

Benefits of Table Tennis for Brain Health Maintenance and Prevention of Dementia


Abstract
:1. Introduction
2. Literature Search Strategy
3. Characteristics of Table Tennis
3.1. The Concept of Table Tennis
3.2. Game Dynamics
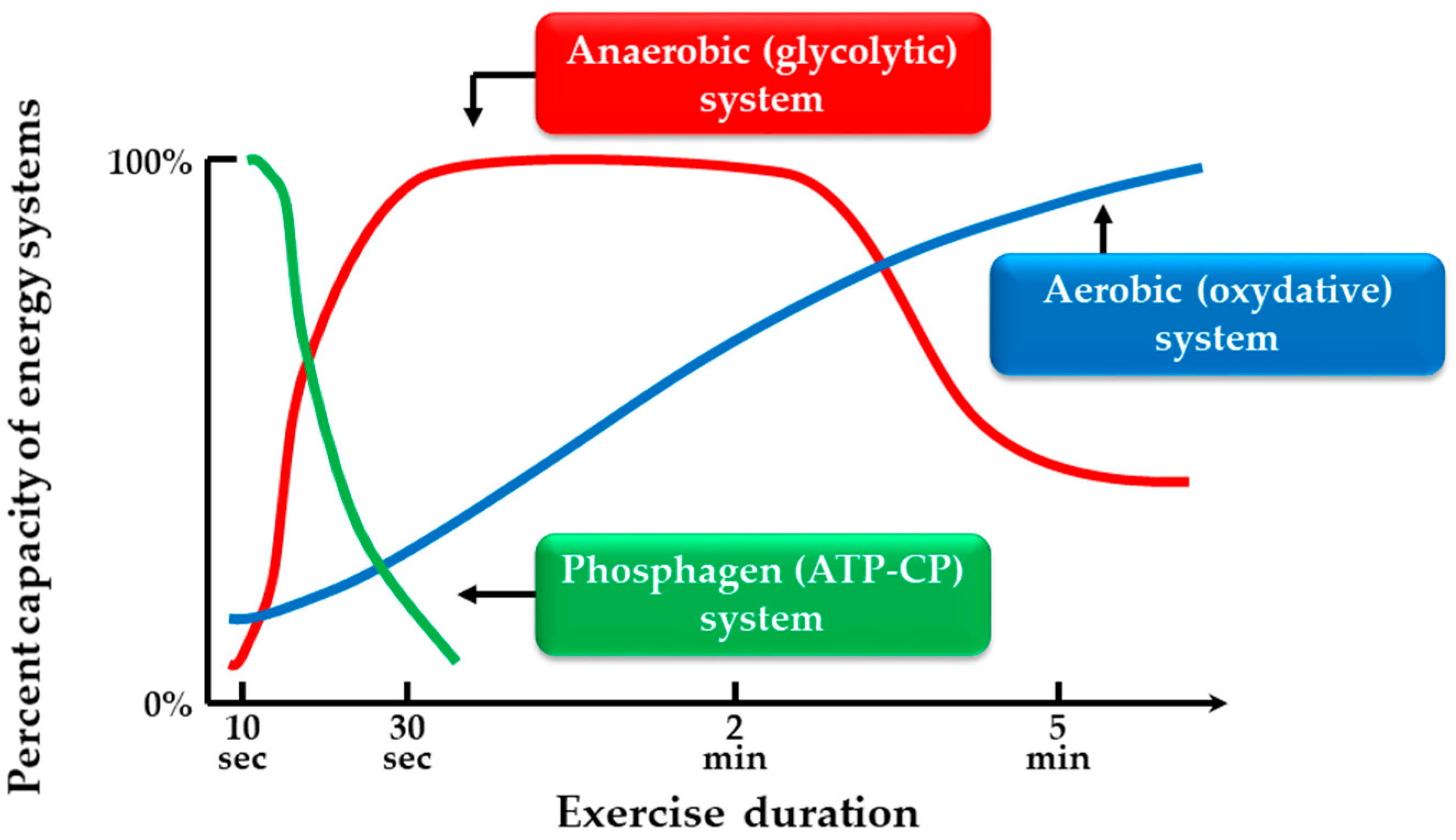
3.3. Three Basic Energy Systems in Humans
3.4. Measurement of Exercise Intensity
3.5. Physiological Responses during Table Tennis
4. Benefits of Table Tennis for Physical and Brain Health
4.1. Benefits of Table Tennis for Physical Health
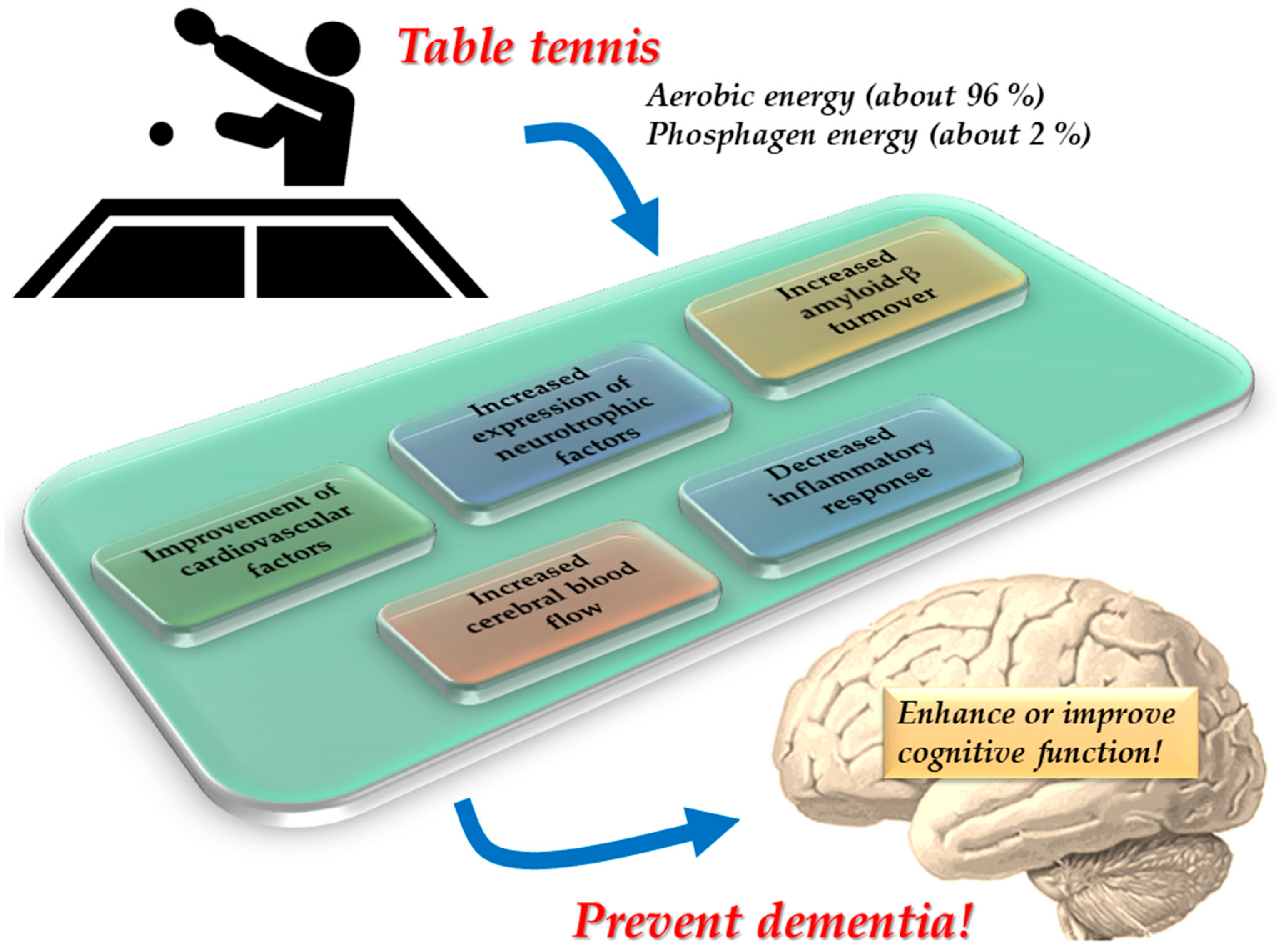
4.2. Benefits of Table Tennis for Brain Health
5. Effectiveness of Table Tennis Intervention in the Prevention of Cognitive Decline and Dementia
5.1. Physical Activity Interventions for the Prevention of Cognitive Decline and Dementia
5.2. Mechanisms Underlying the Benefits of Physical Activity Interventions for Cognitive Decline and Dementia Prevention
5.3. Table Tennis Intervention for Prevention of Cognitive Decline and Dementia
6. Conclusions and Prospects
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pradas, F.; de la Torre, A.; Castellar, C.; Toro-Román, V. Physiological profile, metabolic response and temporal structure in elite individual table tennis: Differences according to gender. Int. J. Environ. Res. Public Health 2021, 18, 11898. [Google Scholar] [CrossRef] [PubMed]
- Pradas, F.; Ara, I.; Toro, V.; Courel-Ibáñez, J. Benefits of regular table tennis practice in body composition and physical fitness compared to physically active children aged 10–11 years. Int. J. Environ. Res. Public Health 2021, 18, 2854. [Google Scholar] [CrossRef] [PubMed]
- Picabea, J.M.; Cámara, J.; Yanci, J. Physical fitness profiling of national category table tennis players: Implication for health and performance. Int. J. Environ. Res. Public Health 2021, 18, 9362. [Google Scholar] [CrossRef] [PubMed]
- The International Table Tennis Federation. ITTF Handbook 2022, 50th ed.; The International Table Tennis Federation: Lausanne, Switzerland, 2022. [Google Scholar]
- Mousset, K.; Violette, L.; Épron, A. The ITTF and Olympic recognition of table tennis: From pure amateurism to the Asian markets (1926–1988). Sport Hist. 2021, 41, 578–595. [Google Scholar] [CrossRef]
- Wang, Y.P.; Chen, G. Table Tennis, 2nd ed.; XanEdu Publishing Company: Ann Arbor, MI, USA, 2006. [Google Scholar]
- Biernat, E.; Buchholtz, S.; Krzepota, J. Eye on the ball: Table tennis as a pro-health form of leisure-time physical activity. Int. J. Environ. Res. Public Health 2018, 15, 738. [Google Scholar] [CrossRef]
- Naderi, A.; Zagatto, A.M.; Akbari, F.; Sakinepoor, A. Body composition and lipid profile of regular recreational table tennis participants: A cross-sectional study of older adult men. Sport Sci. Health 2021, 41, 578–595. [Google Scholar] [CrossRef]
- Jeoung, B.J. Relationships of exercise with frailty, depression, and cognitive function in older women. J. Exerc. Rehabil. 2014, 10, 291–294. [Google Scholar] [CrossRef]
- Shimomura, M.; Hamazaki, H.; Nohara, R.; Fujiwara, H. Effective use of table tennis for patients with chronic ischemic heart disease. Jpn. J. Adapt. Sport Sci. 2004, 2, 38–44. [Google Scholar]
- Inoue, K.; Fujioka, S.; Nagaki, K.; Suenaga, M.; Kimura, K.; Yonekura, Y.; Yamaguchi, Y.; Kitano, K.; Imamura, R.; Uehara, Y.; et al. Table tennis for patients with Parkinson’s disease: A single-center, prospective pilot study. Clin. Park. Relat. Disord. 2021, 4, 100086. [Google Scholar] [CrossRef]
- Pan, C.Y.; Chu, C.H.; Tsai, C.L.; Sung, M.C.; Huang, C.Y.; Ma, W.Y. The impacts of physical activity on physical and cognitive outcomes in children with autism spectrum disorder. Autism 2017, 21, 190–202. [Google Scholar] [CrossRef]
- Pan, C.Y.; Tsai, C.L.; Chu, C.H.; Sung, M.C.; Huang, C.Y.; Ma, W.Y. Effects of physical exercise intervention on motor skills and executive functions in children with ADHD: A pilot study. J. Atten. Disord. 2019, 23, 384–397. [Google Scholar] [CrossRef]
- Chen, M.D.; Tsai, H.Y.; Wang, C.C.; Wuang, Y.P. The effectiveness of racket-sport intervention on visual perception and executive functions in children with mild intellectual disabilities and borderline intellectual functioning. Neuropsychiatr. Dis. Treat. 2015, 11, 2287–2297. [Google Scholar]
- World Health Organization. Dementia. Available online: https://www.who.int/en/news-room/fact-sheets/detail/dementia (accessed on 30 August 2022).
- Alzheimer’s Association. 2022 Alzheimer’s disease facts and figures. Alzheimers Dement. 2022, 18, 700–789. [Google Scholar] [CrossRef]
- Petersen, R.C.; Doody, R.; Kurz, A.; Mohs, R.C.; Morris, J.C.; Rabins, P.V.; Ritchie, K.; Rossor, M.; Thal, L.; Winblad, B. Current concepts in mild cognitive impairment. Arch. Neurol. 2001, 58, 1985–1992. [Google Scholar] [CrossRef]
- Nuzum, H.; Stickel, A.; Corona, M.; Zeller, M.; Melrose, R.J.; Wilkins, S.S. Potential benefits of physical activity in MCI and dementia. Behav. Neurol. 2020, 2020, 7807856. [Google Scholar] [CrossRef]
- Mori, T.; Sato, T. Clinical brain sports medicine. Biomechanisms 2004, 17, 1–8. [Google Scholar] [CrossRef]
- Japan Table Tennis Therapy Association. Available online: https://www.takkyu-ryoho.or.jp/ (accessed on 30 August 2022).
- Elferink-Gemser, M.T.; Faber, I.R.; Visscher, C.; Hung, T.M.; de Vries, S.J.; Nijhuis-Van der Sanden, M.W.G. High-level cognitive functions in Dutch elite and sub-elite table tennis players. PLoS ONE 2018, 13, e0206151. [Google Scholar]
- Zagatto, A.M.; Morel, E.A.; Gobatto, C.A. Physiological responses and characteristics of table tennis matches determined in official tournaments. J. Strength Cond. Res. 2010, 24, 942–949. [Google Scholar] [CrossRef]
- Zagatto, A.M.; Kondric, M.; Knechtle, B.; Nikolaidis, P.T.; Sperlich, B. Energetic demand and physical conditioning of table tennis players. A study review. J. Sports Sci. 2018, 36, 724–731. [Google Scholar] [CrossRef]
- Belli, T.; Misuta, M.S.; de Moura, P.P.R.; Tavares, T.S.; Ribeiro, R.A.; Santos, Y.Y.S.; Sarro, K.J.; Galatti, L.R. Reproducibility and validity of a stroke effectiveness test in table tennis based on the temporal game structure. Front. Psychol. 2019, 10, 427. [Google Scholar] [CrossRef]
- Swanwick, E.; Matthews, M. Energy systems: A new look at aerobic metabolism in stressful exercise. MOJ Sports Med. 2018, 2, 15–22. [Google Scholar] [CrossRef]
- Wells, G.D.; Selvadurai, H.; Tein, I. Bioenergetic provision of energy for muscular activity. Paediatr. Respir. Rev. 2009, 10, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Gastin, P.B. Energy system interaction and relative contribution during maximal exercise. Sports Med. 2001, 31, 725–741. [Google Scholar] [CrossRef] [PubMed]
- Vaquera, A.; Refoyo, I.; Villa, J.G.; Calleja, J.; Rodríguez-Marroyo, J.A.; García-López, J.; Sampedro, J. Heart rate response to game-play in professional basketball players. J. Hum. Sport Exerc. 2008, 3, 9. [Google Scholar]
- Suchomel, A. Aerobic capacity and exercise intensity on different player levels in tennis. Sport Sci. Rev. 2010, 19, 21–29. [Google Scholar] [CrossRef]
- Jetté, M.; Sidney, K.; Blümchen, G. Metabolic equivalents (METS) in exercise testing, exercise prescription, and evaluation of functional capacity. Clin. Cardiol. 1990, 13, 555–565. [Google Scholar] [CrossRef]
- Vanhees, L.; Geladas, N.; Hansen, D.; Kouidi, E.; Niebauer, J.; Reiner, Ž.; Cornelissen, V.; Adamopoulos, S.; Prescott, E.; Börjesson, M. Importance of characteristics and modalities of physical activity and exercise in the management of cardiovascular health in individuals with cardiovascular risk factors: Recommendations from the EACPR (Part II). Eur. J. Prev. Cardiol. 2012, 19, 1005–1033. [Google Scholar] [CrossRef]
- Milioni, F.; Leite, J.V.d.M.; Beneke, R.; de Poli, R.A.B.; Papoti, M.; Zagatto, A.M. Table tennis playing styles require specific energy systems demands. PLoS ONE 2018, 13, e0199985. [Google Scholar] [CrossRef]
- Sperlich, B.; Koehler, K.; Holmberg, H.C.; Zinner, C.; Mester, J. Table tennis: Cardiorespiratory and metabolic analysis of match and exercise in elite junior national players. Int. J. Sports Physiol. Perform. 2011, 6, 234–242. [Google Scholar] [CrossRef]
- Zagatto, A.M.; de Mello Leite, J.V.; Papoti, M.; Beneke, R. Energetics of table tennis and table tennis specific exercise testing. Int. J. Sports Physiol. Perform. 2016, 11, 1012–1017. [Google Scholar] [CrossRef]
- Kondrič, M.; Zagatto, A.M.; Sekulić, D. The physiological demands of table tennis: A review. J. Sports Sci. Med. 2013, 12, 362–370. [Google Scholar]
- Zagatto, A.M.; Milioni, F.; Freitas, I.F.; Arcangelo, S.A.; Padulo, J. Body composition of table tennis players: Comparison between performance level and gender. Sport Sci. Health 2016, 12, 49–54. [Google Scholar] [CrossRef]
- Naderi, A.; Degens, H.; Rezvani, M.H.; Shaabani, F. A retrospective comparison of physical health in regular recreational table tennis participants and sedentary elderly men. J. Musculoskelet. Neuronal Interact. 2018, 18, 200–207. [Google Scholar]
- Pradas, F.; de la Torre, A.; Carrasco, L.; Muñoz, D.; Courel-Ibáñez, J.; González-Jurado, A. Anthropometric profiles in table tennis players: Analysis of sex, age, and ranking. Appl. Sci. 2021, 11, 876. [Google Scholar] [CrossRef]
- Carius, D.; Kenville, R.; Maudrich, D.; Riechel, J.; Lenz, H.; Patrick, R. Cortical processing druing table tennis-an fNIRS study in experts and novices. Eur. J. Sports Sci. 2021, 17, 1315–1325. [Google Scholar]
- Balardin, J.B.; Zimeo Morais, G.A.; Furucho, R.A.; Trambaiolli, L.; Vanzella, P.; Biazoli, C., Jr.; Sato, J.R. Imaging brain function with functional near-infrared spectroscopy in unconstrained environments. Front. Hum. Neurosci. 2017, 11, 258. [Google Scholar] [CrossRef]
- Visser, A.; Büchel, D.; Lehmann, T.; Baumeister, J. Continuous table tennis is associated with processing in frontal brain areas: An EEG approach. Exp. Brain Res. 2022, 240, 1899–1909. [Google Scholar] [CrossRef]
- Kawano, M.M.; Mimura, K.; Kaneko, M. The effect of table tennis practice on mental ability evaluated by Kana-Pick-out test. Int. J. Table Tennis Sci. 1992, 1, 57–62. [Google Scholar]
- Wang, B.; Guo, W.; Zhou, C. Selective enhancement of attentional networks in college table tennis athletes: A preliminary investigation. PeerJ 2016, 4, e2762. [Google Scholar] [CrossRef]
- Wolf, S.; Brölz, E.; Scholz, D.; Ramos-Murguialday, A.; Keune, P.M.; Hautzinger, M.; Birbaumer, N.; Strehl, U. Winning the game: Brain processes in expert, young elite and amateur table tennis players. Front. Behav. Neurosci. 2014, 8, 370. [Google Scholar] [CrossRef]
- Hülsdünker, T.; Ostermann, M.; Mierau, A. The speed of neural visual motion perception and processing determines the visuomotor reaction time of young elite table tennis athletes. Front. Behav. Neurosci. 2019, 13, 165. [Google Scholar] [CrossRef]
- Gao, Q.; Huang, Y.; Xiang, Y.; Yang, C.; Zhang, M.; Guo, J.; Wang, H.; Yu, J.; Cui, Q.; Chen, H. Altered dynamics of functional connectivity density associated with early and advanced stages of motor training in tennis and table tennis athletes. Brain Imaging Behav. 2021, 15, 1323–1334. [Google Scholar] [CrossRef]
- Guo, Z.; Li, A.; Yu, L. “Neural efficiency” of athletes’ brain during visuo-spatial task: An fMRI study on table tennis players. Front. Behav. Neurosci. 2017, 11, 72. [Google Scholar] [CrossRef]
- Yin, D.; Wang, X.; Zhang, X.; Yu, Q.; Wei, Y.; Cai, Q.; Fan, M.; Li, L. Dissociable plasticity of visual-motor system in functional specialization and flexibility in expert table tennis players. Brain Struct. Funct. 2021, 226, 1973–1990. [Google Scholar] [CrossRef]
- World Health Organization. Risk Reduction of Cognitive Decline and Dementia. WHO Guidelines; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Colcombe, S.; Kramer, A.F. Fitness effects on the cognitive function of older adults: A meta-analytic study. Psychol. Sci. 2003, 14, 125–130. [Google Scholar] [CrossRef]
- Smith, P.J.; Blumenthal, J.A.; Hoffman, B.M.; Cooper, H.; Strauman, T.A.; Welsh-Bohmer, K.; Browndyke, J.N. Aerobic exercise and neurocognitive performance: A meta-analytic review of randomized controlled trials. Psychosom. Med. 2010, 72, 239–252. [Google Scholar] [CrossRef]
- Erickson, K.I.; Hillman, C.; Stillman, C.M.; Ballard, R.M.; Bloodgood, B.; Conroy, D.E.; Macko, R.; Marquez, D.X.; Petruzzello, S.J.; Powell, K.E.; et al. Physical activity, cognition, and brain outcomes: A review of the 2018 physical activity guidelines. Med. Sci. Sports Exerc. 2019, 51, 1242–1251. [Google Scholar] [CrossRef]
- Chen, F.T.; Hopman, R.J.; Huang, C.J.; Chu, C.H.; Hillman, C.H.; Hung, T.M.; Chang, Y.K. The effect of exercise training on brain structure and function in older adults: A systematic review based on evidence from randomized control trials. J. Clin. Med. 2020, 9, 914. [Google Scholar] [CrossRef] [Green Version]
- Srinivas, N.S.; Vimalan, V.; Padmanabhan, P.; Gulyás, B. An overview on cognitive function enhancement through physical exercises. Brain Sci. 2021, 11, 1289. [Google Scholar] [CrossRef]
- Öhman, H.; Savikko, N.; Strandberg, T.E.; Pitkälä, K.H. Effect of physical exercise on cognitive performance in older adults with mild cognitive impairment or dementia: A systematic review. Dement. Geriatr. Cogn. Disord. 2014, 38, 347–365. [Google Scholar] [CrossRef]
- Suzuki, T.; Shimada, H.; Makizako, H.; Doi, T.; Yoshida, D.; Ito, K.; Shimokata, H.; Washimi, Y.; Endo, H.; Kato, T. A randomized controlled trial of multicomponent exercise in older adults with mild cognitive impairment. PLoS ONE 2013, 8, e61483. [Google Scholar] [CrossRef] [PubMed]
- Heyn, P.; Abreu, B.C.; Ottenbacher, K.J. The effects of exercise training on elderly persons with cognitive impairment and dementia: A meta-analysis. Arch. Phys. Med. Rehabil. 2004, 85, 1694–1704. [Google Scholar] [CrossRef] [PubMed]
- Demurtas, J.; Schoene, D.; Torbahn, G.; Marengoni, A.; Grande, G.; Zou, L.; Petrovic, M.; Maggi, S.; Cesari, M.; Lamb, S.; et al. Physical activity and exercise in mild cognitive impairment and dementia: An umbrella review of intervention and observational studies. J. Am. Med. Dir. Assoc. 2020, 21, 1415–1422.e6. [Google Scholar] [CrossRef] [PubMed]
- Forbes, D.; Thiessen, E.J.; Blake, C.M.; Forbes, S.C.; Forbes, S. Exercise programs for people with dementia. Cochrane Database Syst. Rev. 2013, 12, CD006489. [Google Scholar]
- Forbes, D.; Forbes, S.C.; Blake, C.M.; Thiessen, E.J.; Forbes, S. Exercise programs for people with dementia. Cochrane Database Syst. Rev. 2015, 4, CD006489. [Google Scholar] [CrossRef]
- De la Rosa, A.; Olaso-Gonzalez, G.; Arc-Chagnaud, C.; Millan, F.; Salvador-Pascual, A.; García-Lucerga, C.; Blasco-Lafarga, C.; Garcia-Dominguez, E.; Carretero, A.; Correas, A.G.; et al. Physical exercise in the prevention and treatment of Alzheimer’s disease. J. Sport Health Sci. 2020, 9, 394–404. [Google Scholar] [CrossRef]
- Kim, Y.J.; Han, K.D.; Baek, M.S.; Cho, H.; Lee, E.J.; Lyoo, C.H. Association between physical activity and conversion from mild cognitive impairment to dementia. Alzheimers Res. Ther. 2020, 12, 136. [Google Scholar] [CrossRef]
- Di Liegro, C.M.; Schiera, G.; Proia, P.; Di Liegro, I. Physical activity and brain health. Genes 2019, 10, 720. [Google Scholar] [CrossRef]
- Gu, Q.; Zou, L.; Loprinzi, P.D.; Quan, M.; Huang, T. Effects of open versus closed skill exercise on cognitive function: A systematic review. Front. Psychol. 2019, 10, 1707. [Google Scholar] [CrossRef] [Green Version]
- Hung, C.L.; Tseng, J.W.; Chao, H.H.; Hung, T.M.; Wang, H.S. Effect of acute exercise mode on serum brain-derived neurotrophic factor (BDNF) and task switching performance. J. Clin. Med. 2018, 7, 301. [Google Scholar] [CrossRef]
- Erickson, K.I.; Voss, M.W.; Prakash, R.S.; Basak, C.; Szabo, A.; Chaddock, L.; Kim, J.S.; Heo, S.; Alves, H.; White, S.M.; et al. Exercise training increases size of hippocampus and improves memory. Proc. Natl. Acad. Sci. USA 2011, 108, 3017–3022. [Google Scholar] [CrossRef]
- Stillman, C.M.; Lopez, O.L.; Becker, J.T.; Kuller, L.H.; Mehta, P.D.; Tracy, R.P.; Erickson, K.I. Physical activity predicts reduced plasma β amyloid in the cardiovascular health study. Ann. Clin. Transl. Neurol. 2017, 4, 284–291. [Google Scholar] [CrossRef]
- Liang, K.Y.; Mintun, M.A.; Fagan, A.M.; Goate, A.M.; Bugg, J.M.; Holtzman, D.M.; Morris, J.C.; Head, D. Exercise and Alzheimer’s disease biomarkers in cognitively normal older adults. Ann. Neurol. 2010, 68, 311–318. [Google Scholar] [CrossRef]
- Bounce Alzheimer’s Therapy Foundation. Available online: https://www.batfoundation.com/ (accessed on 30 August 2022).
- Suzuki, T.; Shimada, H.; Makizako, H.; Doi, T.; Yoshida, D.; Tsutsumimoto, K.; Anan, Y.; Uemura, K.; Lee, S.; Park, H. Effects of multicomponent exercise on cognitive function in older adults with amnestic mild cognitive impairment: A randomized controlled trial. BMC Neurol. 2012, 12, 128. [Google Scholar] [CrossRef]
- Suzuki, T.; Makizako, H.; Doi, T.; Park, H.; Lee, S.; Tsutsumimoto, K.; Umemura, K.; Maki, Y.; Shimada, H. Community-based intervention for prevention of dementia in Japan. J. Prev. Alzheimers Dis. 2015, 2, 71–76. [Google Scholar] [CrossRef]
- Shimada, H.; Makizako, H.; Doi, T.; Park, H.; Tsutsumimoto, K.; Verghese, J.; Suzuki, T. Effects of combined physical and cognitive exercises on cognition and mobility in patients with mild cognitive impairment: A randomized clinical trial. J. Am. Med. Dir. Assoc. 2018, 19, 584–591. [Google Scholar] [CrossRef]
- Ludyga, S.; Gerber, M.; Pühse, U.; Looser, V.N.; Kamijo, K. Systematic review and meta-analysis investigating moderators of long-term effects of exercise on cognition in healthy individuals. Nat. Hum. Behav. 2020, 4, 603–612. [Google Scholar] [CrossRef]
- Kasai, J.I.; Akira, O.; Eung, J.T.; Mori, T. Research on table tennis player’s cardio-respiratory endurance. Int. J. Table Tennis Sci. 2010, 6, 6–8. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Intensity | %HRmax (%) | %VO2max (%) | METs | Lactate (mmol/L) |
|---|---|---|---|---|
| Low intensity, light effort | 45–54 | 28–39 | 2–4 | 2–3 |
| Moderate intensity, moderate effort | 55–69 | 40–59 | 4–6 | 4–5 |
| High intensity, vigorous effect | 70–89 | 60–79 | 6–8 | 6–8 |
| Very hard effort | >89 | >80 | 8–10 | 8–10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamasaki, T. Benefits of Table Tennis for Brain Health Maintenance and Prevention of Dementia. Encyclopedia 2022, 2, 1577-1589. https://doi.org/10.3390/encyclopedia2030107
Yamasaki T. Benefits of Table Tennis for Brain Health Maintenance and Prevention of Dementia. Encyclopedia. 2022; 2(3):1577-1589. https://doi.org/10.3390/encyclopedia2030107
Chicago/Turabian StyleYamasaki, Takao. 2022. "Benefits of Table Tennis for Brain Health Maintenance and Prevention of Dementia" Encyclopedia 2, no. 3: 1577-1589. https://doi.org/10.3390/encyclopedia2030107
APA StyleYamasaki, T. (2022). Benefits of Table Tennis for Brain Health Maintenance and Prevention of Dementia. Encyclopedia, 2(3), 1577-1589. https://doi.org/10.3390/encyclopedia2030107