

The Lymphatic System—A Surgeon’s Point of View


Abstract
:1. Introduction
2. Imaging for Diagnosis
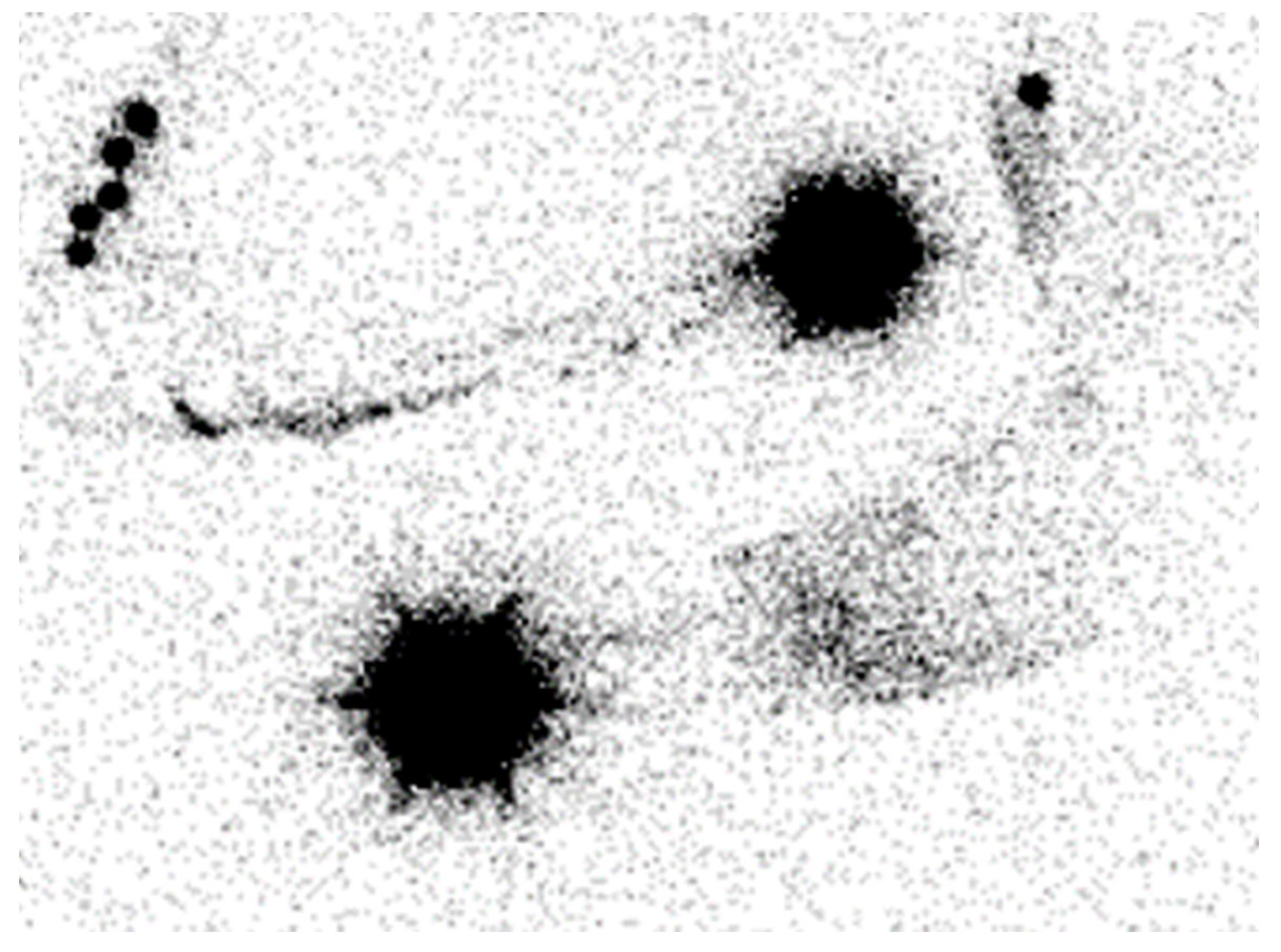
2.1. Lymphoscintigraphy
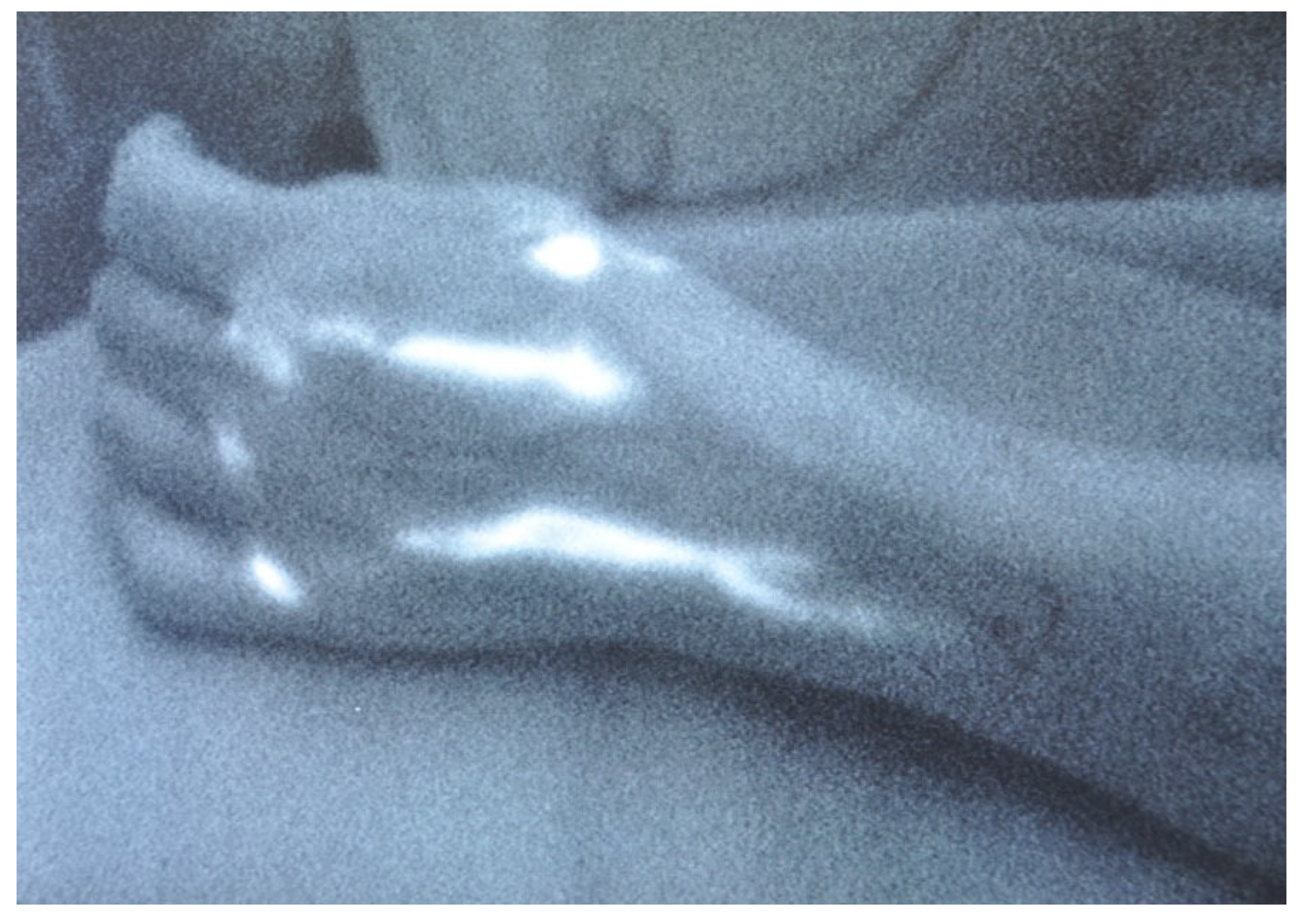
2.2. Indocyanine Green Lymphography
3. Imaging for Treatment
3.1. Indocyanine Green Lymphography
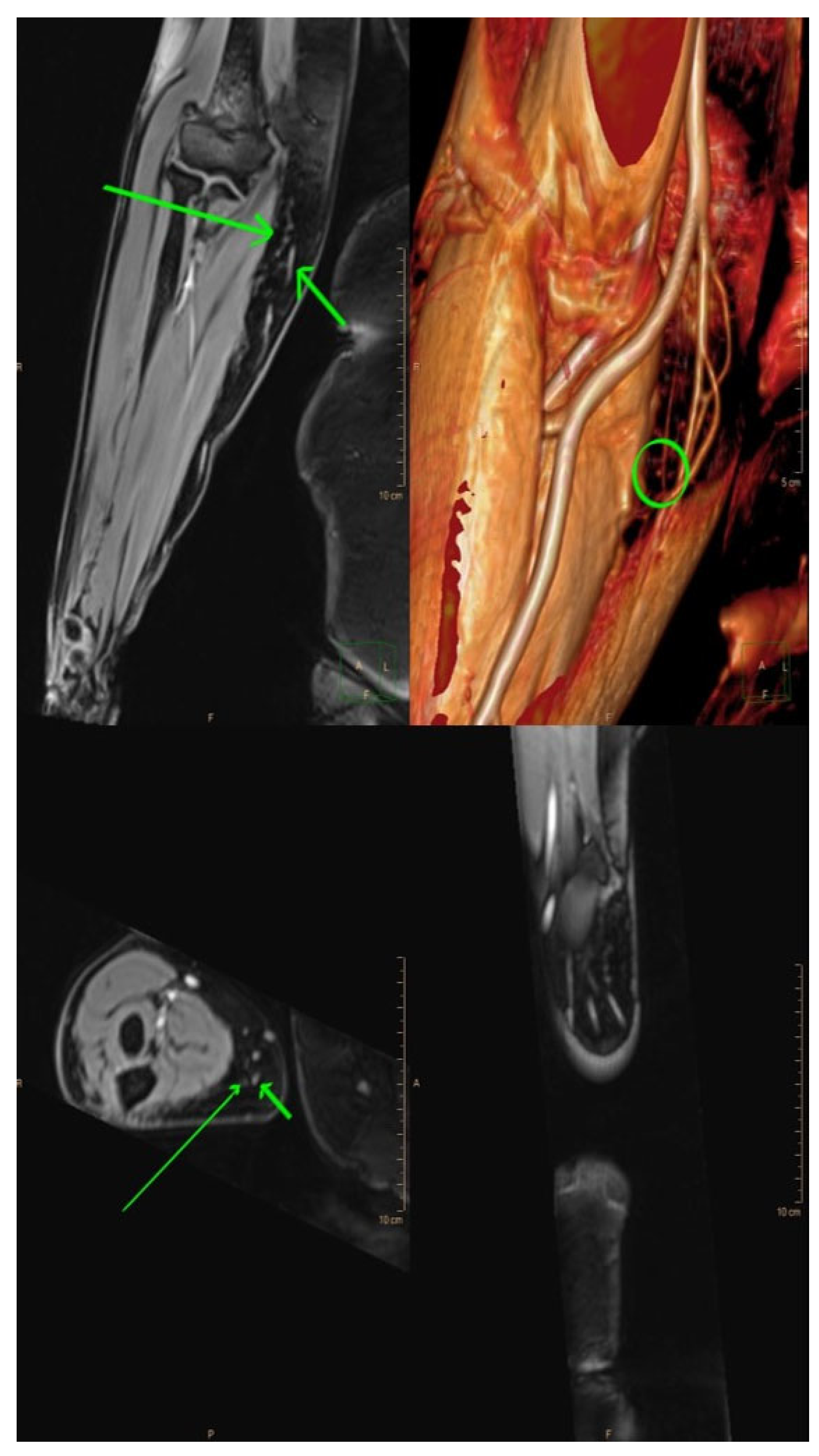
3.2. Magnetic Resonance Lymphangiography (MRL)
3.3. Single-Photon Emission Computed Tomography/Computed Tomography (SPECT/CT)
3.4. Ultra-High-Frequency Ultrasound (UHF-US)
3.5. Photoacoustic (PA) or Optoacoustic Imaging
4. Surgical Treatment
4.1. Debulking Procedures
4.1.1. Suction-Assisted Lipectomy (SAL)
4.1.2. Direct Excision
4.2. Physiologic Procedures
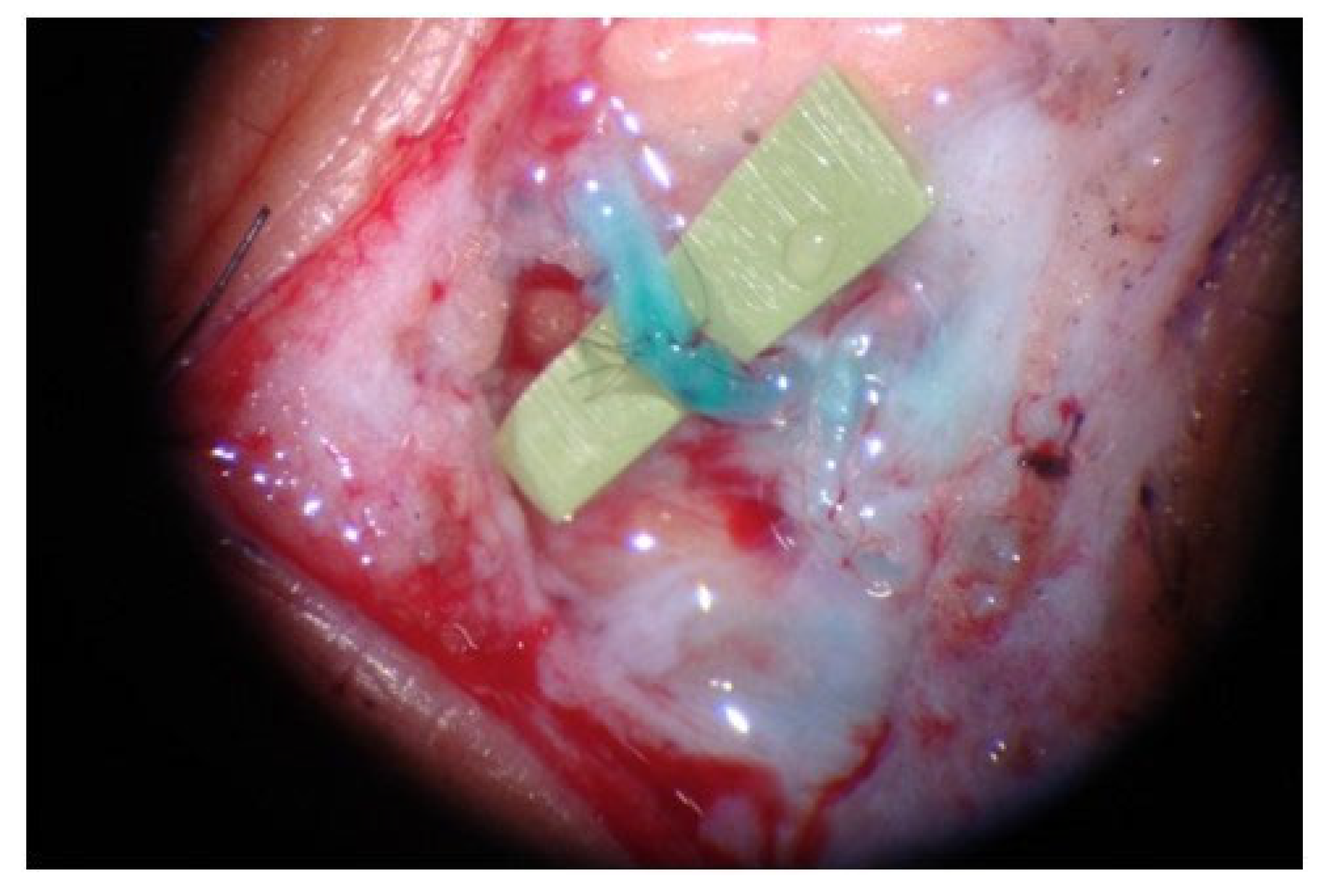
4.2.1. LVA
4.2.2. VLNT
Groin Lymph Node Flap
Lateral Thoracic Lymph Node Flap
Supraclavicular Lymph Node Flap
Submental Lymph Node Flap
Omental Lymph Node Flap
Jejunal Mesenteric Lymph Node Flaps
4.3. Preventive Lymphatic Surgery (LYMPHA Approach) [63]
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zeltzer, A.A.; Anzarut, A.; Hamdi, M. A Review of Lymphedema for the Hand and Upper-Extremity Surgeon. J. Hand Surg. 2018, 43, 1016–1025. [Google Scholar] [CrossRef] [PubMed]
- Zeltzer, A.A.; Brussaard, C.; Koning, M.; De Baerdemaeker, R.; Hendrickx, B.; Hamdi, M.; de Mey, J. MR lymphography in patients with upper limb lymphedema: The GPS for feasibility and surgical planning for lympho-venous bypass. J. Surg. Oncol. 2018, 118, 407–415. [Google Scholar] [CrossRef] [PubMed]
- Will, P.A.; Wan, Z.; Seide, S.E.; Berner, J.E.; Kneser, U.; Gazyakan, E.; Hirche, C. Supermicrosurgical treatment for lymphedema: A systematic review and network meta-analysis protocol. Syst. Rev. 2022, 11, 18. [Google Scholar] [CrossRef]
- Winters, H.; Tielemans, H.J.; Paulus, V.; Hummelink, S.; Slater, N.J.; Ulrich, D.J. A systematic review and meta-analysis of vascularized lymph node transfer for breast cancer-related lymphedema. J. Vasc. Surg. Venous Lymphat. Disord. 2021, 10, 786–795.e1. [Google Scholar] [CrossRef] [PubMed]
- Beederman, M.; Garza, R.M.; Agarwal, S.; Chang, D.W. Outcomes for Physiologic Microsurgical Treatment of Secondary Lymphedema Involving the Extremity. Ann. Surg. 2020, 276, e255–e263. [Google Scholar] [CrossRef] [PubMed]
- Verhey, E.M.B.; Kandi, L.A.B.; Lee, Y.S.; Morris, B.E.; Casey, W.J.; Rebecca, A.M.M.; Marks, L.A.M.; Howard, M.A.; Teven, C.M. Outcomes of Lymphovenous Anastomosis for Lower Extremity Lymphedema: A Systematic Review. Plast. Reconstr. Surg.-Glob. Open 2022, 10, e4529. [Google Scholar] [CrossRef] [PubMed]
- Knackstedt, R.; Chen, W.F. Current Concepts in Surgical Management of Lymphedema. Phys. Med. Rehabil. Clin. N. Am. 2022, 33, 885–899. [Google Scholar] [CrossRef]
- Beederman, M.; Chang, D.W. Advances in surgical treatment of lymphedema. Arch. Plast. Surg. 2021, 48, 670–677. [Google Scholar] [CrossRef]
- Pons, G.; Clavero, J.; Alomar, X.; Rodríguez-Bauza, E.; Tom, L.; Masia, J. Preoperative planning of lymphaticovenous anastomosis: The use of magnetic resonance lymphangiography as a complement to indocyanine green lymphography. J. Plast. Reconstr. Aesthetic Surg. 2019, 72, 884–891. [Google Scholar] [CrossRef]
- Chang, E.I.; Chu, C.K.; Chang, E.I. Advancements in imaging technology for microvascular free tissue transfer. J. Surg. Oncol. 2018, 118, 729–735. [Google Scholar] [CrossRef]
- Akita, S.; Unno, N.; Maegawa, J.; Kimata, Y.; Fukamizu, H.; Yabuki, Y.; Kitayama, S.; Shinaoka, A.; Yamada, K.; Sano, M.; et al. A phase III, multicenter, single-arm study to assess the utility of indocyanine green fluorescent lymphography in the treatment of secondary lymphedema. J. Vasc. Surg. Venous Lymphat. Disord. 2021, 10, 728–737.e3. [Google Scholar] [CrossRef] [PubMed]
- Guerrini, S.; Gentili, F.; Mazzei, F.G.; Gennaro, P.; Volterrani, L.; Mazzei, M.A. Magnetic resonance lymphangiography: With or without contrast? Diagn. Interv. Radiol. 2020, 26, 587–595. [Google Scholar] [CrossRef] [PubMed]
- Park, K.E.; Allam, O.; Chandler, L.; Mozzafari, M.A.; Ly, C.; Lu, X.; Persing, J.A. Surgical management of lymphedema: A review of current literature. Gland. Surg. 2020, 9, 503–511. [Google Scholar] [CrossRef] [PubMed]
- Dayan, J.H.; Wiser, I.M.; Verma, R.; Shen, J.; Talati, N.; Goldman, D.M.; Mehrara, B.J.; Smith, M.L.; Dayan, E.; Coriddi, M.; et al. Regional Patterns of Fluid and Fat Accumulation in Patients with Lower Extremity Lymphedema Using Magnetic Resonance Angiography. Plast. Reconstr. Surg. 2020, 145, 555–563. [Google Scholar] [CrossRef] [PubMed]
- Forte, A.J.; Boczar, D.; Huayllani, M.T.; Avila, F.R.; Guliyeva, G.; Lu, X.; Mash, W.R.; Kung, T.A. Use of magnetic resonance imaging lymphangiography for preoperative planning in lymphedema surgery: A systematic review. Microsurgery 2021, 41, 384–390. [Google Scholar] [CrossRef] [PubMed]
- Gentileschi, S.; Albanese, R.; Pino, V.; Stefanizzi, G.; Fragomeni, S.; Zagaria, L.; Ieria, F.P.; Salgarello, M.; Scambia, G.; Garganese, G. SPECT/CT and fusion ultrasound to target the efferent groin lymph node for lymphatic surgery. Microsurgery 2019, 39, 605–612. [Google Scholar] [CrossRef] [PubMed]
- Du, X.; Liu, C. Application of imaging in lymphedema surgical therapies. Gland. Surg. 2020, 9, 582–588. [Google Scholar] [CrossRef] [PubMed]
- Iimura, T.; Fukushima, Y.; Kumita, S.; Ogawa, R.; Hyakusoku, H. Estimating Lymphodynamic Conditions and Lymphovenous Anastomosis Efficacy Using 99mTc-phytate Lymphoscintigraphy with SPECT-CT in Patients with Lower-limb Lymphedema. Plast. Reconstr. Surg.-Glob. Open 2015, 3, e404. [Google Scholar] [CrossRef]
- Weiss, M.; Baumeister, R.G.; Frick, A.; Wallmichrath, J.; Bartenstein, P.; Rominger, A. Primary Lymphedema of the Lower Limb: The Clinical Utility of Single Photon Emission Computed Tomography/CT. Korean J. Radiol. 2015, 16, 188–195. [Google Scholar] [CrossRef]
- Hayashi, A.; Giacalone, G.; Yamamoto, T.; Belva, F.; Visconti, G.; Hayashi, N.; Handa, M.; Yoshimatsu, H.; Salgarello, M. Ultra High-frequency Ultrasonographic Imaging with 70 MHz Scanner for Visualization of the Lymphatic Vessels. Plast. Reconstr. Surg.-Glob. Open 2019, 7, e2086. [Google Scholar] [CrossRef]
- Van Heumen, S.; Riksen, J.J.M.; Bramer, W.M.; van Soest, G.; Vasilic, D. Imaging of the Lymphatic Vessels for Surgical Planning: A Systematic Review. Ann. Surg. Oncol. 2022, 30, 462–479. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, A.; Visconti, G.; Hayashi, A.; Santoro, A.; Longo, V.; Salgarello, M. Ultra-High frequency ultrasound imaging of lymphatic channels correlates with their histological features: A step forward in lymphatic surgery. J. Plast. Reconstr. Aesthetic Surg. 2020, 73, 1622–1629. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, Y.; Kajita, H.; Watanabe, S.; Okabe, K.; Sakuma, H.; Imanishi, N.; Aiso, S.; Kishi, K. Application of Photoacoustic Imaging for Lymphedema Treatment. J. Reconstr. Microsurg. 2021, 38, 254–262. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, Y.; Kajita, H.; Watanabe, S.; Otaki, M.; Okabe, K.; Sakuma, H.; Takatsume, Y.; Imanishi, N.; Aiso, S.; Kishi, K. Surgical Applications of Lymphatic Vessel Visualization Using Photoacoustic Imaging and Augmented Reality. J. Clin. Med. 2021, 11, 194. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, K.; Marulanda, K.; Gray, S. Surgical Intervention for Lymphedema. Surg. Oncol. Clin. N. Am. 2018, 27, 195–215. [Google Scholar] [CrossRef] [PubMed]
- Schaverien, M.V.; Coroneos, C.J. Surgical Treatment of Lymphedema. Plast. Reconstr. Surg. 2019, 144, 738–758. [Google Scholar] [CrossRef] [PubMed]
- Greene, A.K.M.; Maclellan, R.A.M. Operative Treatment of Lymphedema Using Suction-Assisted Lipectomy. Ann. Plast. Surg. 2016, 77, 337–340. [Google Scholar] [CrossRef] [PubMed]
- Greene, A.K.M.; Maclellan, R.M. Management of Lymphedema with Suction-Assisted Lipectomy. Plast. Reconstr. Surg. 2014, 134, 36. [Google Scholar] [CrossRef]
- Van der Walt, J.C.; Perks, T.J.; Zeeman, B.J.; Bruce-Chwatt, A.J.; Graewe, F.R. Modified Charles Procedure Using Negative Pressure Dressings for Primary Lymphedema: A functional assessment. Ann. Plast. Surg. 2009, 62, 669–675. [Google Scholar] [CrossRef]
- Carl, H.M.; Walia, G.; Bello, R.; Clarke-Pearson, E.; Hassanein, A.H.; Cho, B.; Pedreira, R.; Sacks, J.M. Systematic Review of the Surgical Treatment of Extremity Lymphedema. J. Reconstr. Microsurg. 2017, 33, 412–425. [Google Scholar] [CrossRef]
- Gupta, R.B.; Mathijs, E.; Hart, J.D.; Bates, J.D.; Powers, J.; Chaiyasate, K. May-Thurner Syndrome and Lymphedema Reconstruction. Plast. Reconstr. Surg.-Glob. Open 2022, 10, e4377. [Google Scholar] [CrossRef] [PubMed]
- Chang, D.W.; Masia, J.; Garza, R.; Skoracki, R.; Neligan, P.C. Lymphedema: Surgical and Medical Therapy. Plast. Reconstr. Surg. 2016, 138 (Suppl. 3), 209s–218s. [Google Scholar] [CrossRef] [PubMed]
- Hanson, S.E.; Chang, E.I.; Schaverien, M.V.M.; Chu, C.; Selber, J.C.; Hanasono, M.M. Controversies in Surgical Management of Lymphedema. Plast. Reconstr. Surg.-Glob. Open 2020, 8, e2671. [Google Scholar] [CrossRef]
- Scaglioni, M.F.; Fontein, D.B.Y.; Arvanitakis, M.; Giovanoli, P. Systematic review of lymphovenous anastomosis (LVA) for the treatment of lymphedema. Microsurgery 2017, 37, 947–953. [Google Scholar] [CrossRef] [PubMed]
- De Sire, A.; Losco, L.; Lippi, L.; Spadoni, D.; Kaciulyte, J.; Sert, G.; Ciamarra, P.; Marcasciano, M.; Cuomo, R.; Bolletta, A.; et al. Surgical Treatment and Rehabilitation Strategies for Upper and Lower Extremity Lymphedema: A Comprehensive Review. Medicina 2022, 58, 954. [Google Scholar] [CrossRef] [PubMed]
- De Carvalho, F.M.; Almeida, A.; Silva, Á.; Marques, M. Treatment of Lymphorrhea Associated with an Amputation Stump with Lymphaticovenular Anastomosis. Acta Médica Port. 2022, 35, 384–387. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.C.-S.; Yen, Y.-H.; Wu, S.-C.; Lin, W.-C.; Chiang, M.-H.; Hsieh, C.-H. Supermicrosurgical Lymphaticovenous Anastomosis as an Alternative Treatment Option for Patients with Lymphorrhea. Plast. Reconstr. Surg. 2019, 144, 1214–1224. [Google Scholar] [CrossRef] [PubMed]
- Cheng, M.-H.M.; Huang, J.-J.; Wu, C.-W.; Yang, C.-Y.M.; Lin, C.-Y.M.; Henry, S.L.; Kolios, L. The Mechanism of Vascularized Lymph Node Transfer for Lymphedema: Natural lym-phaticovenous drainage. Plast. Reconstr. Surg. 2014, 133, 192e–198e. [Google Scholar] [CrossRef]
- De Brucker, B.; Zeltzer, A.; Seidenstuecker, K.; Hendrickx, B.; Adriaenssens, N.; Hamdi, M. Breast Cancer–Related Lymphedema: Quality of Life after Lymph Node Transfer. Plast. Reconstr. Surg. 2016, 137, 1673–1680. [Google Scholar] [CrossRef]
- Scaglioni, M.F.; Arvanitakis, M.; Chen, Y.-C.; Giovanoli, P.; Yang, J.C.-S.; Chang, E.I. Comprehensive review of vascularized lymph node transfers for lymphedema: Outcomes and complications. Microsurgery 2016, 38, 222–229. [Google Scholar] [CrossRef]
- Zeltzer, A.A.; Anzarut, A.; Braeckmans, D.; Seidenstuecker, K.; Hendrickx, B.; Van Hedent, E.; Hamdi, M. The vascularized groin lymph node flap (VGLN): Anatomical study and flap planning using multi-detector CT scanner. The golden triangle for flap harvesting. J. Surg. Oncol. 2017, 116, 378–383. [Google Scholar] [CrossRef] [PubMed]
- Vignes, S.; Blanchard, M.; Yannoutsos, A.; Arrault, M. Complications of Autologous Lymph-node Transplantation for Limb Lymphoedema. Eur. J. Vasc. Endovasc. Surg. 2013, 45, 516–520. [Google Scholar] [CrossRef] [PubMed]
- Sulo, E.; Hartiala, P.; Viitanen, T.; Mäki, M.; Seppänen, M.; Saarikko, A. Risk of donor-site lymphatic vessel dysfunction after microvascular lymph node transfer. J. Plast. Reconstr. Aesthetic Surg. 2014, 68, 551–558. [Google Scholar] [CrossRef] [PubMed]
- Viitanen, T.P.; Mäki, M.T.; Seppänen, M.P.; Suominen, E.A.; Saaristo, A.M. Donor-Site Lymphatic Function after Microvascular Lymph Node Transfer. Plast. Reconstr. Surg. 2012, 130, 1246–1253. [Google Scholar] [CrossRef] [PubMed]
- Dayan, J.H.; Dayan, E.; Smith, M.L. Reverse Lymphatic Mapping: A new technique for maximizing safety in vascularized lymph node transfer. Plast. Reconstr. Surg. 2015, 135, 277–285. [Google Scholar] [CrossRef] [PubMed]
- Becker, C.; Assouad, J.; Riquet, M.; Hidden, G. Postmastectomy Lymphedema: Long-term results following microsurgical lymph node transplantation. Ann. Surg. 2006, 243, 313–315. [Google Scholar] [CrossRef] [PubMed]
- Masià, J.; Smith, M.L.; Chang, E.I. Combining Autologous Breast Reconstruction and Vascularized Lymph Node Transfer. Semin. Plast. Surg. 2018, 32, 036–041. [Google Scholar] [CrossRef] [PubMed]
- Chang, E.I. Optimizing Treatment of Breast Cancer Related Lymphedema Using Combined DIEP Flap and Lymphedema Surgery. Arch. Plast. Surg. 2022, 49, 150–157. [Google Scholar] [CrossRef]
- Schaverien, M.V.; Badash, I.; Selber, J.C.; Cheng, M.-H.; Patel, K.M. Vascularized Lymph Node Transfer for Lymphedema. Semin. Plast. Surg. 2018, 32, 28–35. [Google Scholar] [CrossRef]
- Baptista, R.R.; Kasai, K.E.; dos Anjos, D.M.; Busnardo, F.D.F.; Modolin, M.; Ferreira, M.C.; Barreiro, G.C. Lymph Fasciocutaneous Lateral Thoracic Artery Flap: Anatomical Study and Clinical Use. J. Reconstr. Microsurg. 2014, 30, 389–396. [Google Scholar] [CrossRef]
- Tinhofer, I.E.; Meng, S.; Steinbacher, J.; Roka-Palkovits, J.; Györi, E.; Reissig, L.F.; Cheng, M.-H.; Weninger, W.J.; Tzou, C.H. The surgical anatomy of the vascularized lateral thoracic artery lymph node flap-A cadaver study. J. Surg. Oncol. 2017, 116, 1062–1068. [Google Scholar] [CrossRef] [PubMed]
- Coroneos, C.J.; Asaad, M.; Wong, F.C.; Hall, M.S.; Chen, D.N.; Hanasono, M.M.; Schaverien, M.V. Outcomes and technical modifications of vascularized lymph node transplantation from the lateral thoracic region for treatment of lymphedema. J. Surg. Oncol. 2022, 125, 603–614. [Google Scholar] [CrossRef] [PubMed]
- Visconti, G.; Bianchi, A.; Salgarello, M.; Di Leone, A.; Hayashi, A.; Masetti, R.; Franceschini, G. Lymphatic Tissue Transfer: Ultrasound-Guided Description and Preoperative Planning of Vascularised Lymph Nodes, Lymphatic Units, and Lymphatic Vessels Transfers. J. Pers. Med. 2022, 12, 1346. [Google Scholar] [CrossRef] [PubMed]
- Mardonado, A.A.; Chen, R.; Chang, D.W. The use of supraclavicular free flap with vascularized lymph node transfer for treatment of lymphedema: A prospective study of 100 consecutive cases. J. Surg. Oncol. 2016, 115, 68–71. [Google Scholar] [CrossRef]
- Mazerolle, P.; Meresse, T.; Gangloff, D.; Kolsi, K.; Dupret-Bories, A. Vascularized lymph node transfer with submental free flap. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2019, 137, 73–77. [Google Scholar] [CrossRef]
- Paulus, V.A.A.; Winters, H.; Hummelink, S.; Schulten, S.; Ulrich, D.J.O.; Vasilic, D. Submental flap for vascularized lymph node transfer; a CTA-based study on lymph node distribution. J. Surg. Oncol. 2020, 122, 1226–1231. [Google Scholar] [CrossRef] [PubMed]
- Tzou, C.H.; Meng, S.; Ines, T.; Reissig, L.; Pichler, U.; Steinbacher, J.; Pona, I.; Roka-Palkovits, J.; Rath, T.; Weninger, W.J.; et al. Surgical anatomy of the vascularized submental lymph node flap: Anatomic study of correlation of submental artery perforators and quantity of submental lymph node. J. Surg. Oncol. 2016, 115, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Gustafsson, J.; Chu, S.-Y.; Chan, W.-H.; Cheng, M.-H. Correlation between Quantity of Transferred Lymph Nodes and Outcome in Vascularized Submental Lymph Node Flap Transfer for Lower Limb Lymphedema. Plast. Reconstr. Surg. 2018, 142, 1056–1063. [Google Scholar] [CrossRef]
- Danforth, R.; Skoracki, R. Intra-abdominal donors for vascularized lymph node transfer: An update and review. Plast. Aesthetic Res. 2021, 8, 48. [Google Scholar] [CrossRef]
- Kenworthy, E.O.; Nelson, J.A.; Verma, R.; Mbabuike, J.; Mehrara, B.J.; Dayan, J.H. Double vascularized omentum lymphatic transplant (VOLT) for the treatment of lymphedema. J. Surg. Oncol. 2018, 117, 1413–1419. [Google Scholar] [CrossRef]
- Nguyen, A.T.; Suami, H.; Hanasono, M.M.; Womack, V.A.; Wong, F.C.; Chang, E.I. Long-term outcomes of the minimally invasive free vascularized omental lymphatic flap for the treatment of lymphedema. J. Surg. Oncol. 2016, 115, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Kraft, C.T.; Eiferman, D.; Jordan, S.; Skoracki, R.J. Complications after vascularized jejunal mesenteric lymph node transfer: A 3-year experience. Microsurgery 2019, 39, 497–501. [Google Scholar] [CrossRef] [PubMed]
- Boccardo, F.; Casabona, F.; De Cian, F.; Friedman, D.; Villa, G.; Bogliolo, S.; Ferrero, S.; Murelli, F.; Campisi, C. Lymphedema Microsurgical Preventive Healing Approach: A New Technique for Primary Prevention of Arm Lymphedema after Mastectomy. Ann. Surg. Oncol. 2009, 16, 703–708. [Google Scholar] [CrossRef] [PubMed]
- Ciudad, P.; Escandón, J.M.; Bustos, V.P.; Manrique, O.J.; Kaciulyte, J. Primary Prevention of Cancer-Related Lymphedema Using Preventive Lymphatic Surgery: Systematic Review and Meta-analysis. Indian J. Plast. Surg. 2022, 55, 018–025. [Google Scholar] [CrossRef]
- Viviano, S.L.; Neligan, P.C. Updates on Excisional Procedures for Lymphedema. Adv. Wound Care 2022, 11, 419–427. [Google Scholar] [CrossRef]
- Chang, D.W.; Dayan, J.; Greene, A.K.; MacDonald, J.K.; Masia, J.; Mehrara, B.; Neligan, P.C.; Nguyen, D. Surgical Treatment of Lymphedema: A Systematic Review and Meta-Analysis of Controlled Trials. Results of a Consensus Conference. Plast. Reconstr. Surg. 2021, 147, 975–993. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Imaging Modalities | Advantages | Limitations |
|---|---|---|
| LSG |
|
|
| ICG-L |
|
|
| MRL |
|
|
| SPECT/CT |
|
|
| UHF-US |
|
|
| PA imaging |
|
|
| VLNT | Advantages | Limitations |
|---|---|---|
| Groin flap |
|
|
| Lateral thoracic flap |
|
|
| Supraclavicular flap |
|
|
| Submental flap |
|
|
| Omental flap |
|
|
| Jejunal flap |
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almeida, A.; Ofir, H.; Zeltzer, A.A. The Lymphatic System—A Surgeon’s Point of View. Lymphatics 2023, 1, 220-236. https://doi.org/10.3390/lymphatics1020013
Almeida A, Ofir H, Zeltzer AA. The Lymphatic System—A Surgeon’s Point of View. Lymphatics. 2023; 1(2):220-236. https://doi.org/10.3390/lymphatics1020013
Chicago/Turabian StyleAlmeida, Alexandre, Hagit Ofir, and Assaf A. Zeltzer. 2023. "The Lymphatic System—A Surgeon’s Point of View" Lymphatics 1, no. 2: 220-236. https://doi.org/10.3390/lymphatics1020013
APA StyleAlmeida, A., Ofir, H., & Zeltzer, A. A. (2023). The Lymphatic System—A Surgeon’s Point of View. Lymphatics, 1(2), 220-236. https://doi.org/10.3390/lymphatics1020013