
Activity of Eribulin in a Primary Culture of Well-Differentiated/Dedifferentiated Adipocytic Sarcoma

 ,
, 
 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
2.1. Patient History
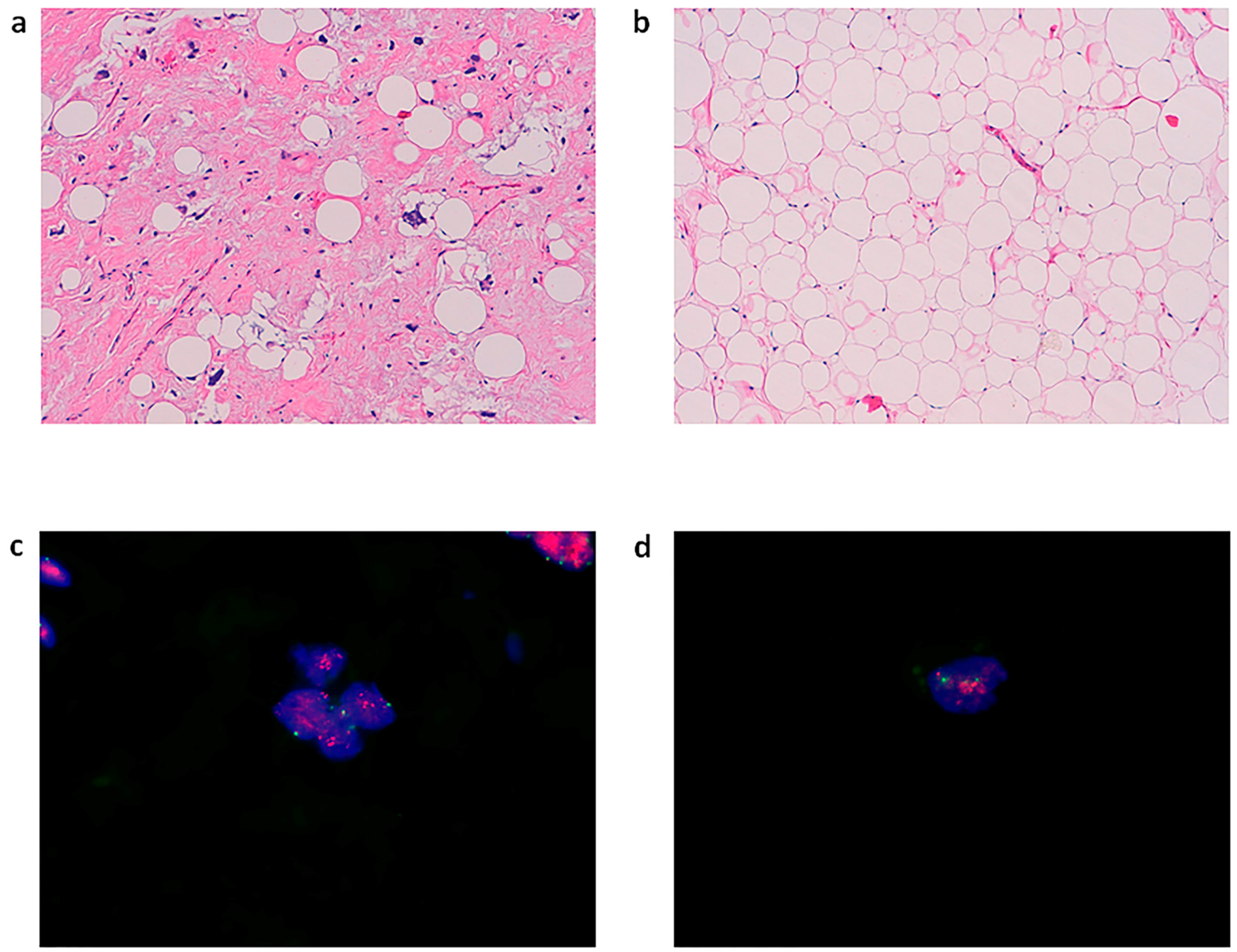
2.2. Establishment of Patient-Derived Culture of Adipocytic Sarcoma
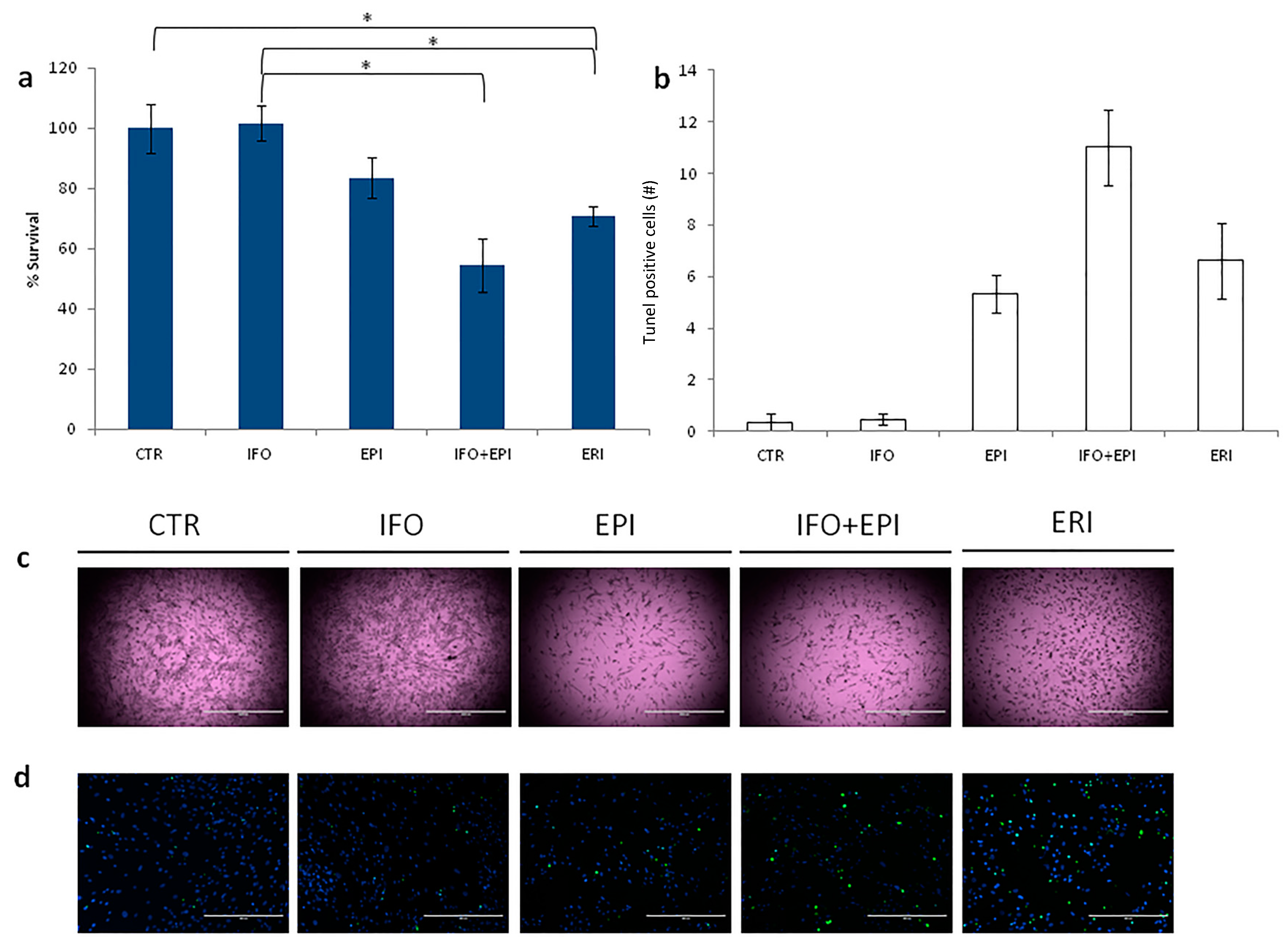
2.3. Eribulin Anticancer Activity on LPS Cells
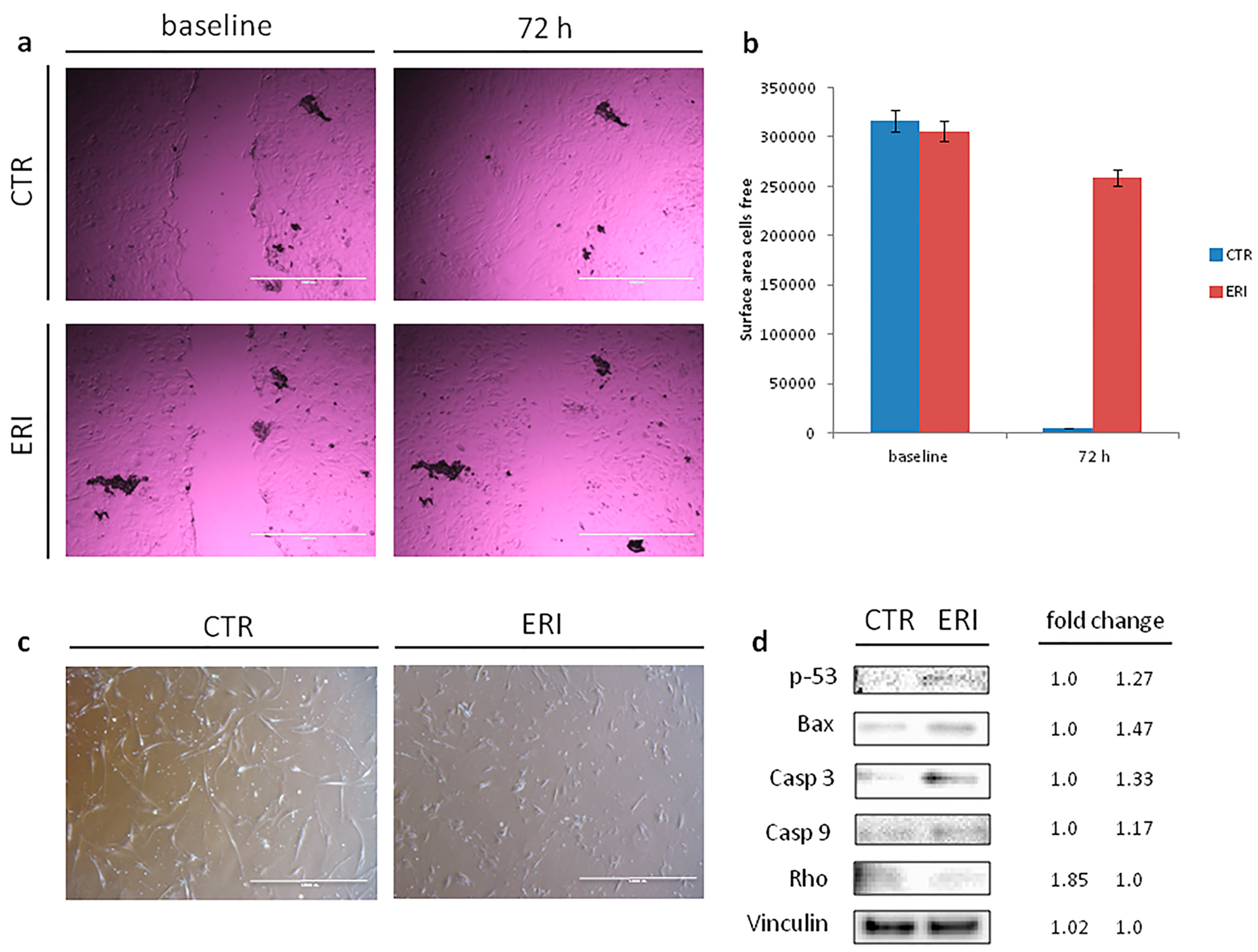
2.4. Eribulin Inhibition of Cell Migration and Induction of Apoptosis
2.5. Eribulin Modulation of the Expressions of Apoptosis and Migration-Related Proteins
3. Discussion
4. Materials and Methods
4.1. Establishment of Primary Cell Culture
4.2. Immunohistochemical Analysis
4.3. Protein Expression Analysis
4.4. Drug Testing
4.5. Tunel Assay
4.6. Cell Migration Assay
4.7. Statistical Analysis
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| ALT/DDLPS | atypical lipomatous tumor/dedifferentiated liposarcoma |
| Bax | apoptosis regulator Bax |
| Casp-3 | caspase-3 |
| Casp-9 | caspase-9 |
| CDK4 | cyclin-dependent kinase 4 |
| CHMP | Committee for Medicinal Products for Human Use |
| CT | Computed tomography |
| DDIT3 | DNA damage inducible transcript 3 |
| DDLPS | dedifferentiated liposarcoma |
| EMA | European Medicines Agency |
| EORTC | European Organisation for Research and Treatment of Cancer |
| FDA | Food and Drug Administration |
| FISH | fluorescence in situ hybridization |
| GLI | glioma-associated oncogene homolog 1 (zinc finger protein) |
| HE | haematoxylin and eosin |
| HMGIC | high-mobility-group protein gene |
| LPS | liposarcoma |
| MDM2 | mouse double minute 2 homolog |
| MLPS | myxoid liposarcoma |
| PLS | pleomorphic liposarcoma |
| Rho | rho family of GTPases |
| STS | soft tissue sarcoma |
| WHO | World Health Organization |
References
- Swami, U.; Shah, U.; Goel, S. Eribulin in Cancer Treatment. Mar. Drugs 2015, 13, 5016–5058. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.A.; Wilson, L.; Azarenko, O.; Zhu, X.; Lewis, B.M.; Littlefield, B.A.; Jordan, M.A. Eribulin binds at microtubule ends to a single site on tubulin to suppress dynamic instability. Biochemistry 2010, 49, 1331–1337. [Google Scholar] [CrossRef] [PubMed]
- Funahashi, Y.; Okamoto, K.; Adachi, Y.; Semba, T.; Uesugi, M.; Ozawa, Y.; Tohyama, O.; Uehara, T.; Kimura, T.; Watanabe, H.; et al. Eribulin mesylate reduces tumor microenvironment abnormality by vascular remodeling in preclinical human breast cancer models. Cancer Sci. 2014, 105, 1334–1342. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, T.; Ozawa, Y.; Kimura, T.; Sato, Y.; Kuznetsov, G.; Xu, S.; Uesugi, M.; Agoulnik, S.; Taylor, N.; Funahashi, Y.; et al. Eribulin mesilate suppresses experimental metastasis of breast cancer cells by reversing phenotype from epithelial-mesenchymal transition (EMT) to mesenchymal-epithelial transition (MET) states. Br. J. Cancer 2014, 110, 1497–1505. [Google Scholar] [CrossRef] [PubMed]
- Osuna, D.; de Álava, E. Molecular Pathology of Sarcomas. Rev. Recent Clin. Trials 2009, 4, 12–26. [Google Scholar] [CrossRef] [PubMed]
- Crago, A.M.; Singer, S. Clinical and molecular approaches to well differentiated and dedifferentiated liposarcoma. Curr. Opin. Oncol. 2011, 23, 373–378. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, C.D. The evolving classification of soft tissue tumours—An update based on the new 2013 WHO classification. Histopathology 2014, 64, 2–11. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, H.; Bartel, F.; Kappler, M. Gains of 13q are correlated with a poor prognosis in liposarcoma. Mod. Pathol. 2005, 18, 638–644. [Google Scholar] [CrossRef] [PubMed]
- Hostein, I.; Pelmus, M.; Aurias, A.; Pedeutour, F.; Mathoulin-Pélissier, S.; Coindre, J.M. Evaluation of MDM2 and CDK4 amplification by real-time PCR on paraffin wax-embedded material: A potential tool for the diagnosis of atypical lipomatous tumours/well-differentiated liposarcomas. J. Pathol. 2004, 202, 95–102. [Google Scholar] [CrossRef] [PubMed]
- The ESMO/European Sarcoma Network Working Group. Soft tissue and visceral sarcomas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2014, 25, iii102–iii112. [Google Scholar]
- Jones, R.L.; Fisher, C.; Al-Muderis, O. Differential sensitivity of liposarcoma subtypes to chemotherapy. Eur. J. Cancer 2005, 41, 2853–2860. [Google Scholar] [CrossRef] [PubMed]
- Schöffski, P.; Ray-Coquard, I.L.; Cioffi, A.; Bui, N.B.; Bauer, S.; Hartmann, J.T.; Krarup-Hansen, A.; Grünwald, V.; Sciot, R.; Dumez, H.; et al. Activity of eribulin mesylate in patients with soft-tissue sarcoma: A phase 2 study in four independent histological subtypes. Lancet Oncol. 2011, 12, 1045–1052. [Google Scholar]
- Schöffski, P.; Chawla, S.; Maki, R.G.; Italiano, A.; Gelderblom, H.; Choy, E.; Grignani, G.; Camargo, V.; Bauer, S.; Rha, S.Y.; et al. Eribulin versus dacarbazine in previously treated patients with advanced liposarcoma or leiomyosarcoma: A randomised, open-label, multicentre, phase 3 trial. Lancet 2016, 387, 1629–1637. [Google Scholar] [CrossRef]
- Steinstraesser, L.; Jacobsen, F.; Schubert, C.; Gevers, K.; Stricker, I.; Steinau, H.U.; Al-Benna, S. Establishment of a primary human sarcoma model in athymic nude mice. Hum. Cell 2010, 23, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Nishikata, T.; Ishikawa, M.; Matsuyama, T.; Takamatsu, K.; Fukuhara, T.; Konishi, Y. Primary culture of breast cancer: A model system for epithelial-mesenchymal transition and cancer stem cells. Anticancer Res. 2013, 33, 2867–2873. [Google Scholar] [PubMed]
- Raouf, A.; Sun, Y.J. In vitro methods to culture primary human breast epithelial cells. Methods Mol. Biol. 2013, 946, 363–381. [Google Scholar] [PubMed]
- Daigeler, A.; Klein-Hitpass, L.; Chromik, M.A.; Müller, O.; Hauser, J.; Homann, H.H.; Steinau, H.U.; Lehnhardt, M. Heterogeneous in vitro effects of doxorubicin on gene expression in primary human liposarcoma cultures. BMC Cancer 2008, 29, 313. [Google Scholar] [CrossRef] [PubMed]
- Schoenfeld, D.; Rosenbaum, C.; Horton, J. A comparison of Adriamycin versus vincristine and Adriamycin and cyclophosphamide for advanced sarcoma. Cancer 1982, 50, 2757–2762. [Google Scholar] [CrossRef]
- Bramwell, V.H.C.; Anderson, D.; Charette, M.L. Doxorubicin-Based Chemotherapy for the Palliative Treatment of Adult Patients with Locally Advanced or Metastatic Soft-Tissue Sarcoma: A Meta-Analysis and Clinical Practice Guideline. Sarcoma 2000, 4, 103–112. [Google Scholar] [CrossRef] [PubMed]
- Borden, E.C.; Amato, D.A.; Edmonson, J.H.; Ritch, P.S.; Shiraki, M. Randomized comparison of doxorubicin and vindesine to doxorubicin for patients with metastatic soft-tissue sarcomas. Cancer 1990, 66, 862–867. [Google Scholar] [CrossRef]
- Edmonson, J.H.; Ryan, L.M.; Blum, R.H.; Brooks, J.S.J.; Shiraki, M.; Frytak, S. Randomized comparison of doxorubicin alone versus ifosfamide plus doxorubicin or mitomycin, doxorubicin, and cisplatin against advanced soft tissue sarcomas. J. Clin. Oncol. 1993, 11, 1269–1275. [Google Scholar] [PubMed]
- Santoro, A.; Tursz, T.; Mouridsen, H.; Verweij, J.; Steward, W.; Somers, R. Doxorubicin versus CYVADIC versus doxorubicin plus ifosfamide in first-line treatment of advanced soft tissue sarcomas: A randomized study of the European organization for research and treatment of cancer soft tissue and bone sarcoma group. J. Clin. Oncol. 1995, 13, 1537–1545. [Google Scholar] [PubMed]
- Judson, I.; Verweij, J.; Gelderblom, H.; Hartmann, J.T.; Schöffski, P.; Blay, J.Y.; Kerst, J.M.; Sufliarsky, J.; Whelan, J.; Hohenberger, P.; et al. Doxorubicin alone versus intensified doxorubicin plus ifosfamide for first-line treatment of advanced or metastatic soft-tissue sarcoma: A randomised controlled phase 3 trial. Lancet Oncol. 2014, 15, 415–423. [Google Scholar] [CrossRef]
- Dumontet, C.; Jordan, M.A. Microtubule-binding agents: A dynamic field of cancer therapeutics. Nat. Rev. Drug Discov. 2010, 9, 790–803. [Google Scholar] [CrossRef] [PubMed]
- Highley, M.S.; Momerency, G.; Sawyers, D.; de Bruijn, E.A.; Prenen, H.; Guetens, G.; de Boeck, G.; van Oosterom, A.T.; Mansi, J.L.; Blake, P.R.; et al. The Neurotoxicity and Pharmacokinetics of Oral Ifosfamide. J. Anal. Oncol. 2015, 4, 13–23. [Google Scholar] [CrossRef]
- Cerny, T.; Leyvraz, S.; von Briel, T.; Küpfer, A.; Schaad, R.; Schmitz, S.F.; Honegger, P.; Sessa, C.; Brunner, J.; Boddy, A.V. Saturable metabolism of continuous high-dose ifosfamide with mesna and GM-CSF: A pharmacokinetic study in advanced sarcoma patients. Swiss Group for Clinical Cancer Research (SAKK). Ann. Oncol. 1999, 10, 1087–1094. [Google Scholar] [CrossRef] [PubMed]
- Fogli, S.; Danesi, R.; Gennari, A.; Donati, S.; Conte, P.F.; Del Tacca, M. Gemcitabine, epirubicin and paclitaxel: Pharmacokinetic and pharmacodynamic interactions in advanced breast cancer. Ann. Oncol. 2002, 13, 919–927. [Google Scholar] [CrossRef] [PubMed]
- Robert, J.; Vrignaud, P.; Nguyen-Ngoc, T.; Iliadis, A.; Mauriac, L.; Hurteloup, P. Comparative pharmacokinetics and metabolism of doxorubicin and epirubicin in patients with metastatic breast cancer. Cancer Treat. Rep. 1985, 69, 633–640. [Google Scholar] [PubMed]
- Danesi, R.; Innocenti, F.; Fogli, S.; Gennari, A.; Baldini, E.; Di Paolo, A.; Salvadori, B.; Bocci, G.; Conte, P.F.; Del Tacca, M. Pharmacokinetics and pharmacodynamics of combination chemotherapy with paclitaxel and epirubicinin breast cancer patients. Br. J. Clin. Pharmacol. 2002, 53, 508–518. [Google Scholar] [CrossRef] [PubMed]
- Devriese, L.A.; Witteveen, P.E.; Wanders, J.; Law, K.; Edwards, G.; Reyderman, L.; Copalu, W.; Peng, F.; Marchetti, S.; Beijnen, J.H.; et al. Pharmacokinetics of eribulin mesylate in patients with solid tumours receiving repeated oral rifampicin. Br. J. Clin. Pharmacol. 2013, 75, 507–515. [Google Scholar] [CrossRef] [PubMed]
- Mercatali, L.; Spadazzi, C.; Miserocchi, G.; Liverani, C.; De Vita, A.; Bongiovanni, A.; Recine, F.; Amadori, D.; Ibrahim, T. The Effect of Everolimus in an In Vitro Model of Triple Negative Breast Cancer and Osteoclasts. Int. J. Mol. Sci. 2016, 17, 1827. [Google Scholar] [CrossRef] [PubMed]
- Bhoopathi, P.; Chetty, C.; Kunigal, S.; Vanamala, S.K.; Rao, J.S.; Lakka, S.S. Blockade of tumor growth due to matrix metalloproteinase-9 inhibition is mediated by sequential activation of beta1-integrin, ERK, and NF-kappaB. J. Biol. Chem. 2008, 283, 1545–1552. [Google Scholar] [CrossRef] [PubMed]
- Hahnel, A.; Wichmann, H.; Kappler, M.; Kotzsch, M.; Vordermark, D.; Taubert, H.; Bache, M. Effects of osteopontin inhibition on radiosensitivity of MDA-MB-231 breast cancer cells. Radiat. Oncol. 2010, 5, 82. [Google Scholar] [CrossRef] [PubMed]
- Sample Availability: Not available.




© 2016 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Vita, A.; Miserocchi, G.; Recine, F.; Mercatali, L.; Pieri, F.; Medri, L.; Bongiovanni, A.; Cavaliere, D.; Liverani, C.; Spadazzi, C.; et al. Activity of Eribulin in a Primary Culture of Well-Differentiated/Dedifferentiated Adipocytic Sarcoma. Molecules 2016, 21, 1662. https://doi.org/10.3390/molecules21121662
De Vita A, Miserocchi G, Recine F, Mercatali L, Pieri F, Medri L, Bongiovanni A, Cavaliere D, Liverani C, Spadazzi C, et al. Activity of Eribulin in a Primary Culture of Well-Differentiated/Dedifferentiated Adipocytic Sarcoma. Molecules. 2016; 21(12):1662. https://doi.org/10.3390/molecules21121662
Chicago/Turabian StyleDe Vita, Alessandro, Giacomo Miserocchi, Federica Recine, Laura Mercatali, Federica Pieri, Laura Medri, Alberto Bongiovanni, Davide Cavaliere, Chiara Liverani, Chiara Spadazzi, and et al. 2016. "Activity of Eribulin in a Primary Culture of Well-Differentiated/Dedifferentiated Adipocytic Sarcoma" Molecules 21, no. 12: 1662. https://doi.org/10.3390/molecules21121662
APA StyleDe Vita, A., Miserocchi, G., Recine, F., Mercatali, L., Pieri, F., Medri, L., Bongiovanni, A., Cavaliere, D., Liverani, C., Spadazzi, C., Amadori, D., & Ibrahim, T. (2016). Activity of Eribulin in a Primary Culture of Well-Differentiated/Dedifferentiated Adipocytic Sarcoma. Molecules, 21(12), 1662. https://doi.org/10.3390/molecules21121662