
Development and Validation of an HPLC Method for the Determination of Meloxicam and Pantoprazole in a Combined Formulation

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Chemicals and Reagents
2.2. Formulation of Tablets
2.3. Instruments
2.4. Preparation of Phosphate Buffer: Acetonitrile (30:70 v/v) Mobile Phase
2.5. Preparation of Stock Solution and Working Solution
2.6. Preparation of Buffer
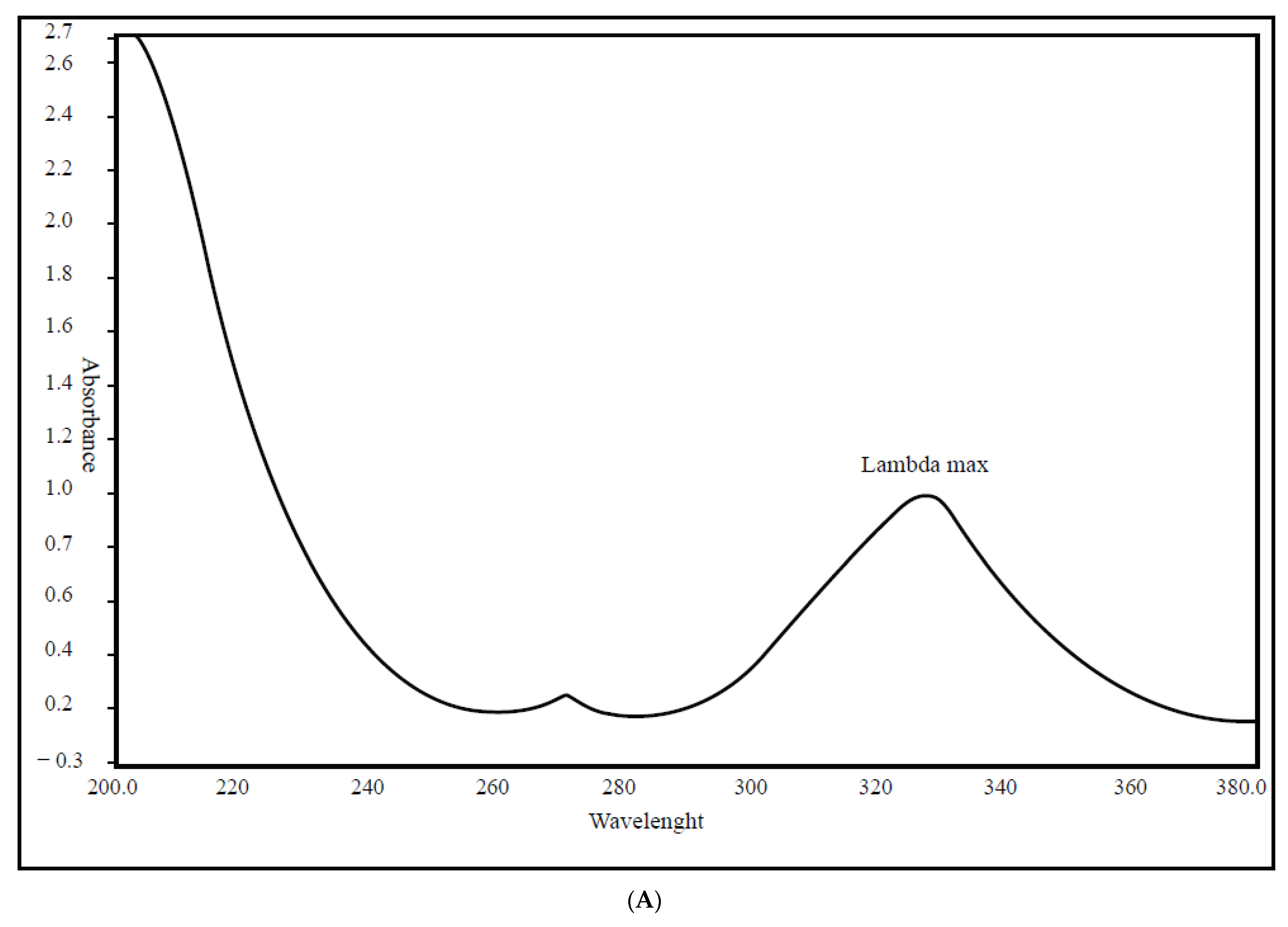
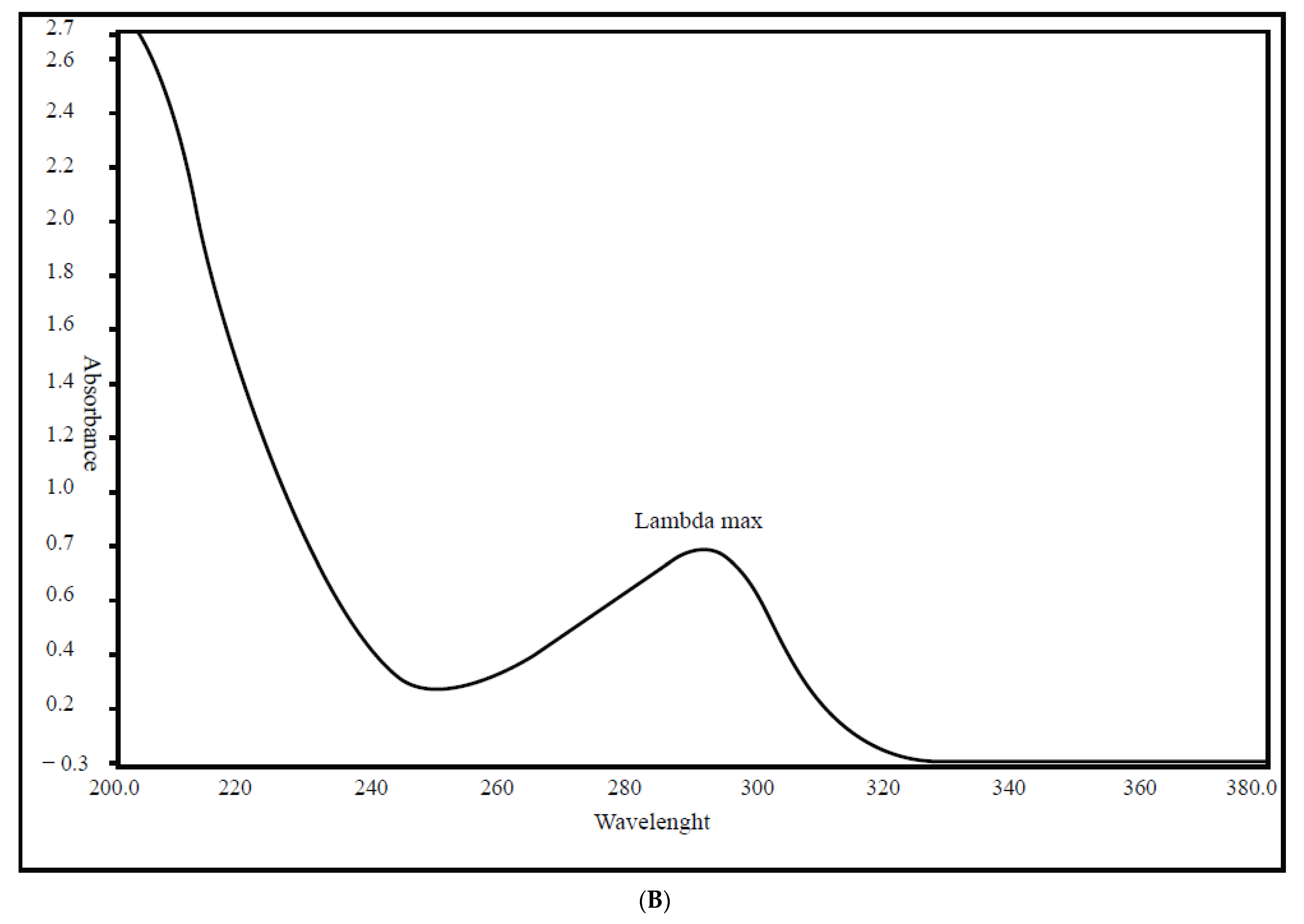
2.7. Wavelength Selection
2.8. Chromatographic Conditions
2.9. Selectivity and Sensitivity Test Preparation
2.10. Linearity Sample Test Preparation
2.11. Preparations for System Precision Test of Samples
2.12. Preparations for Method Precision Test of Samples
2.13. Preparations for Intermediate Precision Tests for Samples
2.14. Preparations for Accuracy Test for Samples
2.15. Recovery Test
2.16. Preparations for Robustness Test
2.16.1. Robustness of the Wavelength (±5 nm)
2.16.2. Robustness of the Temperature (±5 °C)
2.16.3. Robustness of Organic Modified Composition (±5%)
2.16.4. Robustness of Using Different Columns
2.17. Assay Test
2.18. Stability of Preparation for Analytical Solution Test
3. Results and Discussion
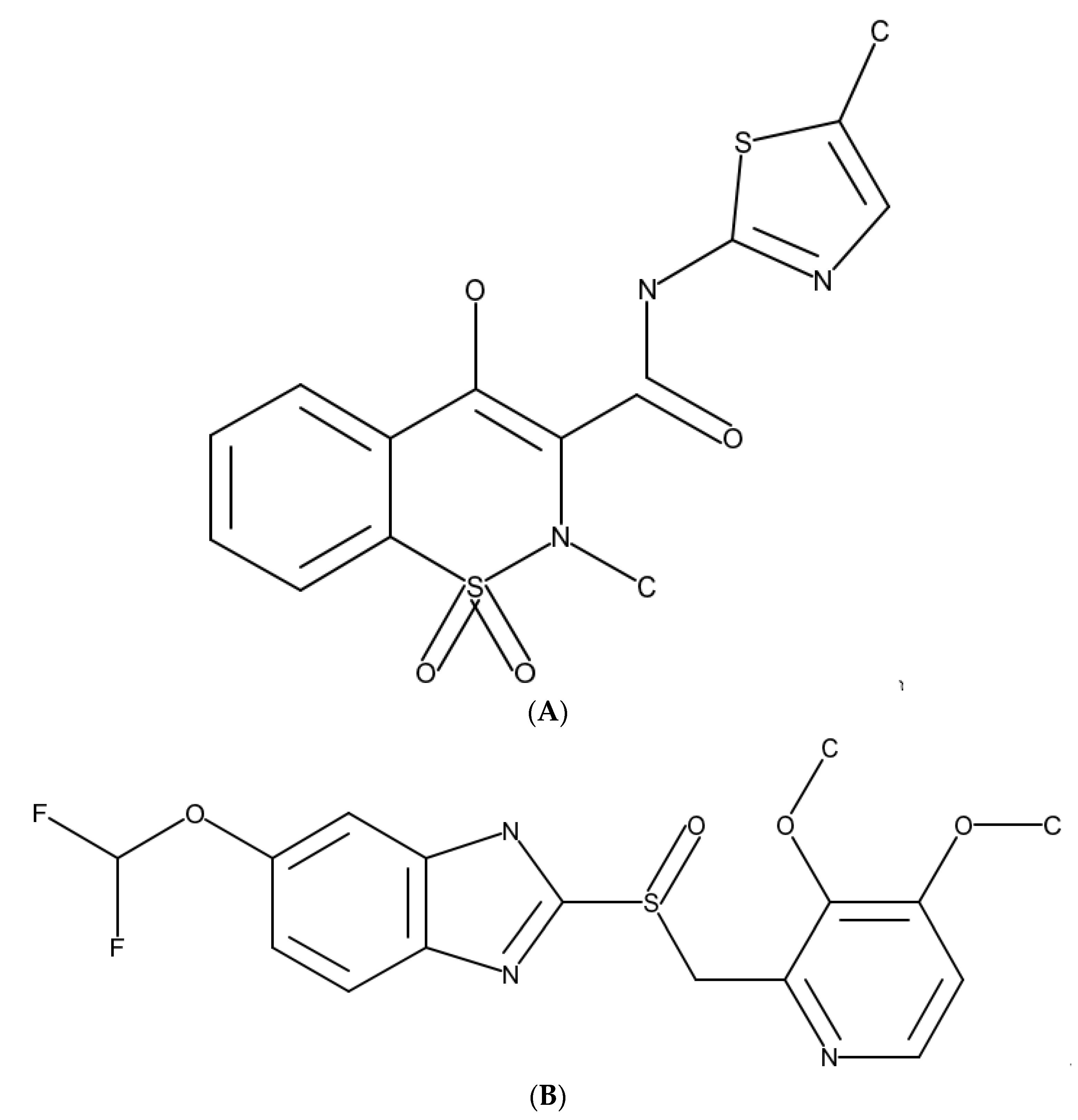
3.1. Identification and Compatibility
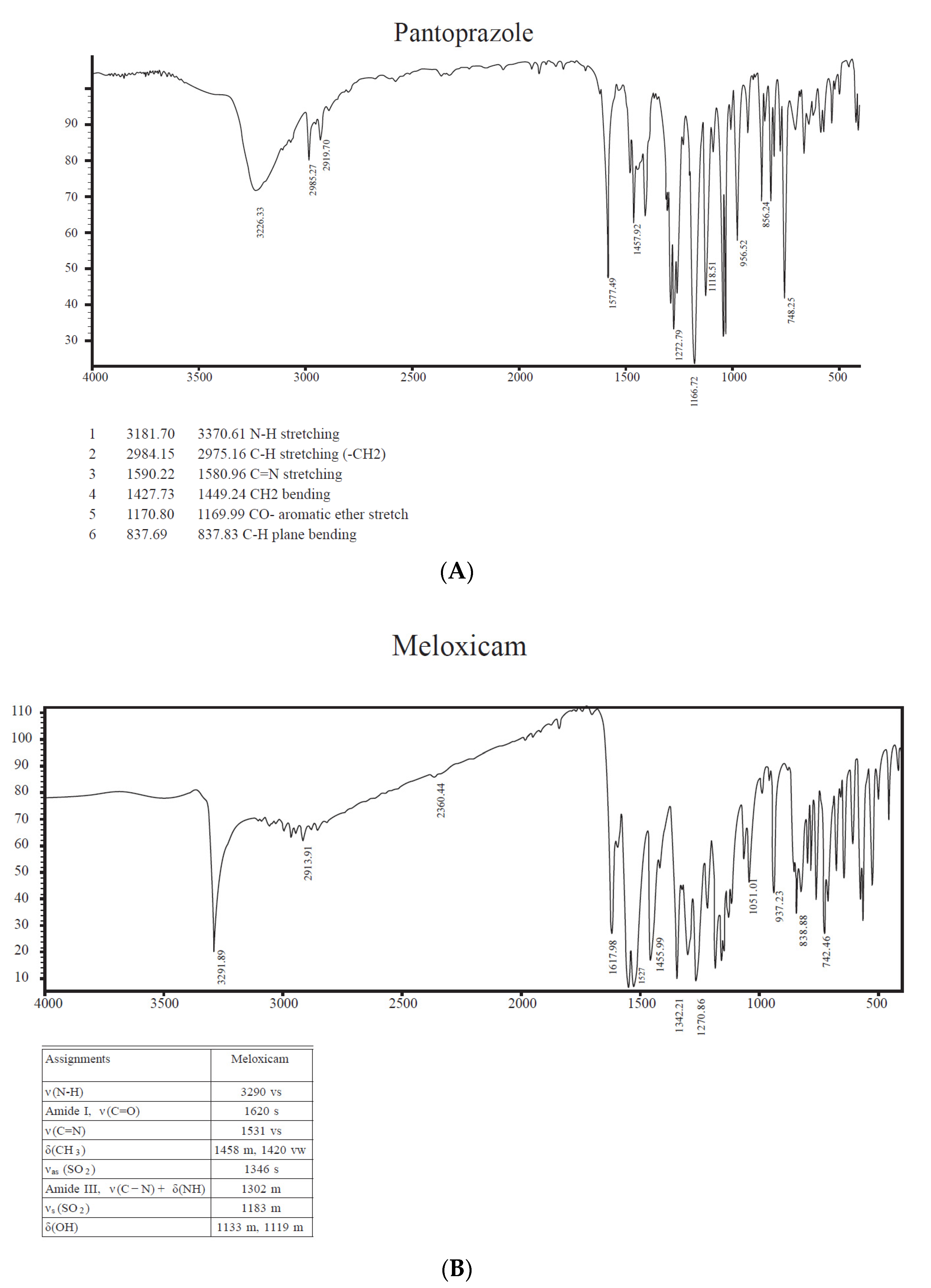
3.2. FTIR of Pantoprazole and Meloxicam
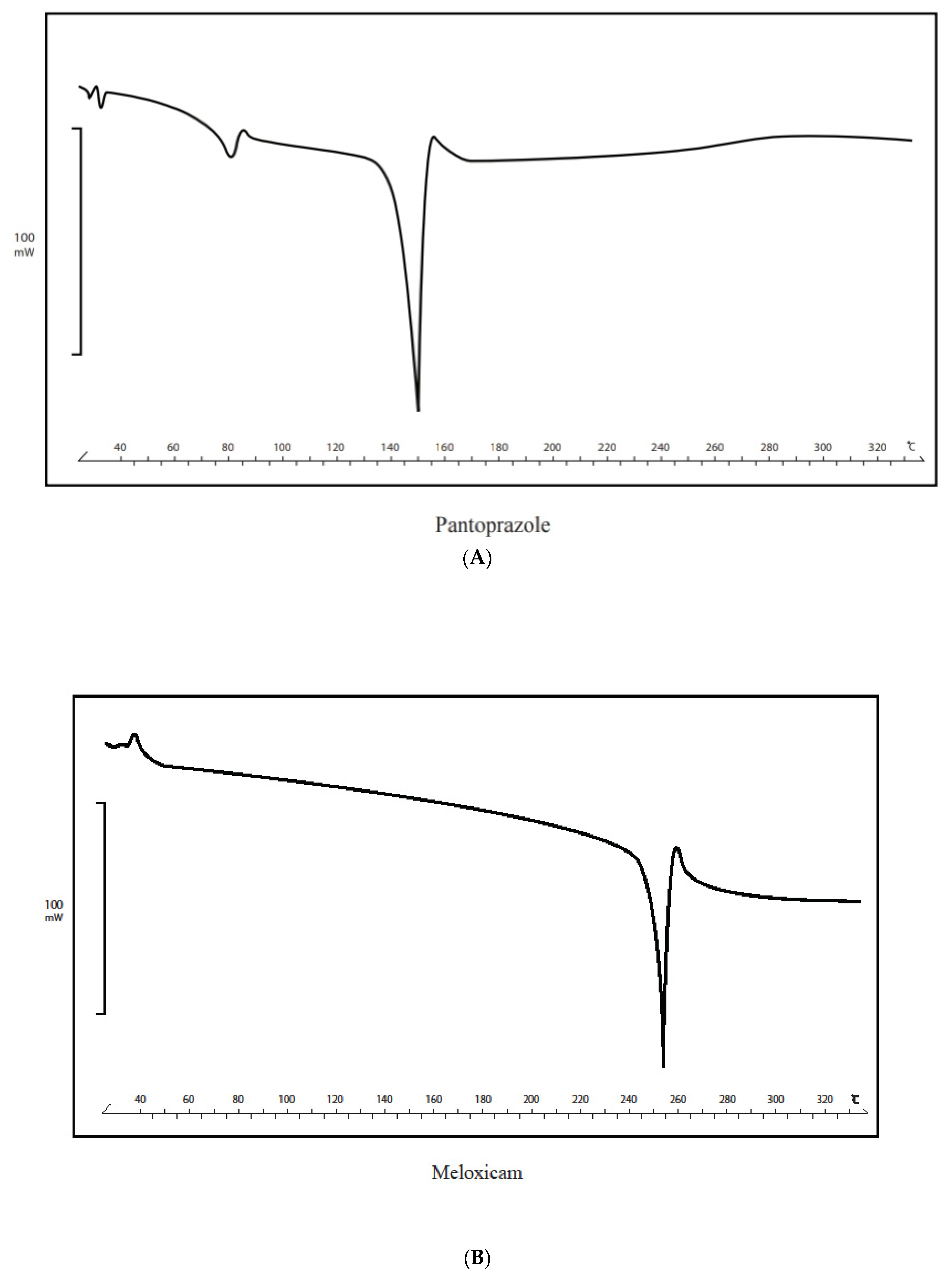
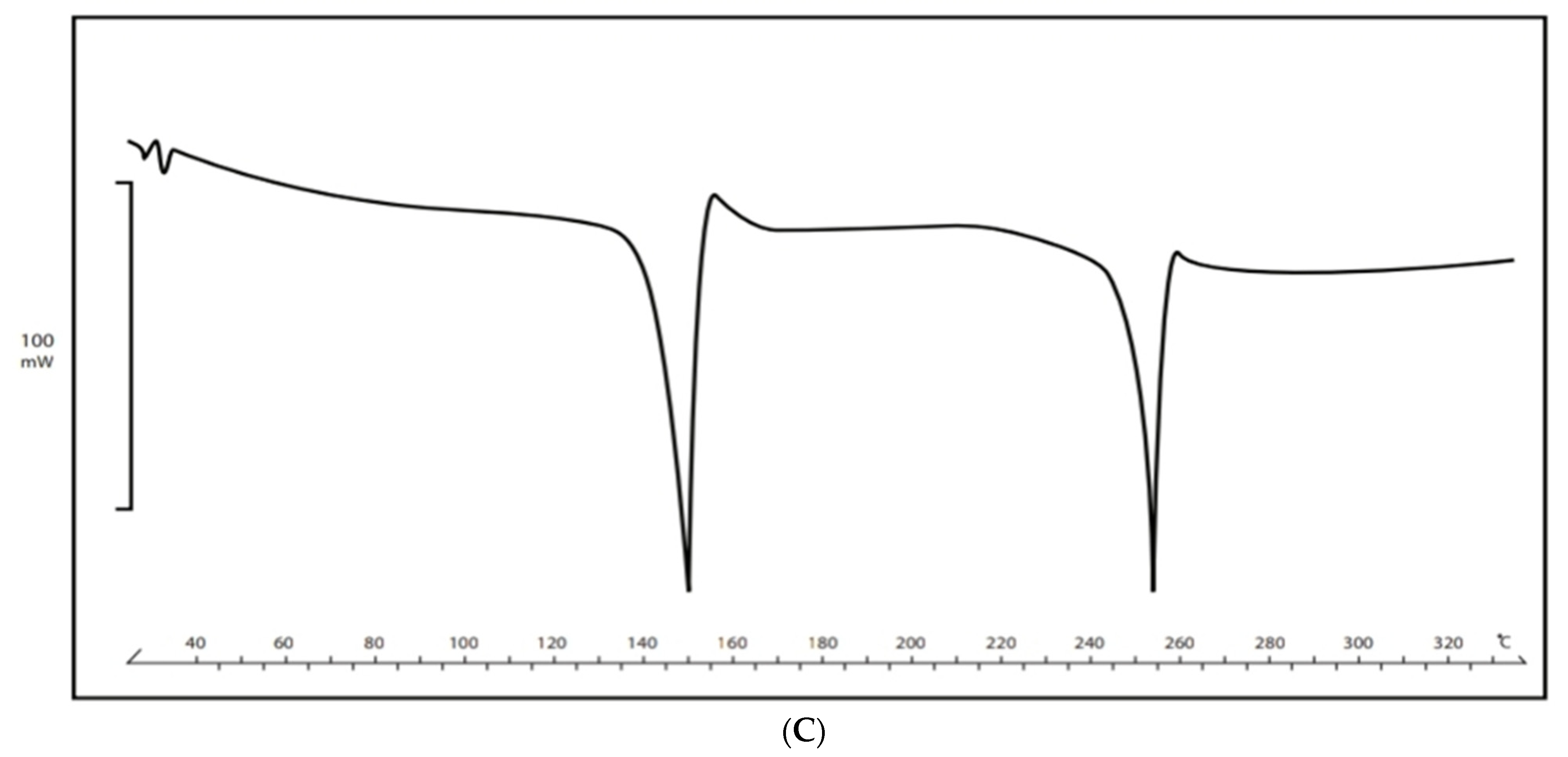
3.3. DSC of Pantoprazole and Meloxicam
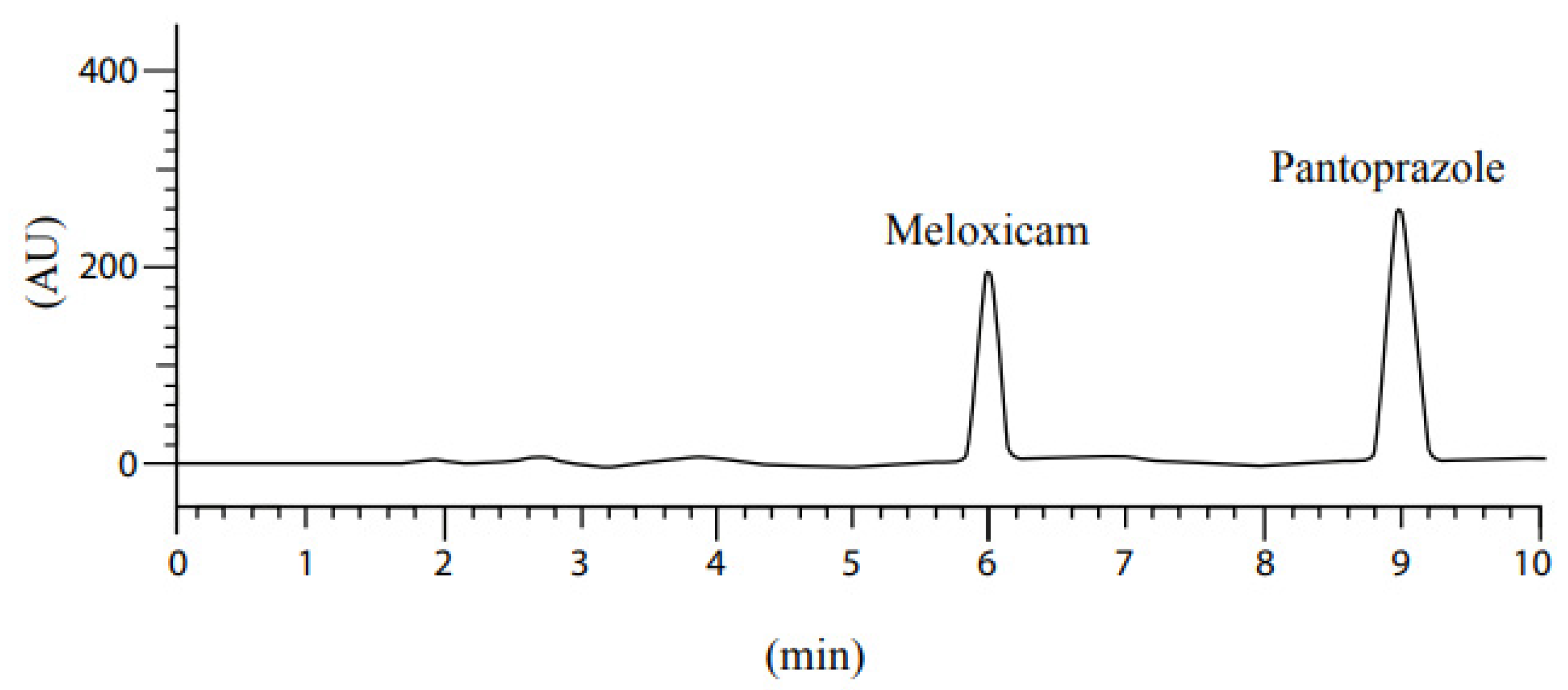
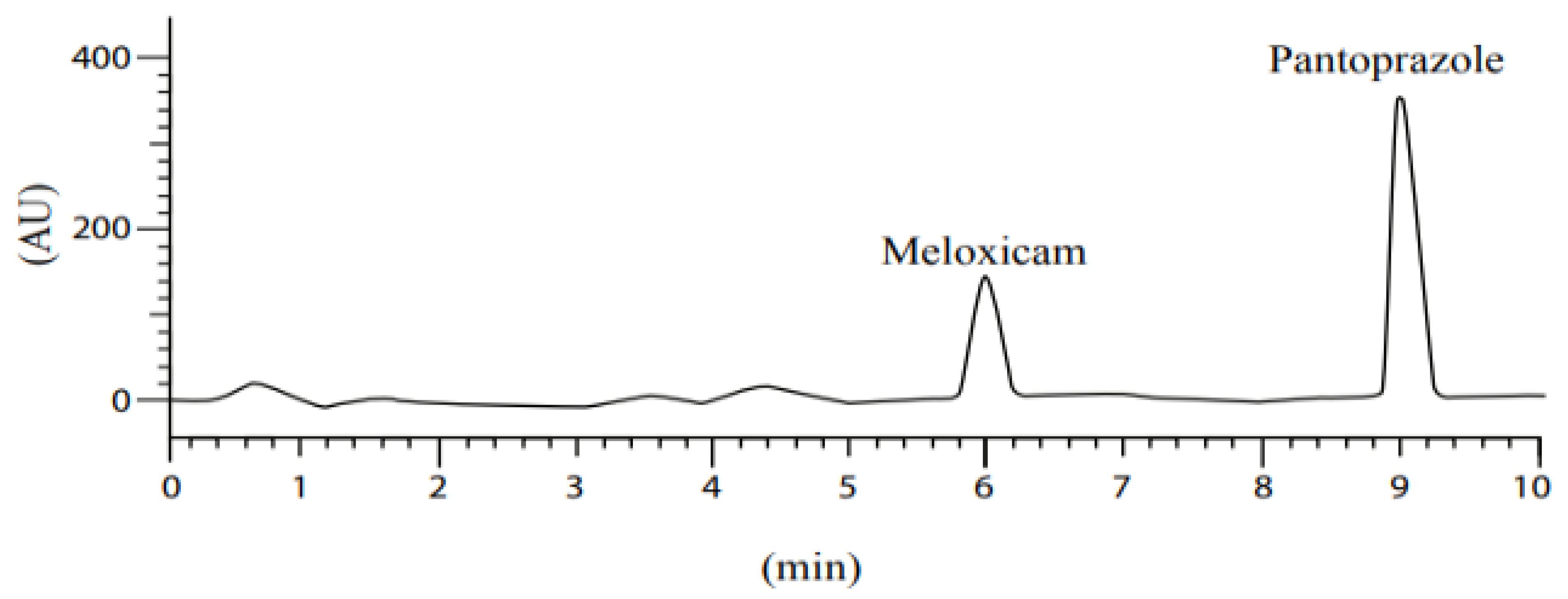
3.4. Selectivity
3.5. Linearity and Range
3.6. System Precision
3.7. Method Precision
3.8. Intermediate Precision
3.9. Recovery “Accuracy”
3.10. Robustness
3.11. Assay Test
4. Dissolution
Stability of Drugs in Analytical Solution
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gunaydin, C.; Bilge, S.S. Effects of Nonsteroidal Anti-Inflammatory Drugs at the Molecular Level. Eurasian, J. Med. 2018, 50, 116. [Google Scholar] [CrossRef] [PubMed]
- Osafo, N.; Agyare, C.; Obiri, D. Mechanism of action of nonsteroidal anti-inflammatory drugs. Anti-Inflamm. Drugs 2017, 18, 120–121. [Google Scholar]
- Perrone, G.M.; Scilimati, A.; Simone, L.; Vitale, P. Selective COX-1 Inhibition: A Therapeutic Target to be Reconsidered. Curr. Med. Chem. 2010, 17, 3769–3805. [Google Scholar] [CrossRef] [PubMed]
- Singh, G. NSAID induced gastrointestinal complications: The ARAMIS perspective–1997. Arthritis, Rheumatism, and Aging Medical Information System. J. Rheumatol. Suppl. 1998, 25, 8–16. [Google Scholar]
- Castellsague, J.; Riera-Guardia, N.; Calingaert, B.; Varas-Lorenzo, C.; Fourrier-Reglat, A.; Nicotra, F.; Sturkenboom, M.; Perez-Gutthann, S. Individual NSAIDs and Upper Gastrointestinal Complications. Drug Saf. 2012, 35, 1127–1146. [Google Scholar] [CrossRef]
- Chi, T.-Y.; Zhu, H.-M.; Zhang, M. Risk factors associated with nonsteroidal anti-inflammatory drugs (NSAIDs)-induced gastrointestinal bleeding resulting on people over 60 years old in Beijing. Medicine 2018, 97, 18. [Google Scholar] [CrossRef]
- Richardson, P.; Hawkey, C.J.; Stack, W.A. Proton Pump Inhibitors. Drugs 1998, 65, 30–335, Erratum in Drugs 2012, 56, 30–335. [Google Scholar] [CrossRef]
- Dellon, E.S.; Speck, O.; Woodward, K.; Covey, S.; Rusin, S.; Gebhart, J.H.; Chen, X.; Woosley, J.T.; Shaheen, N.J. Markers of eosinophilic inflammation for diagnosis of eosinophilic esophagitis and proton pump inhibitor-responsive esophageal eosinophilia: A prospective study. Clin. Gastroenterol. Hepatol. 2014, 12, 2015–2022. [Google Scholar] [CrossRef] [Green Version]
- Long, J.D.; Orlando, R.C. Nonerosive reflux disease: A pathophysiologic perspective. Curr. Gastroenterol. Rep. 2008, 10, 200–207. [Google Scholar] [CrossRef]
- Sandhu, D.S.; Fass, R. Current Trends in the Management of Gastroesophageal Reflux Disease. Gut Liver 2018, 12, 7–16. [Google Scholar] [CrossRef] [Green Version]
- Khan, M.A.; Howden, C.W. The Role of Proton Pump Inhibitors in the Management of Upper Gastrointestinal Disorders. Gastroenterol. Hepatol. 2018, 14, 169. [Google Scholar]
- McCarthy, D.M.; Olinger, E.J.; May, R.J.; Long, B.W.; Gardner, J.D. H2-Histamine receptor blocking agents in the Zollinger-Ellison syndrome. Experience in seven cases and implications for long-term therapy. Ann. Intern. Med. 1977, 87, 668–675. [Google Scholar] [CrossRef] [PubMed]
- Pinto-Sanchez, M.I.; Yuan, Y.; Hassan, A.; Bercik, P.; Moayyedi, P.; Group CUG and PD. Proton pump inhibitors for functional dyspepsia. Cochrane Database Syst. Rev. 2017, 2017, 1–75. [Google Scholar]
- Smoot, D.T. How does Helicobacter pylori cause mucosal damage? Direct mechanisms. Gastroenterology 1997, 113, S31–S34. [Google Scholar] [CrossRef]
- Sreedhar, D.; Subramanian, G.; Udupa, N. Combination drugs: Are they rational? Curr. Sci. 2006, 91, 343–354. [Google Scholar]
- World Health Organization. Guidelines for Registration of Fixed-Dose Combination Medicinal Products; WHO Technical Report Series; No. 929; WHO Headquarters: Geneva, Switzerland, 2005; pp. 95–141. [Google Scholar]
- Walton, S.; Mclaughlin, T.; Kruzikas, D. Gastroenterology undefined, and undefined. Impact of adherence to concomitant gastroprotective therapy on nonsteroidal-related gastroduodenal ulcer complications. Clin. Gastroenterol. Hepatol. 2006, 4, 1337–1345. [Google Scholar]
- Cox, S.; Hayes, J.; Yarbrough, J.; Veiga-Parga, T.; Greenacre, C. High-Performance Liquid Chromatography Determination of Meloxicam and Piroxicam with Ultraviolet Detection. Chromatogr. Res. Int. 2014, 2014, 1–7. [Google Scholar] [CrossRef]
- Zhang, H.; Choi, H.K. Analysis of meloxicam by high-performance liquid chromatography with cloud-point extraction. Anal. Bioanal. Chem. 2008, 392, 947–953. [Google Scholar] [CrossRef]
- Bae, J.W.; Kim, M.J.; Jang, C.G.; Lee, S.Y. Determination of meloxicam in human plasma using a HPLC method with UV detection and its application to a pharmacokinetic study. J. Chromatography. B Anal. Technol. Biomed. Life Sci. 2007, 859, 69–73. [Google Scholar] [CrossRef]
- Miyamoto, A.; Aoyama, T.; Matsumoto, Y. The Measurement of Meloxicam and Meloxicam Metabolites in Rat Plasma Using a High-Performance Liquid Chromatography-Ultraviolet Spectrophotometry Method. Chem. Pharm. Bull. 2017, 65, 121–126. [Google Scholar] [CrossRef] [Green Version]
- Velpandian, T.; Jaiswal, J.; Bhardwaj, R.K.; Gupta, S.K. Development and validation of a new high-performance liquid chromatographic estimation method of meloxicam in biological samples. J. Chromatography. B Biomed. Sci. Appl. 2000, 738, 431–436. [Google Scholar] [CrossRef]
- Ashour, S.; Omar, S. A modified high-performance liquid chromatographic method for the analysis of pantoprazole sodium in pharmaceutical dosage forms using lansoprazole as internal standard. Arab. J. Chem. 2016, 9, S114–S119. [Google Scholar] [CrossRef] [Green Version]
- Patel, B.H.; Suhagia, B.N.; Patel, M.M.; Patel, J.R. Simultaneous estimation of pantoprazole and domperidone in pure powder and a pharmaceutical formulation by high-perfomance liquid chromatography and high-performance thin-layer chromatography methods. J. AOAC Int. 2007, 90, 142–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Sherif, Z.A.; Mohamed, A.O.; El-Bardicy, M.G.; El-Tarras, M.F. Reversed-phase high performance liquid chromatographic method for the determination of lansoprazole, omeprazole and pantoprazole sodium sesquihydrate in presence of their acid-induced degradation products. Chem. Pharm. Bull. 2006, 54, 814–818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Letica, J.; Marković, S.; Zirojević, J.; Nikolić, K.; Agbaba, D. High-performance liquid chromatographic determination of pantoprazole and its main impurities in pharmaceuticals. J. AOAC Int. 2010, 93, 1121–1128. [Google Scholar] [CrossRef] [Green Version]
- Habash, I.W.; Al-Shdefat, R.I.; Hailat, M.M.; Dayyih, W.A. A stability indicating rp-hplc method development for simultaneous estimation of alogliptin, pioglitazone, and metformin in pharmaceutical formulations. Acta Pol. Pharm. Drug Res. 2020, 77, 549–562. [Google Scholar] [CrossRef]
- Hailat, M.; Al-Ani, I.; Hamad, M.; Zakareia, Z.; Dayyih, W.A. Development and Validation of a Method for Quantification of Favipiravir as COVID-19 Management in Spiked Human Plasma. Molecules 2021, 26, 3789. [Google Scholar] [CrossRef]
- Alkather, Z.; Hailat, M.; Al-Shdefat, R.; Abu Dayyih, W. Development and Validation of HPLC Method for Five Gliptins in Pharmaceutical Dosage Forms in Finished Marketed Products. Curr. Pharm. Anal. 2020, 17, 1263–1271. [Google Scholar] [CrossRef]
- Al-Shdefat, R.; Hailat, M.; Kharshid, A.M.; Saadh, M.J.; Hamed, M.F.; Answer, M.K.; Abdel-Halim, H.; Dayyih, W.A. Evidence of human metabolites of omeprazole and its structure elucidation by using HPLC-MS. J. Mol. Struct. 2021, 1230, 129902. [Google Scholar] [CrossRef]
- Sunoqrot, S.; Alfaraj, M.; Hammad, A.M.; Kasabri, V.; Shalabi, D.; Deeb, A.A.; Ibrahim, L.H.; Shnewer, K.; Yousef, I. Development of a Thymoquinone Polymeric Anticancer Nanomedicine through Optimization of Polymer Molecular Weight and Nanoparticle Architecture. Pharmaceutics 2020, 12, 811. [Google Scholar] [CrossRef]
- Jain, D.K.; Jain, N.; Charde, R. The RP-HPLC method for simultaneous estimation of esomeprazole and naproxen in binary combination. Pharm. Methods 2011, 2, 167–172. [Google Scholar] [CrossRef] [Green Version]
- Mohideen, S.; Shivakanth, M.; Sureshkumar, P.; Krishnan, S.N.; Surendranath, Y.; Satyanarayana, T. Development and validation of analytical method for naproxen and pantoprazole in capsule dosage form. Int. J. PharmTech Res. 2011, 3, 1169–1173. [Google Scholar]
- Kumar, R.S.; Sree, U.G.; Malleswara Babu, N.B. A RP-HPLC Method Development and Its Validation for the Simultaneous Estimation of Naproxen and Pantoprazole Sodium in Capsule Dosage Form. Asian J. Res. Chem 2013, 6, 155–168. [Google Scholar]
- ICH. ICH Official Website: ICH Quality Guidelines. Available online: https://www.ich.org/page/quality-guidelines (accessed on 16 May 2020).
- Nasef, A.M.; Gardouh, A.R.; Ghorab, M.M. Formulation and in-vitro evaluation of pantoprazole loaded pH-sensitive polymeric nanoparticles. Future J. Pharm. Sci. 2017, 3, 103–117. [Google Scholar] [CrossRef]
- Pathak, D.; Dahiya, S.; Pathak, K. Solid dispersion of meloxicam: Factorially designed dosage form for geriatric population. Acta Pharm. 2008, 58, 99–110. [Google Scholar] [CrossRef] [PubMed]
- Abd Elbary, A.; Ali, A.A.; Aboud, H.M. Enhanced dissolution of meloxicam from orodispersible tablets prepared by different methods. Bull. Fac. Pharm. Cairo Univ. 2012, 50, 89–97. [Google Scholar] [CrossRef] [Green Version]
- Ahmad, R.; Hailat, M.; Jaber, M.; Alkhawaja, B.; Rasras, A.; Al-Shdefat, R.; Abu Dayyih, W. RP-HPLC Method Development for Simultaneous Estimation of Empagliflozin, Pioglitazone, and Metformin in Bulk and Tablet Dosage Forms. Acta Pol. Pharm. Drug Res. 2021, 78, 305–315. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| The Final Concentrations (mg/L) of the Meloxicam in the Working Solutions | The Final Concentrations (mg/L) of the Pantoprazole in the Working Solutions | |
|---|---|---|
| Cal1 | 0.01 | 0.01 |
| Cal2 | 1 | 1 |
| Cal3 | 10 | 10 |
| Cal4 | 40 | 40 |
| Cal5 | 80 | 80 |
| Cal6 | 120 | 120 |
| Cal7 | 200 | 200 |
| Column | Column: ACE C8—(250 mm × 4.6 mm), Particle Size: 5 µm |
|---|---|
| Mobile phase | phosphate buffer: acetonitrile, (30:70 v/v), adjusted to pH 3.4 |
| Detection | wavelength: 310 nm |
| Injection volume | 20 µL |
| Flow rate | 1.0 mL per min |
| Oven temperature | 25 °C |
| Parameters | Pantoprazole | Meloxicam |
|---|---|---|
| Average area of 10 injections | 110,784.9 | 68,005.2 |
| RSD% | 0.02 | 0.02 |
| Asymmetry | 1 | 1 |
| Theoretical plates | 8754 | 8754 |
| Resolution | 5.6 | 5.6 |
| Initial retention time | 8.8 min | 5.9 min |
| Final retention time | 9.1 min | 6.1 min |
| Intra-Day | |||||
|---|---|---|---|---|---|
| Sample ID | Area | Conc Tctual (mg/L) | Conc Theoretical (mg/L) | Accuracy | RSD% |
| Sample 1 | 265,564 | 10.0 | 10.0 | 100 | 0.8 |
| Sample 2 | 263,485 | 9.9 | 10.0 | 99 | |
| Sample 3 | 264,554 | 9.9 | 10.0 | 99 | |
| Sample 4 | 266,485 | 10.0 | 10.0 | 100 | |
| Sample 5 | 265,654 | 10.0 | 10.0 | 100 | |
| Sample 6 | 260,456 | 9.8 | 10.0 | 98 | |
| Intra-Day | |||||
|---|---|---|---|---|---|
| Sample ID | Area | Conc Tctual (mg/L) | Conc Theoretical (mg/L) | Accuracy | RSD% |
| Sample 1 | 194,555 | 14.9 | 15 | 100 | 0.9 |
| Sample 2 | 195,456 | 15.0 | 15 | 100 | |
| Sample 3 | 192,656 | 14.8 | 15 | 99 | |
| Sample 4 | 193,541 | 14.9 | 15 | 99 | |
| Sample 5 | 197,621 | 15.2 | 15 | 101 | |
| Sample 6 | 195,265 | 15.0 | 15 | 100 | |
| Inter-Day | |||||
|---|---|---|---|---|---|
| Sample ID | Area | Conc Actual (mg/L) | Conc Theoretical (mg/L) | Accuracy | RSD% |
| Sample 1 | 2,640,556 | 101.9 | 100.0 | 102 | 1.2 |
| Sample 2 | 2,694,546 | 104.0 | 100.0 | 104 | |
| Sample 3 | 2,675,845 | 103.3 | 100.0 | 103 | |
| Sample 4 | 2,606,412 | 100.6 | 100.0 | 101 | |
| Sample 5 | 2,657,621 | 102.6 | 100.0 | 103 | |
| Sample 6 | 2,645,881 | 102.1 | 100.0 | 102 | |
| Inter-Day | |||||
|---|---|---|---|---|---|
| Sample ID | Area | Conc Actual (mg/L) | Conc Theoretical (mg/L) | Accuracy | RSD% |
| Sample 1 | 1,946,738 | 152.0 | 150 | 101 | 0.9 |
| Sample 2 | 1,934,376 | 151.0 | 150 | 101 | |
| Sample 3 | 1,956,466 | 152.7 | 150 | 102 | |
| Sample 4 | 1,978,456 | 154.5 | 150 | 103 | |
| Sample 5 | 1,945,532 | 151.9 | 150 | 101 | |
| Sample 6 | 1,976,455 | 154.3 | 150 | 103 | |
| Sample ID | Area | Conc.Actual (mg/L) | Conc.Theoretical (mg/L) | Accuracy | Av. | Precision |
|---|---|---|---|---|---|---|
| Recovery pantoprazole 70% Sample 1 | 1,844,645 | 71.1 | 70.0 | 102 | 100.90 | 0.6 |
| Recovery pantoprazole 70% Sample 2 | 1,825,475 | 70.4 | 70.0 | 101 | ||
| Recovery pantoprazole 70% Sample 3 | 1,827,645 | 70.4 | 70.0 | 101 | ||
| Recovery pantoprazole 100% Sample 1 | 2,658,531 | 102.6 | 100.0 | 103 | 101.25 | 0.8 |
| Recovery pantoprazole 100% Sample 2 | 2,668,650 | 103.0 | 100.0 | 103 | ||
| Recovery pantoprazole 100% Sample 3 | 2,698,456 | 104.2 | 100.0 | 104 | ||
| Recovery pantoprazole 130% Sample 1 | 2,414,379 | 131.9 | 130.0 | 101 | 101.72 | 0.2 |
| Recovery pantoprazole 130% Sample 2 | 3,425,903 | 132.3 | 130.0 | 102 | ||
| Recovery pantoprazole 130% Sample 3 | 3,430,673 | 132.5 | 130.0 | 102 | ||
| Recovery of meloxicam 70% Sample 1 | 1,364,371 | 106.4 | 105.0 | 101 | 100.70 | 0.7 |
| Recovery of meloxicam 70% Sample 2 | 1,355,417 | 105.7 | 105.0 | 101 | ||
| Recovery of meloxicam 70% Sample 3 | 1,346,880 | 105.1 | 105.0 | 100 | ||
| Recovery of meloxicam 100% Sample 1 | 1,859,574 | 145.2 | 150.0 | 97 | 99.83 | 2.7 |
| Recovery of meloxicam 100% Sample 2 | 1,956,642 | 152.7 | 150.0 | 102 | ||
| Recovery of meloxicam 100% Sample 3 | 1,938,548 | 151.3 | 150.0 | 101 | ||
| Recovery of meloxicam 130% Sample 1 | 2,503,437 | 195.5 | 195.0 | 100 | 100.66 | 0.6 |
| Recovery of meloxicam 130% Sample 2 | 2,529,535 | 197.6 | 195.0 | 101 | ||
| Recovery of meloxicam 130% Sample 3 | 2,506,984 | 195.8 | 195.0 | 100 |
| Sample ID | Area | Symmetry | Theoretical Plate |
|---|---|---|---|
| Pantoprazole + 5% Organic solvent | 263,309 | 1.01 | 2754 |
| Pantoprazole − 5% Organic solvent | 268,299 | 1.01 | 2754 |
| Pantoprazole + 5 nm (315 nm) | 266,598 | 1.01 | 2744 |
| Pantoprazole − 5 nm (305 nm) | 259,165 | 1.01 | 2764 |
| Pantoprazole-Column 1 | 264,374 | 1.01 | 2743 |
| Pantoprazole-Column 2 | 263,334 | 1.01 | 2718 |
| Pantoprazole 30 C | 267,545 | 1.01 | 2776 |
| Meloxicam + 5% Organic solvent | 198,895 | 1.01 | 2754 |
| Meloxicam − 5% Organic solvent | 197,574 | 1.01 | 2754 |
| Meloxicam + 5 nm (315 nm) | 199,760 | 1.01 | 2744 |
| Meloxicam − 5 nm (305 nm) | 201,534 | 1.01 | 2764 |
| Meloxicam-Column 1 | 208,696 | 1.01 | 2743 |
| Meloxicam-Column 2 | 201,531 | 1.01 | 2718 |
| Meloxicam 30 C | 207,521 | 1.01 | 2776 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahmad, R.; Hailat, M.; Zakaraya, Z.; Al Meanazel, O.; Abu Dayyih, W. Development and Validation of an HPLC Method for the Determination of Meloxicam and Pantoprazole in a Combined Formulation. Analytica 2022, 3, 161-177. https://doi.org/10.3390/analytica3020012
Ahmad R, Hailat M, Zakaraya Z, Al Meanazel O, Abu Dayyih W. Development and Validation of an HPLC Method for the Determination of Meloxicam and Pantoprazole in a Combined Formulation. Analytica. 2022; 3(2):161-177. https://doi.org/10.3390/analytica3020012
Chicago/Turabian StyleAhmad, Raneem, Mohammad Hailat, Zainab Zakaraya, Osaid Al Meanazel, and Wael Abu Dayyih. 2022. "Development and Validation of an HPLC Method for the Determination of Meloxicam and Pantoprazole in a Combined Formulation" Analytica 3, no. 2: 161-177. https://doi.org/10.3390/analytica3020012
APA StyleAhmad, R., Hailat, M., Zakaraya, Z., Al Meanazel, O., & Abu Dayyih, W. (2022). Development and Validation of an HPLC Method for the Determination of Meloxicam and Pantoprazole in a Combined Formulation. Analytica, 3(2), 161-177. https://doi.org/10.3390/analytica3020012