to occur, leading to greater errors in the activation of the FES
due to the necessity of repeating the training. Performance gradually improved until reaching a more typical result for each of the participants. In Nenadic’s study [
24] it was found that participants take an average of four to five sessions to achieve their best performance. This suggests that performance may improve over time due to human–computer co-adaptation, and perhaps to other factors such as MI reactivation of dormant cortical areas.
Notably, individual performance varied from time to time due to isolated factors on certain days, such as problems with equipment, concentration, or quality in Ac
capture. Therefore, even in instances where several sessions had been performed and there was a full understanding of the researcher’s instructions, there were interventions in which the participants’ performance was lower than on previous ones. This is corroborated by Liu’s work [
6], in which it was found that the best performance in NES
-FES
interfaces requires long training and a high degree of concentration on the part of participants.
For both participants, it was noticed that a sequence of false positives or omissions in the same period of application of the NES
-FES
interface exponentially affected the performance on that day. In these situations, the participants (especially
) started to show greater anxiety about seeking to improve their results, even when external factors were interfering. The work of Hernandez-Rojas et al. [
10] has a strong relationship with this point, as it highlights the need for the BCI system to be able to minimize the rate of false negatives to avoid frustration on the part of patients when they cannot control the activation of the system. Furthermore, the same study found that the time spent by the BCI system to activate the FES
device varied between 8.43 s and 13.91 s among participants with SCI. This is compatible with situations in which the participants in the present study presented a lower Ac
than usual, which contrasted with the more common situation where the activation of the interface occurred almost instantly. Similar findings were reported by Nenadic [
24] and Liu [
6].
Individually, underwent a gradual improvement, improving from hit percentages of 40% (LLL) and 26% (RLL) in the first intervention to a peak of 84% (LLL) and 100% (RLL). The percentage of successful FES activation correlation tests for among all the interventions were RLL = = 0.40 (p = 0.11) and LLL = = 0.12 (p = 0.65). These insignificant correlation outputs represent that the learning curve does not increase along the interventions compared to the percentage of successful FES activation. , on the other hand, maintained high results, obtaining percentages of 83% (LLL) and 95% (RLL) in the first intervention and reaching a peak of 100% in both lower limbs. The percentage of successful FES activation correlation tests for among all interventions was RLL = = −0.04 (p = 0.88) and LLL = = 0.26 (p = 0.32). These insignificant correlation outputs represent that the learning curve does not increase along the interventions to success percentage of FES activation. It should be noted that for certain interventions shown in the images data collection could not be included due to equipment failure.
3.1.4. Inter-Subject Variability
The differences in performance among the participants illustrate the different elements that can affect the learning curve with this interface.
presented high performance values much more quickly than
, obtaining Ac
greater than 90% in the first interventions, while
needed more than half of the sixteen planned interventions to maintain consistent results above 75%. When questioned,
claimed to know about and use audio related to mindfulness, including the content indicated when beginning the study. Furthermore, compared to
,
could be said to have a more restrained and carefree personality; this may be related to greater focus on instructions and less self-pressure related to better performance [
6].
Our results are consistent with the findings of Behrman et al. [
3] for groups with incomplete SCI, where they found that, in addition to differences in protocol execution, variability in the results may reflect the intrinsic heterogeneity between participants. These individual aspects may be associated with direct consequences of the injury (for example, severity, location, and time of injury, as well as the presence of correlated medications) and personal factors (including personal motivation and family support).
It is possible to notice differences in the methods adopted by the participants in terms of the way they performed the MI.
tried to maintain mindfulness with respect to the lower limbs, while
typically directed vision to a neutral location. This element is related to the work of Rimbert et al. [
25], where it is stated that there is considerable inter-subject and intra-subject variability in the ERD/ERS patterns generated during MI tasks and in interface performances. Considering this, factors such as the nature of the movement or force or the opening and closing of the eyes may influence the modulation of ERD/ERS. Therefore, in the context in which
had an MI pattern that does not include the full visualization of the lower limbs in moments of non-execution of movement, a brief observation of the legs could induce the activation of the NES
-FES
interface [
10].
3.2. Study Limitations
Certain situations observed during the study interfered negatively with the achievement of results during the interventions. Occasional problems with the equipment deserve to be highlighted, such as in the capture of EEG by the OpenVibe software and the activation of the FES
. In this regard, problems in the batteries of the devices involved in the NES
-FES
interface were present more frequently. The efficiency of EEG itself has limitations in the implementation of the interface, as discussed by Nenadic [
24]; although the possibility of highly accurate control in EEG-based BCIs has been demonstrated, the implementation of these systems outside the experimental environment may require very high levels of performance. This is due to possible reading errors, such as omissions or false positives, which were consistent in certain interventions. It is evident that even with greater adaptation to the equipment by the participants, the capture of signals by the EEG is susceptible to both biological and non-biological artifacts due to the low field potential produced by neuronal depolarization and the limitations of the electrodes [
6].
Another important limitation is that this was a pilot study to investigate the use of the NES-FES interface and the learning curve in individuals with complete SCI; we used a limited sample of two participants, which may not reflect all cases. Furthermore, the results obtained in this study were limited to activating the interface only for the selected specific task (MI), and it was not applied to any other tasks.
One of the possible artifacts that can compromise the performance of an EEG-based BCI is the electrical network, which can cause noise in the capture of signals. Therefore, the use of electronic devices with Bluetooth connection and an internet network close to the equipment involved in the intervention was avoided due to risk of reducing the efficiency of MI calibration. The participant’s emotional state at the time of the intervention is another factor that can interfere with the results, either for reasons due to events prior to the intervention or due to frustration at not being able to complete a requested task [
3,
6,
11]. In this aspect, it is important to properly calibrate the system in order to avoid false positive results and prevent frustration on the part of the user [
10].
An final point worth mentioning is the uncertainty regarding the reliability of the data, as there is a possibility of the participants contracting the preserved musculature above the injury level during motor imagery training. However, this would lead to a bias in the capture of signals where the activation of FES would be triggered by the voluntary contraction of this musculature, resulting in inconsistent data values during integration with the interface, as the command needs to come directly from the brain. A possible correction would be the collection of data involved with this accessory movement, which could be correlated with the results to verify the level of interference.
4. Conclusions
Relevant variability was observed between individuals, with differences in the values of Ac, hit rates, and repetition of training. These differences can be explained by both individual factors and factors directly related to the NES-FES interface, with the individual factors being more determinative of the variation in the results for each participant. Among the participants, showed gradual development, presenting initial Ac values of 61.5% (LLL) and 50% (RLL) and reaching high values of 91% (LLL) and 88% (RLL), with statistical correlation only for the RLL. Comparatively, started with good results that remained high, presenting initial Ac of 99% (LLL) and 94% (RLL) and reaching 99% bilaterally, with no statistical correlation. This may be due presenting high Ac values from the first intervention. Regarding the percentage of hits, there was variation over the course of the study, although neither participant showed statistical correlation. had initial values of 40% and 26%, respectively, and reached values of 84% and 100%, while initially presented hit rates of 83% and 95%, and eventually reached 100% bilaterally.
Thus, despite the variations between users, sixteen interventions were sufficient to achieve a good learning effect to control the NES-FES interface for quadriceps femoris muscle activation in the sitting position.
For subsequent studies, our research team is developing a Python® framework in which will make possible:
Integration with other sensors;
Use of accelerometer metrics to avoid movement artifacts from head movement;
Accurate measurement of time spent on FES activation;
Better recognition of false positive FES activations;
Accurate real-time identification of the computational cost of a user performing the most proximal MI task;
Correlation of obtained data with the neuroanatomical autonomous system through cardiac frequency and electrodermal activity.


 ,
, {kind=link}
{kind=link}
{kind=link}


