



Medical Applications of Nonadditive Entropies †



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Medical Applications
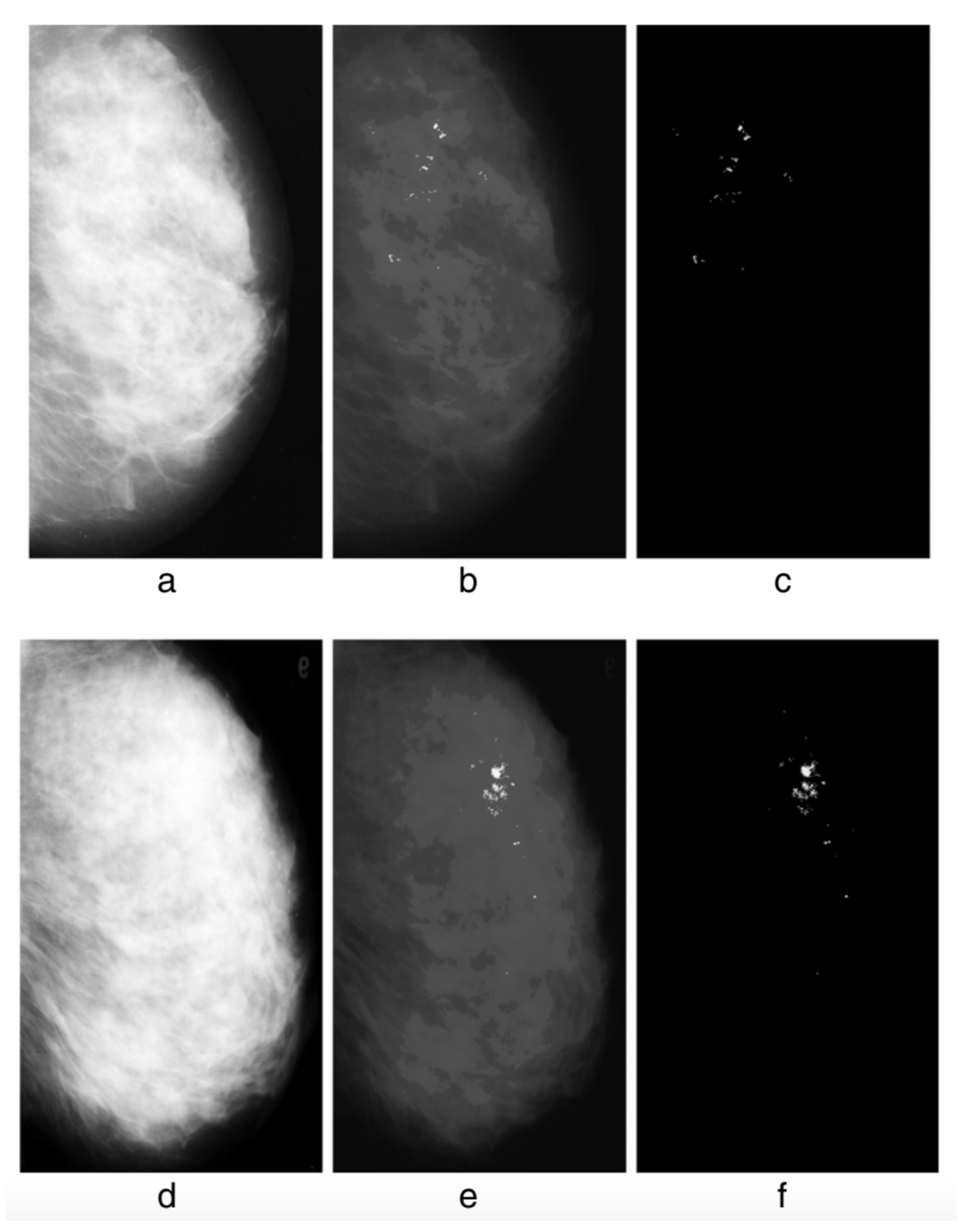
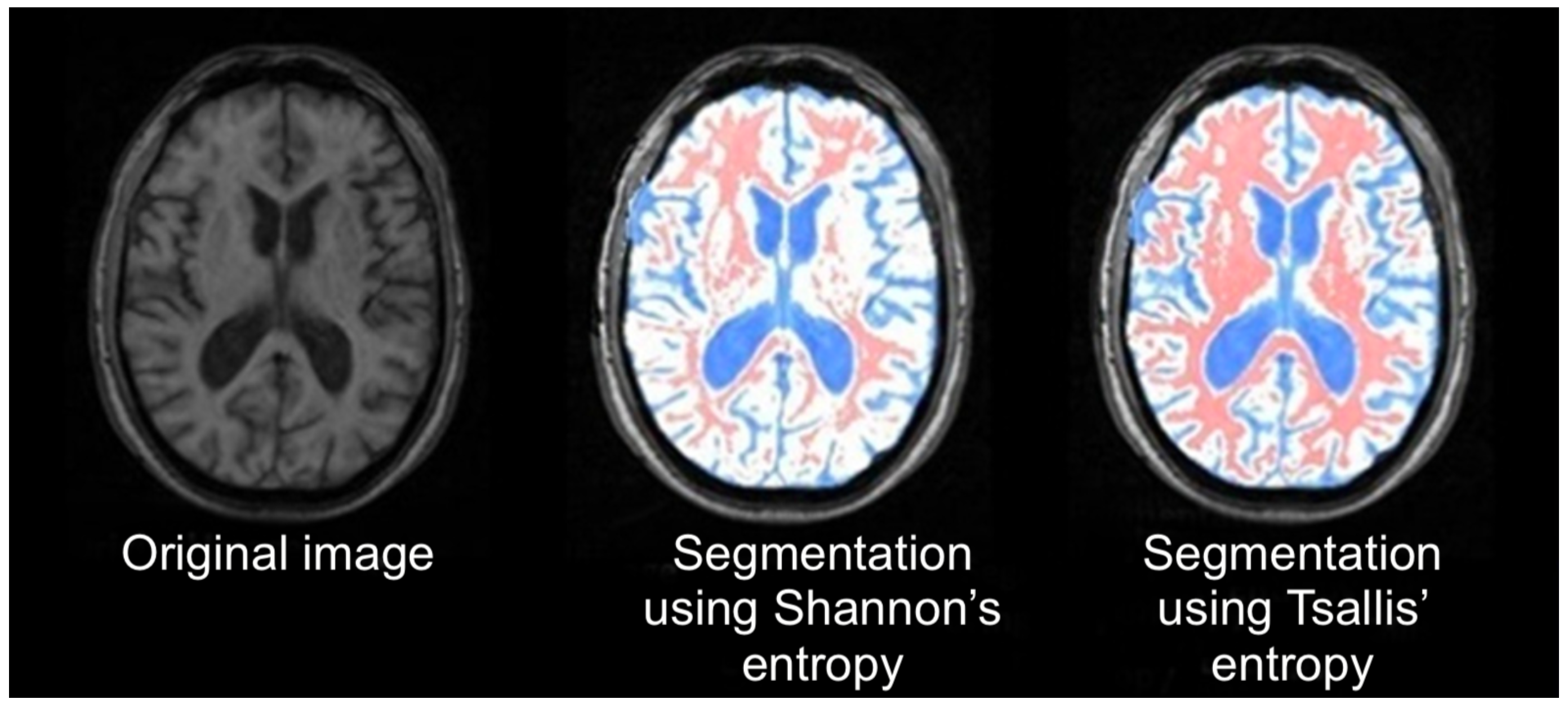
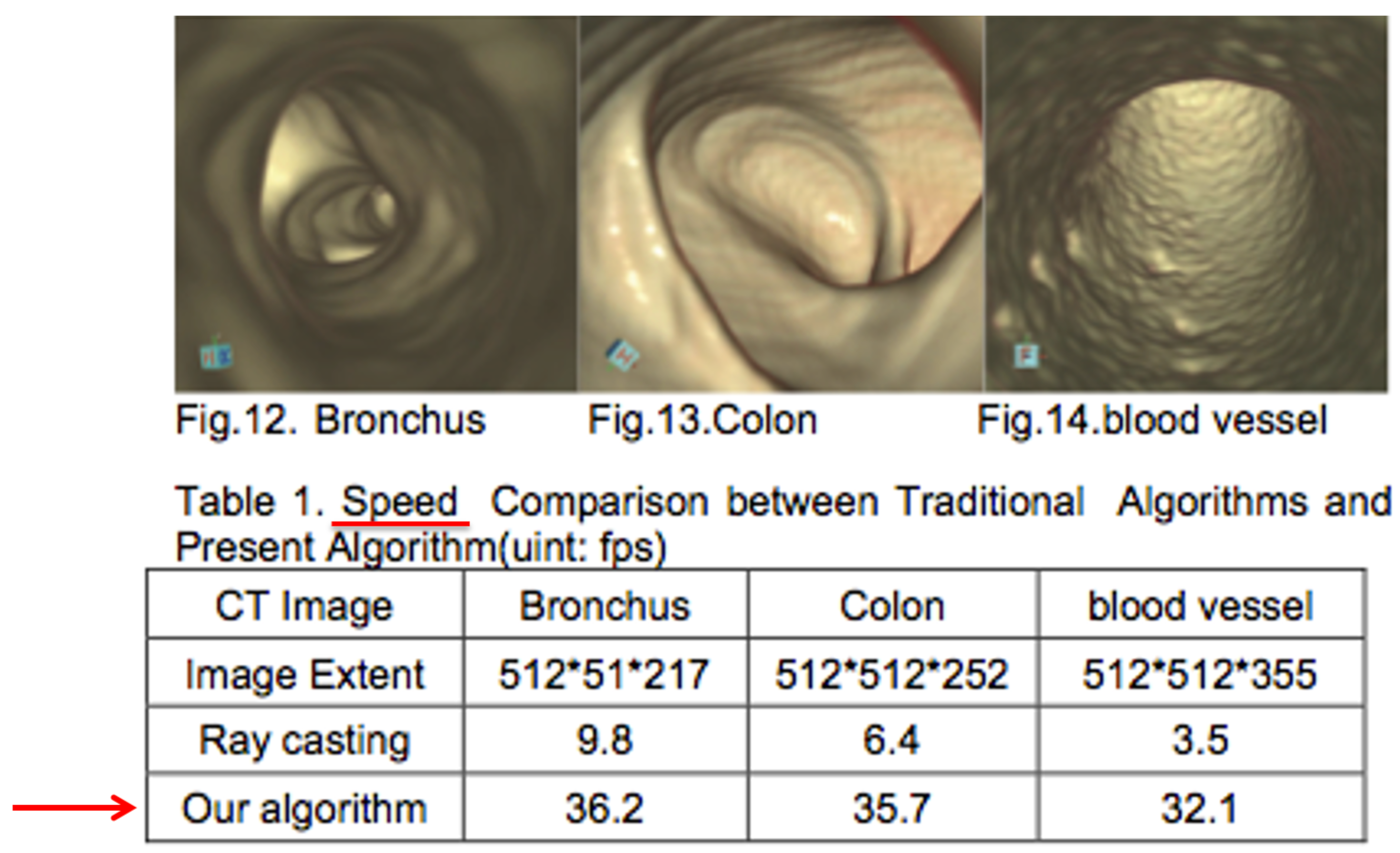
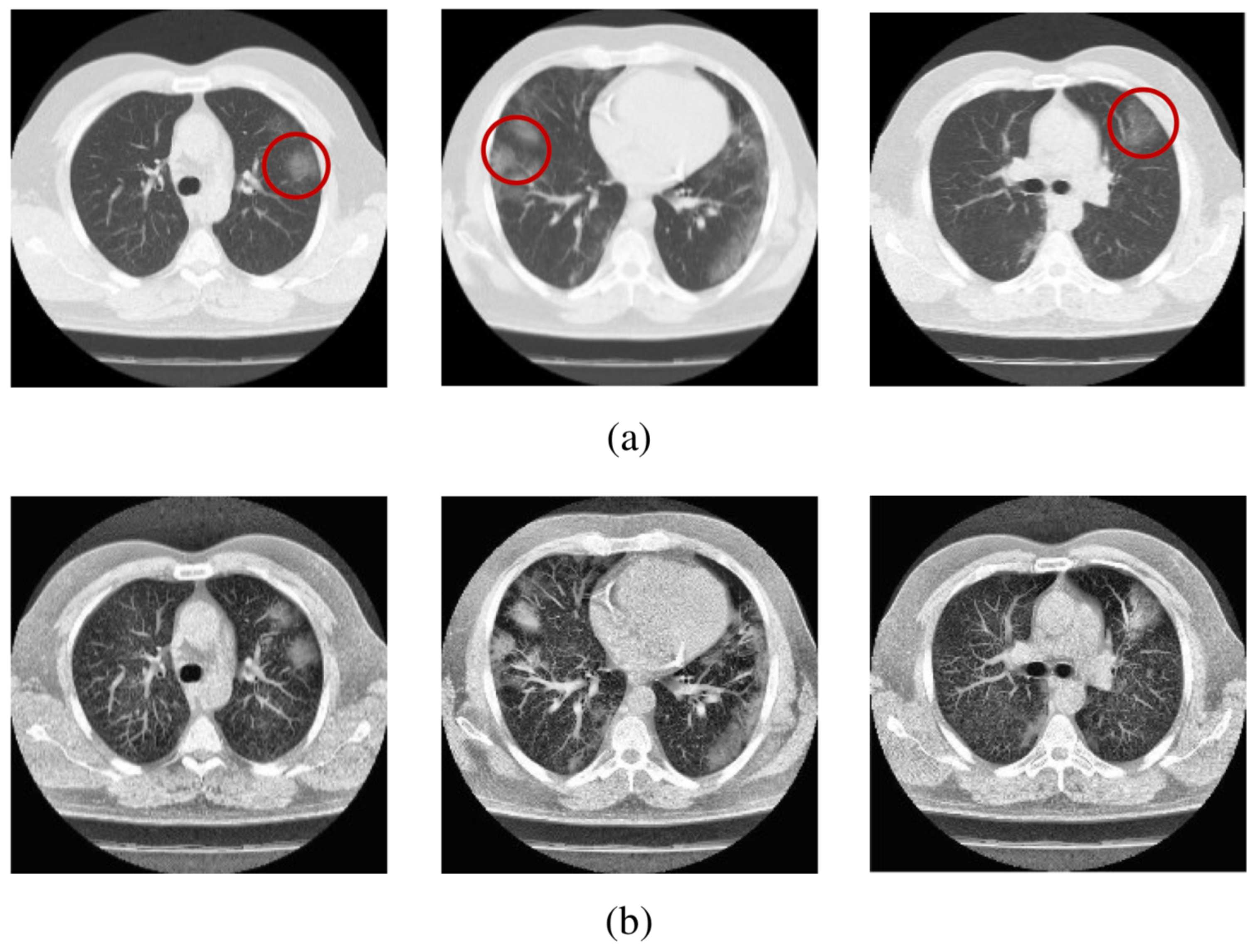
2.1. Image Processing
2.2. Signal Processing
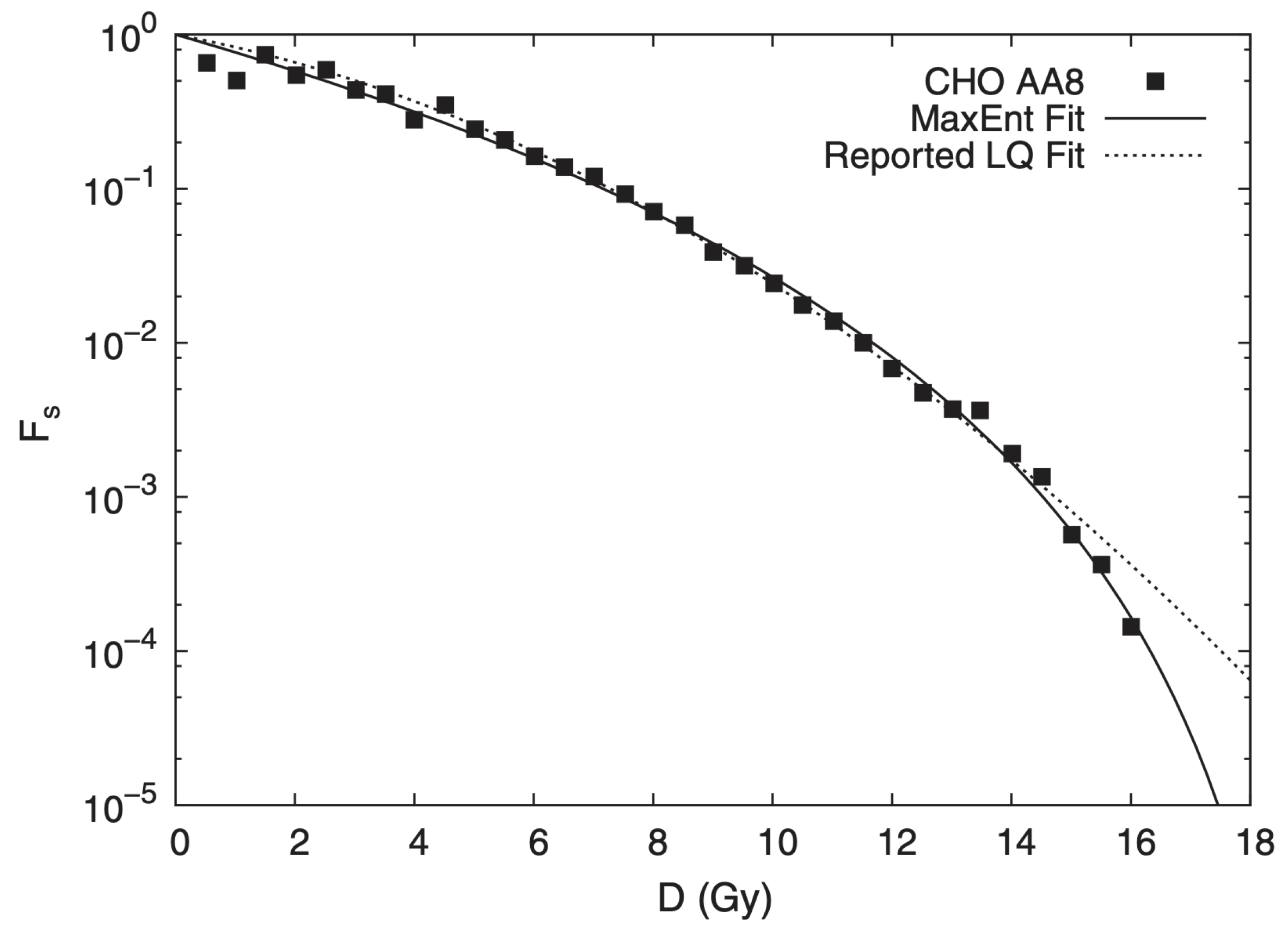
2.3. Tissue Radiation Response
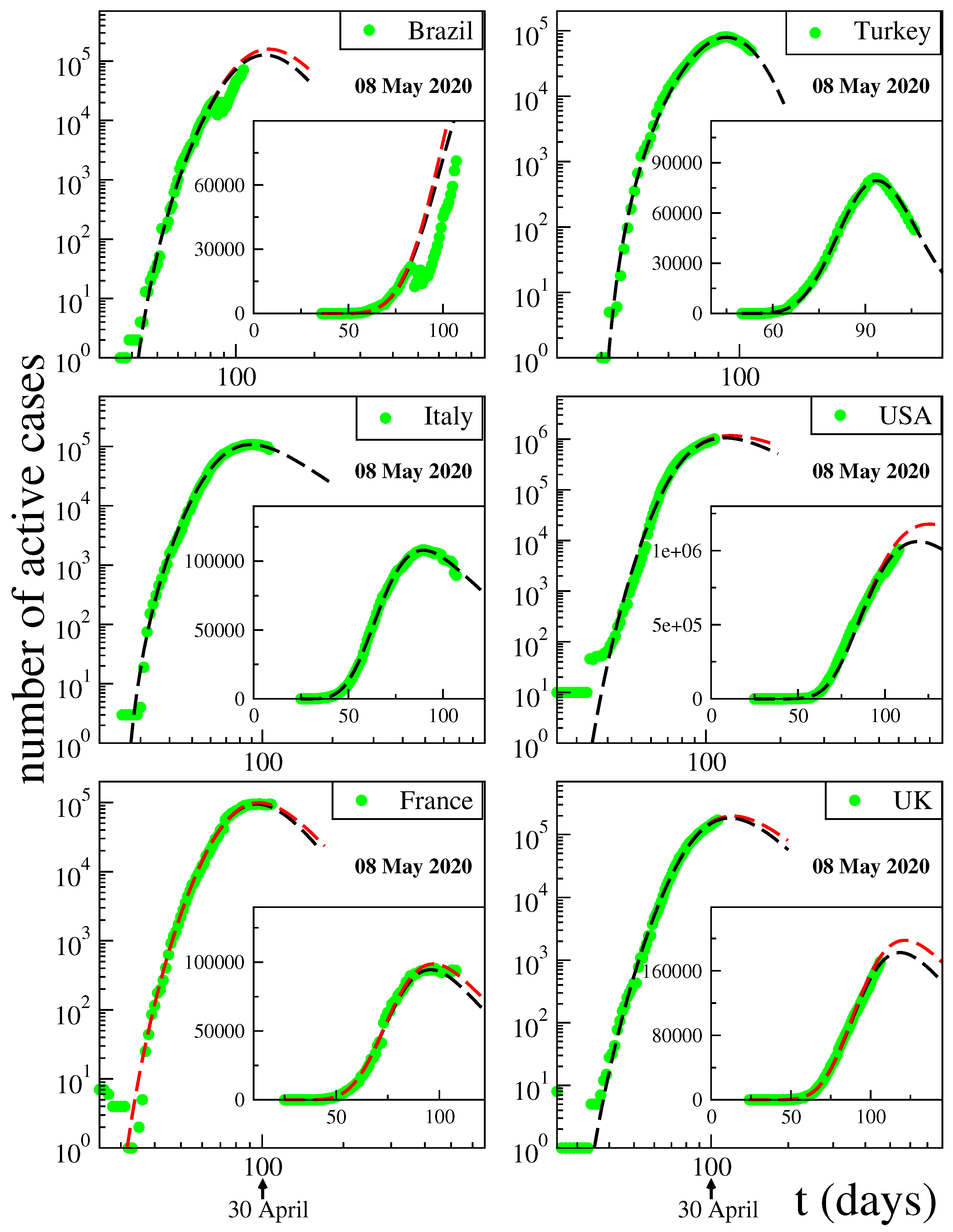
3. Modeling of Disease Kinetics
4. Final Remarks
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Tsallis, C. Entropy. Encyclopedia 2022, 2, 264–300. [Google Scholar] [CrossRef]
- Tsallis, C. Possible generalization of Boltzmann-Gibbs statistics. J. Stat. Phys. 1988, 52, 479–487. [Google Scholar] [CrossRef]
- Penrose, O. Foundations of Statistical Mechanics: A Deductive Treatment; Pergamon: Oxford, UK, 1970; p. 167. [Google Scholar]
- Gell-Mann, M.; Tsallis, C. (Eds.) Nonextensive Entropy—Interdisciplinary Applications; Oxford University Press: New York, NY, USA, 2004. [Google Scholar]
- Tsallis, C. Nonextensive Statistical Mechanics—Approaching a Complex World, 1st ed.; Springer: Berlin/Heidelberg, Germany, 2009. [Google Scholar]
- Regularly Updated Bibliography. Available online: http://tsallis.cat.cbpf.br/biblio.htm (accessed on 23 March 2023).
- Pendrill, L.; Espinoza, A.; Wadman, J.; Nilsask, F.; Wretborn, J.; Ekelund, U.; Pahlm, U. Reducing search times and entropy in hospital emergency departments with real-time location systems. IISE Trans. Healthc. Syst. Eng. 2021, 11, 305–315. [Google Scholar] [CrossRef]
- Melin, J.; Cano, S.J.; Floel, A.; Goschel, L.; Pendrill, L.R. The role of entropy in construct specification equations (CSE) to improve the validity of memory tests: Extension to word lists. Entropy 2022, 24, 934. [Google Scholar] [CrossRef] [PubMed]
- Dakhale, B.J.; Sharma, M.; Arif, M.; Asthana, K.; Bhurane, A.A.; Kothari, A.G.; Acharya, U.R. An automatic sleep-scoring system in elderly women with osteoporosis fractures using frequency localized finite orthogonal quadrature Fejer Korovkin kernels. Med. Eng. Phys. 2023, 112, 103956. [Google Scholar] [CrossRef]
- Mohanalin, J.; Beenamol, M.; Kalra, P.K.; Kumar, N. A novel automatic microcalcification detection technique using Tsallis entropy and a type II fuzzy index. Comput. Math. Appl. 2010, 60, 2426–2432. [Google Scholar] [CrossRef] [Green Version]
- Diniz, P.R.B.; Murta, L.O.; Brum, D.G.; de Araujo, D.B.; Santos, A.C. Brain tissue segmentation using q-entropy in multiple sclerosis magnetic resonance images. Braz. Med. Biol. Res. 2010, 43, 77–84. [Google Scholar] [CrossRef] [Green Version]
- Shi, W.L.; Li, Y.; Miao, Y.; Hu, Y. Research on the key technology of image guided surgery. Electr. Rev. 2012, 88, 29–33. [Google Scholar]
- Al-Azawi, R.J.; Al-Saidi, N.M.G.; Jalab, H.A.; Kahtan, H.; Ibrahim, R.W. Efficient classification of COVID-19 CT scans by using q-transform model for feature extraction. PeerJ. Comput. Sci. 2021, 7, e553. [Google Scholar] [CrossRef]
- Silva, I.; Moody, G.B.; Celi, L. Improving the quality of ECGs collected using mobile phones: The Physionet/Computing in Cardiology Challenge 2011. Comput. Cardiol. 2011, 273–276. [Google Scholar]
- Rautaharju, P.M. Eyewitness to history: Landmarks in the development of computerized electrocardiography. J. Electrocardiol. 2016, 49, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Van der Bijl, K.; Elgendi, M.; Menon, C. Automatic ECG quality assessment techniques: A systematic review. Diagnostics 2022, 12, 2578. [Google Scholar] [CrossRef] [PubMed]
- Stracina, T.; Ronzhina, M.; Redina, R.; Novakova, M. Golden standard or obsolete method? Review of ECG applications in clinical and experimental context. Front. Physiol. 2022, 13, 613. [Google Scholar] [CrossRef]
- Siontis, K.C.; Noseworthy, P.A.; Attia, Z.I.; Friedman, P.A. Artificial intelligence-enhanced electrocardiography in cardiovascular disease management. Nat. Rev. Cardiol. 2021, 18, 465–478. [Google Scholar] [CrossRef]
- Kanani, P.; Padole, M. ECG heartbeat arrhythmia classification using time-series augmented signals and deep learning approach. Procedia Comput. Sci. 2020, 171, 524–531. [Google Scholar] [CrossRef]
- Rathi, R.; Yagnik, N.; Tiwari, S.; Sharma, C. Analysis of statistical models for fast time series ECG classifications. Eng. Lett. 2022, 30, 1–12. [Google Scholar]
- Abdulghani, A.M.; Casson, A.J.; Rodriguez-Villegas, E. Compressive sensing scalp EEG signals: Implementations and practical performance. Med. Biol. Eng. Comput. 2012, 50, 1137–1145. [Google Scholar] [CrossRef]
- Chávez, M.; Martinerie, J.; Le Van Quyen, M. Statistical assessment of nonlinear causality: Application to epileptic EEG signals. J. Neurosci. Methods 2003, 124, 113–128. [Google Scholar] [CrossRef]
- Cook, M.J.; O’Brien, T.J.; Berkovic, S.M.; Murphy, M.; Morokoff, A.; Fabinyi, G.; D’Souza, W.; Yerra, R.; Archer, J.; Litewka, L.; et al. Prediction of seizure likelihood with a long-term, implanted seizure advisory system in patients with drug-resistant epilepsy: A first-in-man study. Lancet Neurol. 2013, 12, 563–571. [Google Scholar] [CrossRef]
- Devarajan, K.; Jyostna, E.; Jayasri, K.; Balasampath, V. EEG-based epilepsy detection and prediction. Int. J. Eng. Technol. 2014, 6, 212. [Google Scholar] [CrossRef] [Green Version]
- Aslam, M.H.; Usman, S.M.; Khalid, S.; Anwar, A.; Alroobaea, R.; Hussain, S.; Almotiri, J.; Ullah, S.S.; Yasin, A. Classification of EEG signals for prediction of epileptic seizures. Appl. Sci. 2022, 12, 7251. [Google Scholar] [CrossRef]
- Gajic, D.; Djurovic, Z.; Di Gennaro, S.; Gustafsson, F. Classification of EEG signals for detection of epileptic seizures based on wavelets and statistical pattern recognition. Biomed. Eng. Appl. Basis Commun. 2014, 26, 1450021. [Google Scholar] [CrossRef] [Green Version]
- Hernández, D.E.; Trujillo, L.; Flores, E.Z.; Villanueva, O.M.; Romo-Fewell, O. Detecting epilepsy in EEG signals using time, frequency and time-frequency domain features. In Computer Science and Engineering-Theory and Applications; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar]
- Coelho, V.N.; Coelho, I.M.; Coelho, B.N.; Souza, M.J.; Guimarães, F.G.; Luz, E.D.; Barbosa, A.C.; Coelho, M.N.; Netto, G.G.; Costa, R.C.; et al. EEG time series learning and classification using a hybrid forecasting model calibrated with GVNS. Electron. Notes Discret. Math. 2017, 58, 79–86. [Google Scholar] [CrossRef]
- Zeger, S.L.; Irizarry, R.; Peng, R.D. On time series analysis of public health and biomedical data. Annu. Rev. Public Health 2006, 27, 57–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aydin, S. Time series analysis and some applications in medical research. J. Math. Stat. Stud. 2022, 3, 31–36. [Google Scholar] [CrossRef]
- Bezerianos, A.; Tong, S.; Thakor, N. Time-dependent entropy estimation of EEG rhythm changes following brain ischemia. Ann. Biomed. Eng. 2003, 31, 221–232. [Google Scholar] [CrossRef]
- Tong, S.; Zhu, Y.; Geocadin, R.G.; Hanley, D.; Thakor, N.V.; Bezerianos, A. Monitoring brain injury with Tsallis entropy. In Proceedings of the 23rd IEEE Engineering in Medicine and Biology Society Annual Conference, Instanbul, Turkey, 26–28 October 2001. [Google Scholar]
- Bezerianos, A.; Tong, S.; Zhu, Y.; Thakor, N.V. Nonadditive information theory for the analyses of brain rythms. In Proceedings of the 23rd IEEE Engineering in Medicine and Biology Society Annual Conference, Instanbul, Turkey, 26–28 October 2001. [Google Scholar]
- Thakor, N.V.; Paul, J.; Tong, S.; Zhu, Y.; Bezerianos, A. Entropy of brain rhythms: Normal versus injury EEG. In Proceedings of the 11th IEEE Signal Processing Workshop, Stockholm, Sweden, 8 August 2001; pp. 261–264. [Google Scholar]
- Bezerianos, A.; Tong, S.; Paul, J.; Zhu, Y.; Thakor, N.V. Information measures of brain dynamics. In Proceedings of the 5th EURASIP Biennal International Workshop on Nonlinear Signal and Image Processing (NSP-01), Baltimore, MD, USA, 3–6 June 2001. [Google Scholar]
- Cimponeriu, L.; Tong, S.; Bezerianos, A.; Thakor, N.V. Synchronization and information processing across the cerebral cortexfollowing cardiac arrest injury. In Proceedings of the 24th Engineering in Medicine & Biology Society Conference, San Antonio, TX, USA, 26–28 October 2002. [Google Scholar]
- Tong, S.; Bezerianos, A.; Paul, J.; Zhu, Y.; Thakor, N. Nonextensive entropy measure of EEG following brain injury from cardiac arrest. Phys. A 2002, 305, 619–628. [Google Scholar] [CrossRef]
- Tong, S.; Bezerianos, A.; Malhotra, A.; Zhu, Y.; Thakor, N. Parameterized entropy analysis of EEG following hypoxic-ischemic brain injury. Phys. Lett. A 2003, 314, 354–361. [Google Scholar] [CrossRef]
- Geocadin, R.G.; Tong, S.; Bezerianos, A.; Smith, S.; Iwamoto, T.; Thakor, N.V.; Hanley, D.F. Approaching brain injury after cardiac arrest: From bench to bedside. In Proceedings of the Neuroengineering Workshop, Capri, Italy, 20–22 March 2003; pp. 277–280. [Google Scholar]
- Thakor, N.; Tong, S. Advances in quantitative electroencephalogram analysis methods. Annu. Rev. Biomed. Eng. 2004, 6, 453. [Google Scholar] [CrossRef]
- Gao, J.; Tung, W.W.; Cao, Y.; Hu, J.; Qi, Y. Power-law sensitivity to initial conditions in a time series with applications to epileptic seizure detection. Phys. A 2005, 353, 613. [Google Scholar] [CrossRef]
- Plastino, A.; Rosso, O.A. Entropy and statistical complexity in brain activity. Europhys. News 2005, 36, 224. [Google Scholar] [CrossRef] [Green Version]
- Cai, S.M.; Jiang, Z.H.; Zhou, T.; Zhou, P.L.; Yang, H.J.; Wang, B.H. Scale invariance of human electroencephalogram signals in sleep. Phys. Rev. E 2007, 76, 061903. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poza, J.; Hornero, R.; Escudero, J.; Fernandez, A.; Sanchez, C.I. Regional analysis of spontaneous MEG rhythms in patients with Alzheimer’s desease using spectral entropies. Ann. Biomed. Eng. 2008, 36, 141–152. [Google Scholar] [CrossRef] [PubMed]
- Sotolongo-Grau, O.; Rodriguez-Perez, D.; Antoranz, J.C.; Sotolongo-Costa, O. Tissue Radiation Response with Maximum Tsallis Entropy. Phys. Rev. Lett. 2010, 105, 158105. [Google Scholar] [CrossRef] [Green Version]
- Tsallis, C.; Tirnakli, U. Predicting COVID-19 peaks around the world. Front. Phys. 2020, 8, 217. [Google Scholar] [CrossRef]
- Tirnakli, U.; Tsallis, C. Epidemiological model with anomalous kinetics–Early stages of the COVID-19 pandemic. Front. Phys. 2020, 8, 613168. [Google Scholar] [CrossRef]
- Available online: https://www.worldometers.info/coronavirus/#countries (accessed on 21 March 2023).











Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsallis, C.; Pasechnik, R. Medical Applications of Nonadditive Entropies. Entropy 2023, 25, 578. https://doi.org/10.3390/e25040578
Tsallis C, Pasechnik R. Medical Applications of Nonadditive Entropies. Entropy. 2023; 25(4):578. https://doi.org/10.3390/e25040578
Chicago/Turabian StyleTsallis, Constantino, and Roman Pasechnik. 2023. "Medical Applications of Nonadditive Entropies" Entropy 25, no. 4: 578. https://doi.org/10.3390/e25040578
APA StyleTsallis, C., & Pasechnik, R. (2023). Medical Applications of Nonadditive Entropies. Entropy, 25(4), 578. https://doi.org/10.3390/e25040578