The Relationship between Mindfulness and Sleep Quality is Mediated by Emotion Regulation



Abstract
:1. Introduction
1.1. Homeostasis: The Circadian Drive
1.2. Sleep Quality, Mental Health, and Emotion
1.3. Mindfulness and Emotion Regulation
1.4. Emotion Regulation and Sleep Quality
1.5. Coping: Intrusiveness, Avoidance, Arousal, and Sleep Quality
1.6. Mindfulness and Sleep Quality
1.7. Mindfulness and Emotion
1.8. Emotion Regulation and Sleep
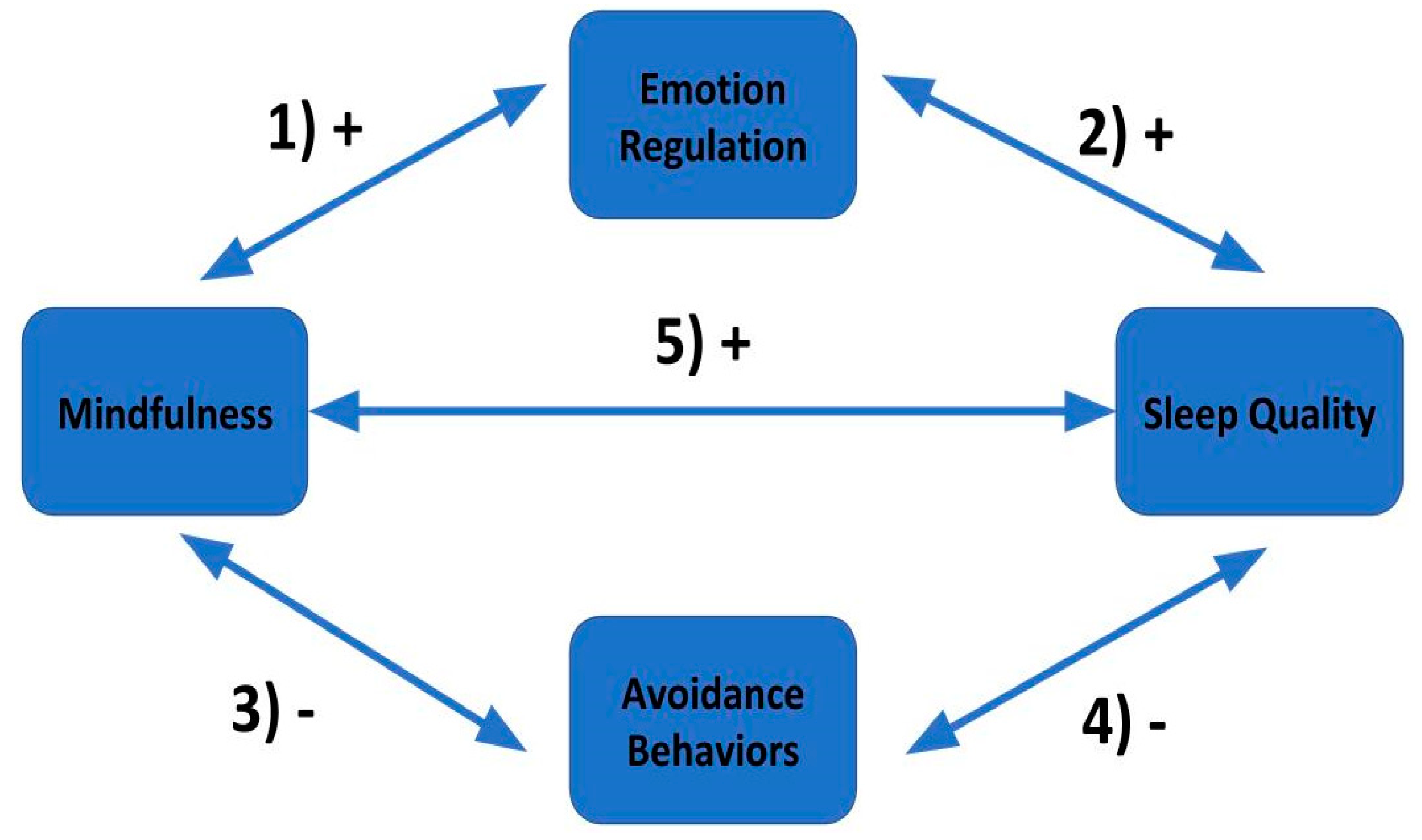
1.9. Hypotheses
2. Participants, Materials, and Procedure
2.1. Participants
2.2. Materials
2.2.1. Pittsburgh Sleep Quality Index (PSQI)
2.2.2. Cognitive and Affective Mindfulness Scale (CAMS-R)
2.2.3. Five Facet Mindfulness Questionnaire (FFMQ)
2.2.4. Impact of Event Scale (IES-R)
2.2.5. Emotion Regulation Questionnaire (ERQ)
2.3. Procedure
3. Results
3.1. Analysis of Data Quality
3.2. Analyses by Construct
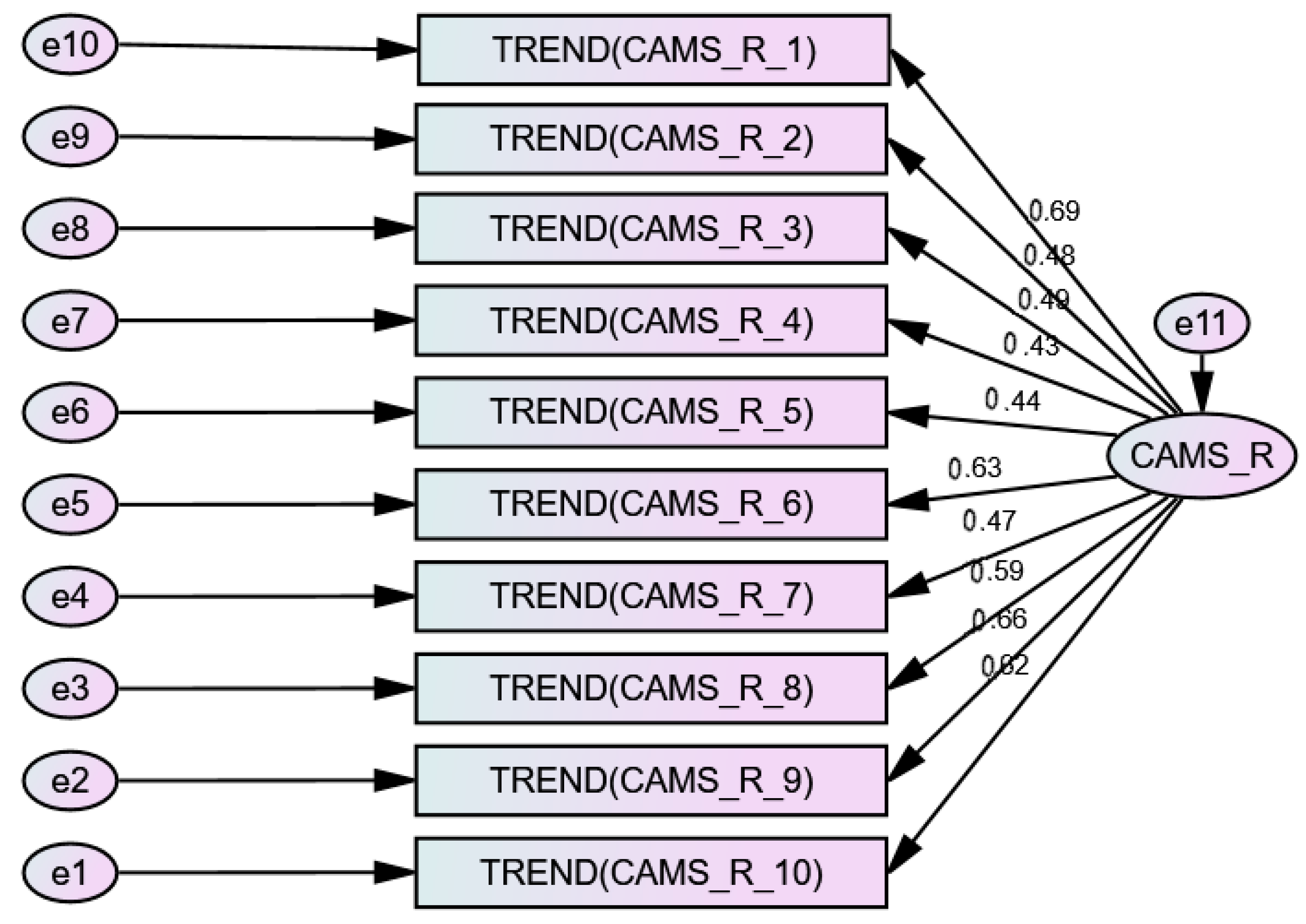
3.2.1. CAMS-R Exploratory Factor Analysis
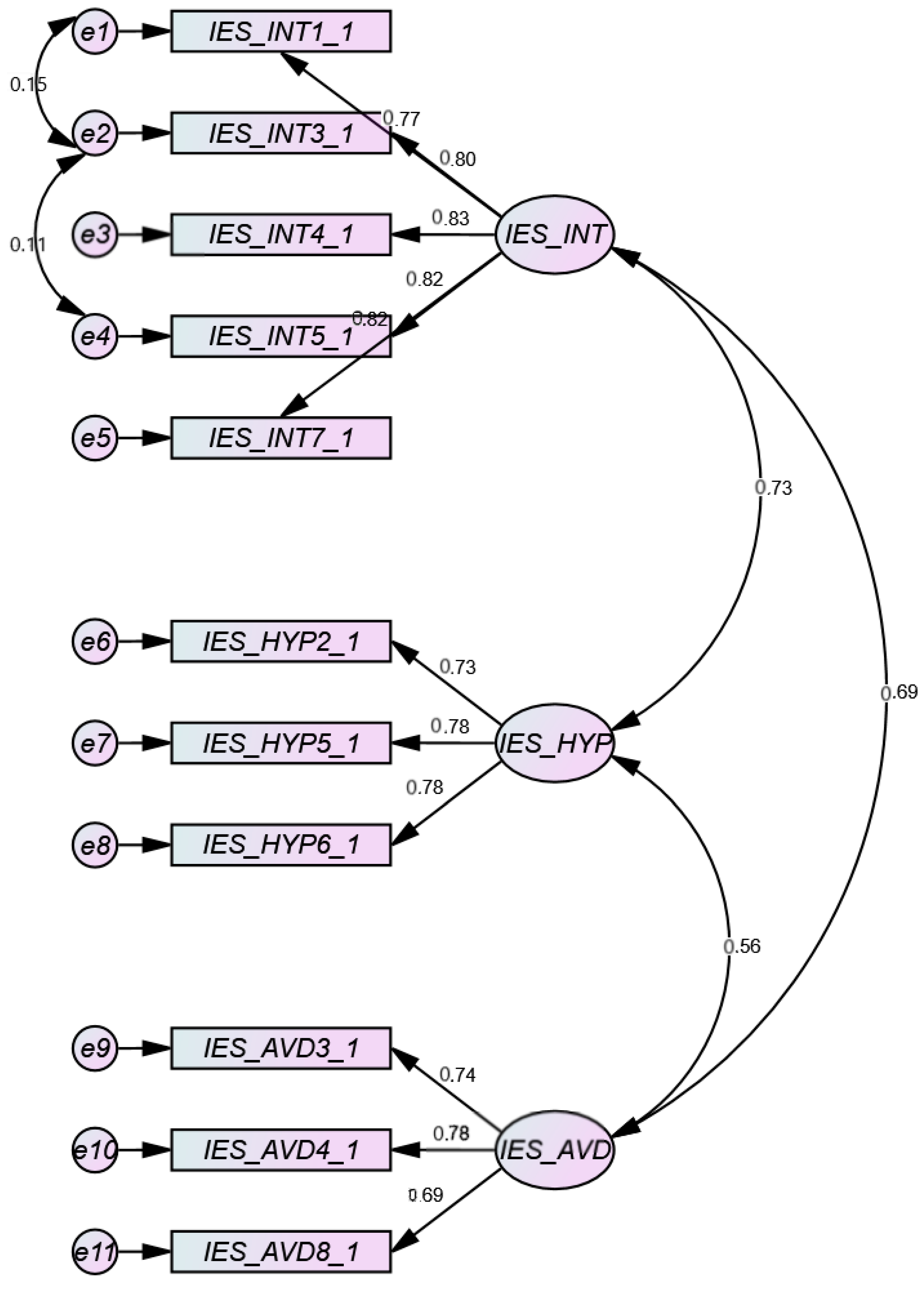
3.2.2. IES Exploratory Factor Analysis
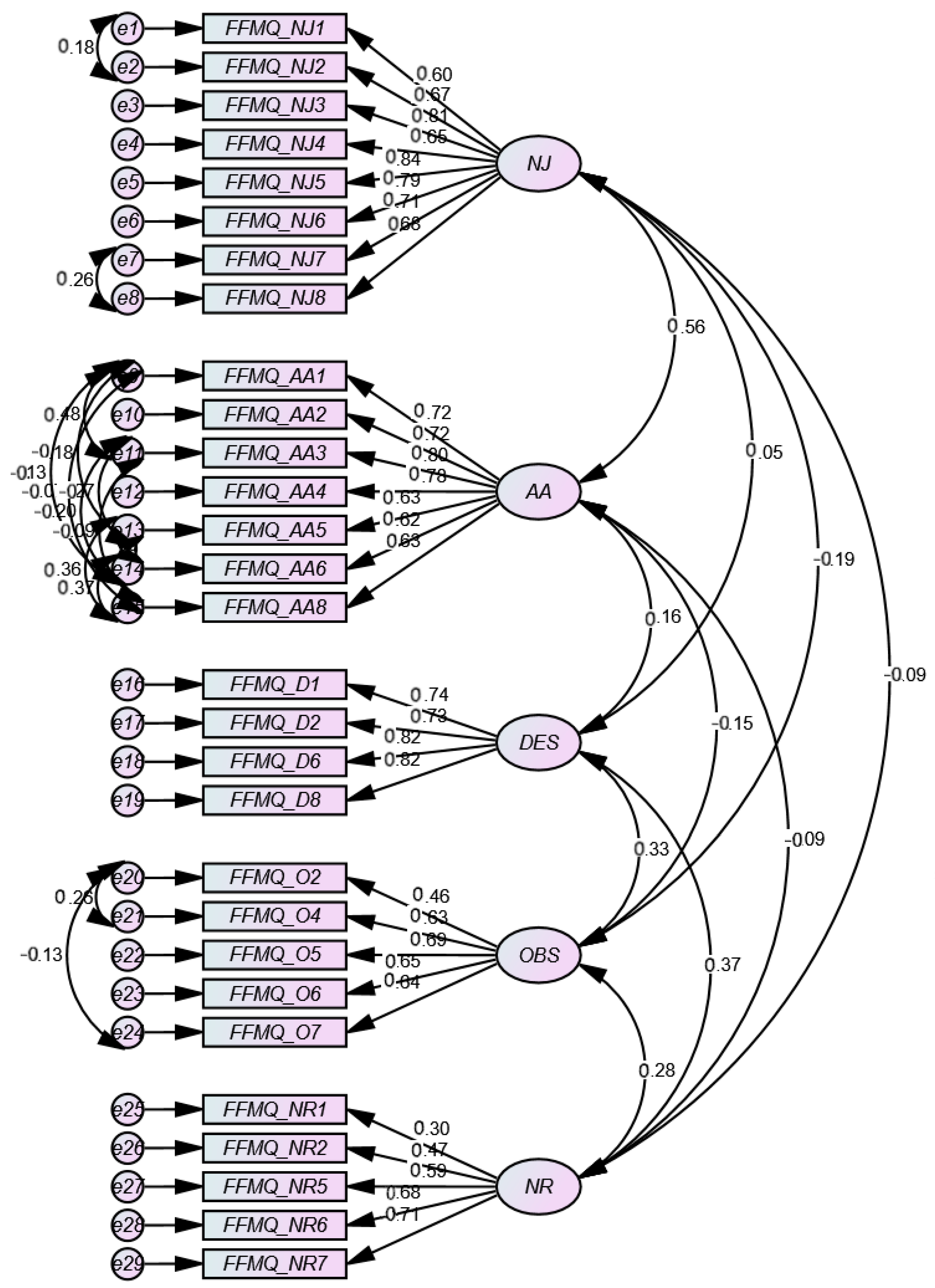
3.2.3. FFMQ Exploratory Factor Analysis
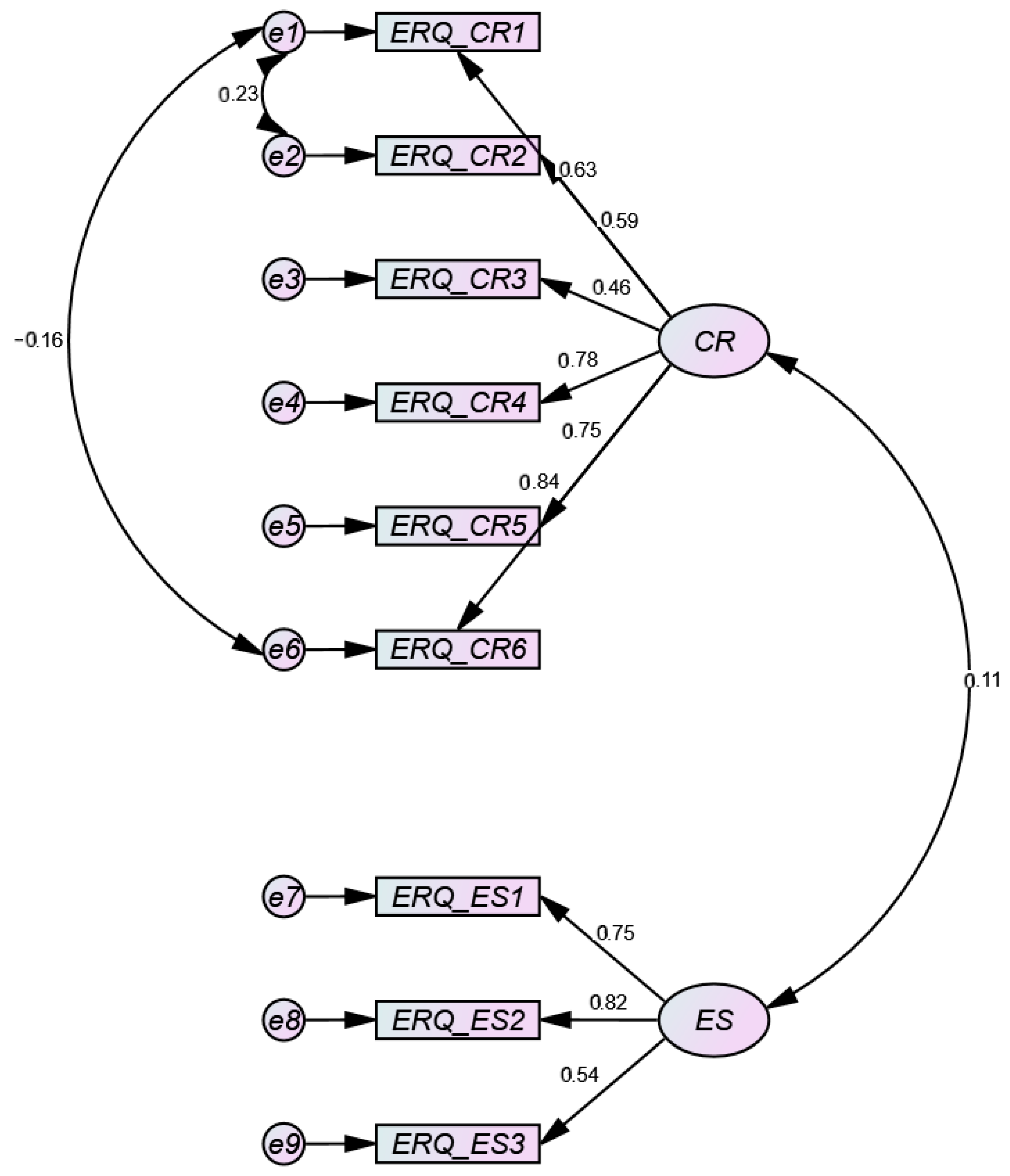
3.2.4. ERQ Exploratory Factor Analysis
3.2.5. Total Variance
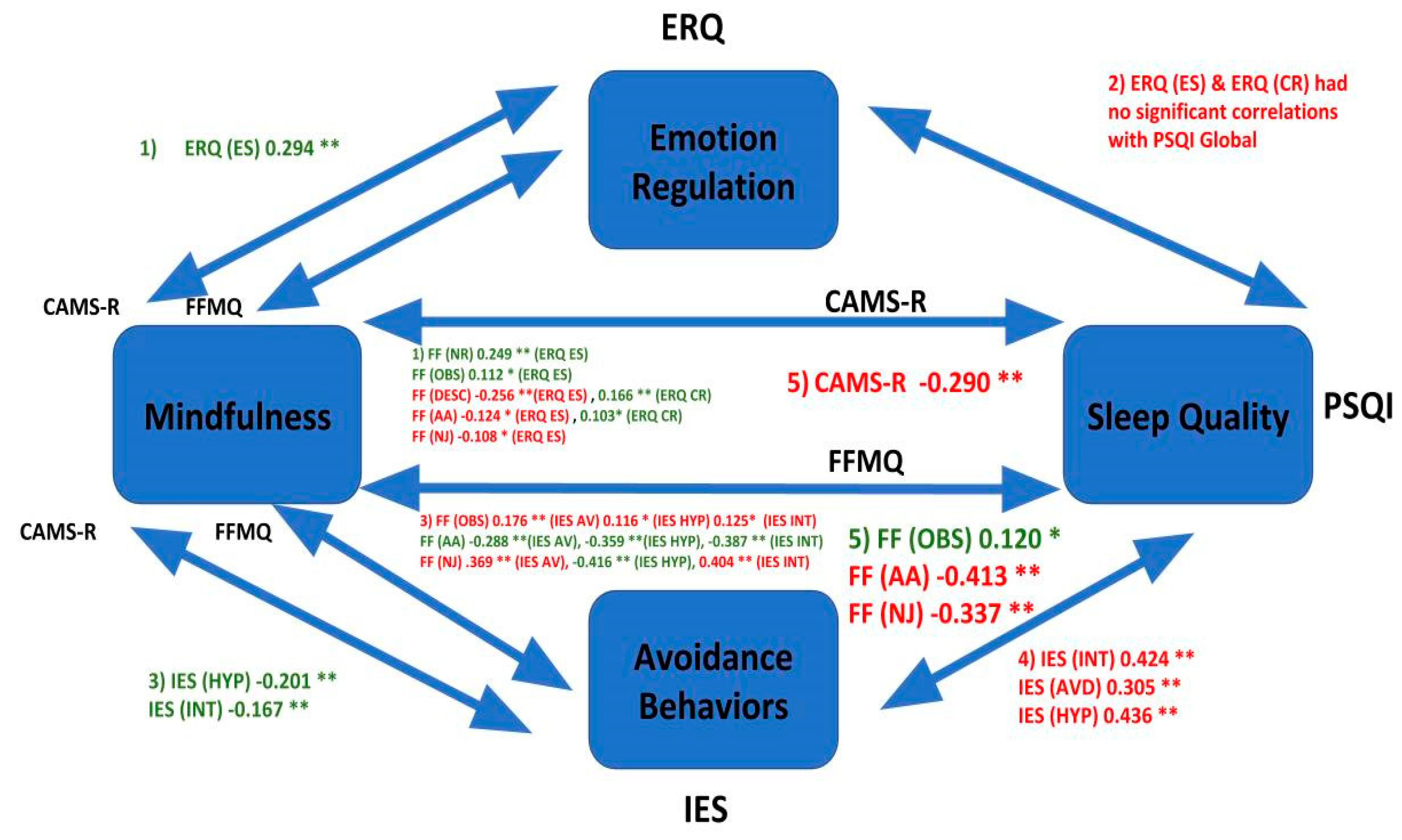
3.2.6. Correlational Analyses
3.2.7. Stepwise Regression
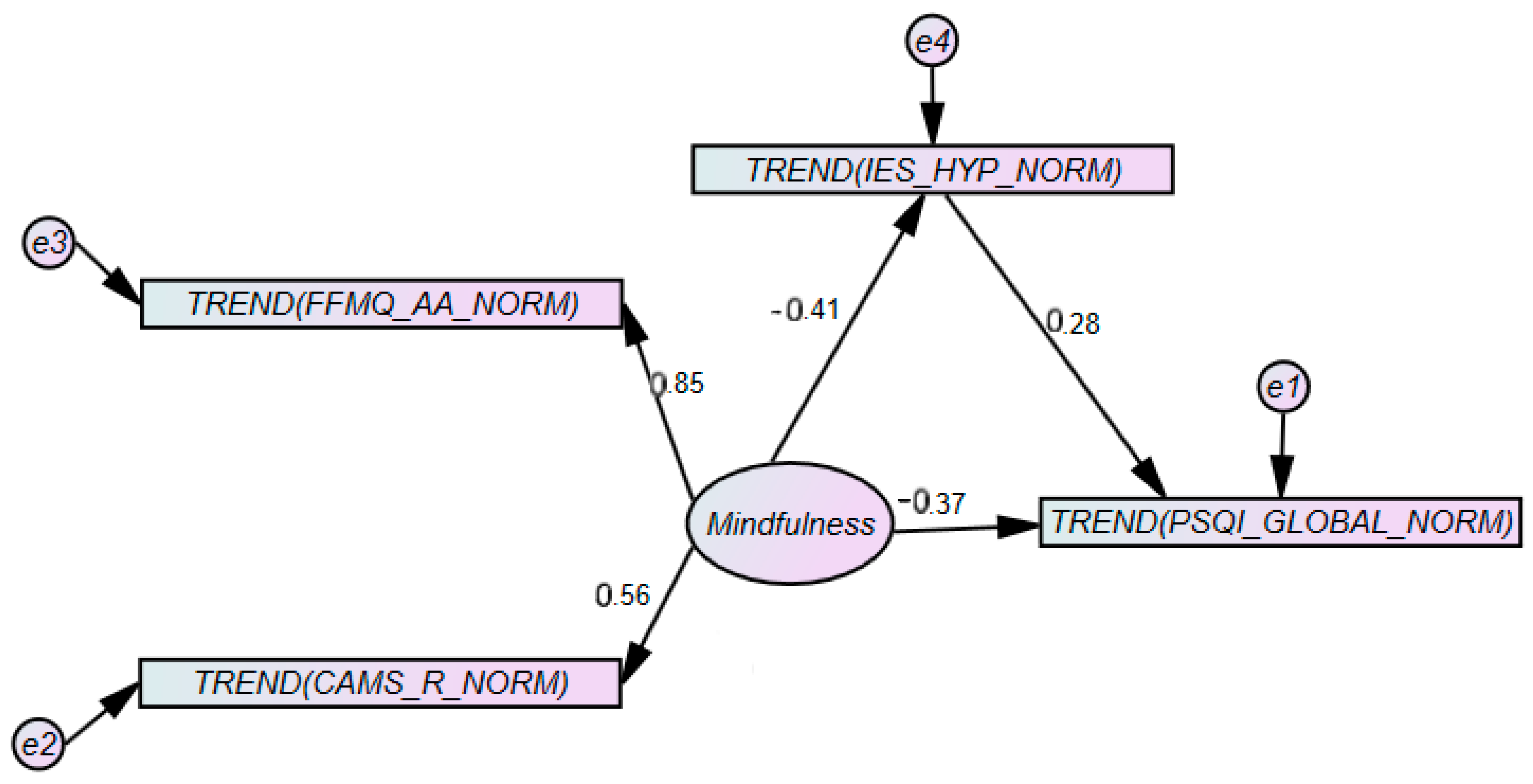
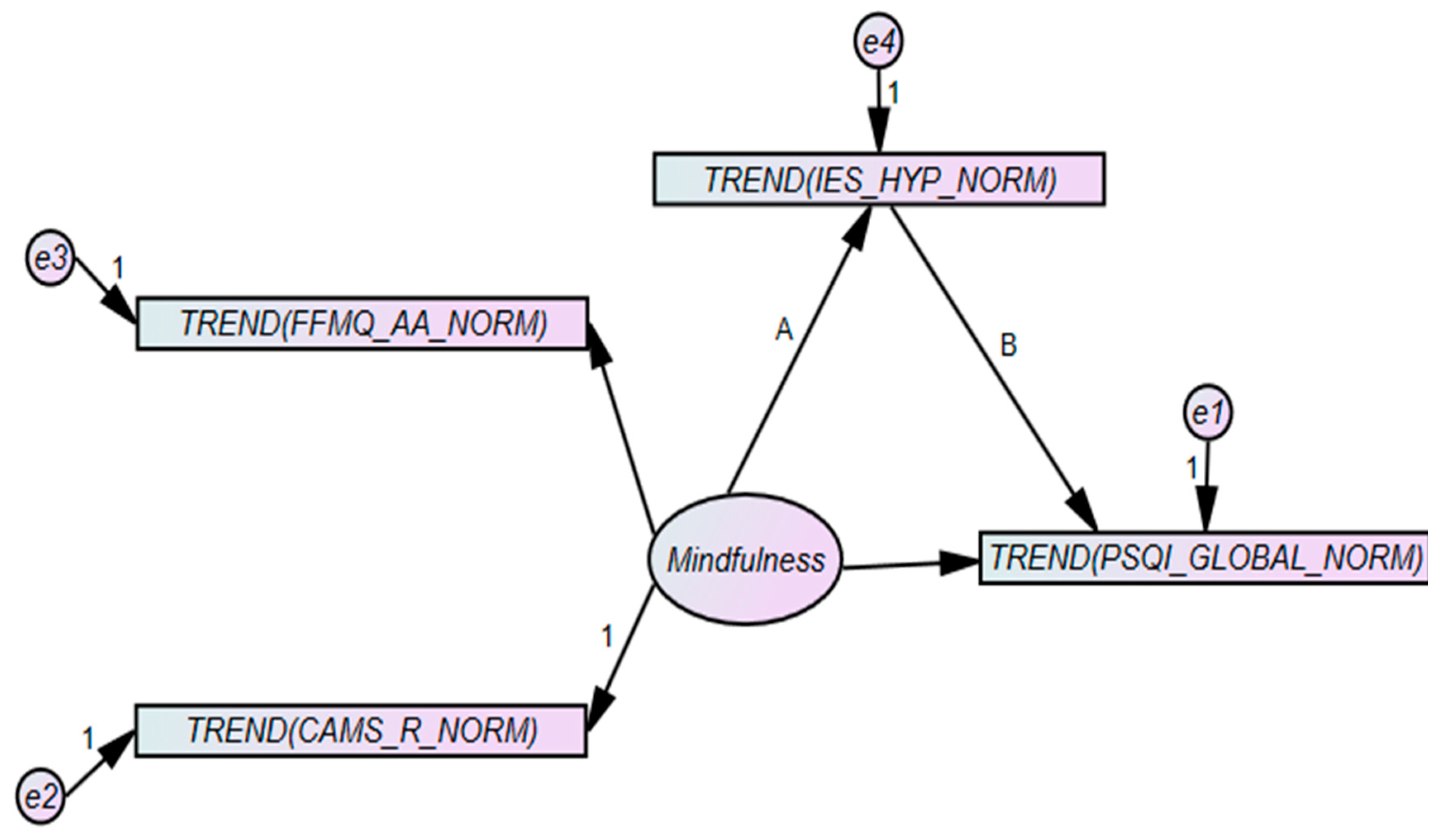
3.2.8. Hyperarousal as a Mediator
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Descriptive Statistics | |||||
|---|---|---|---|---|---|
| N | Minimum | Maximum | Mean | Std. Deviation | |
| Any reminder brought back feelings about it. | 367 | 1 | 5 | 3.08 | 1.247 |
| I had trouble staying asleep. | 366 | 1 | 5 | 2.38 | 1.349 |
| Other things kept making me think about it. | 366 | 1 | 5 | 2.88 | 1.261 |
| I felt irritable and angry. | 367 | 1 | 5 | 2.65 | 1.391 |
| I avoided letting myself get upset when I thought about it or was reminded of it. | 367 | 1 | 5 | 2.81 | 1.221 |
| I thought about it when I didn’t mean to. | 367 | 1 | 5 | 3.16 | 1.271 |
| I felt as if it didn’t happen or wasn’t real. | 366 | 1 | 5 | 2.34 | 1.416 |
| I stayed away from reminders of it. | 364 | 1 | 5 | 2.89 | 1.383 |
| Pictures about it popped into my mind. | 367 | 1 | 5 | 3.02 | 1.378 |
| I was jumpy or easily startled. | 366 | 1 | 5 | 2.02 | 1.294 |
| I tried not to think about it. | 366 | 1 | 5 | 3.37 | 1.334 |
| I was aware that I still had lots of feelings about it, but I didn’t deal with them. | 365 | 1 | 5 | 3.04 | 1.41 |
| My feelings about it were kind of numb. | 367 | 1 | 5 | 2.65 | 1.361 |
| I found myself acting or feeling like I was back at the time. | 366 | 1 | 5 | 2.33 | 1.279 |
| I had trouble falling asleep. | 367 | 1 | 5 | 2.45 | 1.449 |
| I had waves of strong feelings about it. | 366 | 1 | 5 | 2.97 | 1.456 |
| I tried to remove it from my memory. | 367 | 1 | 5 | 2.78 | 1.513 |
| I had trouble concentrating. | 367 | 1 | 5 | 2.63 | 1.375 |
| Reminders of it caused me to have physical reactions, such as sweating, trouble breathing, nausea, or pounding heart. | 364 | 1 | 5 | 2.19 | 1.448 |
| I had dreams about it. | 366 | 1 | 5 | 2.5 | 1.524 |
| I felt watchful and on-guard. | 366 | 1 | 5 | 2.31 | 1.398 |
| I tried not to talk about it. | 366 | 1 | 5 | 2.98 | 1.474 |
| Valid N (listwise) | 353 |
| Descriptive Statistics | |||||
|---|---|---|---|---|---|
| N | Minimum | Maximum | Mean | Std. Deviation | |
| When I’m walking, I deliberately notice the sensations of my body moving. | 367 | 1 | 5 | 2.49 | 1.096 |
| I’m good at finding words to describe my feelings. | 367 | 1 | 5 | 2.9 | 1.14 |
| I criticize myself for having irrational or inappropriate emotions. | 367 | 1 | 5 | 2.97 | 1.23 |
| I perceive my feelings and emotions without having to react to them. | 366 | 1 | 5 | 2.88 | 0.988 |
| When I do things, my mind wanders off and I’m easily distracted. | 367 | 1 | 5 | 2.74 | 1.156 |
| When I take a shower or bath, I stay alert to the sensations of water on my body. | 364 | 1 | 5 | 2.87 | 1.261 |
| I can easily put my beliefs, opinions, and expectations into words. | 365 | 1 | 5 | 3.14 | 1.122 |
| I don’t pay attention to what I’m doing because I’m daydreaming, worrying, or otherwise distracted. | 366 | 1 | 5 | 3.17 | 1.193 |
| I watch my feelings without getting lost in them. | 367 | 1 | 5 | 2.78 | 1.017 |
| I tell myself I shouldn’t be feeling the way I’m feeling. | 363 | 1 | 5 | 2.85 | 1.255 |
| I notice how foods and drinks affect my thoughts, bodily sensations, and emotions. | 367 | 1 | 5 | 2.86 | 1.34 |
| It’s hard for me to find the words to describe what I’m thinking. | 367 | 1 | 5 | 3.18 | 1.212 |
| I am easily distracted. | 367 | 1 | 5 | 2.85 | 1.257 |
| I believe some of my thoughts are abnormal or bad and I shouldn’t think that way. | 364 | 1 | 5 | 3.25 | 1.307 |
| I pay attention to sensations, such as the wind in my hair or sun on my face. | 367 | 1 | 5 | 3.06 | 1.256 |
| I have trouble thinking of the right words to express how I feel about things. | 367 | 1 | 5 | 3.16 | 1.156 |
| I make judgments about whether my thoughts are good or bad. | 366 | 1 | 5 | 2.79 | 1.123 |
| I find it difficult to stay focused on what’s happening in the present. | 366 | 1 | 5 | 3.27 | 1.201 |
| When I have distressing thoughts or images, I “step back” and am aware of the thought or image without getting taken over by it. | 366 | 1 | 5 | 2.84 | 1.138 |
| I pay attention to sounds, such as clocks ticking, birds chirping, or cars passing. | 365 | 1 | 5 | 3.04 | 1.332 |
| In difficult situations, I can pause without immediately reacting. | 364 | 1 | 5 | 2.9 | 1.12 |
| When I have a sensation in my body, it’s difficult for me to describe it because I can’t find the right words. | 366 | 1 | 5 | 3.49 | 1.102 |
| It seems I am “running on automatic” without much awareness of what I’m doing | 364 | 1 | 5 | 3.19 | 1.262 |
| When I have distressing thoughts or images, I feel calm soon after. | 366 | 1 | 5 | 2.46 | 1.074 |
| I tell myself that I shouldn’t be thinking the way I’m thinking. | 365 | 1 | 5 | 3.11 | 1.262 |
| I notice the smells and aromas of things. | 365 | 1 | 5 | 3.42 | 1.178 |
| Even when I’m feeling terribly upset, I can find a way to put it into words. | 363 | 1 | 5 | 2.8 | 1.146 |
| I rush through activities without being really attentive to them. | 366 | 1 | 5 | 3.36 | 1.084 |
| When I have distressing thoughts or images I am able just to notice them without reacting | 366 | 1 | 5 | 2.68 | 1.023 |
| I think some of my emotions are bad or inappropriate and I shouldn’t feel them. | 364 | 1 | 5 | 3.33 | 1.262 |
| I notice visual elements in art or nature, such as colors, shapes, textures, or patterns of light and shadow. | 365 | 1 | 5 | 3.11 | 1.25 |
| My natural tendency is to put my experiences into words. | 365 | 1 | 5 | 2.77 | 1.234 |
| When I have distressing thoughts or images, I just notice them and let them go. | 366 | 1 | 5 | 2.66 | 1.083 |
| I do jobs or tasks automatically without being aware of what I’m doing. | 364 | 1 | 5 | 3.2 | 1.152 |
| When I have distressing thoughts or images, I judge myself as good or bad, depending what the thought/image is about. | 366 | 1 | 5 | 3.26 | 1.225 |
| I pay attention to how my emotions affect my thoughts and behavior. | 364 | 1 | 5 | 3.34 | 1.106 |
| I can usually describe how I feel at the moment in considerable detail. | 366 | 1 | 5 | 2.87 | 1.155 |
| I find myself doing things without paying attention. | 366 | 1 | 5 | 3.09 | 1.149 |
| I disapprove of myself when I have irrational ideas. | 365 | 1 | 5 | 3.25 | 1.222 |
| Valid N (listwise) | 336 |
| Descriptive Statistics | |||||
|---|---|---|---|---|---|
| N | Minimum | Maximum | Mean | Std. Deviation | |
| When I want to feel more positive emotion (such as joy or amusement), I change what I’m thinking about. | 366 | 2 | 7 | 5.3333 | 1.25331 |
| I keep my emotions to myself. | 364 | 1 | 7 | 4.5769 | 1.74619 |
| When I want to feel less negative emotions (such as sadness or anger), I change what I’m thinking about. | 361 | 1 | 7 | 5.0277 | 1.52727 |
| When I’m faced with a stressful situation, I make myself think about it in a way that helps me stay calm. | 361 | 1 | 7 | 4.7535 | 1.63389 |
| I control my emotions by not expressing them. | 355 | 1 | 7 | 4.0282 | 1.94393 |
| When I want to feel more positive emotion, I change the way I’m thinking about the situation. | 364 | 1 | 7 | 5.0714 | 1.46788 |
| I control my emotions by changing the way I think about the situation I’m in. | 362 | 1 | 7 | 4.7541 | 1.53186 |
| When I am feeling negative emotions, I make sure not to express them. | 359 | 1 | 7 | 3.8552 | 1.85544 |
| When I want to feel less negative emotion, I change the way I’m thinking about the situation. | 363 | 1 | 7 | 4.8209 | 1.54434 |
| Valid N (listwise) | 337 |
References
- Palmer, C.A.; Oosterhoff, B.; Bower, J.L.; Kaplow, J.B.; Alfano, C.A. Associations among adolescent sleep problems, emotion regulation, and affective disorders: Findings from a nationally representative sample. J. Psychiatr. Res. 2018, 96, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Backhaus, J.; Junghanns, K. Daytime naps improve procedural motor memory. Sleep Med. 2006, 7, 508–512. [Google Scholar] [CrossRef]
- Debarnot, U.; Castellani, E.; Valenza, G.; Sebastiani, L.; Guillot, A. Daytime naps improve motor imagery learning. Cogn. Affect. Behav. Neurosci. 2011, 11, 541–550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doran, S.M.; Van Dongen, H.P.A.; Dinges, D.F. Sustained attention performance during sleep deprivation: Evidence of state instability. Arch. Ital. De Biol. 2001, 139, 253–267. [Google Scholar]
- Lo, J.C.; Groeger, J.A.; Santhi, N.; Arbon, E.L.; Lazar, A.S.; Hasan, S.; von Schantz, M.; Archer, S.N.; Dijk, D.-J. Effects of Partial and Acute Total Sleep Deprivation on Performance across Cognitive Domains, Individuals and Circadian Phase. PLoS ONE 2012, 7, e45987. [Google Scholar] [CrossRef] [Green Version]
- MacDonald, K.J.; Lockhart, H.A.; Storace, A.C.; Emrich, S.M.; Cote, K.A. A daytime nap enhances visual working memory performance and alters event-related delay activity. Cogn. Affect. Behav. Neurosci. 2018, 18, 1105–1120. [Google Scholar] [CrossRef]
- Palmer, C.A.; Alfano, C.A. Sleep and emotion regulation: An organizing, integrative review. Sleep Med. Rev. 2017, 31, 6–16. [Google Scholar] [CrossRef] [PubMed]
- Gullone, E.; Taffe, J. The Emotion Regulation Questionnaire for Children and Adolescents (ERQ–CA): A psychometric evaluation. Psychol. Assess. 2012, 24, 409–417. [Google Scholar] [CrossRef]
- Thompson, R.A. Emotion Regulation: A theme in Search of Definition. Monogr. Soc. Res. Child. Dev. 1994, 59, 25–52. [Google Scholar] [CrossRef]
- Feldman, G.; Hayes, A.; Kumar, S.; Greeson, J.; Laurenceau, J.-P. Mindfulness and Emotion Regulation: The Development and Initial Validation of the Cognitive and Affective Mindfulness Scale-Revised (CAMS-R). J. Psychopathol. Behav. Assess. 2007, 29, 177–190. [Google Scholar] [CrossRef]
- Gross, J.J.; John, O.P. Individual differences in two emotion regulation processes: Implications for affect, relationships, and well-being. J. Personal. Soc. Psychol. 2003, 85, 348–362. [Google Scholar] [CrossRef] [PubMed]
- Greeson, J.M.; Zarrin, H.; Smoski, M.J.; Brantley, J.G.; Lynch, T.R.; Webber, D.M.; Hall, M.H.; Suarez, E.C.; Wolever, R.Q. Mindfulness Meditation Targets Transdiagnostic Symptoms Implicated in Stress-Related Disorders: Understanding Relationships between Changes in Mindfulness, Sleep Quality, and Physical Symptoms. Evid. Based Complementary Altern. Med. 2018, 2018, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Lutz, J.; Herwig, U.; Opialla, S.; Hittmeyer, A.; Jäncke, L.; Rufer, M.; Grosse Holtforth, M.; Brühl, A.B. Mindfulness and emotion regulation—An fMRI study. Soc. Cogn. Affect. Neurosci. 2014, 9, 776–785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, B.L.; Waltz, J. Mindfulness and experiential avoidance as predictors of posttraumatic stress disorder avoidance symptom severity. J. Anxiety Disord. 2010, 24, 409–415. [Google Scholar] [CrossRef]
- Arch, J.J.; Craske, M.G. Mechanisms of mindfulness: Emotion regulation following a focused breathing induction. Behav. Res. Ther. 2006, 44, 1849–1858. [Google Scholar] [CrossRef] [PubMed]
- Kiken, L.G.; Garland, E.L.; Bluth, K.; Palsson, O.S.; Gaylord, S.A. From a state to a trait: Trajectories of state mindfulness in meditation during intervention predict changes in trait mindfulness. Personal. Individ. Differ. 2015, 81, 41–46. [Google Scholar] [CrossRef] [Green Version]
- Garland, E.L.; Hanley, A.; Farb, N.A.; Froeliger, B. State Mindfulness During Meditation Predicts Enhanced Cognitive Reappraisal. Mindfulness 2015, 6, 234–242. [Google Scholar] [CrossRef] [PubMed]
- Germain, A.; Caroff, K.; Buysse, D.J.; Shear, M.K. Sleep quality in complicated grief. J. Traum. Stress 2005, 18, 343–346. [Google Scholar] [CrossRef]
- Carpenter, J.S.; Andrykowski, M.A. Psychometric evaluation of the pittsburgh sleep quality index. J. Psychosom. Res. 1998, 45, 5–13. [Google Scholar] [CrossRef]
- Hall, M.; Kupfer, D.J. Intrusive thoughts and avoidance behaviors are associated with sleep disturbances in bereavement-related depression. Depress. Anxiety 1997, 7, 106–112. [Google Scholar] [CrossRef]
- Hall, M.; Baum, A.; Buysse, D.J.; Prigerson, H.G.; Kupfer, D.J.; Reynolds, C.F. Sleep as a Mediator of the Stress-Immune Relationship. Psychosom. Med. 1998, 60, 48–51. [Google Scholar] [CrossRef] [PubMed]
- Hall, M.; Buysse, D.J.; Nowell, P.D.; Nofzinger, E.A.; Houck, P.; Reynolds, C.F.; Kupfer, D.J. Symptoms of Stress and Depression as Correlates of Sleep in Primary Insomnia. Psychosom. Med. 2000, 62, 227–230. [Google Scholar] [CrossRef] [PubMed]
- Markarian, S.A.; Pickett, S.M.; Deveson, D.F.; Kanona, B.B. A model of BIS/BAS sensitivity, emotion regulation difficulties, and depression, anxiety, and stress symptoms in relation to sleep quality. Psychiatry Res. 2013, 210, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Hoyt, M.A.; Thomas, K.S.; Epstein, D.R.; Dirksen, S.R. Coping Style and Sleep Quality in Men with Cancer. Ann. Behav. Med. 2009, 37, 88–93. [Google Scholar] [CrossRef] [Green Version]
- Payne, A.; Kralj, A.; Young, J.; Meiser-Stedman, R. The prevalence of intrusive memories in adult depression: A meta-analysis. J. Affect. Disord. 2019, 253, 193–202. [Google Scholar] [CrossRef] [Green Version]
- Roemer, L.; Orsillo, S.M. Expanding Our Conceptualization of and Treatment for Generalized Anxiety Disorder: Integrating Mindfulness/Acceptance-Based Approaches With Existing Cognitive-Behavioral Models. Clin. Psychol. Sci. Pract. 2006, 9, 54–68. [Google Scholar] [CrossRef]
- Cowdrey, F.A.; Park, R.J. The role of experiential avoidance, rumination and mindfulness in eating disorders. Eat. Behav. 2012, 13, 100–105. [Google Scholar] [CrossRef]
- Liu, Q.-Q.; Zhou, Z.-K.; Yang, X.-J.; Kong, F.-C.; Sun, X.-J.; Fan, C.-Y. Mindfulness and sleep quality in adolescents: Analysis of rumination as a mediator and self-control as a moderator. Personal. Individ. Differ. 2018, 122, 171–176. [Google Scholar] [CrossRef]
- Murnieks, C.Y.; Arthurs, J.D.; Cardon, M.S.; Farah, N.; Stornelli, J.; Michael Haynie, J. Close your eyes or open your mind: Effects of sleep and mindfulness exercises on entrepreneurs’ exhaustion. J. Bus. Ventur. 2019, S0883902617305281. [Google Scholar] [CrossRef]
- Rash, J.A.; Kavanagh, V.A.J.; Garland, S.N. A Meta-Analysis of Mindfulness-Based Therapies for Insomnia and Sleep Disturbance. Sleep Med. Clin. 2019, 14, 209–233. [Google Scholar] [CrossRef]
- Baer, R.A.; Smith, G.T.; Hopkins, J.; Krietemeyer, J.; Toney, L. Using Self-Report Assessment Methods to Explore Facets of Mindfulness. Assessment 2006, 13, 27–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Creamer, M.; Bell, R.; Failla, S. Psychometric properties of the Impact of Event Scale—Revised. Behav. Res. Ther. 2003, 41, 1489–1496. [Google Scholar] [CrossRef] [PubMed]
- Horowitz, M.; Wilner, N.; Alvarez, W. Impact of Event Scale: A Measure of Subjective Stress. Psychosom. Med. 1979, 41, 209–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaskin, J. Gaskination’s StatWiki. S.E.M. 2020. Available online: http://statwiki.kolobkreations.com (accessed on 5 November 2020).
- Ong, J.C. Mindfulness-Based Therapy for Insomnia; American Psychological Association: Washington, DC, USA, 2017; p. 233. ISBN 978-1-4338-2241-4. [Google Scholar]
- Mustian, K.M.; Janelsins, M.; Peppone, L.J.; Kamen, C. Yoga for the Treatment of Insomnia among Cancer Patients: Evidence, Mechanisms of Action, and Clinical Recommendations. Oncol. Hematol. Rev. 2014, 10, 164–168. [Google Scholar] [CrossRef] [Green Version]








| N | Mean | Skewness | Kurtosis | |||||
|---|---|---|---|---|---|---|---|---|
| Measure | Statistic | Statistic | Std. Error | Std. Deviation | Statistic | Std. Error | Statistic | Std. Error |
| PSQI_GLOBAL_NORM | 367 | 13.80 | 0.22 | 4.21 | 0.06 | 0.13 | −0.09 | 0.25 |
| IES_AVD_NORM | 367 | 2.70 | 0.05 | 0.91 | 0.08 | 0.13 | −0.30 | 0.25 |
| IES_HYP_NORM | 367 | 1.93 | 0.04 | 0.85 | 0.08 | 0.13 | −0.30 | 0.25 |
| IES_INT_NORM | 367 | 2.55 | 0.05 | 0.90 | 0.08 | 0.13 | −0.30 | 0.25 |
| ERQ_ES_NORM | 367 | 3.26 | 0.06 | 1.16 | 0.05 | 0.13 | −0.08 | 0.25 |
| ERQ_CR_NORM | 367 | 3.13 | 0.04 | 0.73 | 0.05 | 0.13 | −0.08 | 0.25 |
| FFMQ_NR_NORM | 366 | 0.93 | 0.01 | 0.25 | 0.00 | 0.13 | −0.17 | 0.25 |
| FFMQ_OBS_NORM | 366 | 1.75 | 0.03 | 0.50 | 0.00 | 0.13 | −0.17 | 0.25 |
| FFMQ_DESC_NORM | 366 | 2.65 | 0.04 | 0.78 | 0.00 | 0.13 | −0.17 | 0.25 |
| FFMQ_AA_NORM | 366 | 2.67 | 0.04 | 0.77 | 0.00 | 0.13 | −0.17 | 0.25 |
| FFMQ_NJ_NORM | 366 | 2.28 | 0.04 | 0.70 | 0.00 | 0.13 | −0.17 | 0.25 |
| Valid N (listwise) | 363 | |||||||
| n | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. CAMS_R | Pearson Correlation | 367 | 1 | −0.290 ** | −0.070 | −0.201 ** | −0.167 ** | −0.088 | 0.294 ** | 0.277 ** | 0.128 * | 0.517 ** | 0.474 ** | 0.310 ** |
| 2. PSQI_GLOBAL | Pearson Correlation | 367 | −0.290 ** | 1 | 0.305 ** | 0.436 ** | 0.424 ** | 0.093 | −0.051 | −0.079 | 0.120 * | −0.096 | −0.413 ** | −0.337 ** |
| 3. IES_AVD | Pearson Correlation | 367 | −0.070 | 0.305 ** | 1 | 0.727 ** | 0.792 ** | 0.145 ** | 0.067 | 0.085 | 0.176 ** | −0.016 | −0.288 ** | −0.369 ** |
| 4. IES_HYP | Pearson Correlation | 367 | −0.201 ** | 0.436 ** | 0.727 ** | 1 | 0.860 ** | 0.015 | −0.048 | −0.026 | 0.116 * | −0.067 | −0.359 ** | −0.416 ** |
| 5. IES_INT | Pearson Correlation | 367 | −0.167 ** | 0.424 ** | 0.792 ** | 0.860 ** | 1 | 0.039 | −0.008 | −0.016 | 0.125 * | −0.029 | −0.378 ** | −0.404 ** |
| 6. ERQ_ES | Pearson Correlation | 367 | −0.088 | 0.093 | 0.145 ** | 0.015 | 0.039 | 1 | 0.171 ** | 0.060 | −0.070 | −0.256 ** | −0.124 * | −0.108 * |
| 7. ERQ_CR | Pearson Correlation | 367 | 0.294 ** | −0.051 | 0.067 | −0.048 | −0.008 | 0.171 ** | 1 | 0.249 ** | 0.112 * | 0.166 ** | 0.103 * | −0.013 |
| 8. FFMQ_NR | Pearson Correlation | 367 | 0.277 ** | −0.079 | 0.085 | −0.026 | −0.016 | 0.060 | 0.249 ** | 1 | 0.383 ** | 0.440 ** | −0.105 * | −0.111 * |
| 9. FFMQ_OBS | Pearson Correlation | 367 | 0.128 * | 0.120 * | 0.176 ** | 0.116 * | 0.125 * | −0.070 | 0.112 * | 0.383 ** | 1 | 0.380 ** | −0.150 ** | −0.206 ** |
| 10. FFMQ_DESC | Pearson Correlation | 367 | 0.517 ** | −0.096 | −0.016 | −0.067 | −0.029 | −0.256 ** | 0.166 ** | 0.440 ** | 0.380 ** | 1 | 0.190 ** | 0.069 |
| 11. FFMQ_AA | Pearson Correlation | 367 | 0.474 ** | −0.413 ** | −0.288 ** | −0.359 ** | −0.378 ** | −0.124 * | 0.103 * | −0.105 * | −0.150 ** | 0.190 ** | 1 | 0.613 ** |
| 12. FFMQ_NJ | Pearson Correlation | 367 | 0.310 ** | −0.337 ** | −0.369 ** | −0.416 ** | −0.404 ** | −0.108 * | −0.013 | −0.111 * | −0.206 ** | 0.069 | 0.613 ** | 1 |
| Predictor | ∆R2 | β | Total R2 |
|---|---|---|---|
| Step 1 Control: IES (HYP) | 0.190 ** | 0.436 ** | 0.188 ** |
| Step 2 IES (HYP) FFMQ (AA) | 0.076 ** | 0.330 ** −0.295 ** | 0.262 ** |
| Step 3 IES (HYP) FFMQ (AA) CAMS-R | 0.009 * | 0.326 ** −0.245 ** −0.108 * | 0.269 * |
| n1 = 365 n2 = 364 n3 = 363 |
| Measure | df | F |
|---|---|---|
| Model 1 Constant IES (HYP) | 1 | F(1, 365) = 85.04 ** |
| Model 2 IES (HYP) FFMQ (AA) | 2 | F(2, 364) = 65.83 ** |
| Model 3 IES (HYP) FFMQ (AA) CAMS-R n = 366 | 3 | F(3, 363) = 45.82 ** |
| Measure | Unst. Coefficients β | Std. Error | t | Zero Order | Partial Correlations | Semi-Partial Correlations |
|---|---|---|---|---|---|---|
| Constant | 9.626 | 4.93 | 19.522 ** | |||
| IES (HYP) | 2.165 | 0.234 | 9.247 ** | 0.436 | 0.436 | 0.436 |
| Constant | 14.939 | 0.986 | 15.152 ** | |||
| IES (HYP) | 1.639 | 0.239 | 6.852 ** | 0.436 | 0.338 | 0.308 |
| FFMQ (AA) | −1.607 | 0.262 | −6.131 ** | −0.413 | −0.306 | −0.275 |
| Constant | 16.476 | 1.218 | 13.522 ** | |||
| IES (HYP) | 1.620 | 0.238 | 6.800 ** | 0.436 | 0.336 | −0.304 |
| FFMQ (AA) | −1.336 | 0.290 | −4.599 ** | −0.413 | −0.235 | −0.206 |
| CAMS-R | −1.089 | 0.512 | −2.128 * | −0.290 | −0.111 | −0.095 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Talley, G.; Shelley-Tremblay, J. The Relationship between Mindfulness and Sleep Quality is Mediated by Emotion Regulation. Psychiatry Int. 2020, 1, 42-66. https://doi.org/10.3390/psychiatryint1020007
Talley G, Shelley-Tremblay J. The Relationship between Mindfulness and Sleep Quality is Mediated by Emotion Regulation. Psychiatry International. 2020; 1(2):42-66. https://doi.org/10.3390/psychiatryint1020007
Chicago/Turabian StyleTalley, Garrett, and John Shelley-Tremblay. 2020. "The Relationship between Mindfulness and Sleep Quality is Mediated by Emotion Regulation" Psychiatry International 1, no. 2: 42-66. https://doi.org/10.3390/psychiatryint1020007
APA StyleTalley, G., & Shelley-Tremblay, J. (2020). The Relationship between Mindfulness and Sleep Quality is Mediated by Emotion Regulation. Psychiatry International, 1(2), 42-66. https://doi.org/10.3390/psychiatryint1020007