

Disparities in Survival Outcomes among Racial/Ethnic Minorities with Head and Neck Squamous Cell Cancer in the United States


 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
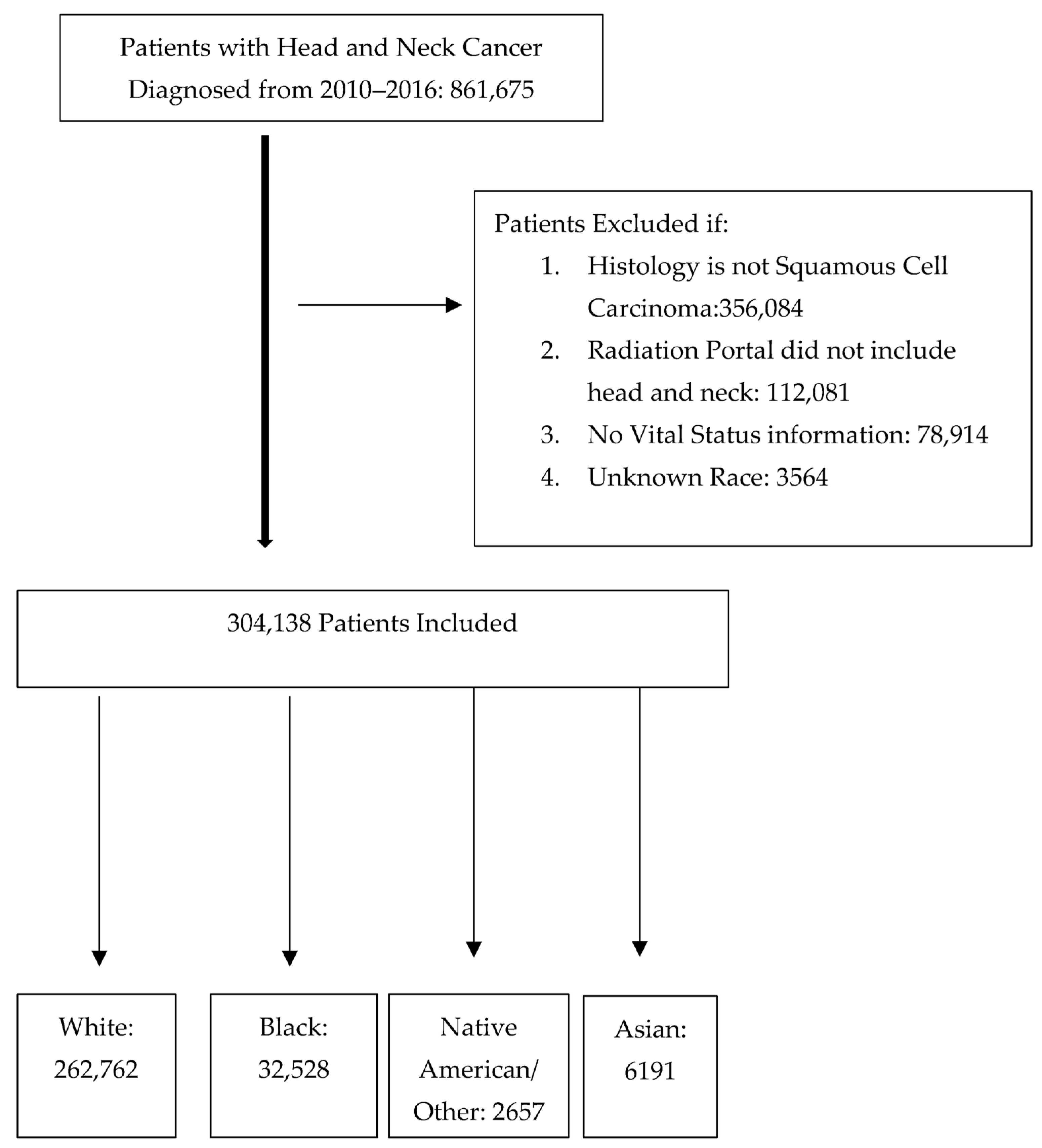
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Demographic and Clinical Comparisons
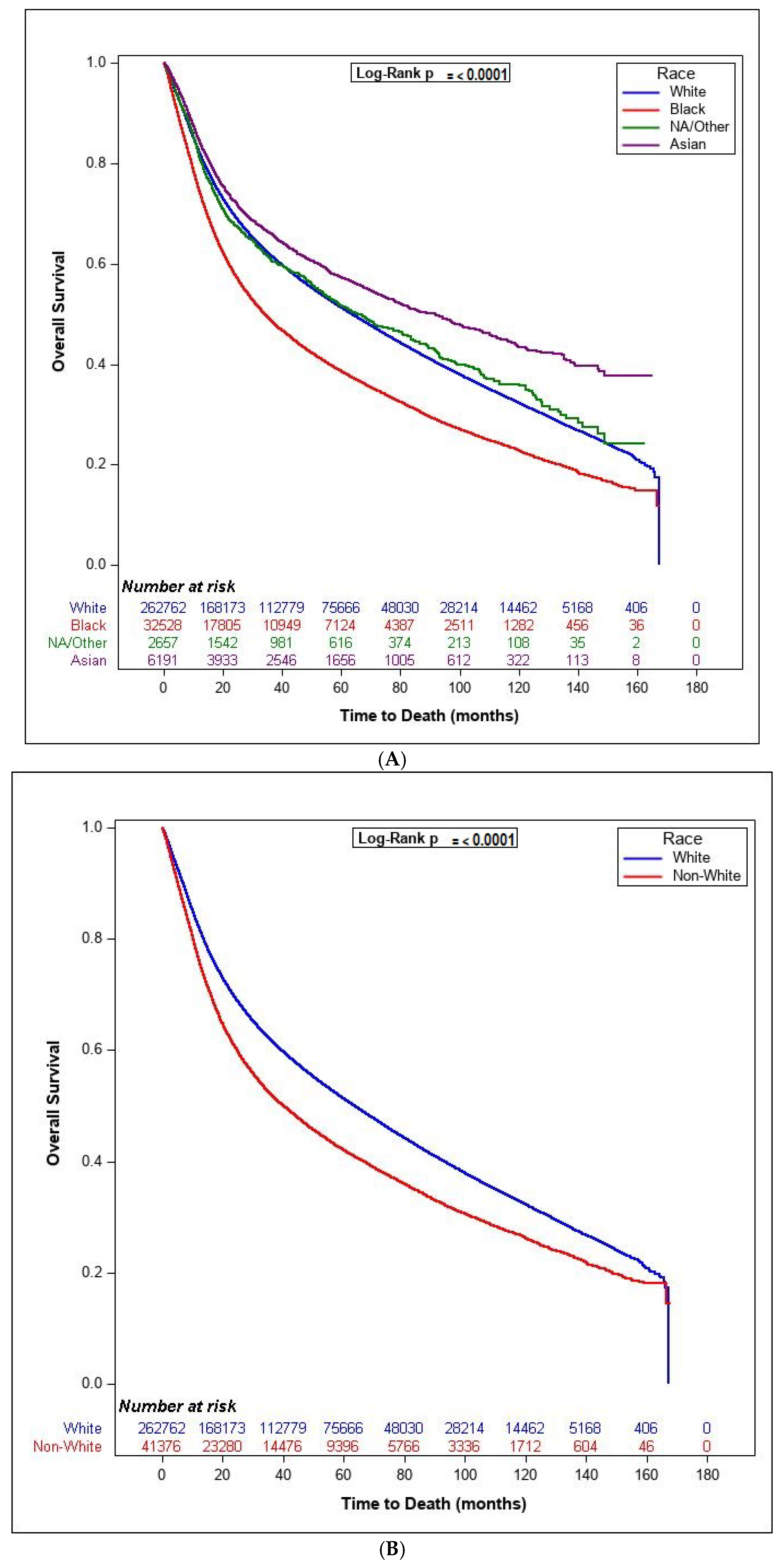
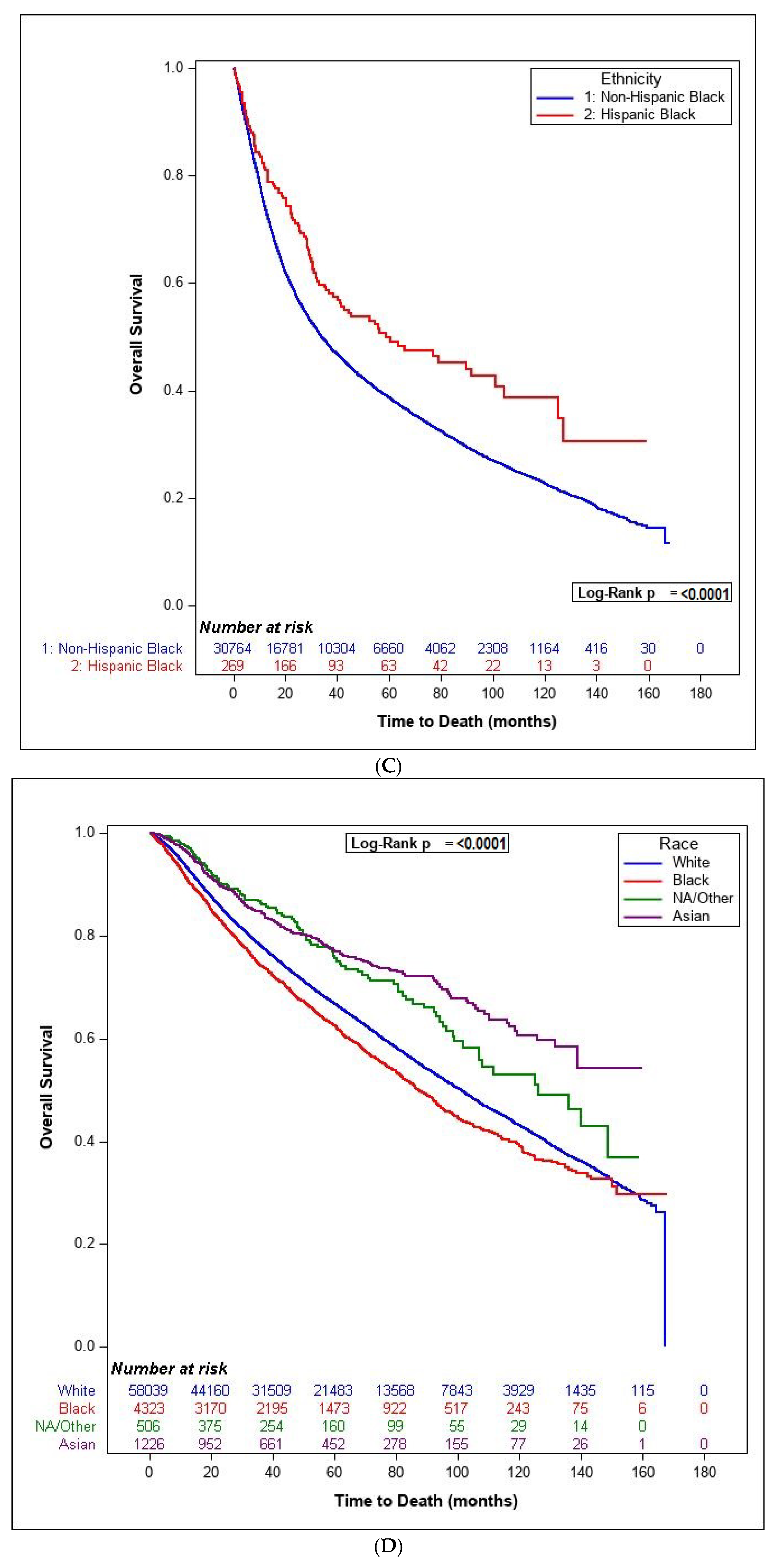
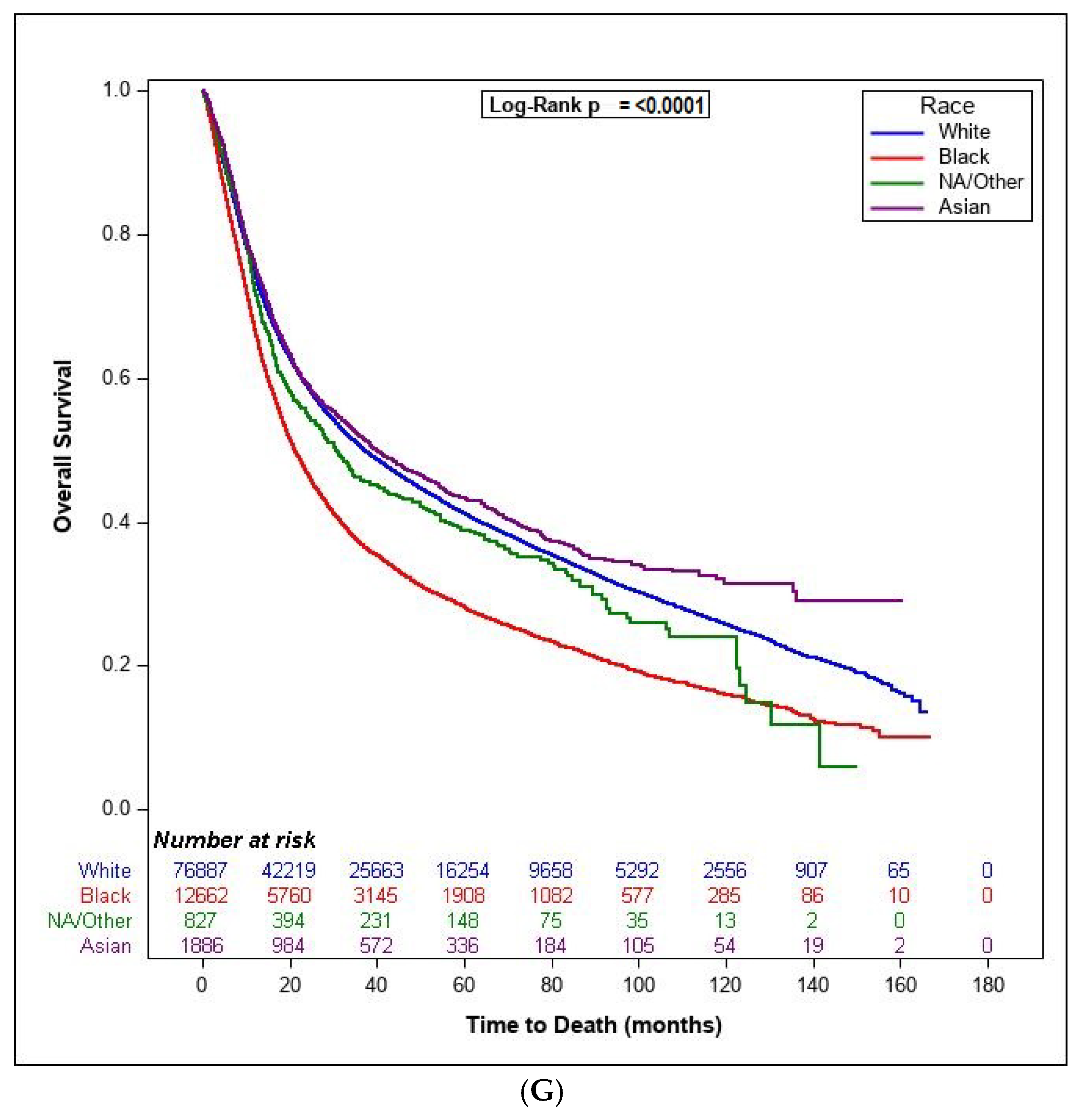
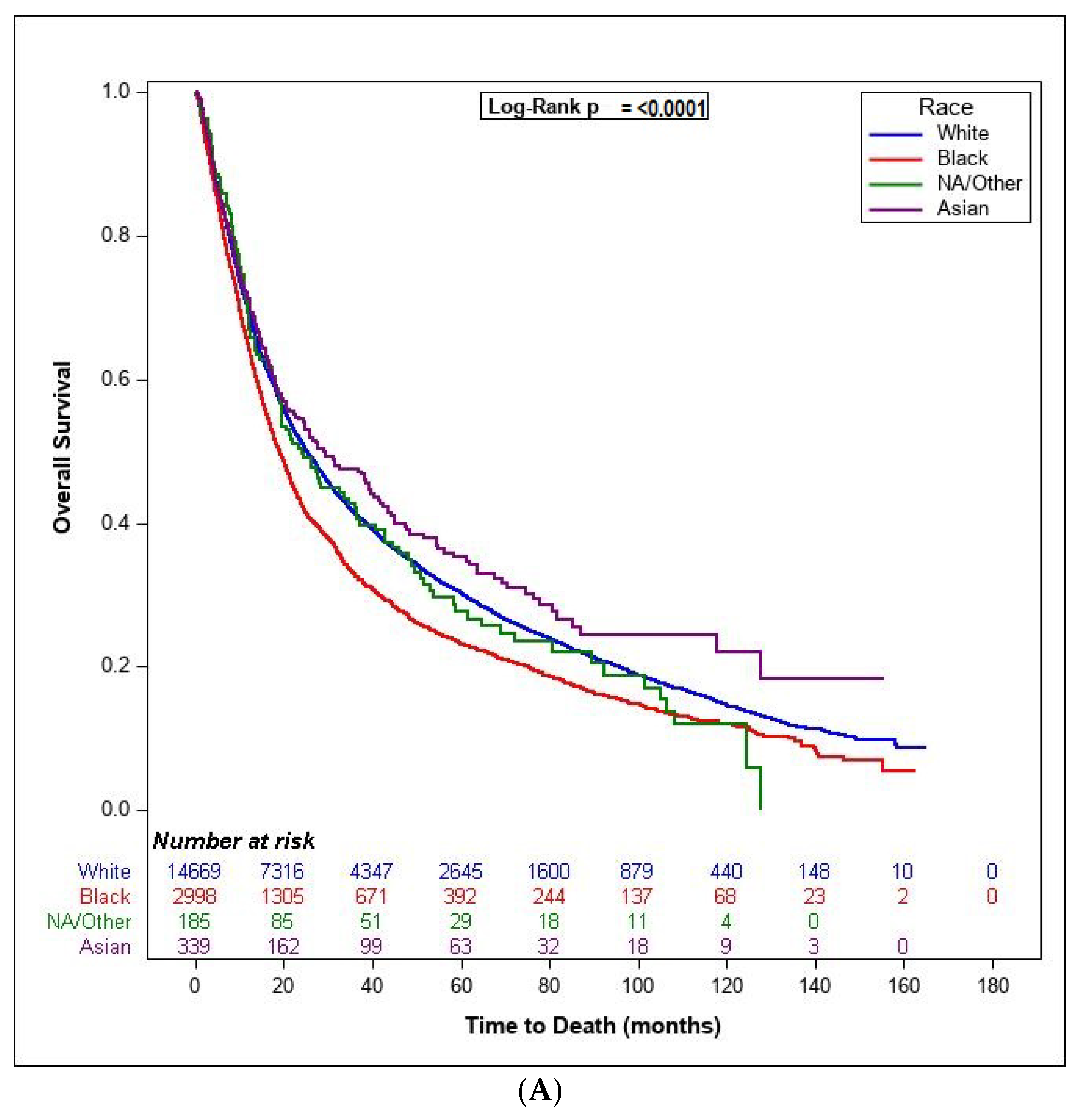
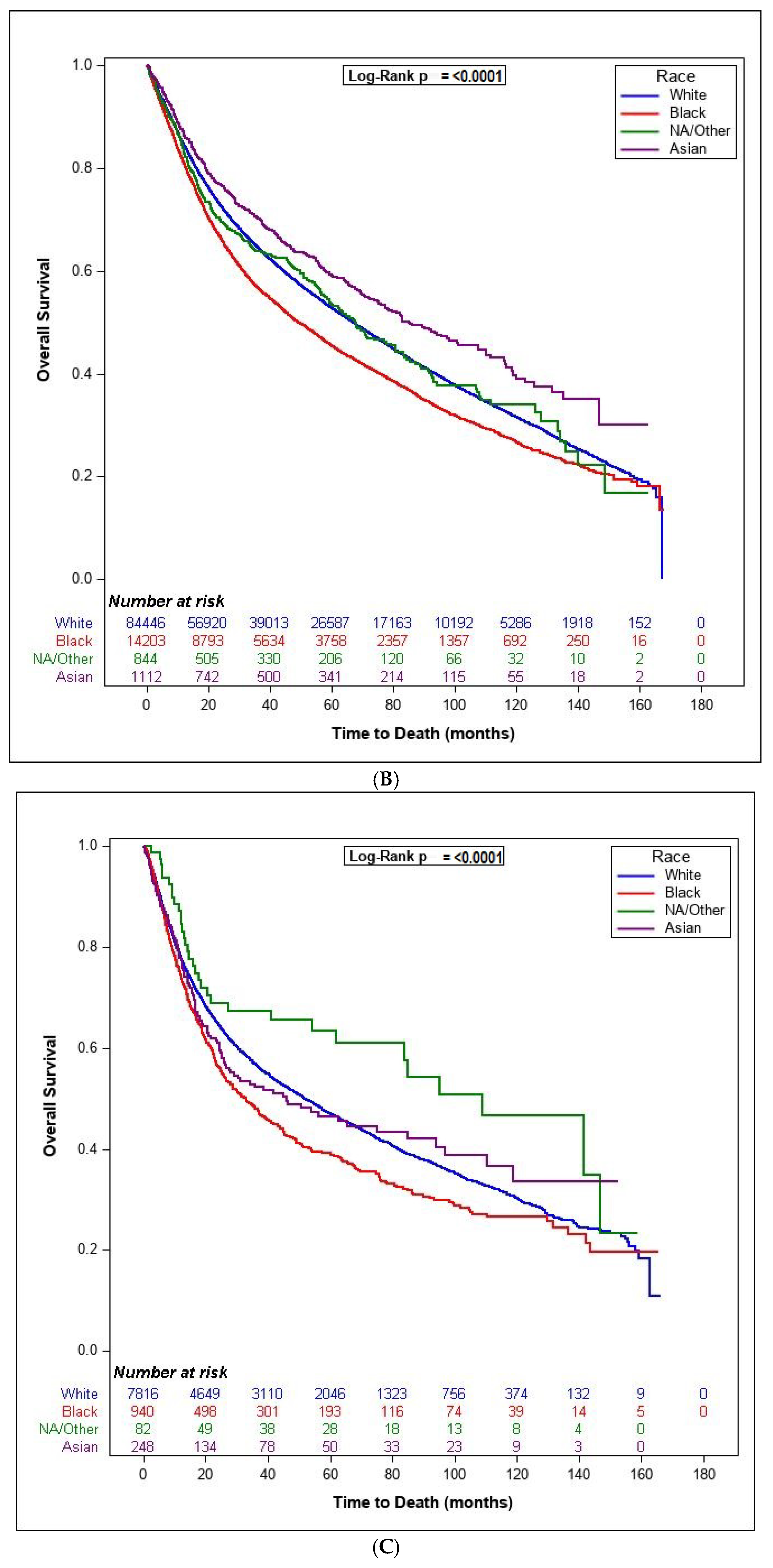
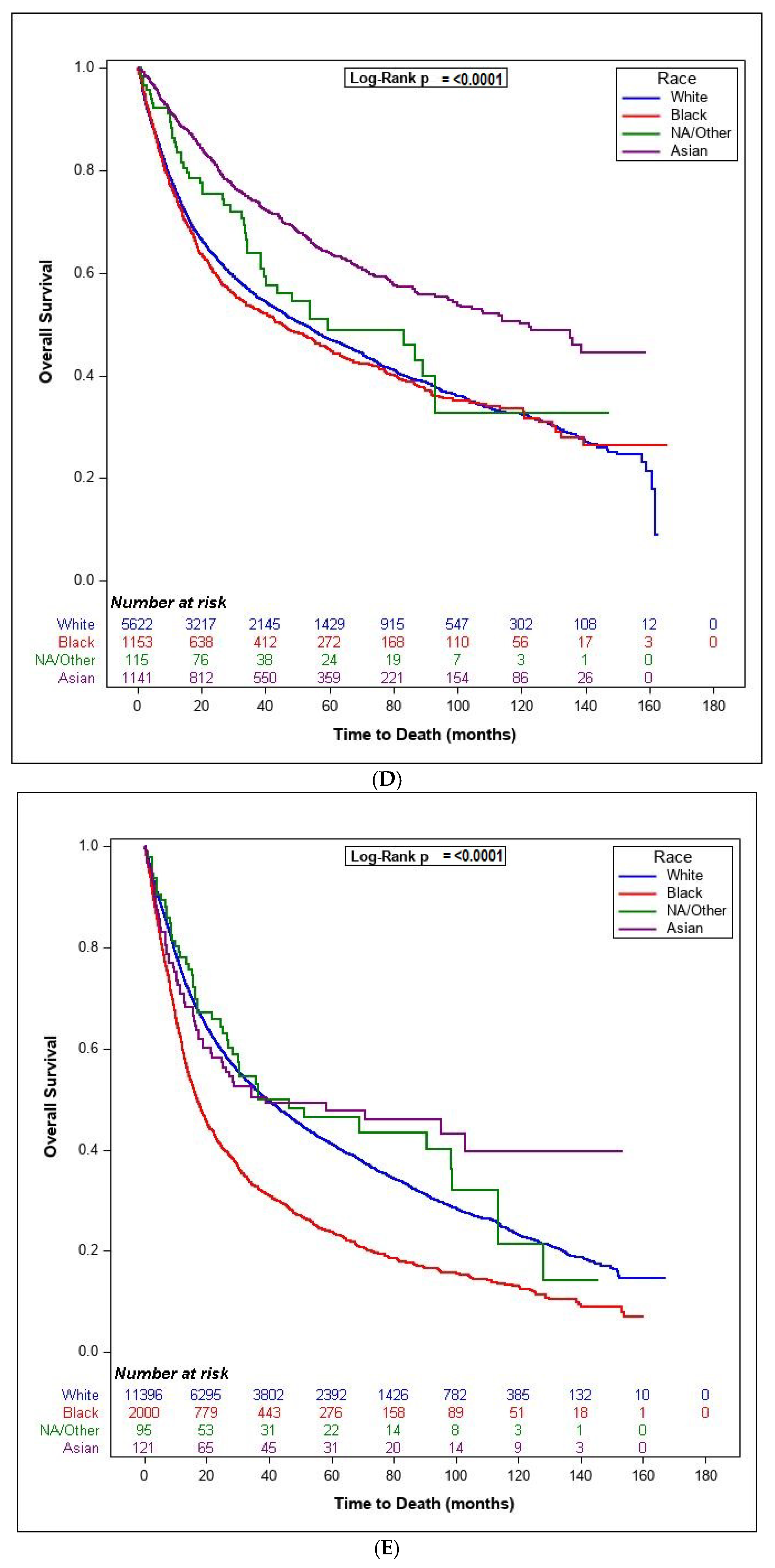
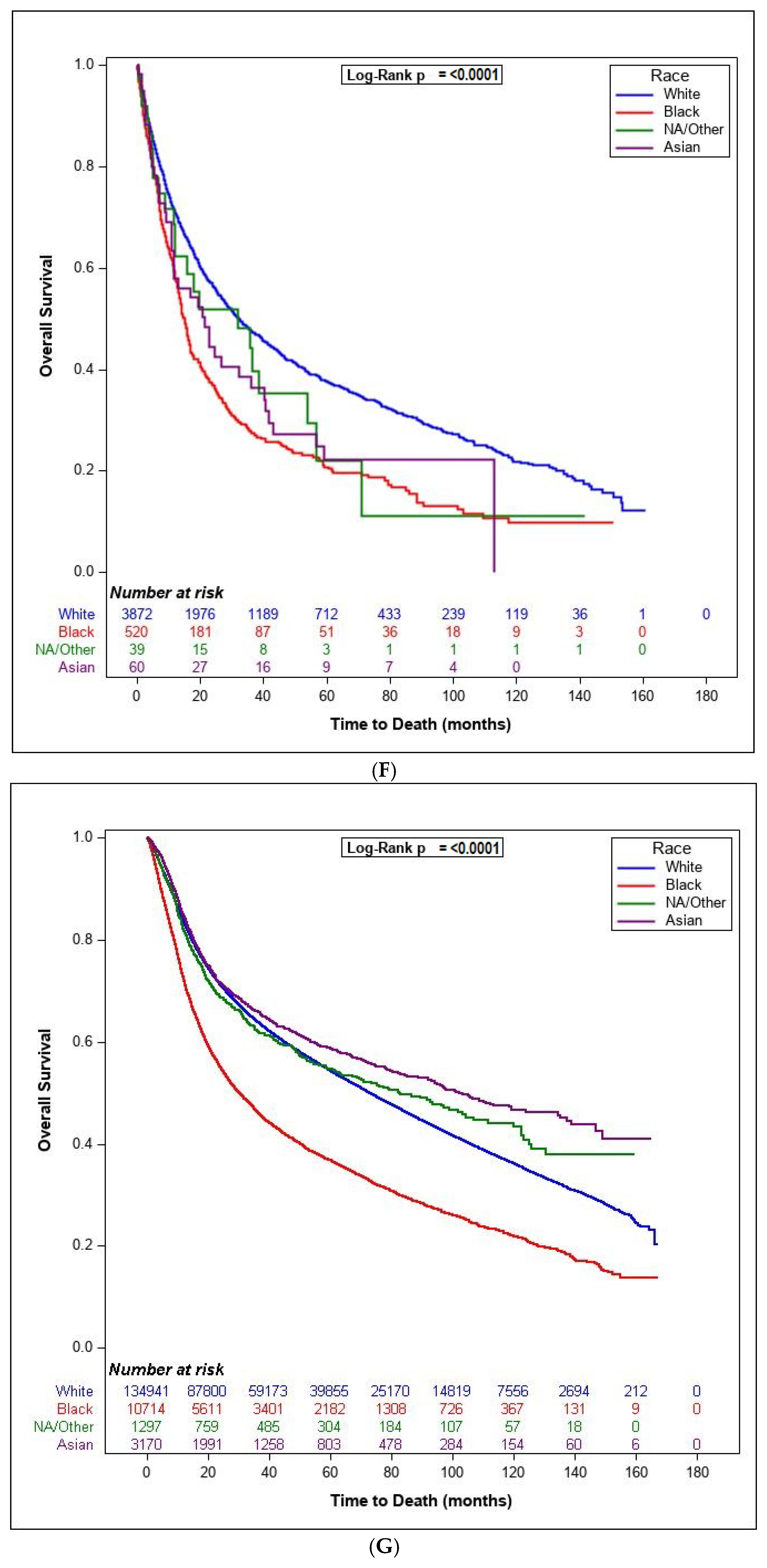
3.2. Survival Analysis
3.3. Analysis of Treatment Time
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Islami, F.; Ward, E.M.; Sung, H.; Cronin, K.A.; Tangka, F.K.L.; Sherman, R.L.; Zhao, J.; Anderson, R.N.; Henley, S.J.; Yabroff, K.R.; et al. Annual Report to the Nation on the Status of Cancer, Part 1: National Cancer Statistics. J. Natl. Cancer Inst. 2021, 113, 1648–1669. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Massa, S.T.; Cass, L.M.; Christopher, K.M.; Walker, R.J.; Varvares, M.A.; Osazuwa-Peters, N. Decreased cancer-independent life expectancy in the head and neck cancer population. Head Neck 2017, 39, 1845–1853. [Google Scholar] [CrossRef] [PubMed]
- Osazuwa-Peters, N.; Simpson, M.C.; Zhao, L.; Boakye, E.A.; Olomukoro, S.I.; Deshields, T.; Loux, T.M.; Varvares, M.A.; Schootman, M. Suicide risk among cancer survivors: Head and neck versus other cancers. Cancer 2018, 124, 4072–4079. [Google Scholar] [CrossRef] [Green Version]
- Ang, K.K.; Harris, J.; Wheeler, R.; Weber, R.; Rosenthal, D.I.; Nguyen-Tân, P.F.; Westra, W.H.; Chung, C.H.; Jordan, R.C.; Lu, C.; et al. Human Papillomavirus and Survival of Patients with Oropharyngeal Cancer. N. Engl. J. Med. 2010, 363, 24–35. [Google Scholar] [CrossRef] [Green Version]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef]
- Zakeri, K.; MacEwan, I.; Vazirnia, A.; Cohen, E.E.; Spiotto, M.T.; Haraf, D.J.; Vokes, E.E.; Weichselbaum, R.R.; Mell, L.K. Race and competing mortality in advanced head and neck cancer. Oral Oncol. 2014, 50, 40–44. [Google Scholar] [CrossRef] [Green Version]
- Rose, B.S.; Jeong, J.-H.; Nath, S.K.; Lu, S.M.; Mell, L.K. Population-Based Study of Competing Mortality in Head and Neck Cancer. J. Clin. Oncol. 2011, 29, 3503–3509. [Google Scholar] [CrossRef]
- Molina, M.A.; Cheung, M.C.; Perez, E.A.; Byrne, M.M.; Franceschi, D.; Moffat, F.L.; Koniaris, L.G. African american and poor patients have a dramatically worse prognosis for head and neck cancer: An examination of 20,915 patients. Cancer 2008, 113, 2797–2806. [Google Scholar] [CrossRef]
- Settle, K.; Posner, M.R.; Schumaker, L.M.; Tan, M.; Suntharalingam, M.; Goloubeva, O.; Strome, S.E.; Haddad, R.I.; Patel, S.S.; Cambell, E.V.; et al. Racial Survival Disparity in Head and Neck Cancer Results from Low Prevalence of Human Papillomavirus Infection in Black Oropharyngeal Cancer Patients. Cancer Prev. Res. 2009, 2, 776–781. [Google Scholar] [CrossRef] [Green Version]
- Choi, S.H.; Terrell, J.E.; Fowler, K.; McLean, S.A.; Ghanem, T.; Wolf, G.T.; Bradford, C.R.; Taylor, J.; Duffy, S.A. Socioeconomic and Other Demographic Disparities Predicting Survival among Head and Neck Cancer Patients. PLoS ONE 2016, 11, e0149886. [Google Scholar] [CrossRef]
- Gourin, C.G.; Podolsky, R.H. Racial Disparities in Patients with Head and Neck Squamous Cell Carcinoma. Laryngoscope 2006, 116, 1093–1106. [Google Scholar] [CrossRef]
- Al-Qurayshi, Z.; Srivastav, S.; Wang, A.; Boh, E.; Hamner, J.; Hassan, M.; Kandil, E. Disparities in the Presentation and Management of Cutaneous Melanoma That Required Admission. Oncology 2018, 95, 69–80. [Google Scholar] [CrossRef]
- Ragin, C.C.; Langevin, S.; Marzouk, M.; Grandis, J.R.; Taioli, E. Determinants of head and neck cancer survival by race. Head Neck 2010, 33, 1092–1098. [Google Scholar] [CrossRef] [Green Version]
- Taylor, D.B.; Osazuwa-Peters, O.L.; Okafor, S.I.; Boakye, E.A.; Kuziez, D.; Perera, C.; Simpson, M.C.; Barnes, J.M.; Bulbul, M.G.; Cannon, T.Y.; et al. Differential Outcomes Among Survivors of Head and Neck Cancer Belonging to Racial and Ethnic Minority Groups. JAMA Otolaryngol. Neck Surg. 2022, 148, 119. [Google Scholar] [CrossRef]
- Halpern, M.T.; Ward, E.M.; Pavluck, A.L.; Schrag, N.M.; Bian, J.; Chen, A.Y. Association of insurance status and ethnicity with cancer stage at diagnosis for 12 cancer sites: A retrospective analysis. Lancet Oncol. 2008, 9, 222–231. [Google Scholar] [CrossRef]
- Li, H.; Torabi, S.; Yarbrough, W.G.; Mehra, S.; Osborn, H.A.; Judson, B. Association of Human Papillomavirus Status at Head and Neck Carcinoma Subsites with Overall Survival. JAMA Otolaryngol. Neck Surg. 2018, 144, 519–525. [Google Scholar] [CrossRef] [Green Version]
- Yom, S.S.; Torres-Saavedra, P.; Caudell, J.J.; Waldron, J.N.; Gillison, M.L.; Xia, P.; Truong, M.T.; Kong, C.; Jordan, R.; Subramaniam, R.M.; et al. Reduced-Dose Radiation Therapy for HPV-Associated Oropharyngeal Carcinoma (NRG Oncology HN002). J. Clin. Oncol. 2021, 39, 956–965. [Google Scholar] [CrossRef]
- Taberna, M.; Mena, M.; Pavón, M.A.; Alemany, L.; Gillison, M.L.; Mesía, R. Human papillomavirus-related oropharyngeal cancer. Ann. Oncol. 2017, 28, 2386–2398. [Google Scholar] [CrossRef]
- Gillison, M.L.; Trotti, A.M.; Harris, J.; Eisbruch, A.; Harari, P.M.; Adelstein, D.J.; Jordan, R.C.K.; Zhao, W.; Sturgis, E.M.; Burtness, B.; et al. Radiotherapy plus cetuximab or cisplatin in human papillomavirus-positive oropharyngeal cancer (NRG Oncology RTOG 1016): A randomised, multicentre, non-inferiority trial. Lancet 2018, 393, 40–50. [Google Scholar] [CrossRef] [PubMed]
- Mehanna, H.; Robinson, M.; Hartley, A.; Kong, A.; Foran, B.; Fulton-Lieuw, T.; Clark, C. Radiotherapy plus cisplatin or cetuximab in low-risk human papillomavirus-positive oropharyngeal cancer (de-escalate hpv): An open-label randomised controlled phase 3 trial. Lancet 2019, 393, 51–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chera, B.S.; Amdur, R.J.; Green, R.; Shen, C.; Gupta, G.; Tan, X.; Knowles, M.; Fried, D.; Hayes, N.; Weiss, J.; et al. Phase II Trial of De-Intensified Chemoradiotherapy for Human Papillomavirus–Associated Oropharyngeal Squamous Cell Carcinoma. J. Clin. Oncol. 2019, 37, 2661–2669. [Google Scholar] [CrossRef] [PubMed]
- Sheth, S.; Farquhar, D.R.; Lenze, N.R.; Mazul, A.; Brennan, P.; Anantharaman, D.; Abedi-Ardekani, B.; Zevallos, J.P.; Hayes, D.N.; Olshan, F. Decreased overall survival in black patients with HPV-associated oropharyngeal cancer. Am. J. Otolaryngol. 2021, 42, 102780. [Google Scholar] [CrossRef]
- Pike, L.R.; Royce, T.J.; Mahal, A.R.; Kim, D.W.; Hwang, W.L.; Mahal, B.A.; Sanford, N.N. Outcomes of HPV-Associated Squamous Cell Carcinoma of the Head and Neck: Impact of Race and Socioeconomic Status. J. Natl. Compr. Cancer Netw. 2020, 18, 177–184. [Google Scholar] [CrossRef]
- Graboyes, E.M.; Garrett-Mayer, E.; Ellis, M.A.; Sharma, A.K.; Wahlquist, A.E.; Lentsch, E.J.; Nussenbaum, B.; Day, T.A. Effect of time to initiation of postoperative radiation therapy on survival in surgically managed head and neck cancer. Cancer 2017, 123, 4841–4850. [Google Scholar] [CrossRef] [Green Version]
- Goel, A.N.; Frangos, M.I.; Raghavan, G.; Lazaro, S.L.; Tang, B.; Chhetri, D.K.; Long, J.L.; John, M.A.S. The impact of treatment package time on survival in surgically managed head and neck cancer in the United States. Oral Oncol. 2018, 88, 39–48. [Google Scholar] [CrossRef]
- Ang, K.K.; Trotti, A.; Brown, B.W.; Garden, A.S.; Foote, R.L.; Morrison, W.H.; Peters, L.J. Randomized trial addressing risk features and time factors of surgery plus radiotherapy in advanced head-and-neck cancer. Int. J. Radiat. Oncol. Biol. Phys. 2001, 5, 571–578. [Google Scholar] [CrossRef]
- Ang, K.K.; Trotti, A.; Brown, B.W.; Garden, A.S.; Foote, R.L.; Morrison, W.H.; Peters, L.J. Treatment delays, race, and outcomes in head and neck cancer. Cancer Epidemiol. 2016, 45, 18–25. [Google Scholar]
- Emerson, M.A.; Golightly, Y.M.; Aiello, A.E.; Reeder-Hayes, K.E.; Tan, X.; Maduekwe, U.; Johnson-Thompson, M.; Olshan, A.F.; Troester, M.A. Breast cancer treatment delays by socioeconomic and health care access latent classes in Black and White women. Cancer 2020, 126, 4957–4966. [Google Scholar] [CrossRef]
- Chaudhary, S.; Dam, V.; Ganguly, K.; Sharma, S.; Atri, P.; Chirravuri-Venkata, R.; Cox, J.L.; Sayed, Z.; Jones, D.T.; Ganti, A.K.; et al. Differential mutation spectrum and immune landscape in African Americans versus Whites: A possible determinant to health disparity in head and neck cancer. Cancer Lett. 2020, 492, 44–53. [Google Scholar] [CrossRef]
- Kim, H.A.J.; Zeng, P.Y.F.; Sorgini, A.; Shaikh, M.H.; Khan, H.; MacNeil, D.; Khan, M.I.; Mendez, A.; Yoo, J.; Fung, K.; et al. Tumor molecular differences associated with outcome disparities of Black patients with head and neck cancer. Head Neck 2022, 44, 1124–1135. [Google Scholar] [CrossRef]
- Bazan, J.G.; Obeng-Gyasi, S.; Gamez, M.E. Reporting of Race and Hispanic Ethnicity in Breast Cancer Studies from the National Cancer Database. JAMA Oncol. 2022, 8, 1507. [Google Scholar] [CrossRef]
- Primm, K.M.; Zhao, H.; Hernandez, D.C.; Chang, S. A Contemporary Analysis of Racial and Ethnic Disparities in Diagnosis of Early-Stage Breast Cancer and Stage-Specific Survival by Molecular Subtype. Cancer Epidemiology Biomarkers Prev. 2022, 31, 1185–1194. [Google Scholar] [CrossRef]
- Charlot, M.; Stein, J.N.; Damone, E.; Wood, I.; Forster, M.; Baker, S.; Emerson, M.; Samuel-Ryals, C.; Yongue, C.; Eng, E.; et al. Effect of an Antiracism Intervention on Racial Disparities in Time to Lung Cancer Surgery. J. Clin. Oncol. 2022, 40, 1755–1762. [Google Scholar] [CrossRef]
- Brooks, S.E.; Muller, C.Y.; Robinson, W.; Walker, E.M.; Yeager, K.; Cook, E.D.; Friedman, S.; Somkin, C.P.; Brown, C.L.; McCaskill-Stevens, W. Increasing Minority Enrollment onto Clinical Trials: Practical Strategies and Challenges Emerge from the NRG Oncology Accrual Workshop. J. Oncol. Pract. 2015, 11, 486–490. [Google Scholar] [CrossRef] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Level | White (n = 262,762) | Black (n = 32,528) | NA/Other (n = 2657) | Asian (n = 6191) | Total (n = 304,138) | p-Value * |
|---|---|---|---|---|---|---|---|
| Age at Diagnosis | Mean (SD) (min, max) | 64 (12.2) (18, 90) | 61.2 (11.1) (18, 90) | 61.4 (12.4) (20, 90) | 61 (14.1) (18, 90) | 63.6 (12.1) (18, 90) | <0.0001 |
| Site | Oral Cavity | 134,941 (51%) | 10,714 (33%) | 1297 (49%) | 3170 (51%) | 150,122 (49%) | <0.0001 |
| Hypopharynx | 14,669 (6%) | 2998 (9%) | 185 (7%) | 339 (5%) | 18,191 (6%) | ||
| Larynx | 84,446 (32%) | 14,203 (44%) | 844 (32%) | 1112 (18%) | 100,605 (33%) | ||
| Nasal Cavity | 7816 (3%) | 940 (3%) | 82 (3%) | 248 (4%) | 9086 (3%) | ||
| Nasopharynx | 5622 (2%) | 1153 (4%) | 115 (4%) | 1141 (18%) | 8031 (3%) | ||
| Oropharynx | 11,396 (4%) | 2000 (6%) | 95 (4%) | 121 (2%) | 13,612 (4%) | ||
| Pharynx | 3872 (1%) | 520 (2%) | 39 (1%) | 60 (1%) | 4491 (1%) | ||
| Sex | Female | 73,263 (28%) | 8255 (25%) | 682 (26%) | 1899 (31%) | 84,099 (28%) | <0.0001 |
| Male | 189,499 (72%) | 24,273 (75%) | 1975 (74%) | 4292 (69%) | 220,039 (72%) | ||
| Ethnicity | Hispanic | 11,036 (4%) | 269 (1%) | 553 (23%) | 47 (1%) | 11,905 (4%) | <0.0001 |
| Non-Hispanic | 238,635 (96%) | 30,764 (99%) | 1848 (77%) | 5958 (99%) | 277,205 (96%) | ||
| Insurance | Not Insured | 11,968 (5%) | 2884 (9%) | 207 (8%) | 404 (7%) | 15,463 (5%) | <0.0001 |
| Private Insurance/Managed Care | 98,657 (38%) | 8051 (25%) | 903 (34%) | 2719 (44%) | 110,330 (36%) | ||
| Medicaid | 21,348 (8%) | 7111 (22%) | 395 (15%) | 947 (15%) | 29,801 (10%) | ||
| Medicare | 119,955 (46%) | 12,766 (39%) | 891 (34%) | 1943 (31%) | 135,555 (45%) | ||
| Other Government | 5279 (2%) | 707 (2%) | 139 (5%) | 44 (1%) | 6169 (2%) | ||
| Insurance Status Unknown | 5555 (2%) | 1009 (3%) | 122 (5%) | 134 (2%) | 6820 (2%) | ||
| Income | <$30,000 | 33,005 (13%) | 13,263 (42%) | 605 (23%) | 428 (7%) | 47,301 (16%) | <0.0001 |
| $30,000–$34,999 | 50,406 (20%) | 6856 (22%) | 459 (18%) | 687 (11%) | 58,408 (20%) | ||
| $35,000–$45,999 | 75,161 (30%) | 6746 (21%) | 609 (24%) | 1394 (23%) | 83,910 (28%) | ||
| ≥$46,000 | 95,980 (38%) | 4876 (15%) | 912 (35%) | 3489 (58%) | 105,257 (36%) | ||
| AJCC Clinical Stage Group (7th Edition) | 0 | 8621 (3%) | 735 (2%) | 76 (3%) | 134 (2%) | 9566 (3%) | <0.0001 |
| 1 | 58,039 (22%) | 4323 (13%) | 506 (19%) | 1226 (20%) | 64,094 (21%) | ||
| 2 | 33,649 (13%) | 3708 (11%) | 316 (12%) | 753 (12%) | 38,426 (13%) | ||
| 3 | 35,741 (14%) | 5161 (16%) | 396 (15%) | 915 (15%) | 42,213 (14%) | ||
| 4 | 76,887 (29%) | 12,662 (39%) | 827 (31%) | 1886 (30%) | 92,262 (30%) | ||
| 4C | 5187 (2%) | 1286 (4%) | 77 (3%) | 176 (3%) | 6726 (2%) | ||
| Surgery | Primary Site only | 68,269 (26%) | 4906 (15%) | 560 (21%) | 1367 (22%) | 75,102 (25%) | <0.0001 |
| Primary and Lymph Node | 64,837 (25%) | 6424 (20%) | 740 (28%) | 1897 (31%) | 73,898 (24%) | ||
| Lymph Node only | 13,080 (5%) | 1141 (4%) | 125 (5%) | 373 (6%) | 14,719 (5%) | ||
| No primary or lymph Node | 116,576 (44%) | 20,057 (62%) | 1232 (46%) | 2554 (41%) | 140,419 (46%) | ||
| Palliative Care | No palliative care provided | 256,845 (98%) | 31,377 (96%) | 2546 (96%) | 6053 (98%) | 296,821 (98%) | <0.0001 |
| Surgery | 1046 (0%) | 192 (1%) | 12 (0%) | 27 (0%) | 1277 (0%) | ||
| Radiation Therapy | 1391 (1%) | 368 (1%) | 23 (1%) | 24 (0%) | 1806 (1%) | ||
| Chemo/hormone/other systemic drugs | 811 (0%) | 205 (1%) | 12 (0%) | 17 (0%) | 1045 (0%) | ||
| Pain management | 799 (0%) | 117 (0%) | 6 (0%) | 27 (0%) | 949 (0%) | ||
| Other | 947 (0%) | 201 (1%) | 14 (1%) | 41 (1%) | 1203 (0%) | ||
| Unknown | 923 (0%) | 68 (0%) | 44 (2%) | 2 (0%) | 1037 (0%) | ||
| Charlson–Deyo Score | 0 | 199,731 (76%) | 23,922 (74%) | 2048 (77%) | 4985 (81%) | 230,686 (76%) | <0.0001 |
| 1 | 46,509 (18%) | 6131 (19%) | 455 (17%) | 976 (16%) | 54,071 (18%) | ||
| 2 | 12,084 (5%) | 1602 (5%) | 116 (4%) | 178 (3%) | 13,980 (5%) | ||
| 3 | 4438 (2%) | 873 (3%) | 38 (1%) | 52 (1%) | 5401 (2%) | ||
| Metastatic Disease | No | 246,892 (98%) | 29,638 (95%) | 2469 (97%) | 5613 (96%) | 284,612 (97%) | <0.0001 |
| Yes | 6248 (2%) | 1467 (5%) | 86 (3%) | 222 (4%) | 8023 (3%) | ||
| Chemotherapy | No | 135,110 (58%) | 13,523 (47%) | 1323 (56%) | 2837 (52%) | 152,793 (57%) | <0.0001 |
| Yes | 98,139 (42%) | 15,122 (53%) | 1032 (44%) | 2597 (48%) | 116,890 (43%) | ||
| Radiation (RT) | No | 99,367 (39%) | 9483 (30%) | 1017 (39%) | 2312 (38%) | 112,179 (38%) | <0.0001 |
| Yes | 158,685 (61%) | 22,223 (70%) | 1563 (61%) | 3739 (62%) | 186,210 (62%) | ||
| HPV Status | Negative | 28,293 (19%) | 3717 (21%) | 350 (21%) | 931 (24%) | 33,291 (20%) | <0.0001 |
| Positive | 16,859 (11%) | 1128 (6%) | 132 (8%) | 236 (6%) | 18,355 (11%) | ||
| Unknown | 102,171 (69%) | 12,586 (72%) | 1154 (71%) | 2763 (70%) | 118,674 (70%) | ||
| Total dose | Median [IQR] | 6000 [0, 7000] | 6300 [0, 7000] | 5412 [0, 7000] | 6000 [0, 7000] | 6000 [0, 7000] | <0.0001 |
| Great Circle Distance | Median [IQR] (min, max) | 12.6 [5, 31.5] (0, 4960.8) | 6.5 [3, 16.6] (0, 1938) | 12.7 [5, 36.2] (0.1, 2447.2) | 7.8 [4, 15.4] (0, 4963.1) | 11.6 [5, 29.6] (0, 4963.1) | <0.0001 |
| Surgery to Start of RT interval | <6 weeks | 20,359 (42%) | 1939 (36%) | 162 (33%) | 439 (35%) | 22,899 (41%) | <0.0001 |
| ≥6 weeks | 28,590 (58%) | 3515 (64%) | 324 (67%) | 824 (65%) | 33,253 (59%) | ||
| Distance | <4.8 | 60,996 (23%) | 12,761 (39%) | 619 (23%) | 1972 (32%) | 76,348 (25%) | <0.0001 |
| 4.8–29.7 | 132,913 (51%) | 14,741 (45%) | 1296 (49%) | 3547 (57%) | 152,497 (50%) | ||
| >29.7 | 68,853 (26%) | 5026 (15%) | 742 (28%) | 672 (11%) | 75,293 (25%) | ||
| Total Treatment Time | Median [IQR] | 101 [80, 135] | 107 [84, 145] | 107 [83, 146] | 107 [85, 142] | 102 [81, 136] | <0.0001 |
| Univariate | Multivariable | ||||
|---|---|---|---|---|---|
| HR (95%CL) | p-Value | HR (95%CL) | p-Value | ||
| Age | 1.03 (1.02 1.03) | <0.0001 | 1.02 (1.02 1.03) | <0.0001 | |
| Sex | Male | Ref | Ref | ||
| Female | 1.01 (1 1.02) | 0.0584 | 0.97 (0.94 1.01) | 0.2732 | |
| Race | White | Ref | Ref | ||
| Asian | 0.8 (0.77 0.84) | 0.84 (0.74 0.96) | 0.0098 | ||
| Black | 1.41 (1.39 1.43) | <0.0001 | 1.09 (1.03 1.15) | 0.0018 | |
| Native American/Other | 0.98 (0.93 1.04) | 0.6226 | 0.95 (0.78 1.15) | 0.6157 | |
| Ethnicity | Hispanic | Ref | Ref | ||
| Non-Hispanic | 1.05 (1.02 1.08) | 0.0003 | 1.31 (1.19 1.45) | <0.0001 | |
| Insurance Status | Private Insurance/Managed Care | Ref | Ref | ||
| Not Insured | 1.8 (1.75 1.84) | <0.0001 | 1.55 (1.43 1.68) | <0.0001 | |
| Medicaid | 2.2 (2.16 2.24) | <0.0001 | 1.83 (1.73 1.94) | <0.0001 | |
| Other Government | 1.69 (1.63 1.76) | <0.0001 | 1.15 (1.00 1.31) | 0.0359 | |
| Income | ≥$46,000 | Ref | Ref | ||
| $35,000–$45,999 | 1.18 (1.16 1.19) | <0.0001 | 1.17 (1.12 1.22) | <0.0001 | |
| $30,000–$34,999 | 1.28 (1.26 1.3) | <0.0001 | 1.21 (1.15 1.27) | <0.0001 | |
| <$30,000 | 1.46 (1.44 1.48) | <0.0001 | 1.26 (1.21 1.35) | <0.0001 | |
| TNM Clinical Stage | 1 | Ref | Ref | ||
| 2 | 1.58 (1.55 1.61) | <0.0001 | 1.53 (1.43 1.64) | <0.0001 | |
| 3 | 1.84 (1.81 1.87) | <0.0001 | 1.89 (1.77 2.02) | <0.0001 | |
| 4 | 2.29 (2.26 2.33) | <0.0001 | 2.60 (2.45 2.76) | <0.0001 | |
| Surgery | Primary Site Only | Ref | Ref | ||
| Primary and Lymph Node | 1.3 (1.27 1.32) | <0.0001 | 0.93 (0.88 0.99) | 0.0334 | |
| Lymph Node Only | 1.12 (1.09 1.15) | <0.0001 | 0.79 (0.72 0.86) | <0.0001 | |
| No Primary or Lymph Node | 1.86 (1.83 1.88) | <0.0001 | 1.20 (1.13 1.27) | <0.0001 | |
| Charlson Score | 0 | Ref | Ref | ||
| 1 | 1.38 (1.36 1.4) | <0.0001 | 1.19 (1.14 1.24) | <0.0001 | |
| 2 | 1.83 (1.79 1.87) | <0.0001 | 1.40 (1.30 1.50) | <0.0001 | |
| 3 | 2.17 (2.1 2.25) | <0.0001 | 1.94 (1.75 2.14) | <0.0001 | |
| Metastatic Disease | No | Ref | Ref | ||
| Yes | 3.87 (2.78 3.97) | <0.0001 | 2.40 (2.07 2.79) | <0.0001 | |
| HPV Status | Positive | Ref | Ref | ||
| Negative | 1.93 (1.87 2) | <0.00001 | 2.02 (1.94 2.11) | <0.0001 | |
| Distance from Facility | <4.8 | Ref | Ref | ||
| 4.8–29.7 | 0.84 (0.83 0.85) | <0.0001 | 0.91 (0.87 0.94) | <0.0001 | |
| 29.7 | 0.84 (0.83 0.86) | <0.0001 | 0.93 (0.88 0.98) | <0.001 | |
| Travel Distance | 1 (1 1) | <0.0001 | 1 (1 1) | 0.0213 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baliga, S.; Yildiz, V.O.; Bazan, J.; Palmer, J.D.; Jhawar, S.R.; Konieczkowski, D.J.; Grecula, J.; Blakaj, D.M.; Mitchell, D.; Henson, C.; et al. Disparities in Survival Outcomes among Racial/Ethnic Minorities with Head and Neck Squamous Cell Cancer in the United States. Cancers 2023, 15, 1781. https://doi.org/10.3390/cancers15061781
Baliga S, Yildiz VO, Bazan J, Palmer JD, Jhawar SR, Konieczkowski DJ, Grecula J, Blakaj DM, Mitchell D, Henson C, et al. Disparities in Survival Outcomes among Racial/Ethnic Minorities with Head and Neck Squamous Cell Cancer in the United States. Cancers. 2023; 15(6):1781. https://doi.org/10.3390/cancers15061781
Chicago/Turabian StyleBaliga, Sujith, Vedat O. Yildiz, Jose Bazan, Joshua D. Palmer, Sachin R. Jhawar, David J. Konieczkowski, John Grecula, Dukagjin M. Blakaj, Darrion Mitchell, Christina Henson, and et al. 2023. "Disparities in Survival Outcomes among Racial/Ethnic Minorities with Head and Neck Squamous Cell Cancer in the United States" Cancers 15, no. 6: 1781. https://doi.org/10.3390/cancers15061781
APA StyleBaliga, S., Yildiz, V. O., Bazan, J., Palmer, J. D., Jhawar, S. R., Konieczkowski, D. J., Grecula, J., Blakaj, D. M., Mitchell, D., Henson, C., Hu, K., Yamoah, K., & Gamez, M. E. (2023). Disparities in Survival Outcomes among Racial/Ethnic Minorities with Head and Neck Squamous Cell Cancer in the United States. Cancers, 15(6), 1781. https://doi.org/10.3390/cancers15061781