

Artificial Intelligence in Bladder Cancer Diagnosis: Current Applications and Future Perspectives

 , , ,
, , ,  , , and
, , and
Abstract
:1. Introduction
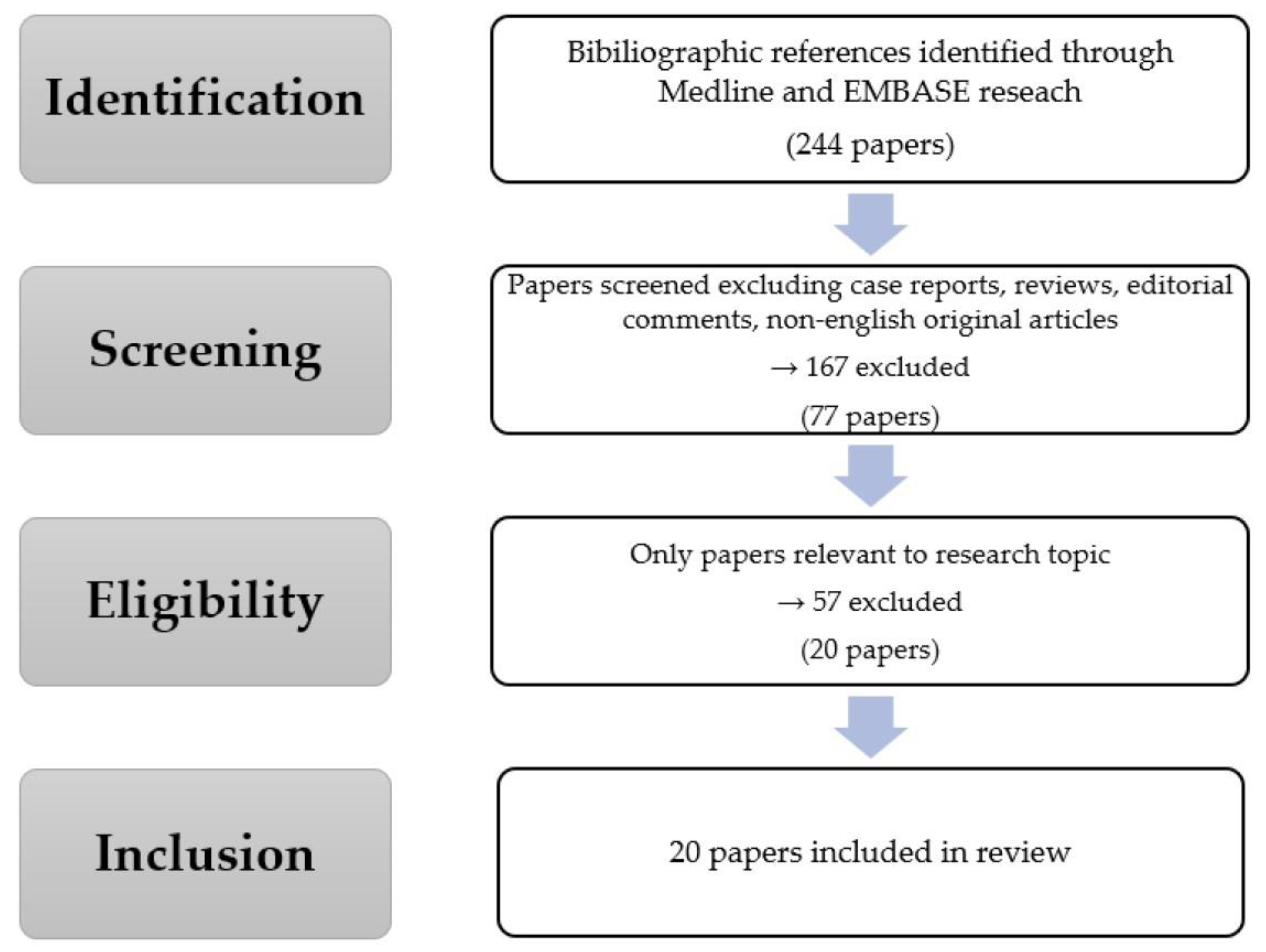
2. Materials and Methods
3. AI-Enhanced BCa Diagnostical Pathway
3.1. AI-Enhanced Cystoscopy
3.2. AI-Enhanced Radiological Imaging
3.3. AI-Enhanced Histopathology Diagnosis and Molecular Subtyping Analysis
4. Conclusions and Future Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA A Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Khadhouri, S.; Gallagher, K.M.; MacKenzie, K.R.; Shah, T.T.; Gao, C.; Moore, S.; Zimmermann, E.F.; Edison, E.; Jefferies, M.; Nambiar, A.; et al. The IDENTIFY Study: The Investigation and Detection of Urological Neoplasia in Patients Referred with Suspected Urinary Tract Cancer—A Multicentre Observational Study. BJU Int. 2021, 128, 440–450. [Google Scholar] [CrossRef]
- Laukhtina, E.; Pradere, B.; Lemberger, U.; Karakiewicz, P.I.; Fajkovic, H.; Shariat, S.F. Molecular Biomarkers to Help Select Neoadjuvant Systemic Therapy for Urothelial Carcinoma of the Bladder. Curr. Opin. Urol. 2022, 32, 561–566. [Google Scholar] [CrossRef] [PubMed]
- Laukhtina, E.; Boehm, A.; Peyronnet, B.; Bravi, C.A.; Batista Da Costa, J.; Soria, F.; D’Andrea, D.; Rajwa, P.; Quhal, F.; Yanagisawa, T.; et al. Urethrectomy at the Time of Radical Cystectomy for Non-Metastatic Urothelial Carcinoma of the Bladder: A Collaborative Multicenter Study. World J. Urol. 2022, 40, 1689–1696. [Google Scholar] [CrossRef] [PubMed]
- Claps, F.; van de Kamp, M.W.; Mayr, R.; Bostrom, P.J.; Boormans, J.L.; Eckstein, M.; Mertens, L.S.; Boevé, E.R.; Neuzillet, Y.; Burger, M.; et al. Risk Factors Associated with Positive Surgical Margins’ Location at Radical Cystectomy and Their Impact on Bladder Cancer Survival. World J. Urol. 2021, 39, 4363–4371. [Google Scholar] [CrossRef]
- Claps, F.; Rai, S.; Mir, M.C.; van Rhijn, B.W.G.; Mazzon, G.; Davis, L.E.; Valadon, C.L.; Silvestri, T.; Rizzo, M.; Ankem, M.; et al. Prognostic Value of Preoperative Albumin-to-Fibrinogen Ratio (AFR) in Patients with Bladder Cancer Treated with Radical Cystectomy. Urol. Oncol. 2021, 39, 835.e9–835.e17. [Google Scholar] [CrossRef]
- Laukhtina, E.; Pradere, B.; Mori, K.; Schuettfort, V.M.; Quhal, F.; Mostafaei, H.; Sari Motlagh, R.; Aydh, A.; Moschini, M.; Enikeev, D.; et al. Prognostic Blood-Based Biomarkers in Patients Treated with Neoadjuvant Chemotherapy for Urothelial Carcinoma of the Bladder: A Systematic Review. Urol. Oncol. 2021, 39, 471–479. [Google Scholar] [CrossRef]
- Mertens, L.S.; Claps, F.; Mayr, R.; Bostrom, P.J.; Shariat, S.F.; Zwarthoff, E.C.; Boormans, J.L.; Abas, C.; van Leenders, G.J.L.H.; Götz, S.; et al. Prognostic Markers in Invasive Bladder Cancer: FGFR3 Mutation Status versus P53 and KI-67 Expression: A Multi-Center, Multi-Laboratory Analysis in 1058 Radical Cystectomy Patients. Urol. Oncol. 2022, 40, 110.e1–110.e9. [Google Scholar] [CrossRef]
- Mori, K.; Abufaraj, M.; Mostafaei, H.; Quhal, F.; Karakiewicz, P.I.; Briganti, A.; Kimura, S.; Egawa, S.; Shariat, S.F. A Systematic Review and Meta-Analysis of Variant Histology in Urothelial Carcinoma of the Bladder Treated with Radical Cystectomy. J. Urol. 2020, 204, 1129–1140. [Google Scholar] [CrossRef]
- Claps, F.; Mir, M.C.; van Rhijn, B.W.G.; Mazzon, G.; Soria, F.; D’Andrea, D.; Marra, G.; Boltri, M.; Traunero, F.; Massanova, M.; et al. Impact of the Controlling Nutritional Status (CONUT) Score on Perioperative Morbidity and Oncological Outcomes in Patients with Bladder Cancer Treated with Radical Cystectomy. Urol. Oncol. 2023, 41, 49.e13–49.e22. [Google Scholar] [CrossRef]
- de Kruijff, I.E.; Beije, N.; Martens, J.W.M.; de Wit, R.; Boormans, J.L.; Sleijfer, S. Liquid Biopsies to Select Patients for Perioperative Chemotherapy in Muscle-Invasive Bladder Cancer: A Systematic Review. Eur. Urol. Oncol. 2021, 4, 204–214. [Google Scholar] [CrossRef] [PubMed]
- Claps, F.; Mir, M.C.; Zargar, H. Molecular Markers of Systemic Therapy Response in Urothelial Carcinoma. Asian J. Urol. 2021, 8, 376–390. [Google Scholar] [CrossRef] [PubMed]
- Mertens, L.S.; Claps, F.; Mayr, R.; Hodgson, A.; Shariat, S.F.; Hippe, K.; Neuzillet, Y.; Sanders, J.; Burger, M.; Pouessel, D.; et al. The Search for the Optimal Cut-off Value of P53-Immunohistochemistry to Predict Prognosis of Invasive Bladder Cancer: A Multi-Center, Multi-Laboratory Analysis. Int. J. Surg. Pathol. 2022, 24, 10668969221095172. [Google Scholar] [CrossRef]
- Claps, F.; Pavan, N.; Umari, P.; Rizzo, M.; Barbone, F.; Giangreco, M.; Liguori, G.; Mir, C.M.; Bussani, R.; Trombetta, C. Incidence, Predictive Factors and Survival Outcomes of Incidental Prostate Cancer in Patients Who Underwent Radical Cystectomy for Bladder Cancer. Minerva Urol. Nephrol. 2021, 73, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Liu, L.; Ding, L.; Zhang, Z.; Zhang, M. Quantitative Assessment of Bladder Cancer Reflects Grade and Recurrence: Comparing of Three Methods of Positioning Region of Interest for ADC Measurements at Diffusion-Weighted MR Imaging. Acad. Radiol. 2019, 26, 1148–1153. [Google Scholar] [CrossRef]
- Cimadamore, A.; Lonati, C.; Di Trapani, E.; De Cobelli, O.; Rink, M.; Zamboni, S.; Simeone, C.; Soria, F.; Briganti, A.; Montorsi, F.; et al. Variant Histologies in Bladder Cancer: Does the Centre Have an Impact in Detection Accuracy? Urol. Oncol. 2022, 40, 273.e11–273.e20. [Google Scholar] [CrossRef]
- Azad, R.K.; Shulaev, V. Metabolomics Technology and Bioinformatics for Precision Medicine. Brief. Bioinform. 2019, 20, 1957–1971. [Google Scholar] [CrossRef]
- Gupta, R.; Srivastava, D.; Sahu, M.; Tiwari, S.; Ambasta, R.K.; Kumar, P. Artificial Intelligence to Deep Learning: Machine Intelligence Approach for Drug Discovery. Mol. Divers. 2021, 25, 1315–1360. [Google Scholar] [CrossRef]
- Choi, R.Y.; Coyner, A.S.; Kalpathy-Cramer, J.; Chiang, M.F.; Campbell, J.P. Introduction to Machine Learning, Neural Networks, and Deep Learning. Transl. Vis. Sci. Technol. 2020, 9, 14. [Google Scholar] [CrossRef]
- Tran, K.A.; Kondrashova, O.; Bradley, A.; Williams, E.D.; Pearson, J.V.; Waddell, N. Deep Learning in Cancer Diagnosis, Prognosis and Treatment Selection. Genome Med. 2021, 13, 152. [Google Scholar] [CrossRef]
- Checcucci, E.; Autorino, R.; Cacciamani, G.E.; Amparore, D.; De Cillis, S.; Piana, A.; Piazzolla, P.; Vezzetti, E.; Fiori, C.; Veneziano, D.; et al. Artificial Intelligence and Neural Networks in Urology: Current Clinical Applications. Minerva Urol. E Nefrol. Ital. J. Urol. Nephrol. 2020, 72, 49–57. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, J.; Minsky, M.L.; Rochester, N.; Corporation, I.B.M.; Shannon, C.E. A proposal for the dartmouth summer research project on artificial intelligence. AI Mag. 1955, 27, 12. [Google Scholar]
- Hamet, P.; Tremblay, J. Artificial Intelligence in Medicine. Metabolism 2017, 69, S36–S40. [Google Scholar] [CrossRef] [PubMed]
- Zhong, F.; Xing, J.; Li, X.; Liu, X.; Fu, Z.; Xiong, Z.; Lu, D.; Wu, X.; Zhao, J.; Tan, X.; et al. Artificial Intelligence in Drug Design. Sci. China Life Sci. 2018, 61, 1191–1204. [Google Scholar] [CrossRef]
- Isfoss, B.L. The Sensitivity of Fluorescent-Light Cystoscopy for the Detection of Carcinoma in Situ (CIS) of the Bladder: A Meta-Analysis with Comments on Gold Standard. BJU Int. 2011, 108, 1703–1707. [Google Scholar] [CrossRef]
- Shkolyar, E.; Jia, X.; Chang, T.C.; Trivedi, D.; Mach, K.E.; Meng, M.Q.-H.; Xing, L.; Liao, J.C. Augmented Bladder Tumor Detection Using Deep Learning. Eur. Urol. 2019, 76, 714–718. [Google Scholar] [CrossRef]
- Wu, S.; Chen, X.; Pan, J.; Dong, W.; Diao, X.; Zhang, R.; Zhang, Y.; Zhang, Y.; Qian, G.; Chen, H.; et al. An Artificial Intelligence System for the Detection of Bladder Cancer via Cystoscopy: A Multicenter Diagnostic Study. J. Natl. Cancer Inst. 2022, 114, 220–227. [Google Scholar] [CrossRef]
- Yoo, J.W.; Koo, K.C.; Chung, B.H.; Baek, S.Y.; Lee, S.J.; Park, K.H.; Lee, K.S. Deep Learning Diagnostics for Bladder Tumor Identification and Grade Prediction Using RGB Method. Sci. Rep. 2022, 12, 17699. [Google Scholar] [CrossRef] [PubMed]
- Mutaguchi, J.; Morooka, K.; Kobayashi, S.; Umehara, A.; Miyauchi, S.; Kinoshita, F.; Inokuchi, J.; Oda, Y.; Kurazume, R.; Eto, M. Artificial Intelligence for Segmentation of Bladder Tumor Cystoscopic Images Performed by U-Net with Dilated Convolution. J. Endourol. 2022, 36, 827–834. [Google Scholar] [CrossRef]
- Burger, M.; Grossman, H.B.; Droller, M.; Schmidbauer, J.; Hermann, G.; Drăgoescu, O.; Ray, E.; Fradet, Y.; Karl, A.; Burgués, J.P.; et al. Photodynamic Diagnosis of Non-Muscle-Invasive Bladder Cancer with Hexaminolevulinate Cystoscopy: A Meta-Analysis of Detection and Recurrence Based on Raw Data. Eur. Urol. 2013, 64, 846–854. [Google Scholar] [CrossRef]
- Heer, R.; Lewis, R.; Vadiveloo, T.; Yu, G.; Mariappan, P.; Cresswell, J.; McGrath, J.; Nabi, G.; Mostafid, H.; Lazarowicz, H.; et al. A Randomized Trial of PHOTOdynamic Surgery in Non–Muscle-Invasive Bladder Cancer. NEJM Evidence 2022, 1, EVIDoa2200092. [Google Scholar] [CrossRef]
- Ali, N.; Bolenz, C.; Todenhöfer, T.; Stenzel, A.; Deetmar, P.; Kriegmair, M.; Knoll, T.; Porubsky, S.; Hartmann, A.; Popp, J.; et al. Deep Learning-Based Classification of Blue Light Cystoscopy Imaging during Transurethral Resection of Bladder Tumors. Sci. Rep. 2021, 11, 11629. [Google Scholar] [CrossRef] [PubMed]
- Claps, F.; Amparore, D.; Esperto, F.; Cacciamani, G.; Fiori, C.; Minervini, A.; Liguori, G.; Trombetta, C.; Porpiglia, F.; Serni, S.; et al. Smart Learning for Urology Residents during the COVID-19 Pandemic and beyond: Insights from a Nationwide Survey in Italy. Minerva Urol. Nefrol. Ital. J. Urol. Nephrol. 2020, 72, 647–649. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, A.; Nosato, H.; Kochi, Y.; Negoro, H.; Kojima, T.; Sakanashi, H.; Murakawa, M.; Nishiyama, H. Cystoscopic Imaging for Bladder Cancer Detection Based on Stepwise Organic Transfer Learning with a Pretrained Convolutional Neural Network. J. Endourol. 2021, 35, 1030–1035. [Google Scholar] [CrossRef] [PubMed]
- Du, Y.; Yang, R.; Chen, Z.; Wang, L.; Weng, X.; Liu, X. A Deep Learning Network-Assisted Bladder Tumour Recognition under Cystoscopy Based on Caffe Deep Learning Framework and EasyDL Platform. Int. J. Med. Robot. Comput. Assist. Surg. MRCAS 2021, 17, 1–8. [Google Scholar] [CrossRef]
- Babjuk, M.; Burger, M.; Capoun, O.; Cohen, D.; Compérat, E.M.; Dominguez Escrig, J.L.; Gontero, P.; Liedberg, F.; Masson-Lecomte, A.; Mostafid, A.H.; et al. European Association of Urology Guidelines on Non-Muscle-Invasive Bladder Cancer (Ta, T1, and Carcinoma in Situ). Eur. Urol. 2022, 81, 75–94. [Google Scholar] [CrossRef]
- Loehfelm, T.W. Artificial Intelligence for Quality Improvement in Radiology. Radiol. Clin. 2021, 59, 1053–1062. [Google Scholar] [CrossRef]
- Zhang, G.; Wu, Z.; Xu, L.; Zhang, X.; Zhang, D.; Mao, L.; Li, X.; Xiao, Y.; Guo, J.; Ji, Z.; et al. Deep Learning on Enhanced CT Images Can Predict the Muscular Invasiveness of Bladder Cancer. Front. Oncol. 2021, 11, 654685. [Google Scholar] [CrossRef]
- Yang, Y.; Zou, X.; Wang, Y.; Ma, X. Application of Deep Learning as a Noninvasive Tool to Differentiate Muscle-Invasive Bladder Cancer and Non-Muscle-Invasive Bladder Cancer with CT. Eur. J. Radiol. 2021, 139, 109666. [Google Scholar] [CrossRef]
- Liu, D.; Wang, S.; Wang, J. The Effect of CT High-Resolution Imaging Diagnosis Based on Deep Residual Network on the Pathology of Bladder Cancer Classification and Staging. Comput. Methods Programs Biomed. 2022, 215, 106635. [Google Scholar] [CrossRef]
- Taguchi, S.; Tambo, M.; Watanabe, M.; Machida, H.; Kariyasu, T.; Fukushima, K.; Shimizu, Y.; Okegawa, T.; Yokoyama, K.; Fukuhara, H. Prospective Validation of Vesical Imaging-Reporting and Data System Using a Next-Generation Magnetic Resonance Imaging Scanner-Is Denoising Deep Learning Reconstruction Useful? J. Urol. 2021, 205, 686–692. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Cai, L.; Chen, C.; Fu, X.; Wang, L.; Yuan, B.; Yang, X.; Lu, Q. Cascade Path Augmentation Unet for Bladder Cancer Segmentation in MRI. Med. Phys. 2022, 49, 4622–4631. [Google Scholar] [CrossRef] [PubMed]
- Cha, K.H.; Hadjiiski, L.M.; Cohan, R.H.; Chan, H.-P.; Caoili, E.M.; Davenport, M.S.; Samala, R.K.; Weizer, A.Z.; Alva, A.; Kirova-Nedyalkova, G.; et al. Diagnostic Accuracy of CT for Prediction of Bladder Cancer Treatment Response with and without Computerized Decision Support. Acad. Radiol. 2019, 26, 1137–1145. [Google Scholar] [CrossRef] [PubMed]
- Jansen, I.; Lucas, M.; Bosschieter, J.; de Boer, O.J.; Meijer, S.L.; van Leeuwen, T.G.; Marquering, H.A.; Nieuwenhuijzen, J.A.; de Bruin, D.M.; Savci-Heijink, C.D. Automated Detection and Grading of Non-Muscle-Invasive Urothelial Cell Carcinoma of the Bladder. Am. J. Pathol. 2020, 190, 1483–1490. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Jiang, L.; Zheng, X.; Shao, J.; Wang, T.; Zhang, E.; Gao, F.; Wang, X.; Zheng, J. Clinical Use of Machine Learning-Based Pathomics Signature for Diagnosis and Survival Prediction of Bladder Cancer. Cancer Sci. 2021, 112, 2905–2914. [Google Scholar] [CrossRef]
- Yin, P.-N.; Kc, K.; Wei, S.; Yu, Q.; Li, R.; Haake, A.R.; Miyamoto, H.; Cui, F. Histopathological Distinction of Non-Invasive and Invasive Bladder Cancers Using Machine Learning Approaches. BMC Med. Inform. Decis. Mak. 2020, 20, 162. [Google Scholar] [CrossRef] [PubMed]
- Harmon, S.A.; Sanford, T.H.; Brown, G.T.; Yang, C.; Mehralivand, S.; Jacob, J.M.; Valera, V.A.; Shih, J.H.; Agarwal, P.K.; Choyke, P.L.; et al. Multiresolution Application of Artificial Intelligence in Digital Pathology for Prediction of Positive Lymph Nodes From Primary Tumors in Bladder Cancer. JCO Clin. Cancer Inform. 2020, 4, 367–382. [Google Scholar] [CrossRef]
- Article, O. Comprehensive Molecular Characterization of Papillary Renal-Cell Carcinoma. N. Engl. J. Med. 2016, 374, 135–145. [Google Scholar] [CrossRef]
- Choi, W.; Porten, S.; Kim, S.; Willis, D.; Plimack, E.R.; Hoffman-Censits, J.; Roth, B.; Cheng, T.; Tran, M.; Lee, I.-L.; et al. Identification of Distinct Basal and Luminal Subtypes of Muscle-Invasive Bladder Cancer with Different Sensitivities to Frontline Chemotherapy. Cancer Cell 2014, 25, 152–165. [Google Scholar] [CrossRef]
- Sjödahl, G.; Eriksson, P.; Liedberg, F.; Höglund, M. Molecular Classification of Urothelial Carcinoma: Global MRNA Classification versus Tumour-Cell Phenotype Classification. J. Pathol. 2017, 242, 113–125. [Google Scholar] [CrossRef]
- Kardoust Parizi, M.; Margulis, V.; Lotan, Y.; Mori, K.; Shariat, S.F. Fibroblast Growth Factor Receptor: A Systematic Review and Meta-Analysis of Prognostic Value and Therapeutic Options in Patients with Urothelial Bladder Carcinoma. Urol. Oncol. 2021, 39, 409–421. [Google Scholar] [CrossRef] [PubMed]
- Loeffler, C.M.L.; Ortiz Bruechle, N.; Jung, M.; Seillier, L.; Rose, M.; Laleh, N.G.; Knuechel, R.; Brinker, T.J.; Trautwein, C.; Gaisa, N.T.; et al. Artificial Intelligence-Based Detection of FGFR3 Mutational Status Directly from Routine Histology in Bladder Cancer: A Possible Preselection for Molecular Testing? Eur. Urol. Focus 2022, 8, 472–479. [Google Scholar] [CrossRef] [PubMed]
- Velmahos, C.S.; Badgeley, M.; Lo, Y.-C. Using Deep Learning to Identify Bladder Cancers with FGFR-Activating Mutations from Histology Images. Cancer Med. 2021, 10, 4805–4813. [Google Scholar] [CrossRef]
- Xu, H.; Liu, Z.; Weng, S.; Dang, Q.; Ge, X.; Zhang, Y.; Ren, Y.; Xing, Z.; Chen, S.; Zhou, Y.; et al. Artificial Intelligence-Driven Consensus Gene Signatures for Improving Bladder Cancer Clinical Outcomes Identified by Multi-Center Integration Analysis. Mol. Oncol. 2022, 16, 4023–4042. [Google Scholar] [CrossRef]
- Wessels, F.; Kuntz, S.; Krieghoff-Henning, E.; Schmitt, M.; Braun, V.; Worst, T.S.; Neuberger, M.; Steeg, M.; Gaiser, T.; Fröhling, S.; et al. Artificial Intelligence to Predict Oncological Outcome Directly from Hematoxylin and Eosin-Stained Slides in Urology. Minerva Urol. Nephrol. 2022, 74, 538–550. [Google Scholar] [CrossRef]
- Hughes, C.; Iqbal-Wahid, J.; Brown, M.; Shanks, J.H.; Eustace, A.; Denley, H.; Hoskin, P.J.; West, C.; Clarke, N.W.; Gardner, P. FTIR Microspectroscopy of Selected Rare Diverse Sub-Variants of Carcinoma of the Urinary Bladder. J. Biophotonics 2013, 6, 73–87. [Google Scholar] [CrossRef]
- Sokolov, I.; Dokukin, M.E.; Kalaparthi, V.; Miljkovic, M.; Wang, A.; Seigne, J.D.; Grivas, P.; Demidenko, E. Noninvasive Diagnostic Imaging Using Machine-Learning Analysis of Nanoresolution Images of Cell Surfaces: Detection of Bladder Cancer. Proc. Natl. Acad. Sci. USA 2018, 115, 12920–12925. [Google Scholar] [CrossRef]
- Joshi, G.; Jain, A.; Adhikari, S.; Garg, H.; Bhandari, M. FDA Approved Artificial Intelligence and Machine Learning (AI/ML)-Enabled Medical Devices: An Updated 2022 Landscape; Health Informatics: Glenn Dale, MD, USA, 2022. [Google Scholar] [CrossRef]


{kind=link}
| Author | Year | Patients/Images | AI Technology | Outcomes |
|---|---|---|---|---|
| Shkolyar et al. [26] | 2019 | 95 patients/2752 frames (internal) | CystoNet | Prospective validation in an additional cohort of 54 patients. Per-frame sensitivity and specificity: 90.9% (95% CI, 90.3–91.6%) and 98.6% (95% CI, 98.5–98.8%), respectively. Per-tumor sensitivity: 90.9% (95% CI, 90.3–91.6%). CystoNet detected 39 of 41 papillary and 3 of 3 flat BCas. |
| Du et al. [35] | 2020 | 175 patients/1736 frames | Caffe deep learning framework and EasyDL platform | Accuracy rate in BCa detection: 82.9% based on Caffe framework, 96.9% on the EasyDL platform. |
| Ali et al. [32] | 2021 | 216 blue-light frames (multicentric, from 4 urological departments) | InceptionV3 network, MobileNetV2 network, ResNet50 network, VGG16 network | Classification of malignant lesions sensitivity/specificity: 95.77% and 87.84% respectively; tumor invasiveness mean sensitivity/specificity: 88% and 96.56%, respectively. |
| Ikeda et al. [34] | 2021 | 2104 frames (external—ImageNet data set) | GoogLeNet | 95.4% sensitivity and 97.6% specificity (superior diagnostic accuracy when tumors occupied >10% of the image) |
| S. Wu et al. [27] | 2021 | 10,729 patients/69,204 frames | Cystoscopy Artificial Intelligence Diagnostic System (CAIDS) | CIADS diagnostic accuracies: 0.977 (95% CI 1⁄4 0.974 to 0.979) in the internal validation set and 0.990 (95% CI 1⁄4 0.979 to 0.996), 0.982 (95% CI 1⁄4 0.974 to 0.988), 0.978 (95% CI 1⁄4 0.959 to 0.989), and 0.991 (95% CI 1⁄4 0.987 to 0.994) in different external validation sets.CAIDS vs. urologist comparisons: high accuracy and sensitivity (accuracy 1⁄4 0.939, 95% CI 1⁄4 0.902 to 0.964; sensitivity 1⁄4 0.954, 95% CI 1⁄4 0.902 to 0.983) with a short latency of 12 s, which was more accurate and quicker than the expert urologists. |
| Yoo et al. [28] | 2022 | 1310 patients/10,991 frames | Mask RCNN with a ResNeXt-101-32 × 8d-FPN backbone | Sensitivity, specificity, diagnostic accuracy, and DSC of AI: 95.0%, 93.7%, 94.1%, and 74.7%, respectively. AI-diagnostic performance in WLI: ≥98% benign vs. low-and high-grade tumors, >90% non-specific inflammation vs. carcinoma in situ. |
| Mutaguchi et al. [29] | 2022 | 120 patients/1790 frames | Dilated U-Net | Overlooking bladder tumors risk reduction: PWSe, PWSp, PWPPV, and DSC of the dilated U-Net were 84.9%, 88.5%, 86.7%, and 83.0%, respectively. |
| Author | Year | Imaging | Patients/Frames | AI Technology | Outcomes |
|---|---|---|---|---|---|
| Cha et al. [43] | 2018 | CT | 123 patients/157 ROI (MIBC foci) | CDSS-T | Mean AUCs for the assessment of pathologic T0 disease after NAC in MIBC: 0.80 for CDSS-T alone, 0.74 for physicians not using CDSS-T, and 0.77 for physicians using CDSS-T. The increase in the physicians’ performance was statistically significant (p < 0.05). |
| Zhang et al. [38] | 2021 | CT | 441 patients | Filter-guided Pyramid Network (FGP-Net) | Prediction ability of muscle-invasive status: sensitivity: 0.733, specificity: 0.810 (internal validation cohort); sensitivity 0.710, specificity 0.773 (external validation cohort). |
| Taguchi et al. [41] | 2021 | T2W MRI | 98 patients | “Next-generation” 3T-MRI with dDLR | The optimal cut-off value of the VI-RADS score was determined to be 4, and the accuracy of diagnosing MIBC by VI-RADS 4 was 94% (AUC 0.92). The AUC for assessment of final VI-RADS score was significantly improved from 0.84 with T2WI alone to 0.88 with T2WI + dDLR (p < 0.01). |
| Yang et al. [39] | 2021 | CT | 369 patients/1200 cross-sectional CT frames | VGG16, VGG19, Xception, InceptionV3, InceptionResNetV2, Dense-Net121, DenseNet169, DenseNet201 | Ability to classify MIBC vs. NMICB: the AUC of the validation and testing datasets for the small DL-CNN was 0.946 and 0.998, respectively. The AUROCs of eight deep learning algorithms with pretrained bases ranged from 0.762 to 0.997 in the testing dataset. The VGG16 model had the largest AUROC of 0.997 among the eight algorithms with a sensitivity and specificity of 0.889 and 0.989, respectively. |
| Liu et al. [40] | 2022 | CT | 76 patients | ResNet18 network | To predict BCa staging through DL enhanced high-resolution CT scans: 52 cases were diagnosed <T1 stage, 16 cases belonged to T2 stage, 2 cases T3 stage, and 2 cases T4 stage. The sensitivity rate of experimental diagnosis was 94.74%, which was not significantly different from the sensitivity rate of preoperative pathological diagnosis. |
| Yu et al. [42] | 2022 | T2W MRI | 1545 T2-weighted MRI scans | CPA-Unet network | Segmentation accuracy of IW, OW, and BCa through MRI scans: CPA-Unet achieves superior segmentation results in terms of DSC and HD (IW:DSC = 98.19%, HD = 2.07 mm; OW:DSC = 82.24%, HD = 2.62 mm; BCa:DSC = 87.40%, HD = 0.76 mm). |
| Author | Year | H&E Stains | Specimen | AI Technology | Outcomes |
|---|---|---|---|---|---|
| Jansen et al. [44] | 2020 | 328 | TURBt | U-Net based seg- mentation network—deep learning | Automated classification correctly graded 76% low-grade cancers and 71% high-grade cancers |
| Chen et al. [45] | 2021 | 643 | Radical/partial cystectomy | Machine learning algorithm | Cross-verified automatic diagnosis accuracy: AUC of 96.3%, 89.2%, and 94.1% (for three testing cohorts), prognosis accuracy: AUC values of 77.7%, 83.8%, and 81.3% (for 1-, 3-, and 5-y overall survival prediction of patients with BCa) |
| Yin et al. [46] | 2020 | 1177 | Surgical excision | Imaging processing software: ImageJ and CellProfiler—Machine learning | Distinguish between Ta or T1 images with six supervised learning methods (91–96% accuracy) vs. CNN (84% accuracy) |
| Harmon et al. [47] | 2020 | 307 | Radical cystectomy | DL (ResNet-101) | Comparison on likelihood of positive lymph nodes between clinicopathologic model vs. AI score respectively (AUC of 0.755, 95% CI 0.680 to 0.831 vs. AUC of 0.866, 95% CI 0.812 to 0.920; p = 0.021) |
| Author | Year | Pathway/Genes | AI Technology | Outcomes |
|---|---|---|---|---|
| Loeffler et al. [52] | 2021 | FGFR3/327 | DL network | The accuracy in detecting FGFR3 mutations in the three cohorts were 0.701 (p < 0.0001), 0.725 (p < 0.0001), and 0.625 (p = 0.0112) |
| Xu et al. [54] | 2022 | 1218 | ML AIGS (artificial intelligence-derived gene signature) | AIGS demonstrated superior performance among 76 model types: higher risk of mortality, recurrence, and disease progression. AIGS demonstrated superior performance on clinical traits and molecular features |
| Velmahos et al. [53] | 2021 | FGFR/418 | Convolutional neural network (CNN) identified tumor-infiltrating lymphocytes (TIL)—DL | Predictive model identifies patients with FGFR gene aberrations with a sensitivity of 0.89, specificity of 0.42, and AUROC = 0.76. A similar model predicting FGFR2/FGFR3 mutation was also highly sensitive and specific (sensitivity = 0.82, specificity = 0.85, AUROC = 0.86) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rossin, G.; Zorzi, F.; Ongaro, L.; Piasentin, A.; Vedovo, F.; Liguori, G.; Zucchi, A.; Simonato, A.; Bartoletti, R.; Trombetta, C.; et al. Artificial Intelligence in Bladder Cancer Diagnosis: Current Applications and Future Perspectives. BioMedInformatics 2023, 3, 104-114. https://doi.org/10.3390/biomedinformatics3010008
Rossin G, Zorzi F, Ongaro L, Piasentin A, Vedovo F, Liguori G, Zucchi A, Simonato A, Bartoletti R, Trombetta C, et al. Artificial Intelligence in Bladder Cancer Diagnosis: Current Applications and Future Perspectives. BioMedInformatics. 2023; 3(1):104-114. https://doi.org/10.3390/biomedinformatics3010008
Chicago/Turabian StyleRossin, Giulio, Federico Zorzi, Luca Ongaro, Andrea Piasentin, Francesca Vedovo, Giovanni Liguori, Alessandro Zucchi, Alchiede Simonato, Riccardo Bartoletti, Carlo Trombetta, and et al. 2023. "Artificial Intelligence in Bladder Cancer Diagnosis: Current Applications and Future Perspectives" BioMedInformatics 3, no. 1: 104-114. https://doi.org/10.3390/biomedinformatics3010008
APA StyleRossin, G., Zorzi, F., Ongaro, L., Piasentin, A., Vedovo, F., Liguori, G., Zucchi, A., Simonato, A., Bartoletti, R., Trombetta, C., Pavan, N., & Claps, F. (2023). Artificial Intelligence in Bladder Cancer Diagnosis: Current Applications and Future Perspectives. BioMedInformatics, 3(1), 104-114. https://doi.org/10.3390/biomedinformatics3010008