



Cancers 2024, 16(10), 1807; https://doi.org/10.3390/cancers16101807 - 9 May 2024
Cited by 1 | Viewed by 1150
Abstract
►
Show Figures
Non-Hispanic Black breast cancer survivors have poorer outcomes and higher mortality rates than White survivors, but systemic biological mechanisms underlying these disparities are unclear. We used circulating leukocytes as a surrogate for measuring systemic mechanisms, which might be different from processes in the
[...] Read more.
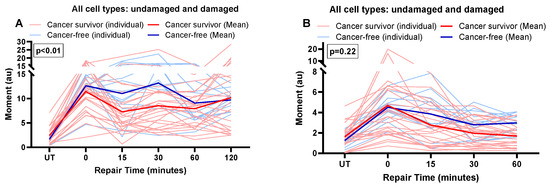
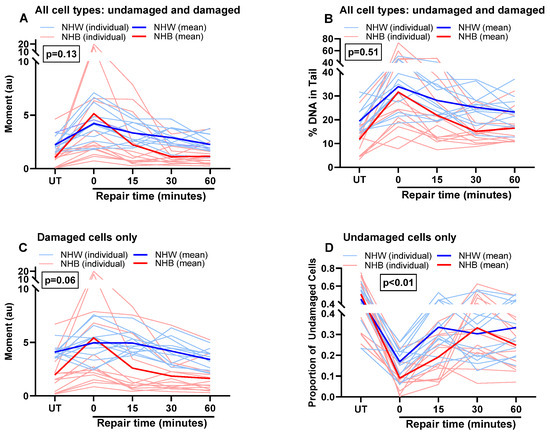
Non-Hispanic Black breast cancer survivors have poorer outcomes and higher mortality rates than White survivors, but systemic biological mechanisms underlying these disparities are unclear. We used circulating leukocytes as a surrogate for measuring systemic mechanisms, which might be different from processes in the target tissue (e.g., breast). We investigated race-based differences in DNA damage and repair, using a novel CometChip assay, in circulating leukocytes from breast cancer survivors who had completed primary cancer therapy and were cancer free. We observed novel race-based differences in systemic DNA damage and repair activity in cancer survivors, but not in cells from healthy volunteers. Basal DNA damage in leukocytes was higher in White survivors, but Black survivors showed a much higher induction after bleomycin treatment. Double-strand break repair activity was also significantly different between the races, with cells from White survivors showing more sustained repair activity compared to Black leukocytes. These results suggest that cancer and cancer therapy might have long-lasting effects on systemic DNA damage and repair mechanisms that differ in White survivors and Black survivors. Findings from our preliminary study in non-cancer cells (circulating leukocytes) suggest systemic effects beyond the target site, with implications for accelerated aging-related cancer survivorship disparities.
Full article

Figure 1


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}