Adiponectin, Leptin, and Leptin Receptor in Obese Patients with Type 2 Diabetes Treated with Insulin Detemir




 , , , and
, , , and
Abstract
:1. Introduction
2. Results
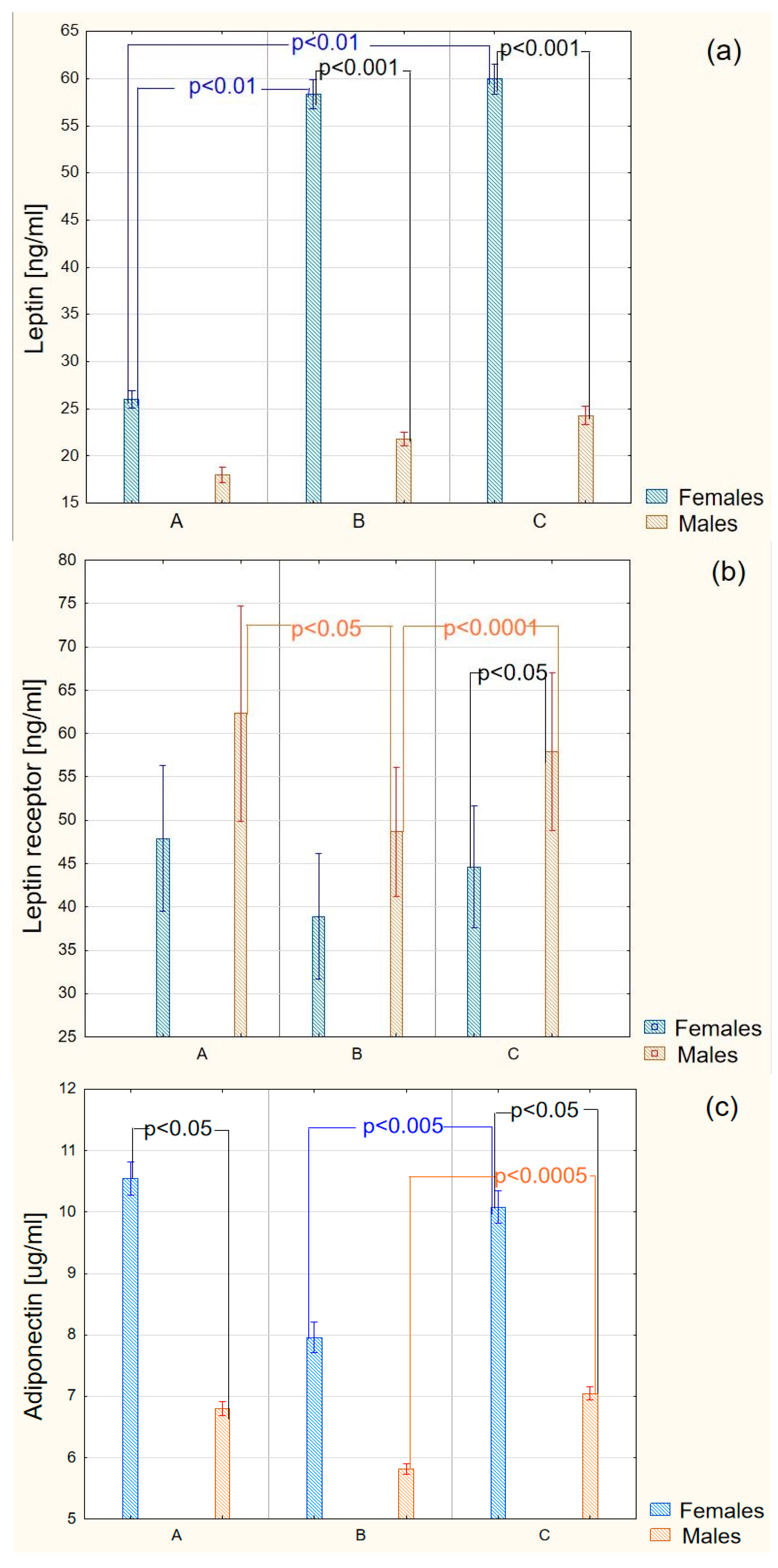
2.1. Biochemical Results
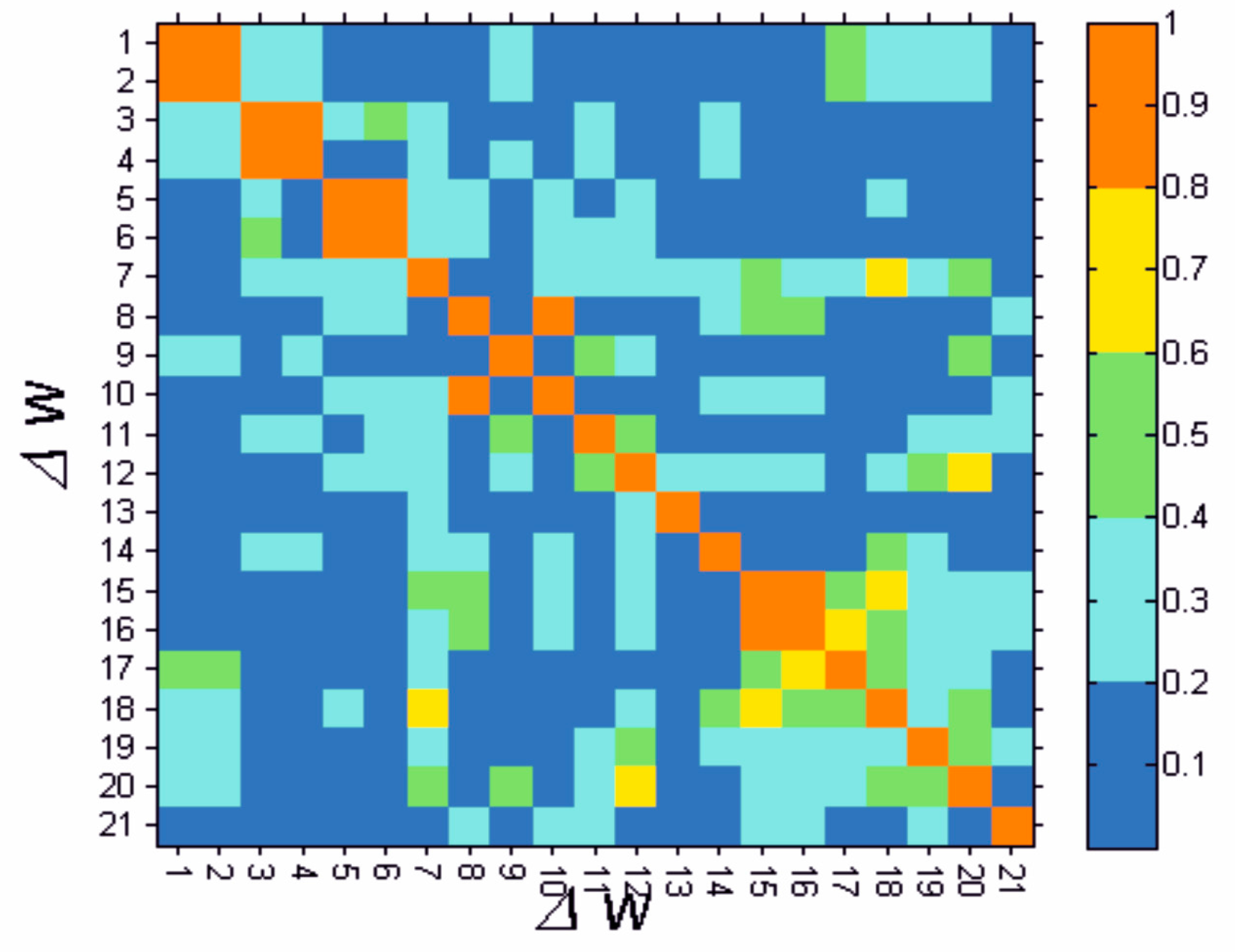
2.2. Bioinformatic Results
2.2.1. Introductory Results
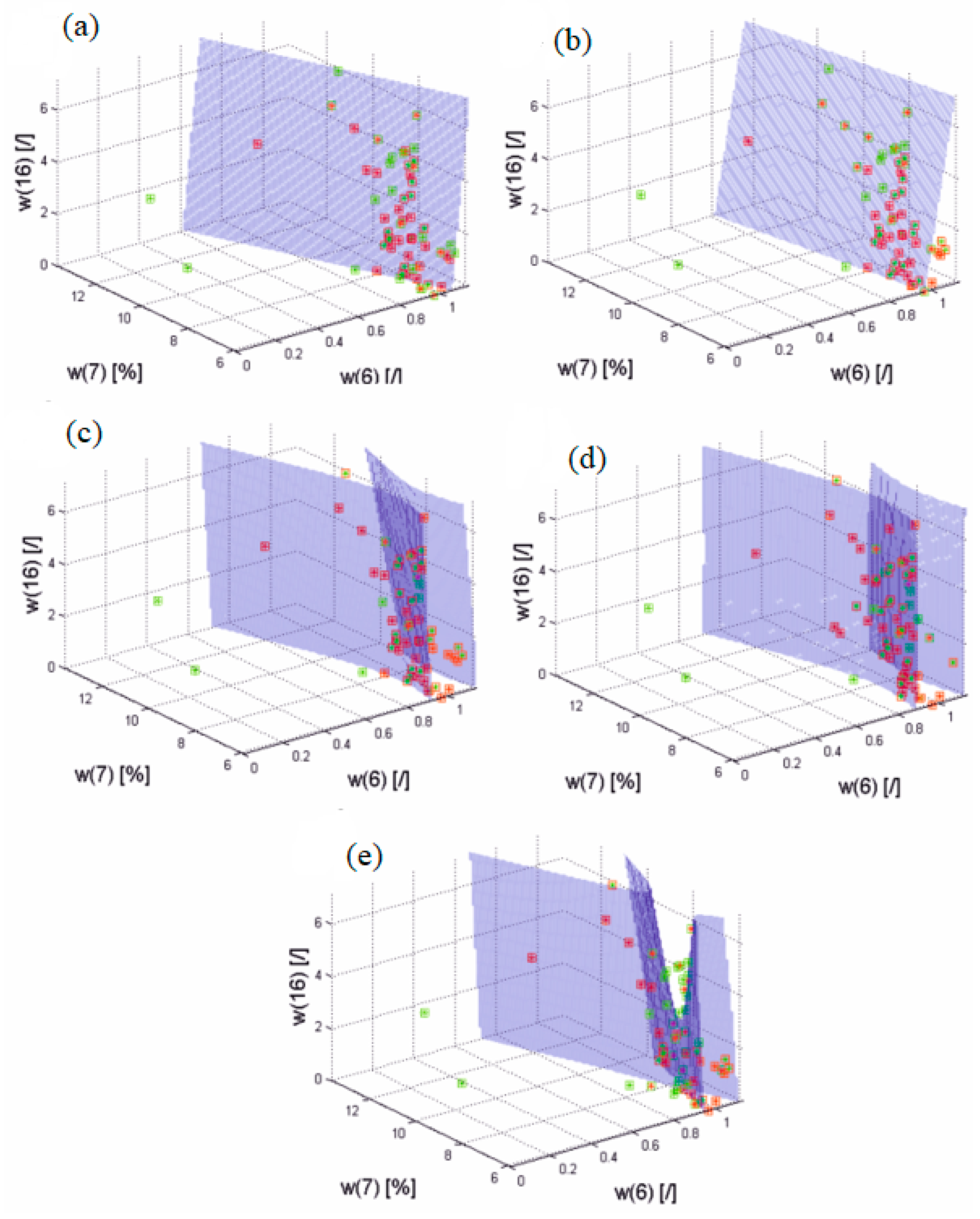
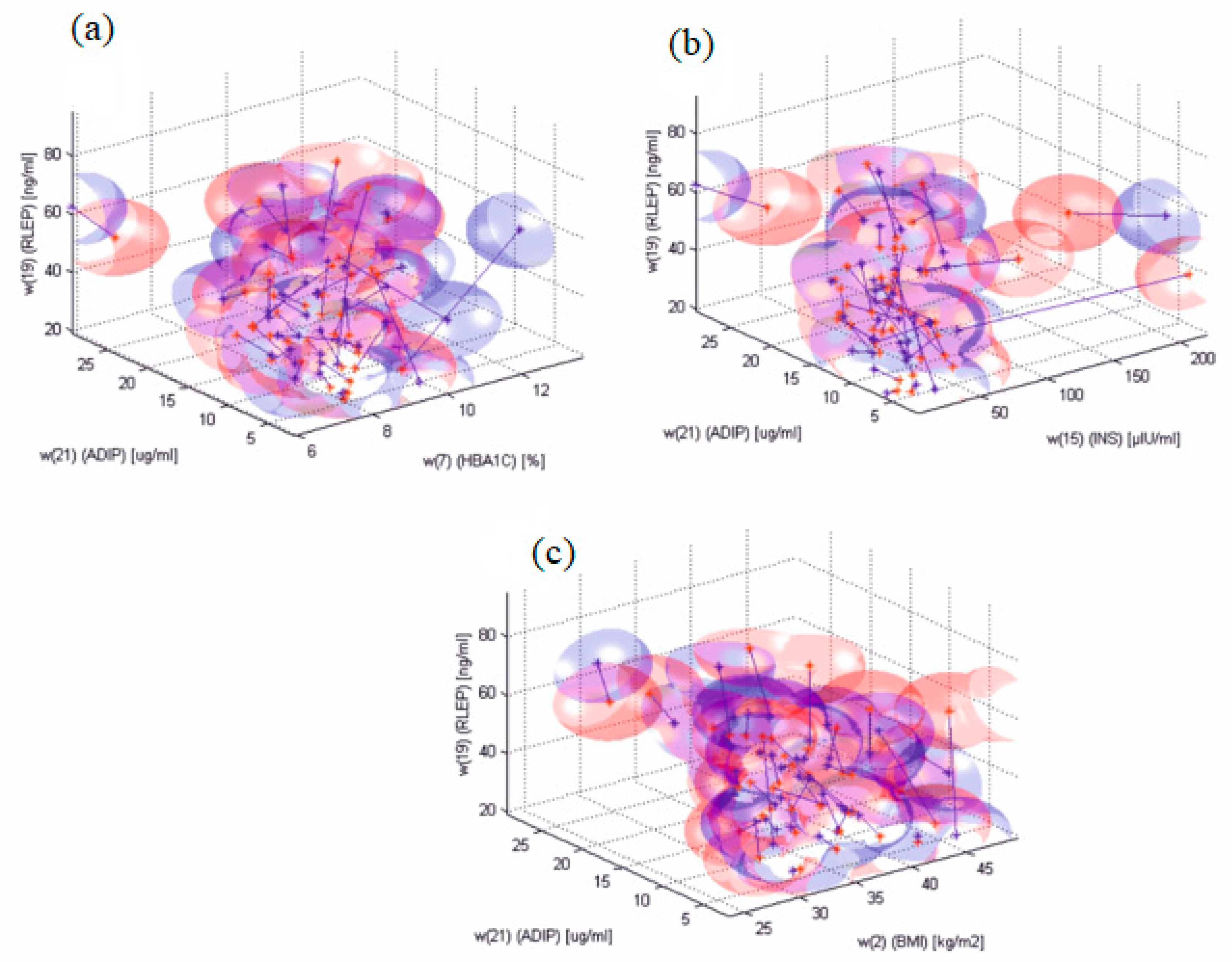
2.2.2. Results of Discriminant Analysis
3. Discussion
4. Material and Methods
4.1. Subjects
4.2. Biochemical Analysis
4.3. Statistical Analysis
4.4. Bioinformatic Analysis
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Tibaldi, J.M. The future of insulin therapy for patients with type 2 diabetes mellitus. J. Am. Osteopath. Assoc. 2013, 113, S29–S39. [Google Scholar] [PubMed]
- Nyenwe, E.A.; Jerkins, T.W.; Umpierrez, G.E.; Kitabchi, A.E. Management of type 2 diabetes: Evolving strategies for the treatment of patients with type 2 diabetes. Metabolism 2011, 60, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Palikhe, G.; Gupta, R.; Behera, B.N.; Sachdeva, N.; Gangadhar, P.; Bhansali, A. Efficacy of laparoscopic sleeve gastrectomy and intensive medical management in obese patients with type 2 diabetes mellitus. Obes. Surg. 2014, 24, 529–535. [Google Scholar] [CrossRef] [PubMed]
- Yadav, A.; Kataria, M.A.; Saini, V.; Yadav, A. Role of leptin and adiponectin in insulin resistance. Clin. Chim. Acta 2013, 417, 80–84. [Google Scholar] [CrossRef] [PubMed]
- Fjeldborg, K.; Christiansen, T.; Bennetzen, M.; Møller, H.J.; Pedersen, S.B.; Richelsen, B. The macrophage-specific serum marker, soluble CD163, is increased in obesity and reduced after dietary-induced weight loss. Obesity 2013, 21, 2437–2443. [Google Scholar] [CrossRef] [PubMed]
- Hellmann, J.; Tang, Y.; Kosuri, M.; Bhatnagar, A.; Spite, M. Resolvin D1 decreases adipose tissue macrophage accumulation and improves insulin sensitivity in obese-diabetic mice. FASEB J. 2011, 7, 2399–2407. [Google Scholar] [CrossRef] [PubMed]
- Blüher, M.; Mantzoros, C.S. From leptin to other adipokines in health and disease: Facts and expectations at the beginning of the 21st century. Metabolism 2015, 64, 131–145. [Google Scholar] [CrossRef] [PubMed]
- Blüher, M. Clinical relevance of adipokines. Diabetes Metab. J. 2012, 36, 317–327. [Google Scholar] [CrossRef] [PubMed]
- Blüher, M. Adipokines—Removing road blocks to obesity and diabetes therapy. Mol. Metab. 2014, 3, 230–240. [Google Scholar] [CrossRef] [PubMed]
- Petznick, A. Insulin management of type 2 diabetes mellitus. Am. Fam. Physician 2011, 84, 183–190. [Google Scholar] [PubMed]
- Hollander, P.A. Insulin detemir for the treatment of obese patients with type 2 diabetes. Diabetes Metab. Syndr. Obes. 2012, 5, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Frier, B.M.; Russell-Jones, D.; Heise, T. A comparison of insulin detemir and neutral protamine hagedorn (isophane) insulin in the treatment of diabetes: A systematic review. Diabetes Obes. Metab. 2013, 15, 978–986. [Google Scholar] [CrossRef] [PubMed]
- Monnier, L.; Colette, C.; Owens, D. Basal insulin analogs: From pathophysiology to therapy. What we see, know, and try to comprehend? Diabetes Metab. 2013, 39, 468–476. [Google Scholar] [CrossRef] [PubMed]
- Chaplin, S.; Joseph, F. Insulin degludec (tresiba): New ultra long-acting basal insulin. Prescriber 2013, 24, 13–18. [Google Scholar] [CrossRef]
- Surmacz, E. Leptin and adiponectin: Emerging therapeutic targets in breast cancer. J. Mammary Gland Biol. Neoplasia 2013, 18, 321–332. [Google Scholar] [CrossRef] [PubMed]
- Foster, K.R.; Koprowski, R.; Skufca, J.D. Machine learning, medical diagnosis, and biomedical engineering research—Commentary. Biomed. Eng. Online 2014, 13, 94. [Google Scholar] [CrossRef] [PubMed]
- Güngör, N.K. Overweight and obesity in children and adolescents. J. Clin. Res. Pediatr. Endocrinol. 2014, 6, 129–143. [Google Scholar] [CrossRef] [PubMed]
- Parimisetty, A.; Dorsemans, A.C.; Awada, R.; Ravanan, P.; Diotel, N.; Lefebvre d’Hellencourt, C. Secret talk between adipose tissue and central nervous system via secreted factors—An emerging frontier in the neurodegenerative research. J. Neuroinflamm. 2016, 13, 67. [Google Scholar] [CrossRef] [PubMed]
- Jung, U.J.; Choi, M.S. Obesity and its metabolic complications: The role of adipokines and the relationship between obesity, inflammation, insulin resistance, dyslipidemia and nonalcoholic fatty liver disease. Int. J. Mol. Sci. 2014, 15, 6184–6223. [Google Scholar] [CrossRef] [PubMed]
- Piya, M.K.; McTernan, P.G.; Kumar, S. Adipokine inflammation and insulin resistance: The role of glucose, lipids and endotoxin. J. Endocrinol. 2013, 216, T1–T15. [Google Scholar] [CrossRef] [PubMed]
- Barwell, N.D.; McKay, G.A.; Fisher, M. Drugs for diabetes: Part 7 insulin. Br. J. Cardiol. 2011, 18, 224–228. [Google Scholar]
- Uribarri, J.; Cai, W.; Ramdas, M.; Goodman, S.; Pyzik, R.; Chen, X.; Zhu, L.; Striker, G.E.; Vlassara, H. Restriction of advanced glycation end products improves insulin resistance in human type 2 diabetes: Potential role of AGER1 and SIRT1. Diabetes Care 2011, 34, 1610–1616. [Google Scholar] [CrossRef] [PubMed]
- Zachariah, S.; Sheldon, B.; Shojaee-Moradie, F.; Jackson, N.C.; Backhouse, K.; Johnsen, S.; Jones, R.H.; Umpleby, A.M.; Russell-Jones, D.L. Insulin detemir reduces weight gain as a result of reduced food intake in patients with type 1 diabetes. Diabetes Care 2011, 34, 1487–1491. [Google Scholar] [CrossRef] [PubMed]
- Gurkan, E.; Tarkun, I.; Sahin, T.; Cetinarslan, B.; Canturk, Z. Evaluation of exenatide versus insulin glargine for the impact on endothelial functions and cardiovascular risk markers. Diabetes Res. Clin. Pract. 2014, 106, 567–575. [Google Scholar] [CrossRef] [PubMed]
- Bunck, M.C.; Diamant, M.; Eliasson, B.; Cornér, A.; Shaginian, R.M.; Heine, R.J.; Taskinen, M.R.; Yki-Järvinen, H.; Smith, U. Exenatide affects circulating cardiovascular risk biomarkers independently of changes in body composition. Diabetes Care 2010, 33, 1734–1737. [Google Scholar] [CrossRef] [PubMed]
- Joya-Galeana, J.; Fernandez, M.; Cervera, A.; Reyna, S.; Ghosh, S.; Triplitt, C.; Musi, N.; DeFronzo, R.A.; Cersosimo, E. Effects of insulin and oral anti-diabetic agents on glucose metabolism, vascular dysfunction and skeletal muscle inflammation in type 2 diabetic subjects. Diabetes Metab. Res. Rev. 2011, 27, 373–382. [Google Scholar] [CrossRef] [PubMed]
- Considine, R.V.; Sinha, M.K.; Heiman, M.L.; Kriauciunas, A.; Stephens, T.W.; Nyce, M.R.; Ohannesian, J.P.; Marco, C.C.; McKee, L.J.; Bauer, T.L.; et al. Serum immunoreactive-leptin concentrations in normal-weight and obese humans. N. Engl. J. Med. 1996, 334, 292–295. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, T.; Hirose, H.; Yamamoto, Y.; Nishikai, K.; Miyashita, K.; Nakamura, H.; Saito, I.; Saruta, T. Relationships between serum soluble leptin receptor level and serum leptin and adiponectin levels, insulin resistance index, lipid profile, and leptin receptor gene polymorphisms in the Japanese population. Metabolism 2004, 53, 879–885. [Google Scholar] [CrossRef] [PubMed]
- Iglesias, M.J.; Eiras, S.; Piñeiro, R.; López-Otero, D.; Gallego, R.; Fernández, A.L.; Lago, F.; González-Juanatey, J.R. Gender differences in adiponectin and leptin expression in epicardial and subcutaneous adipose tissue. Findings in patients undergoing cardiac surgery. Rev. Esp. Cardiol. 2006, 59, 1252–1260. [Google Scholar] [CrossRef]
- Al Maskari, M.Y.; Alnaqdy, A.A. Correlation between serum leptin levels, body mass index and obesity in omanis. Sultan Qaboos Univ. Med. J. 2006, 6, 27–31. [Google Scholar] [PubMed]
- Kazmi, A.; Tariq, K.M.; Hashim, R. Association of leptin with type 2 diabetes in non-obese subjects. J. Ayub Med. Coll. Abbottabad 2012, 24, 186–189. [Google Scholar] [PubMed]
- Martins Mdo, C.; Lima Faleiro, L.; Fonseca, A. Relationship between leptin and body mass and metabolic syndrome in an adult population. Rev. Port. Cardiol. 2012, 31, 711–719. [Google Scholar] [CrossRef] [PubMed]
- Monti, V.; Carlson, J.J.; Hunt, S.C.; Adams, T.D. Relationship of ghrelin and leptin hormones with body mass index and waist circumference in a random sample of adults. J. Am. Diet. Assoc. 2006, 106, 822–828. [Google Scholar] [CrossRef] [PubMed]
- Vinitha, R.; Ram, J.; Snehalatha, C.; Nanditha, A.; Shetty, A.S.; Arun, R.; Godsland, I.F.; Johnston, D.G.; Ramachandran, A. Adiponectin, leptin, interleukin-6 and HbA1c in the prediction of incident type 2 diabetes: A nested case-control study in Asian Indian men with impaired glucose tolerance. Diabetes Res. Clin. Pract. 2015, 109, 340–346. [Google Scholar] [CrossRef] [PubMed]
- Mohiti, J.; Afkhami, M.; Babaei, A. Relation between leptin and insulin in patients with type II diabetes mellitus. Int. J. Endocrinol. Metab. 2015, 3, 121–125. [Google Scholar]
- Owecki, M.; Nikisch, E.; Miczke, A.; Pupek-Musialik, D.; Sowiński, J. Free leptin index as a marker for leptin action in diabetes and obesity: Leptin and soluble leptin receptors relationship with HbA1c. Neuro Endocrinol. Lett. 2010, 31, 679–683. [Google Scholar] [PubMed]
- Taghdir, M.; Djazayeri, A.; Djalali, M.; Eshraghian, M.; Rajab, A.; Yegane, H.S.; Ashourpour, M.; Sepandi, M. Relationships of serum leptin concentration with insulin, glucose, HbA1c levels and insulin resistance in overweight post-menopausal diabetic women. ARYA Atheroscler. 2010, 5, 175–180. [Google Scholar]
- Moriya, M.; Okumura, T.; Takahashi, N.; Yamagata, K.; Motomura, W.; Kohgo, Y. An inverse correlation between serum leptin levels and hemoglobin A1c in patients with non-insulin dependent diabetes mellitus. Diabetes Res. Clin. Pract. 1999, 43, 187–191. [Google Scholar] [CrossRef]
- Gogga, P.; Karbowska, J.; Meissner, W.; Kochan, Z. Rola leptyny w regulacji metabolizmu lipidów i węglowodanów. Post. Hig. Med. Dośw. 2011, 65, 255–262. [Google Scholar] [CrossRef]
- Murawska, S.; Kuczyńska, R.; Mierzwa, G.; Kulwas, A.; Rość, D.; Landowski, P.; Kamińska, B.; Czerwionka-Szaflarska, M. Evaluation of concentration of leptin and soluble receptor bound fraction of leptin in children and youth with Crohn’s disease. Przegląd Gastroenterol. 2009, 4, 262–272. [Google Scholar]
- Arnold, T.; Brandlhofer, S.; Vrtikapa, K.; Stangl, H.; Hermann, M.; Zwiauer, K.; Mangge, H.; Karwautz, A.; Huemer, J.; Koller, D.; et al. Effect of Obesity on Plasma Clusterin: A Proposed Modulator of Leptin Action. Pediatr. Res. 2011, 69, 237–242. [Google Scholar] [CrossRef] [PubMed]
- Szalecki, M.; Pańkowska, E.; Wysocka-Mincewicz, M.; Klupa, T.; Janas, R. Leptyna i rozpuszczalna forma receptora leptyny u dzieci z cukrzycą typu 1. Pediatr. Endocrinol. Diabetes Metab. 2010, 16, 262–269. [Google Scholar] [PubMed]
- Sun, Q.; van Dam, R.M.; Meigs, J.B.; Franco, O.H.; Mantzoros, C.S.; Hu, F.B. Leptin and soluble leptin receptor levels in plasma and risk of type 2 diabetes in U.S. women: A prospective study. Diabetes 2010, 59, 611–618. [Google Scholar] [CrossRef] [PubMed]
- Laimer, M.; Ebenbichler, C.F.; Kaser, S.; Sandhofer, A.; Weiss, H.; Nehoda, H.; Aigner, F.; Patsch, J.R. Weight loss increases soluble leptin receptor levels and the soluble receptor bound fraction of leptin. Obes. Res. 2002, 10, 597–601. [Google Scholar] [CrossRef] [PubMed]
- van Dielen, F.M.; van ’t Veer, C.; Buurman, W.A.; Greve, J.W. Leptin and soluble leptin receptor levels in obese and weight-losing individuals. J. Clin. Endocrinol. Metab. 2002, 87, 1708–1716. [Google Scholar] [CrossRef] [PubMed]
- Vasselli, J.R.; Scarpace, P.J.; Harris, R.B.S.; Banks, W.A. Dietary components in the development of leptin resistance. Adv. Nutr. 2013, 4, 164–175. [Google Scholar] [CrossRef] [PubMed]
- Kratzsch, J.; Deimel, A.; Galler, A.; Kapellen, T.; Klinghammer, A.; Kiess, W. Increased serum soluble leptin receptor levels in children and adolescents with type 1 diabetes mellitus. Eur. J. Endocrinol. 2004, 151, 475–481. [Google Scholar] [CrossRef] [PubMed]
- Dąbrowska, M.; Szydlarska, D.; Bar-Andziak, E. Adiponektyna a insulinooporność i miażdżyca. Endokrynol. Otyłość 2011, 7, 186–191. [Google Scholar]
- Gola, M.; Grzeszczak, W. Adiponektyna—Mechanizm działania, aktywność biologiczna i nadzieje terapeutyczne. Diabetol. Dośw. Klin. 2011, 11, 78–83. [Google Scholar]
- Aleidi, S.; Issa, A.; Bustanji, H.; Khalil, M.; Bustanji, Y. Adiponectin serum levels correlate with insulin resistance in type 2 diabetic patients. Saudi Pharm. J. 2015, 23, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Jung, C.H.; Kim, B.Y.; Mok, J.O.; Kang, S.K.; Kim, C.H. Association between serum adipocytokine levels and microangiopathies in patients with type 2 diabetes mellitus. J. Diabetes Investig. 2014, 5, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Al-Hamodi, Z.; Al-Habori, M.; Al-Meeri, A.; Saif-Ali, R. Association of adipokines, leptin/adiponectin ratio and C-reactive protein with obesity and type 2 diabetes mellitus. Diabetol. Metab. Syndr. 2014, 6, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Schulze, M.B.; Rimm, E.B.; Shai, I.; Rifai, N.; Hu, F.B. Relationship between adiponectin and glycemic control, blood lipids, and inflammatory markers in men with type 2 diabetes. Diabetes Care 2004, 27, 1680–1687. [Google Scholar] [CrossRef] [PubMed]
- Galdo, J.A.; Thurston, M.M.; Bourg, C.A. Clinical Considerations for Insulin Pharmacotherapy in Ambulatory Care, Part One: Introduction and Review of Current Products and Guidelines. Clin. Diabetes 2014, 32, 66–75. [Google Scholar] [CrossRef] [PubMed]
- Koprowski, R.; Wilczyński, S.; Wróbel, Z.; Błońska-Fajfrowska, B. Calibration and segmentation of skin areas in hyperspectral imaging for the needs of dermatology. Biomed. Eng. Online 2014, 13, 113. [Google Scholar] [CrossRef] [PubMed]
- Koprowski, R.; Wilczyński, S.; Wróbel, Z.; Kasperczyk, S.; Błońska-Fajfrowska, B. Automatic method for the dermatological diagnosis of selected hand skin features in hyperspectral imaging. Biomed. Eng. Online 2014, 13, 47. [Google Scholar] [CrossRef] [PubMed]
Sample Availability: Samples of the compounds are not available from the authors. |





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Healthy Subjects A | Untreated Diabetic Patients B | Diabetic Patients after Six-Months of Therapy C | ||
|---|---|---|---|---|
| Weight (kg) | w(1) | 84.4 ± 22.4 | 94.9 ± 14.6 a | 95.2 ± 15.4 a |
| BMI (kg/m2) | w(2) | 30.63 ± 5.4 | 34.18 ± 5.43 b | 34.4 ± 5.5 b |
| Waist (cm) | w(3) | 100.0 ± 15.3 | 112.7 ± 11.4 b | 111.2 ± 10.2 b |
| Hips (cm) | w(4) | 105.6 ± 15.9 | 112.6 ± 11.4 a | 111.5 ± 10.6 |
| Waist-hip ratio (WHR) (cm2) | w(5) | 0.95 ± 0,1 | 0.9995 ± 0.049 | 1.001 ± 0.06 |
| WHR without any reference (cm2) | w(6) | 0.95 ± 0,1 | 0.9995 ± 0.049 | 1.003 ± 0.06 |
| Glycated hemoglobin (%) | w(7) | 5.17 ± 0.45 | 7.87 ± 1.4 b | 7.78 ± 0.89 b |
| Total cholesterol (mg/dL) | w(8) | 192.3 ± 34.5 | 196.4 ± 36.1 | 188.8 ± 30.3 |
| High-density lipoprotein (HDL) cholesterol (mg/dL) | w(9) | 46.8 ± 8.76 | 49.5 ± 13.6 | 48.1 ± 12.9 |
| LDL cholesterol (mg/dL) | w(10) | 115.7 ± 28.6 | 111.4 ± 32.9 | 99.1 ± 29.9 |
| Triacylglycerols (mg/dL) | w(11) | 145.7 ± 60.7 | 176.8 ± 88.4 | 182.5 ± 68.5 |
| Creatinine (mg/dL) | w(12) | 0.84 ± 0.09 | 0.834 ± 0.528 | 0.993 ± 0.86 |
| Albumin in urine (µg/mL) | w(13) | 2.5 (2.5–4.3) * | 4.3 (2.5–15.50) *,a | 2.5 (2.5–8.4) * |
| Glucose (mg/dL) | w(14) | 90.85 ± 7.3 | 155.3 ± 45.2 | 150.6 ± 33.01 |
| Insulin (µIU/mL) | w(15) | 10.6 (4.7–23.8) * | 11.4 (4.5–25.6) * | 16.0 (7.6–29.9) *,a |
| homeostatic model assessment-insulin resistance index (HOMA—IR) | w(16) | 1.29 (0.5–2.4) * | 2.0 (1.2–3.9) *,a | 2.5 (1.6–3.8) *,a |
| Insulin sensitivity index (%S) | w(17) | 77.6 (41.1–189.5) * | 50.7 (25.8–86.8) *,a | 40.2 (26.4–63.9) *,b,c |
| Function index of the pancreatic islets β cells (%B) | w(18) | 98.8 (70.6–171.0) * | 53.5 (32.0–92.9) *,b | 71.9 (41.6–92.2) *,b |
| Leptin receptor (ng/mL) | w(19) | 56.9 ± 21.4 | 44.3 ± 16.4 b | 51.9 ± 18.9 d |
| Leptin (ng/mL) | w(20) | 21.1 ± 10.8 | 39.0 ± 16.2 a | 39.6 ± 18.4 a |
| Adiponectin (µg/mL) | w(21) | 9.01 ± 3.7 | 6.8 ± 4.2 a | 8.4 ± 4.6 d |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Olczyk, P.; Koprowski, R.; Komosinska-Vassev, K.; Jura-Półtorak, A.; Winsz-Szczotka, K.; Kuźnik-Trocha, K.; Mencner, Ł.; Telega, A.; Ivanova, D.; Olczyk, K. Adiponectin, Leptin, and Leptin Receptor in Obese Patients with Type 2 Diabetes Treated with Insulin Detemir. Molecules 2017, 22, 1274. https://doi.org/10.3390/molecules22081274
Olczyk P, Koprowski R, Komosinska-Vassev K, Jura-Półtorak A, Winsz-Szczotka K, Kuźnik-Trocha K, Mencner Ł, Telega A, Ivanova D, Olczyk K. Adiponectin, Leptin, and Leptin Receptor in Obese Patients with Type 2 Diabetes Treated with Insulin Detemir. Molecules. 2017; 22(8):1274. https://doi.org/10.3390/molecules22081274
Chicago/Turabian StyleOlczyk, Paweł, Robert Koprowski, Katarzyna Komosinska-Vassev, Agnieszka Jura-Półtorak, Katarzyna Winsz-Szczotka, Kornelia Kuźnik-Trocha, Łukasz Mencner, Alicja Telega, Diana Ivanova, and Krystyna Olczyk. 2017. "Adiponectin, Leptin, and Leptin Receptor in Obese Patients with Type 2 Diabetes Treated with Insulin Detemir" Molecules 22, no. 8: 1274. https://doi.org/10.3390/molecules22081274
APA StyleOlczyk, P., Koprowski, R., Komosinska-Vassev, K., Jura-Półtorak, A., Winsz-Szczotka, K., Kuźnik-Trocha, K., Mencner, Ł., Telega, A., Ivanova, D., & Olczyk, K. (2017). Adiponectin, Leptin, and Leptin Receptor in Obese Patients with Type 2 Diabetes Treated with Insulin Detemir. Molecules, 22(8), 1274. https://doi.org/10.3390/molecules22081274