
Anti-Inflammatory and Antioxidant Properties of Carvacrol and Magnolol, in Periodontal Disease and Diabetes Mellitus

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection and Eligibility Criteria
3. Pathogenesis of Periodontal Disease and Diabetes Mellitus
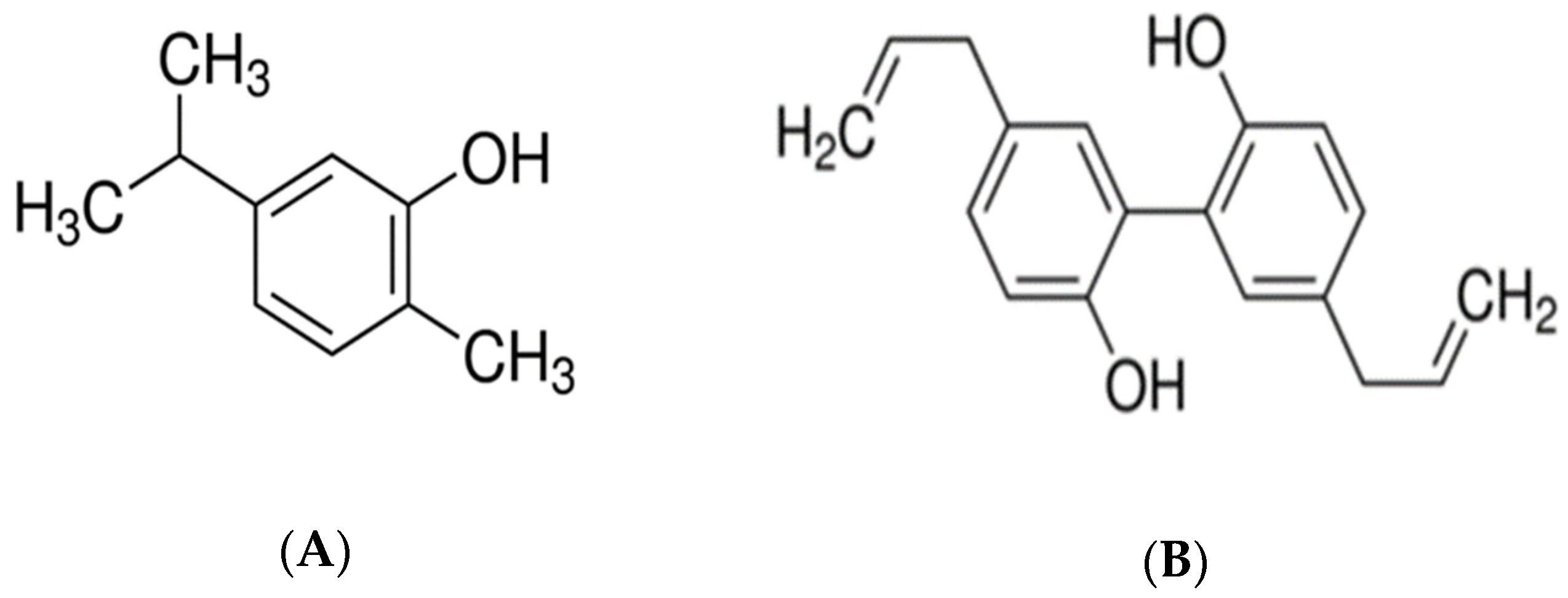
4. Chemistry of Carvacrol and Magnolol
5. Biological Activities of Carvacrol and Magnolol on Periodontitis and Diabetes
5.1. Anti-Inflammatory Effects of Carvacrol and Magnolol
5.2. Antioxidant Properties of Carvacrol and Magnolol in Association with Periodontal Disease and Diabetes Mellitus
5.3. Antimicrobial Activity of Carvacrol and Magnolol against Periodontal Pathogens
5.4. Anti-Osteoclastic Properties of Carvacrol and Magnolol
5.5. Anti-Diabetic Properties of Carvacrol and Magnolol
5.6. Toxicity of Carvacrol and Magnolol
6. Conclusions and Prospective
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| A. actinomycetemcomitans | Aggregatibacter actinomycetemcomitans |
| A.D. | Anno Domini |
| AGEs | advanced glycation end products |
| Akt | protein kinase B |
| ALP | alkaline phosphatase |
| ALT | alanine aminotransferase |
| AP-1 | activator protein-1 |
| AST | aspartate aminotransferase |
| B.C. | Before Christ |
| B. subtilis | Bacillus subtilis |
| BW | body weight |
| CAR | carvacrol |
| CAS | Chemical Abstracts Service |
| CAT | catalase |
| c-fos | C-proto-oncogene |
| CFA | complete Freund’s adjuvant |
| CHX | chlorhexidine |
| COX | cyclooxygenase |
| COX-1 | cyclooxygenase-1 |
| COX-2 | cyclooxygenase-2 |
| CRP | C-reactive protein |
| CYP2E1 | cytochrome P450 2E1 |
| DM | diabetes mellitus |
| DMSO | dimethylsulfoxide |
| DNA | deoxyribonucleic acid |
| E. coli | Escherichia coli |
| F. nucleatum | Fusobacterium nucleatum |
| FOXO1 | forkhead box protein O1 |
| ERK | extracellular signal-regulated kinases |
| GBD | Global Burden of Disease |
| GPx | glutathione peroxidase |
| GR | glutathione reductase |
| GSH | glutathione |
| HFD | high-fat diet |
| HO | hemogen oxygenase |
| HO-1 | hemogen oxygenase-1 |
| IDDM | insulin-dependent diabetes mellitus |
| IG | intragastric |
| IκB | inhibitor of kappa B kinase |
| IκBa | inhibitor of kappa B kinase α |
| IκBβ | inhibitor of kappa B kinase β |
| IL | interleukin |
| IL-1 | interleukin-1 |
| IL-1β | interleukin-1β |
| IL-4 | interleukin-4 |
| IL-6 | interleukin-6 |
| IL-8 | Interleukin-8 |
| IL-10 | interleukin-10 |
| IL-17 | interleukin-17 |
| iNOS | inducible nitric oxide synthase |
| IP | intraperitoneal |
| IUPAC | International Union of Pure and Applied Chemistry |
| IV | intravenous |
| JNK | c-Jun N-terminal kinase |
| LDH | lactate dehydrogenase |
| LDL | low-density lipoprotein |
| LPS | lipopolysaccharides |
| M. luteus | Micrococcus luteus |
| MAG | magnolol |
| MAPK | mitogen-activated protein kinase |
| MBC | minimum bactericidal concentration |
| MBE | magnolia bark extract |
| MRE | magnolia root extract |
| MDA | malondialdehyde |
| MEK | mitogen-activated protein kinase |
| MIC | minimum inhibitory concentration |
| MMP-2 | matrix metalloproteinase-2, gelatinase A |
| MMP-3 | matrix metalloproteinase-3 |
| MMP-9 | matrix metalloproteinase-9, gelatinase B |
| MMP-13 | matrix metalloproteinase-13 |
| MMPs | matrix metalloproteinases |
| MPO | myeloperoxidase |
| mRNA | messenger ribonucleic acid |
| MRSA | Methicillin-resistant Staphylococcus aureus |
| NF-κB | nuclear factor-kappa B |
| NIDDM | non-insulin-dependent diabetes mellitus |
| NK | natural killer |
| NO | nitric oxide |
| Nrf2 | nuclear factor erythroid 2-related factor 2 |
| OECD | Organisation for Economic Co-operative and Development |
| –OH | hydroxyl group |
| OG | oral gavage |
| OPG | osteoprotegerin |
| P. gingivalis | Porphyromonas gingivalis |
| P. intermedia | Prevotella intermedia |
| PGE | prostaglandins |
| PGE2 | prostaglandins E2 |
| PGF1 | prostaglandins F1 |
| PGF2 | prostaglandins F2 |
| PI3K | phosphoinositide 3-kinase |
| PO | per os |
| PPAR-γ | peroxisome proliferator-activated receptor gamma |
| Propionibacterium acnes | P. acnes |
| RANKL | receptor activator of nuclear factor-kappa B ligand |
| ROS | reactive oxygen species |
| RSG | rosiglitazone |
| S. mutans | Streptococcus mutans |
| SOD | superoxide dismutase |
| STZ | streptozotocin |
| T. denticola | Treponema denticola |
| T. forsythia | Tannerella forsythia |
| TC | total plasma cholesterol |
| TG | triglycerides |
| TGF-1β | transforming growth factor-1β |
| Th17 | T helper 17 cells |
| TNF-α | tumor necrosis factor alpha |
| TRAP | tartrate-resistant acid phosphatase |
| WHO | World Health Organization |
References
- Hernández-Monjaraz, B.; Santiago-Osorio, E.; Monroy-García, A.; Ledesma-Martínez, E.; Mendoza-Núñez, V.M. Mesenchymal stem cells of dental origin for inducing tissue regeneration in periodontitis:A mini-review. Int. J. Mol. Sci. 2018, 19, 944. [Google Scholar] [CrossRef] [Green Version]
- Reynolds, I.; Duane, B. Periodontal disease has an impact on patients′ quality of life. Evid.-Based Dent. 2018, 19, 14–15. [Google Scholar] [CrossRef] [PubMed]
- Tonetti, M.S.; Jepsen, S.; Jin, L.; Otomo-Corgel, J. Impact of the global burden of periodontal diseases on health, nutrition and wellbeing of mankind: A call for global action. J. Clin. Periodontol. 2017, 44, 456–462. [Google Scholar] [CrossRef] [Green Version]
- Vos, T.; Abajobir, A.; Abbafati, C.; Abbas, K.M.; Abate, K.H.; Abd-Allah, F.; Abebo, T.A.; Abera, S.F.; Aboyans, V.; Abu-Raddad, L.J.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016:A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1211–1259. [Google Scholar] [CrossRef] [Green Version]
- Sanz, M.; D′Aiuto, F.; Deanfield, J.; Fernandez-Aviles, F. European workshop in periodontal health and cardiovascular disease-scientific evidence on the association between periodontal and cardiovascular diseases: A review of the literature. Eur. Heart J. Suppl. 2010, 12, B3–B12. [Google Scholar] [CrossRef]
- Mealey, B.L.; Oates, T.W. Diabetes mellitus and periodontal diseases. J. Periodontol. 2006, 77, 1289–1303. [Google Scholar] [CrossRef]
- Ogurtsova, K.; da Rocha Fernandes, J.D.; Huang, Y.; Linnenkamp, U.; Guariguata, L.; Cho, N.H.; Cavan, D.; Shaw, J.E.; Makaroff, L.E. IDF Diabetes Atlas: Global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res. Clin. Pr. 2017, 128, 40–50. [Google Scholar] [CrossRef] [Green Version]
- Mathers, C.D.; Loncar, D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS. Med. 2006, 3, 442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samarghandian, S.; Farkhondeh, T.; Samini, F.; Borji, A. Protective effects of carvacrol against oxidative stress induced by chronic stress in rat’s brain, liver, and kidney. Biochem. Res. Int. 2016, 2016. [Google Scholar] [CrossRef] [Green Version]
- Suntres, Z.E.; Coccimiglio, J.; Alipour, M. The bioactivity and toxicological actions of carvacrol. Crit. Rev. Food Sci. Nutr. 2015, 55, 304–318. [Google Scholar] [CrossRef]
- Sikkema, J.; de Bont, J.A.; Poolman, B. Mechanisms of membrane toxicity of hydrocarbons. Microbiol. Rev. 1995, 59, 201–222. [Google Scholar] [CrossRef]
- Botelho, M.A.; Nogueira, N.A.; Bastos, G.M.; Fonseca, S.G.; Lemos, T.L.; Matos, F.J.; Montenegro, D.; Heukelbach, J.; Rao, V.S.; Brito, G.A. Antimicrobial activity of the essential oil from Lippia sidoides, carvacrol and thymol against oral pathogens. Braz. J. Med. Biol. Res. 2007, 40, 349–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Can Baser, K.H. Biological and pharmacological activities of carvacrol and carvacrol bearing essential oils. Curr. Pharm. Des. 2008, 14, 3106–3119. [Google Scholar] [CrossRef] [PubMed]
- Deepak, V.; Kasonga, A.; Kruger, M.C.; Coetzee, M. Carvacrol inhibits osteoclastogenesis and negatively regulates the survival of mature osteoclasts. Biol. Pharm. Bull. 2016, 39, 1150–1158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedman, M. Chemistry and multibeneficial bioactivities of carvacrol (4-isopropyl-2-methylphenol), a component of essential oils produced by aromatic plants and spices. J. Agric. Food Chem. 2014, 62, 7652–7670. [Google Scholar] [CrossRef]
- Karkabounas, S.; Kostoula, O.K.; Daskalou, T.; Veltsistas, P.; Karamouzis, M.; Zelovitis, I.; Metsios, A.; Lekkas, P.; Evangelou, A.M.; Kotsis, N.; et al. Anticarcinogenic and antiplatelet effects of carvacrol. Exp. Oncol. 2006, 28, 121–125. [Google Scholar]
- Aydin, S.; Başaran, A.A.; Başaran, N. The effects of thyme volatiles on the induction of DNA damage by the heterocyclic amine IQ and mitomycin C. Mutat. Res. 2005, 581, 43–53. [Google Scholar] [CrossRef]
- Wagner, H.; Wierer, M.; Bauer, R. In vitro inhibition of prostaglandin biosynthesis by essential oils and phenolic compounds. Planta Med. 1986, 3, 184–187. [Google Scholar] [CrossRef]
- Uyanoglu, M.; Canbek, M.; Aral, E.; Can Baser, K.H. Effects of carvacrol upon the liver of rats undergoing partial hepatectomy. Phytomedicine 2008, 15, 226–229. [Google Scholar] [CrossRef]
- Force, M.; Sparks, W.S.; Ronzio, R.A. Inhibition of enteric parasites by emulsified oil of oregano in vivo. Phytother. Res. 2000, 14, 213–214. [Google Scholar] [CrossRef]
- Kachur, K.; Suntres, Z. The antibacterial properties of phenolic isomers, carvacrol and thymol. Crit. Rev. Food Sci. Nutr. 2020, 60, 3042–3053. [Google Scholar] [CrossRef] [PubMed]
- Kwak, E.J.; Lee, Y.S.; Choi, E.M. Effect of magnolol on the function of osteoblastic MC3T3-E1 cells. Mediat. Inflamm. 2012, 2012, 96. [Google Scholar] [CrossRef] [Green Version]
- Yang, T.C.; Zhang, S.W.; Sun, L.N.; Wang, H.; Ren, A.M. Magnolol attenuates sepsis-induced gastrointestinal dysmotility in rats by modulating inflammatory mediators. World. J. Gastroenterol. 2008, 14, 7353–7360. [Google Scholar] [CrossRef]
- Weeks, B.S. Formulations of dietary supplements and herbal extracts for relaxation and anxiolytic action: Relarian. Med. Sci. Monit. 2009, 15, RA256–RA262. [Google Scholar] [PubMed]
- Chen, Y.H.; Lin, F.Y.; Liu, P.L.; Huang, Y.T.; Chiu, J.H.; Chang, Y.C.; Man, K.M.; Hong, C.Y.; Ho, Y.Y.; Lai, M.T. Antioxidative and hepatoprotective effects of magnolol on acetaminophen-induced liver damage in rats. Arch. Pharm. Res. 2009, 32, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Kang, Y.J.; Park, H.J.; Chung, H.J.; Min, H.Y.; Park, E.J.; Lee, M.A.; Shin, Y.; Lee, S.K. Wnt/β-catenin signaling mediates the antitumor activity of magnolol in colorectal cancer cells. Mol. Pharm. 2012, 82, 168–177. [Google Scholar] [CrossRef] [Green Version]
- Tsai, Y.C.; Cheng, P.Y.; Kung, C.W.; Peng, Y.J.; Ke, T.H.; Wang, J.J.; Yen, M.H. Beneficial effects of magnolol in a rodent model of endotoxin shock. Eur. J. Pharm. 2010, 641, 67–73. [Google Scholar] [CrossRef]
- Kang, J.S.; Lee, K.H.; Han, M.H.; Lee, H.; Ahn, J.M.; Han, S.B.; Han, G.; Lee, K.; Park, S.K.; Kim, H.M. Antiinflammatory activity of methanol extract isolated from stem bark of Magnolia kobus. Phytother. Res. 2008, 22, 883–888. [Google Scholar] [CrossRef]
- Shih, C.Y.; Chou, T.C. The antiplatelet activity of magnolol is mediated by PPAR-β/γ. Biochem. Pharm. 2012, 84, 793–803. [Google Scholar] [CrossRef]
- SigmaAldrich. Merck. Available online: https://www.sigmaaldrich.com/RO/en/product/aldrich/282197?context=product (accessed on 20 July 2021).
- PubChem. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/Magnolol (accessed on 20 July 2021).
- Page, R.C. The role of inflammatory mediators in the pathogenesis of periodontal disease. J. Periodontal. Res. 1991, 26, 230–242. [Google Scholar] [CrossRef]
- Lindhe, J.; Nyman, S. Clinical trials in periodontal therapy. J. Periodontal. Res. 1987, 22, 217–221. [Google Scholar] [CrossRef]
- Listgarten, M.A. Nature of periodontal diseases:Pathogenic mechanisms. J. Periodontal. Res. 1987, 22, 172–178. [Google Scholar] [CrossRef] [PubMed]
- Borgnakke, W.S.; Ylöstalo, P.V.; Taylor, G.W.; Genco, R.J. Effect of periodontal disease on diabetes:Systematic review of epidemiologic observational evidence. J. Periodontol. 2013, 84, S135–S152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Socransky, S.S.; Haffajee, A.D.; Cugini, M.A.; Smith, C.; Kent, R.L., Jr. Microbial complexes in subgingival plaque. J. Clin. Periodontol. 1998, 25, 134–144. [Google Scholar] [CrossRef]
- Carrouel, F.; Viennot, S.; Santamaria, J.; Veber, P.; Bourgeois, D. Quantitative molecular detection of 19 major pathogens in the interdental biofilm of periodontally healthy young adults. Front. Microbiol. 2016, 7, 840. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, N.; Yoneda, M.; Hirofuji, T. Mixed red-complex bacterial infection in periodontitis. Int. J. Dent. 2013, 2013, 6. [Google Scholar] [CrossRef]
- Hughes, F.J. Periodontium and periodontal disease. In Stem Cell Biology and Tissue Engineering in Dental Sciences, 1st ed.; Vishwakarma, A., Sharpe, P., Songtao, S., Ramalingam, M., Eds.; Academic Press: New York, NY, USA, 2015; pp. 433–444. [Google Scholar] [CrossRef]
- Hussain, M.; Stover, C.M.; Dupont, A.P. gingivalis in periodontal disease and atherosclerosis–scenes of action for antimicrobial peptides and complement. Front. Immunol. 2015, 6, 45. [Google Scholar] [CrossRef] [Green Version]
- Graves, D. Cytokines that promote periodontal tissue destruction. J. Periodontol. 2008, 79, 1585–1591. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Q.; Desta, T.; Fenton, M.; Graves, D.T.; Amar, S. Cytokine profiling of macrophages exposed to Porphyromonas gingivalis, its lipopolysaccharide, or its FimA protein. Infect. Immun. 2005, 73, 935–943. [Google Scholar] [CrossRef] [Green Version]
- Zhang, D.; Chen, L.; Li, S.; Gu, Z.; Yan, J. Lipopolysaccharide (LPS) of Porphyromonas gingivalis induces IL-1β, TNF-α and IL-6 production by THP-1 cells in a way different from that of Escherichia coli LPS. Innate. Immun. 2008, 14, 99–107. [Google Scholar] [CrossRef]
- Sapna, G.; Gokul, S.; Bagri-Manjrekar, K. Matrix metalloproteinases and periodontal diseases. Oral Dis. 2014, 20, 538–550. [Google Scholar] [CrossRef] [PubMed]
- Marcaccini, A.M.; Meschiari, C.A.; Zuardi, L.R.; de Sousa, T.S.; Taba, M., Jr.; Teofilo, J.M.; Jacob-Ferreira, A.L.; Tanus-Santos, J.E.; Novaes, A.B., Jr.; Gerlach, R.F. Gingival crevicular fluid levels of MMP-8, MMP-9, TIMP-2, and MPO decrease after periodontal therapy. J. Clin. Periodontol. 2010, 37, 180–190. [Google Scholar] [CrossRef] [PubMed]
- Aspriello, S.D.; Zizzi, A.; Tirabassi, G.; Buldreghini, E.; Biscotti, T.; Faloia, E.; Stramazzotti, D.; Boscaro, M.; Piemontese, M. Diabetes mellitus-associated periodontitis:Differences between type 1 and type 2 diabetes mellitus. J. Periodontal. Res. 2011, 46, 164–169. [Google Scholar] [CrossRef] [PubMed]
- Salvi, G.E.; Beck, J.D.; Offenbacher, S. PGE2, IL-1 β, and TNF-α responses in diabetics as modifiers of periodontal disease expression. Ann. Periodontol. 1998, 3, 40–50. [Google Scholar] [CrossRef]
- Salvi, G.E.; Collins, J.G.; Yalda, B.; Arnold, R.R.; Lang, N.P.; Offenbacher, S. Monocytic TNFα secretion patterns in IDDM patients with periodontal diseases. J. Clin. Periodontol. 1997, 24, 8–16. [Google Scholar] [CrossRef]
- Kamimura, D.; Ishihara, K.; Hirano, T. IL-6 Signal Transduction and Its Physiological Roles: The Signal Orchestration Model; Springer: Berlin, Germany, 2003; pp. 1–38. [Google Scholar] [CrossRef]
- Kristiansen, O.P.; Mandrup-Poulsen, T. Interleukin-6 and diabetes:The good, the bad, or the indifferent? Diabetes 2005, 54, S114–S124. [Google Scholar] [CrossRef] [Green Version]
- Hughes, F.J.; Turner, W.; Belibasakis, G.; Martuscelli, G. Effects of growth factors and cytokines on osteoblast differentiation. Periodontol. 2000 2006, 41, 48–72. [Google Scholar] [CrossRef]
- Kiritsy, C.P.; Lynch, A.B.; Lynch, S.E. Role of growth factors in cutaneous wound healing: A review. Crit. Rev. Oral. Biol. Med. 1993, 4, 729–760. [Google Scholar] [CrossRef] [Green Version]
- Marek, A.; Brodzicki, J.; Liberek, A.; Korzon, M. TGF-beta (transforming growth factor-beta) in chronic inflammatory conditions-a new diagnostic and prognostic marker. Med. Sci. Monit. 2002, 8, 145–151. [Google Scholar]
- Sporn, M.B.; Roberts, A.B. A major advance in the use of growth factors to enhance wound healing. J. Clin. Invest. 1993, 92, 2565–2566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, J.; Kakkar, P. Antihyperglycemic and antioxidant effect of Berberis aristata root extract and its role in regulating carbohydrate metabolism in diabetic rats. J. Ethnopharmacol. 2009, 123, 22–26. [Google Scholar] [CrossRef] [PubMed]
- Ban, C.R.; Twigg, S.M. Fibrosis in diabetes complications:Pathogenic mechanisms and circulating and urinary markers. Vasc. Health. Risk. Manag. 2008, 4, 575. [Google Scholar] [CrossRef] [Green Version]
- Adeva-Andany, M.M.; Pérez-Felpete, N.; Fernández-Fernández, C.; Donapetry-García, C.; Pazos-García, C. Liver glucose metabolism in humans. Biosci. Rep. 2016, 36, e00416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deshpande, A.D.; Harris-Hayes, M.; Schootman, M. Epidemiology of diabetes and diabetes-related complications. Phys. Therapy 2008, 88, 1254–1264. [Google Scholar] [CrossRef] [Green Version]
- El-Zainy, M.A.; Halawa, A.M.; Saad, F.A. Effect of diabetes mellitus on cementum periodontal interface in streptozotocin-induced diabetic rat model. Future Dent. J. 2018, 4, 181–188. [Google Scholar] [CrossRef]
- Ritchie, C.S. Mechanistic links between type 2 diabetes and periodontitis. J. Dent. 2009, 37, S578–S579. [Google Scholar] [CrossRef] [PubMed]
- Moore, P.A.; Weyant, R.J.; Mongelluzzo, M.B.; Myers, D.E.; Rossie, K.; Guggenheimer, J.; Block, H.M.; Huber, H.; Orchard, T. Type 1 diabetes mellitus and oral health:Assessment of periodontal disease. J. Periodontol. 1999, 70, 409–417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Maskari, A.Y.; Al-Maskari, M.Y.; Al-Sudairy, S. Oral manifestations and complications of diabetes mellitus: A review. Sultan. Qaboos. Univ. Med. J. 2011, 11, 179–186. [Google Scholar] [PubMed]
- Doğan, Ş.B.; Ballı, U.; Dede, F.Ö.; Sertoğlu, E.; Tazegül, K. Chemerin as a novel crevicular fluid marker of patients with periodontitis and type 2 diabetes mellitus. J. Periodontol. 2016, 87, 923–933. [Google Scholar] [CrossRef]
- Jourdain, M.L.; Velard, F.; Pierrard, L.; Sergheraert, J.; Gangloff, S.C.; Braux, J. Cationic antimicrobial peptides and periodontal physiopathology: A systematic review. J. Periodontal. Res. 2019, 54, 589–600. [Google Scholar] [CrossRef]
- Sanz, M.; Ceriello, A.; Buysschaert, M.; Chapple, I.; Demmer, R.T.; Graziani, F.; Herrera, D.; Jepsen, S.; Lione, L.; Madianos, P.; et al. Scientific evidence on the links between periodontal diseases and diabetes: Consensus report and guidelines of the joint workshop on periodontal diseases and diabetes by the International Diabetes Federation and the European Federation of Periodontology. Diabetes. Res. Clin. Pr. 2018, 137, 231–241. [Google Scholar] [CrossRef]
- Mohamed, H.G.; Idris, S.B.; Mustafa, M.; Ahmed, M.F.; Åstrøm, A.N.; Mustafa, K.; Ibrahim, S.O. Impact of chronic periodontitis on levels of glucoregulatory biomarkers in gingival crevicular fluid of adults with and without type 2 diabetes. PLoS. ONE 2015, 10, e0127660. [Google Scholar] [CrossRef] [Green Version]
- Casanova, L.; Hughes, F.J.; Preshaw, P.M. Diabetes and periodontal disease:A two-way relationship. Br. Dent. J. 2014, 217, 433–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sonnenschein, S.K.; Meyle, J. Local inflammatory reactions in patients with diabetes and periodontitis. Periodontol 2000 2015, 69, 221–254. [Google Scholar] [CrossRef] [PubMed]
- Graves, D.T.; Liu, R.; Alikhani, M.; Al-Mashat, H.; Trackman, P.C. Diabetes-enhanced inflammation and apoptosis—impact on periodontal pathology. J. Dent. Res. 2006, 85, 15–21. [Google Scholar] [CrossRef]
- Salvi, G.E.; Kandylaki, M.; Troendle, A.; Persson, G.R.; Lang, N.P. Experimental gingivitis in type 1 diabetics:A controlled clinical and microbiological study. J. Clin. Periodontol. 2005, 32, 310–316. [Google Scholar] [CrossRef]
- Ardakani, M.R.; Moeintaghavi, A.; Haerian, A.; Ardakani, M.A.; Hashemzadeh, M. Correlation between levels of sulcular and capillary blood glucose. J. Contemp. Dent. Pr. 2009, 10, 10–17. [Google Scholar]
- Sakallioğlu, E.E.; Lütfioğlu, M.; Sakallioğlu, U.; Diraman, E.; Keskiner, I. Fluid dynamics of gingiva in diabetic and systemically healthy periodontitis patients. Arch. Oral Biol. 2008, 53, 646–651. [Google Scholar] [CrossRef] [PubMed]
- Salvi, G.E.; Franco, L.M.; Braun, T.M.; Lee, A.; Rutger Persson, G.; Lang, N.P.; Giannobile, W.V. Pro-inflammatory biomarkers during experimental gingivitis in patients with type 1 diabetes mellitus:A proof-of-concept study. J. Clin. Periodontol. 2010, 37, 9–16. [Google Scholar] [CrossRef] [Green Version]
- Engebretson, S.; Chertog, R.; Nichols, A.; Hey-Hadavi, J.; Celenti, R.; Grbic, J. Plasma levels of tumour necrosis factor-alpha in patients with chronic periodontitis and type 2 diabetes. J. Clin. Periodontol. 2007, 34, 18–24. [Google Scholar] [CrossRef]
- de Miguel-Infante, A.; Martinez-Huedo, M.A.; Mora-Zamorano, E.; Hernández-Barrera, V.; Jiménez-Trujillo, I.; de Burgos-Lunar, C.; Cardenas Valladolid, J.; Jiménez-García, R.; Lopez-de-Andrés, A. Periodontal disease in adults with diabetes, prevalence and risk factors. Results of an observational study. Int. J. Clin. Pr. 2019, 73, e13294. [Google Scholar] [CrossRef] [PubMed]
- Lim, L.P.; Tay, F.B.; Sum, C.F.; Thai, A.C. Relationship between markers of metabolic control and inflammation on severity of periodontal disease in patients with diabetes mellitus. J. Clin. Periodontol. 2007, 34, 118–123. [Google Scholar] [CrossRef]
- Grossi, S.G.; Zambon, J.J.; Ho, A.W.; Koch, G.; Dunford, R.G.; Machtei, E.E.; Norderyd, O.M.; Genco, R.J. Assessment of risk for periodontal disease. I. Risk indicators for attachment loss. J. Periodontol. 1994, 65, 260–267. [Google Scholar] [CrossRef] [PubMed]
- Mealey, B. Diabetes and periodontal diseases. J. Periodontol. 1999, 70, 935–949. [Google Scholar] [CrossRef]
- Salvi, G.E.; Yalda, B.; Collins, J.G.; Jones, B.H.; Smith, F.W.; Arnold, R.R.; Offenbacher, S. Inflammatory mediator response as a potential risk marker for periodontal diseases in insulin-dependent diabetes mellitus patients. J. Periodontol. 1997, 68, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Santos Tunes, R.; Foss-Freitas, M.C.; Nogueira-Filho, G.d.R. Impact of periodontitis on the diabetes-related inflammatory status. J. Can. Dent. Assoc. 2010, 76, 1–7. [Google Scholar]
- Noack, B.; Genco, R.J.; Trevisan, M.; Grossi, S.; Zambon, J.J.; De Nardin, E. Periodontal infections contribute to elevated systemic C-reactive protein level. J. Periodontol. 2001, 72, 1221–1227. [Google Scholar] [CrossRef] [Green Version]
- Loos, B.G.; Craandijk, J.; Hoek, F.J.; Wertheim-van Dillen, P.M.; van der Velden, U. Elevation of systemic markers related to cardiovascular diseases in the peripheral blood of periodontitis patients. J. Periodontol. 2000, 71, 1528–1534. [Google Scholar] [CrossRef]
- Wu, T.; Trevisan, M.; Genco, R.J.; Falkner, K.L.; Dorn, J.P.; Sempos, C.T. Examination of the relation between periodontal health status and cardiovascular risk factors:Serum total and high density lipoprotein cholesterol, C-reactive protein, and plasma fibrinogen. Am. J. Epidemiol. 2000, 151, 273–282. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.; Wei, B.; Li, J.; Liu, F.; Xuan, D.; Xie, B.; Zhang, J. Association of periodontal parameters with metabolic level and systemic inflammatory markers in patients with type 2 diabetes. J. Periodontol. 2010, 81, 364–371. [Google Scholar] [CrossRef]
- Patil, V.S.; Patil, V.P.; Gokhale, N.; Acharya, A.; Kangokar, P. Chronic periodontitis in type 2 diabetes mellitus:Oxidative stress as a common factor in periodontal tissue injury. J. Clin. Diagn. Res. 2016, 10, 12–16. [Google Scholar] [CrossRef]
- Potra Cicalău, G.I.; Babeș, P.A.; Domocoș, D.; Pogan, M. The assessment of two-way relationship between periodontal diseases and diabetes mellitus. Acta Stomatol. Mar. 2021, 4, 18–24. [Google Scholar] [CrossRef]
- Liccardo, D.; Cannavo, A.; Spagnuolo, G.; Ferrara, N.; Cittadini, A.; Rengo, C.; Rengo, G. Periodontal disease:A risk factor for diabetes and cardiovascular disease. Int. J. Mol. Sci. 2019, 20, 1414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, C.H.; Yu, C.C.; Lee, S.S.; Yu, H.C.; Huang, F.M.; Chang, Y.C. Upregulation of Slug expression by cyclosporine A contributes to the pathogenesis of gingival overgrowth. J. Med. Assoc. 2016, 115, 602–608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- PubChem. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/Carvacrol#section=Depositor-Supplied-Synonyms (accessed on 20 July 2021).
- Yadav, G.; Kamble, S.B. Synthesis of carvacrol by Friedel–Crafts alkylation of o-cresol with isopropanol using superacidic catalyst UDCaT-5. JCTB 2009, 84, 1499–1508. [Google Scholar] [CrossRef]
- Lu, S.H.; Hsu, W.L.; Chen, T.H.; Chou, T.C. Activation of Nrf2/HO-1signaling pathway involves the anti-inflammatory activity of magnolol in Porphyromonas gingivalis lipopolysaccharide-stimulated mouse RAW 264.7 macrophages. Int. Immunopharmacol. 2015, 29, 770–778. [Google Scholar] [CrossRef]
- Lee, Y.J.; Lee, Y.M.; Lee, C.K.; Jung, J.K.; Han, S.B.; Hong, J.T. Therapeutic applications of compounds in the Magnolia family. Pharm. Ther. 2011, 130, 157–176. [Google Scholar] [CrossRef]
- De Almeida, J.; Ervolino, E.; Bonfietti, L.H.; Novaes, V.C.; Theodoro, L.H.; Fernandes, L.A.; Martins, T.M.; Faleiros, P.L.; Garcia, V.G. Adjuvant therapy with sodium alendronate for the treatment of experimental periodontitis in rats. J. Periodontol. 2015, 86, 1166–1175. [Google Scholar] [CrossRef]
- Ardila, C.M.; López, M.A.; Guzmán, I.C. High resistance against clindamycin, metronidazole and amoxicillin in Porphyromonas gingivalis and Aggregatibacter actinomycetemcomitans isolates of periodontal disease. Med. Oral. Patol. Oral. Cir. Bucal. 2010, 15, e947–e951. [Google Scholar] [CrossRef] [Green Version]
- Anand, B. Herbal therapy in periodontics: A review. J. Res. Pharm. Sci. 2017, 3, 1–7. [Google Scholar]
- Huang, R.Y.; Lu, S.H.; Su, K.W.; Chen, J.K.; Fang, W.H.; Liao, W.N.; Chen, S.Y.; Shieh, Y.S. Diacerein:A potential therapeutic drug for periodontal disease. Med. Hypotheses 2012, 79, 165–167. [Google Scholar] [CrossRef]
- Hosadurga, R.R.; Rao, S.N.; Edavanputhalath, R.; Jose, J.; Rompicharla, N.C.; Shakil, M.; Raju, S. Evaluation of the efficacy of 2% Ocimum sanctum gel in the treatment of experimental periodontitis. Int. J. Pharm. Investig. 2015, 5, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cai, X.; Li, C.; Du, G.; Cao, Z. Protective effects of baicalin on ligature-induced periodontitis in rats. J. Periodontal. Res. 2008, 43, 14–21. [Google Scholar] [CrossRef]
- Tu, H.P.; Fu, M.M.; Kuo, P.J.; Chin, Y.T.; Chiang, C.Y.; Chung, C.L.; Fu, E. Berberine’s effect on periodontal tissue degradation by matrix metalloproteinases:An in vitro and in vivo experiment. Phytomedicine 2013, 20, 1203–1210. [Google Scholar] [CrossRef]
- Sastravaha, G.; Gassmann, G.; Sangtherapitikul, P.; Grimm, W.D. Adjunctive periodontal treatment with Centella asiatica and Punica granatum extracts in supportive periodontal therapy. J. Int. Acad. Periodontol. 2005, 7, 70–79. [Google Scholar]
- Pimentel, S.P.; Barrella, G.E.; Casarin, R.C.; Cirano, F.R.; Casati, M.Z.; Foglio, M.A.; Figueira, G.M.; Ribeiro, F.V. Protective effect of topical Cordia verbenacea in a rat periodontitis model: Immune-inflammatory, antibacterial and morphometric assays. BMC Complement. Altern. Med. 2012, 12, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuo, P.J.; Hung, T.F.; Lin, C.Y.; Hsiao, H.Y.; Fu, M.W.; Hong, P.D.; Chiu, H.C.; Fu, E. Carvacrol ameliorates ligation-induced periodontitis in rats. J. Periodontol. 2017, 88, e120–e128. [Google Scholar] [CrossRef]
- Botelho, M.A.; Martins, J.G.; Ruela, R.S.; Rachid, I.; Santos, J.A.; Soares, J.B.; França, M.C.; Montenegro, D.; Ruela, W.S.; Barros, L.P.; et al. Protective effect of locally applied carvacrol gel on ligature-induced periodontitis in rats: A tapping mode AFM study. Phytother. Res. 2009, 23, 1439–1448. [Google Scholar] [CrossRef]
- Botelho, M.A.; Rao, V.S.; Montenegro, D.; Bandeira, M.A.; Fonseca, S.G.; Nogueira, N.A.; Ribeiro, R.A.; Brito, G.A. Effects of a herbal gel containing carvacrol and chalcones on alveolar bone resorption in rats on experimental periodontitis. Phytother. Res. 2008, 22, 442–449. [Google Scholar] [CrossRef]
- Lu, S.H.; Huang, R.Y.; Chou, T.C. Magnolol ameliorates ligature-induced periodontitis in rats and osteoclastogenesis:In vivo and in vitro study. Evid. Based Complement Altern. Med. 2013, 2013, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, Y.H.; Yu, C.C.; Lee, S.S.; Chang, Y.C. Elevated Snail expression in human gingival fibroblasts by cyclosporine A as the possible pathogenesis for gingival overgrowth. J. Med. Assoc. 2015, 114, 1181–1186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conti, B.; Tabarean, I.; Andrei, C.; Bartfai, T. Cytokines and fever. Front. Biosci. 2004, 9, 1433–1449. [Google Scholar] [CrossRef] [Green Version]
- Cunha, F.Q.; Ferreira, S.H. Peripheral hyperalgesic cytokines. Adv. Exp. Med. Biol. 2003, 521, 22–39. [Google Scholar]
- Hopkins, S.J. The pathophysiological role of cytokines. Leg. Med. 2003, 5, S45–S57. [Google Scholar] [CrossRef]
- Kim, Y.K.; Na, K.S.; Myint, A.M.; Leonard, B.E. The role of pro-inflammatory cytokines in neuroinflammation, neurogenesis and the neuroendocrine system in major depression. Prog. Neuropsychopharmacol. Biol. Psychiatry. 2016, 64, 277–284. [Google Scholar] [CrossRef]
- Kalliolias, G.D.; Ivashkiv, L.B. TNF biology, pathogenic mechanisms and emerging therapeutic strategies. Nat. Rev. Rheumatol. 2016, 12, 49–62. [Google Scholar] [CrossRef] [PubMed]
- Chehimi, M.; Vidal, H.; Eljaafari, A. Pathogenic role of IL-17-producing immune cells in obesity, and related inflammatory diseases. J. Clin. Med. 2017, 6, 68. [Google Scholar] [CrossRef] [Green Version]
- Chen, K.W.; Groß, C.J.; Sotomayor, F.V.; Stacey, K.J.; Tschopp, J.; Sweet, M.J.; Schroder, K. The neutrophil NLRC4 inflammasome selectively promotes IL-1β maturation without pyroptosis during acute Salmonella challenge. Cell. Rep. 2014, 8, 570–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- da Silva Lima, M.; Quintans-Júnior, L.J.; de Santana, W.A.; Martins Kaneto, C.; Pereira Soares, M.B.; Villarreal, C.F. Anti-inflammatory effects of carvacrol:Evidence for a key role of interleukin-10. Eur. J. Pharm. 2013, 699, 112–117. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.H.; Lu, M.H.; Guo, D.S.; Zhai, Y.Y.; Miao, D.; Yue, J.Y.; Yuan, C.H.; Zhao, M.M.; An, D.R. Antifungal effect of magnolol and honokiol from Magnolia officinalis on Alternaria alternata causing tobacco brown spot. Molecules 2019, 24, 2140. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.; Hua, C.; Pan, X.; Fu, X.; Wu, W. Carvacrol exerts neuroprotective effects via suppression of the inflammatory response in middle cerebral artery occlusion rats. Inflammation 2016, 39, 1566–1572. [Google Scholar] [CrossRef] [PubMed]
- Landa, P.; Kokoska, L.; Pribylova, M.; Vanek, T.; Marsik, P. In vitro anti-inflammatory activity of carvacrol: Inhibitory effect on COX-2 catalyzed prostaglandin E 2 biosynthesisb. Arch. Pharm. Res. 2009, 32, 75–78. [Google Scholar] [CrossRef] [PubMed]
- Hotta, M.; Nakata, R.; Katsukawa, M.; Hori, K.; Takahashi, S.; Inoue, H. Carvacrol, a component of thyme oil, activates PPARα and γ and suppresses COX-2 expression [S]. J. Lipid. Res. 2010, 51, 132–139. [Google Scholar] [CrossRef] [Green Version]
- Fachini-Queiroz, F.C.; Kummer, R.; Estevão-Silva, C.F.; Carvalho, M.D.; Cunha, J.M.; Grespan, R.; Bersani-Amado, C.A.; Cuman, R.K. Effects of thymol and carvacrol, constituents of Thymus vulgaris L. essential oil, on the inflammatory response. Evid. Based. Complement. Altern. Med. 2012, 2012, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tabibzadeh Dezfuli, S.A.; Ehsani, M.; Lakzaei Azar, O. Carvacrol Alleivated Negative Effects of Diabetes on Inflammation and Oxidation by Modulation in Gene Expression of Inflammatory and Antioxidant System in Diabetic Rat Model. GMJ Med. 2017, 1, 15–20. [Google Scholar] [CrossRef] [Green Version]
- de Carvalho, F.O.; Silva, É.R.; Gomes, I.A.; Santana, H.S.R.; do Nascimento Santos, D.; de Oliveira Souza, G.P.; de Jesus Silva, D.; Monteiro, J.C.M.; de Albuquerque Júnior, R.L.C.; de Souza Araújo, A.A.; et al. Anti-inflammatory and antioxidant activity of carvacrol in the respiratory system: A systematic review and meta-analysis. Phytother. Res. 2020, 34, 2214–2229. [Google Scholar] [CrossRef]
- Xiao, Y.; Li, B.; Liu, J.; Ma, X. Carvacrol ameliorates inflammatory response in interleukin 1β-stimulated human chondrocytes. Mol. Med. Rep. 2018, 17, 3987–3992. [Google Scholar] [CrossRef] [Green Version]
- Lai, C.S.; Lay, Y.S.; Kuo, D.H.; Wu, C.H.; Ho, C.T.; Pan, M.H. Magnolol potently suppressed lipopolysaccharide-induced iNOS and COX-2 expression via downregulating MAPK and NF-κB signaling pathways. J. Funct. Foods 2011, 3, 198–206. [Google Scholar] [CrossRef]
- Lu, S.H.; Chen, T.H.; Chou, T.C. Magnolol Inhibits RANKL-induced osteoclast differentiation of raw 264.7 macrophages through heme oxygenase-1-dependent inhibition of NFATc1 expression. J. Nat. Prod. 2015, 78, 61–68. [Google Scholar] [CrossRef]
- Lin, M.H.; Chen, M.C.; Chen, T.H.; Chang, H.Y.; Chou, T.C. Magnolol ameliorates lipopolysaccharide-induced acute lung injury in rats through PPAR-γ-dependent inhibition of NF-kB activation. Int. Immunopharmacol. 2015, 28, 270–278. [Google Scholar] [CrossRef]
- Yang, B.; Xu, Y.; Yu, S.; Huang, Y.; Lu, L.; Liang, X. Anti-angiogenic and anti-inflammatory effect of Magnolol in the oxygen-induced retinopathy model. Inflamm. Res. 2016, 65, 81–93. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Jung, E.; Park, J.; Jung, K.; Lee, S.; Hong, S.; Park, J.; Park, E.; Kim, J.; Park, S.; et al. Anti-inflammatory effects of magnolol and honokiol are mediated through inhibition of the downstream pathway of MEKK-1 in NF-κB activation signaling. Planta Med. 2005, 71, 338–343. [Google Scholar] [CrossRef]
- Liang, W.Z.; Lu, C.H. Carvacrol-induced [Ca2+] i rise and apoptosis in human glioblastoma cells. Life Sci. 2012, 90, 703–711. [Google Scholar] [CrossRef] [PubMed]
- Halliwell, B. Free radicals, antioxidants, and human disease:Curiosity, cause, or consequence? Lancet 1994, 344, 721–724. [Google Scholar] [CrossRef]
- Bioclinica. Analize Medicale. Available online: https://bioclinica.ro/pentru-pacienti/informatii-analize/stres-oxidativ (accessed on 20 July 2021).
- Ighodaro, O.M.; Akinloye, O.A. First line defence antioxidants-superoxide dismutase (SOD), catalase (CAT) and glutathione peroxidase (GPX): Their fundamental role in the entire antioxidant defence grid. Alex. J. Med. 2018, 54, 287–293. [Google Scholar] [CrossRef] [Green Version]
- Aeschbach, R.; Löliger, J.; Scott, B.C.; Murcia, A.; Butler, J.; Halliwell, B.; Aruoma, O.I. Antioxidant actions of thymol, carvacrol, 6-gingerol, zingerone and hydroxytyrosol. Food Chem. Toxicol. 1994, 32, 31–36. [Google Scholar] [CrossRef]
- Aydın, E.; Türkez, H.; Keleş, M.S. The effect of carvacrol on healthy neurons and N2a cancer cells:Some biochemical, anticancerogenicity and genotoxicity studies. Cytotechnology 2014, 66, 149–157. [Google Scholar] [CrossRef] [Green Version]
- Hariri, A.T.; Moallem, S.A.; Mahmoudi, M.; Memar, B.; Hosseinzadeh, H. Sub-acute effects of diazinon on biochemical indices and specific biomarkers in rats:Protective effects of crocin and safranal. Food Chem. Toxicol. 2010, 48, 2803–2808. [Google Scholar] [CrossRef]
- Kohen, R.; Nyska, A. Oxidation of biological systems:Oxidative stress phenomena, antioxidants, redox reactions, and methods for their quantification. Toxicol. Pathol. 2002, 30, 620–650. [Google Scholar] [CrossRef] [Green Version]
- Aristatile, B.; Al-Numair, K.S.; Al-Assaf, A.H.; Veeramani, C.; Pugalendi, K.V. Protective effect of carvacrol on oxidative stress and cellular DNA damage induced by UVB irradiation in human peripheral lymphocytes. J. Biochem. Mol. Toxicol. 2015, 29, 497–507. [Google Scholar] [CrossRef]
- Guimarães, A.G.; Oliveira, G.F.; Melo, M.S.; Cavalcanti, S.C.; Antoniolli, A.R.; Bonjardim, L.R.; Silva, F.A.; Santos, J.P.; Rocha, R.F.; Moreira, J.C.; et al. Bioassay-guided evaluation of antioxidant and antinociceptive activities of carvacrol. Basic. Clin. Pharm. Toxicol. 2010, 107, 949–957. [Google Scholar] [CrossRef]
- Chen, H.Y.; Hung, Y.C.; Lee, E.J.; Chen, T.Y.; Chuang, I.C.; Wu, T.S. The protective efficacy of magnolol in hind limb ischemia-reperfusion injury. Phytomedicine 2009, 16, 976–981. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Fang, Q.; Lin, J.; Yuan, Z. Chemistry Study on Protective Effect against· OH-induced DNA Damage and Antioxidant Mechanism of Cortex Magnoliae Officinalis. Bull. Korean Chem. Soc. 2014, 35, 117–122. [Google Scholar] [CrossRef] [Green Version]
- Pang, Y.; Han, X.; Bamikole, M.; Gong, Z.; Tang, S.; Tan, Z.; Xiao, W.; Zhou, C.; Wang, M.; Deng, Y.l. Anti-diarrhea and anti-oxidant properties of Magnolol. Trop. J. Pharm. Res. 2013, 12, 85–91. [Google Scholar] [CrossRef]
- Zhao, X.; Li, F.; Sun, W.; Gao, L.; Kim, K.S.; Kim, K.T.; Cai, L.; Zhang, Z.; Zheng, Y. Extracts of magnolia species-induced prevention of diabetic complications:A brief review. Int. J. Mol. Sci. 2016, 17, 1629. [Google Scholar] [CrossRef] [PubMed]
- Kuo, N.C.; Huang, S.Y.; Yang, C.Y.; Shen, H.H.; Lee, Y.M. Involvement of HO-1 and autophagy in the protective effect of magnolol in hepatic steatosis-induced NLRP3 inflammasome activation in vivo and in vitro. Antioxidants 2020, 9, 924. [Google Scholar] [CrossRef] [PubMed]
- Kashiwagi, Y.; Takedachi, M.; Mori, K.; Kubota, M.; Yamada, S.; Kitamura, M.; Murakami, S. High glucose-induced oxidative stress increases IL-8 production in human gingival epithelial cells. Oral. Dis. 2016, 22, 578–584. [Google Scholar] [CrossRef]
- Liu, C.M.; Chen, S.H.; Liao, Y.W.; Yu, C.H.; Yu, C.C.; Hsieh, P.L. Magnolol ameliorates the accumulation of reactive oxidative stress and inflammation in diabetic periodontitis. J. Med. Assoc. 2021, 120, 1452–1458. [Google Scholar] [CrossRef]
- Ho, K.Y.; Tsai, C.C.; Chen, C.P.; Huang, J.S.; Lin, C.C. Antimicrobial activity of honokiol and magnolol isolated from Magnolia officinalis. Phytother. Res. 2001, 15, 139–141. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, N.; Thornalley, P.J. Advanced glycation endproducts:What is their relevance to diabetic complications? Diabetes. Obes. Metab. 2007, 9, 233–245. [Google Scholar] [CrossRef] [PubMed]
- Ross, J.H.; Hardy, D.C.; Schuyler, C.A.; Slate, E.H.; Mize, T.W.; Huang, Y. Expression of periodontal interleukin-6 protein is increased across patients with neither periodontal disease nor diabetes, patients with periodontal disease alone and patients with both diseases. J. Periodontal. Res. 2010, 45, 688–694. [Google Scholar] [CrossRef] [PubMed]
- Dong, L.; Zhou, S.; Yang, X.; Chen, Q.; He, Y.; Huang, W. Magnolol protects against oxidative stress-mediated neural cell damage by modulating mitochondrial dysfunction and PI3K/Akt signaling. J. Mol. Neurosci. 2013, 50, 469–481. [Google Scholar] [CrossRef] [PubMed]
- La Storia, A.; Ercolini, D.; Marinello, F.; Di Pasqua, R.; Villani, F.; Mauriello, G. Atomic force microscopy analysis shows surface structure changes in carvacrol-treated bacterial cells. Res. Microbiol. 2011, 162, 164–172. [Google Scholar] [CrossRef] [PubMed]
- Helander, I.M.; Alakomi, H.L.; Latva-Kala, K.; Mattila-Sandholm, T.; Pol, I.; Smid, E.J.; Gorris, L.G.M.; von Wright, A. Characterization of the action of selected essential oil components on Gram-negative bacteria. J. Agric. Food. Chem. 1998, 46, 3590–3595. [Google Scholar] [CrossRef]
- Wang, T.H.; Hsia, S.M.; Wu, C.H.; Ko, S.Y.; Chen, M.Y.; Shih, Y.H.; Shieh, T.M.; Chuang, L.C.; Wu, C.Y. Evaluation of the antibacterial potential of liquid and vapor phase phenolic essential oil compounds against oral microorganisms. PLoS ONE 2016, 11, e0163147. [Google Scholar] [CrossRef] [Green Version]
- Maquera-Huacho, P.M.; Tonon, C.C.; Correia, M.F.; Francisconi, R.S.; Bordini, E.A.F.; Marcantonio, É.; Spolidorio, D.M.P. In vitro antibacterial and cytotoxic activities of carvacrol and terpinen-4-ol against biofilm formation on titanium implant surfaces. Biofouling 2018, 34, 699–709. [Google Scholar] [CrossRef] [Green Version]
- Chiu, K.C.; Shih, Y.H.; Wang, T.H.; Lan, W.C.; Li, P.J.; Jhuang, H.S.; Hsia, S.M.; Shen, Y.W.; Yuan-Chien Chen, M.; Shieh, T.M. In vitro antimicrobial and antipro-inflammation potential of honokiol and magnolol against oral pathogens and macrophages. J. Med. Assoc. 2021, 120, 827–837. [Google Scholar] [CrossRef]
- Braun, T.; Zwerina, J. Positive regulators of osteoclastogenesis and bone resorption in rheumatoid arthritis. Arthritis. Res. 2011, 13, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, I.; Jimi, E. Regulation of osteoclast differentiation and function by interleukin-1. Vitam. Horm. 2006, 74, 357–370. [Google Scholar] [CrossRef]
- Jimi, E.; Nakamura, I.; Duong, L.T.; Ikebe, T.; Takahashi, N.; Rodan, G.A.; Suda, T. Interleukin 1 induces multinucleation and bone-resorbing activity of osteoclasts in the absence of osteoblasts/stromal cells. Exp. Cell. Res. 1999, 247, 84–93. [Google Scholar] [CrossRef]
- Lee, Z.H.; Lee, S.E.; Kim, C.W.; Lee, S.H.; Kim, S.W.; Kwack, K.; Walsh, K.; Kim, H.H. IL-1α stimulation of osteoclast survival through the PI 3-kinase/Akt and ERK pathways. J. Biochem. 2002, 131, 161–166. [Google Scholar] [CrossRef]
- Tanaka, S.; Nakamura, K.; Takahasi, N.; Suda, T. Role of RANKL in physiological and pathological bone resorption and therapeutics targeting the RANKL–RANK signaling system. Immunol. Rev. 2005, 208, 30–49. [Google Scholar] [CrossRef]
- Ha, H.; Lee, J.H.; Kim, H.N.; Kim, H.M.; Kwak, H.B.; Lee, S.; Kim, H.H.; Lee, Z.H. α-Lipoic acid inhibits inflammatory bone resorption by suppressing prostaglandin E2 synthesis. J. Immunol. 2006, 176, 111–117. [Google Scholar] [CrossRef] [Green Version]
- Shim, K.S.; Kim, T.; Ha, H.; Lee, C.J.; Lee, B.; Kim, H.S.; Park, J.H.; Ma, J.Y. Water extract of Magnolia officinalis cortex inhibits osteoclastogenesis and bone resorption by downregulation of nuclear factor of activated T cells cytoplasmic 1. Integr. Med. Res. 2015, 4, 102–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hwang, Y.H.; Kim, T.; Kim, R.; Ha, H. Magnolol inhibits osteoclast differentiation via suppression of RANKL expression. Molecules 2018, 23, 1598. [Google Scholar] [CrossRef] [Green Version]
- Bayramoglu, G.; Senturk, H.; Bayramoglu, A.; Uyanoglu, M.; Colak, S.; Ozmen, A.; Kolankaya, D. Carvacrol partially reverses symptoms of diabetes in STZ-induced diabetic rats. Cytotechnology 2014, 66, 251–257. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Mai, Y.; Qiu, X.; Chen, X.; Li, C.; Yuan, W.; Hou, N. Effect of long-term treatment of Carvacrol on glucose metabolism in Streptozotocin-induced diabetic mice. BMC Complement. Med. 2020, 20, 1–8. [Google Scholar] [CrossRef]
- Ezhumalai, M.; Radhiga, T.; Pugalendi, K.V. Antihyperglycemic effect of carvacrol in combination with rosiglitazone in high-fat diet-induced type 2 diabetic C57BL/6J mice. Mol. Cell. Biochem. 2014, 385, 23–31. [Google Scholar] [CrossRef]
- Atanasov, A.G.; Wang, J.N.; Gu, S.P.; Bu, J.; Kramer, M.P.; Baumgartner, L.; Fakhrudin, N.; Ladurner, A.; Malainer, C.; Vuorinen, A.; et al. Honokiol:A non-adipogenic PPARγ agonist from nature. Biochim. Biophys. Acta. 2013, 1830, 4813–4819. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, S.S.; Cha, B.Y.; Lee, Y.S.; Yonezawa, T.; Teruya, T.; Nagai, K.; Woo, J.T. Magnolol enhances adipocyte differentiation and glucose uptake in 3T3-L1 cells. Life Sci. 2009, 84, 908–914. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.J.; Zhao, R.; Liang, J.C.; Chen, Y. The antidiabetic and hepatoprotective effects of magnolol on diabetic rats induced by high-fat diet and streptozotocin. Yao. Xue. Xue. Bao. 2014, 49, 476–481. [Google Scholar]
- Sun, J.; Fu, X.; Liu, Y.; Wang, Y.; Huo, B.; Guo, Y.; Gao, X.; Li, W.; Hu, X. Hypoglycemic effect and mechanism of honokiol on type 2 diabetic mice. Drug. Des. Devel. 2015, 9, 6327. [Google Scholar] [CrossRef] [Green Version]
- Vigan, M. Essential oils:Renewal of interest and toxicity. Eur. J. Derm. 2010, 20, 685–692. [Google Scholar] [CrossRef]
- Burt, S. Essential oils:Their antibacterial properties and potential applications in foods—a review. Int. J. Food. Microbiol. 2004, 94, 223–253. [Google Scholar] [CrossRef] [PubMed]
- Kohlert, C.; Schindler, G.; März, R.W.; Abel, G.; Brinkhaus, B.; Derendorf, H.; Gräfe, E.U.; Veit, M. Systemic availability and pharmacokinetics of thymol in humans. J. Clin. Pharm. 2002, 42, 731–737. [Google Scholar] [CrossRef] [PubMed]
- Undeğer, U.; Başaran, A.; Degen, G.H.; Başaran, N. Antioxidant activities of major thyme ingredients and lack of (oxidative) DNA damage in V79 Chinese hamster lung fibroblast cells at low levels of carvacrol and thymol. Food Chem. Toxicol. 2009, 47, 2037–2043. [Google Scholar] [CrossRef]
- Sharifi-Rad, M.; Varoni, E.M.; Iriti, M.; Martorell, M.; Setzer, W.N.; Del Mar Contreras, M.; Salehi, B.; Soltani-Nejad, A.; Rajabi, S.; Tajbakhsh, M.; et al. Carvacrol and human health: A comprehensive review. Phytother. Res. 2018, 32, 1675–1687. [Google Scholar] [CrossRef]
- LLana-Ruiz-Cabello, M.; Maisanaba, S.; Puerto, M.; Prieto, A.I.; Pichardo, S.; Jos, Á.; Cameán, A.M. Evaluation of the mutagenicity and genotoxic potential of carvacrol and thymol using the Ames Salmonella test and alkaline, Endo III-and FPG-modified comet assays with the human cell line Caco-2. Food Chem. Toxicol. 2014, 72, 122–128. [Google Scholar] [CrossRef]
- Llana-Ruiz-Cabello, M.; Pichardo, S.; Maisanaba, S.; Puerto, M.; Prieto, A.I.; Gutiérrez-Praena, D.; Jos, A.; Cameán, A.M. In vitro toxicological evaluation of essential oils and their main compounds used in active food packaging: A review. Food Chem. Toxicol. 2015, 81, 9–27. [Google Scholar] [CrossRef]
- Maisanaba, S.; Prieto, A.I.; Puerto, M.; Gutiérrez-Praena, D.; Demir, E.; Marcos, R.; Cameán, A.M. In vitro genotoxicity testing of carvacrol and thymol using the micronucleus and mouse lymphoma assays. Mutat. Res. Genet. Toxicol. Environ. Mutagen. 2015, 784, 37–44. [Google Scholar] [CrossRef]
- Saito, J.; Sakai, Y.; Nagase, H. In vitro anti-mutagenic effect of magnolol against direct and indirect mutagens. Mutat. Res. 2006, 609, 68–73. [Google Scholar] [CrossRef]
- Sarrica, A.; Kirika, N.; Romeo, M.; Salmona, M.; Diomede, L. Safety and toxicology of magnolol and honokiol. Planta. Med. 2018, 84, 1151–1164. [Google Scholar] [CrossRef] [Green Version]
- Garrison, R.; Chambliss, W.G. Effect of a proprietary Magnolia and Phellodendron extract on weight management:A pilot, double-blind, placebo-controlled clinical trial. Altern. Health. Med. 2006, 12, 50–55. [Google Scholar]
- Mucci, M.; Carraro, C.; Mancino, P.; Monti, M.; Papadia, L.S.; Volpini, G.; Benvenuti, C. Soy isoflavones, lactobacilli, Magnolia bark extract, vitamin D3 and calcium. Controlled clinical study in menopause. Minerva. Ginecol. 2006, 58, 323–334. [Google Scholar] [PubMed]
- Teschke, R.; Wolff, A.; Frenzel, C.; Schulze, J. Herbal hepatotoxicity–an update on traditional Chinese medicine preparations. Aliment. Pharm. 2014, 40, 32–50. [Google Scholar] [CrossRef] [PubMed]
- Teschke, R.; Zhang, L.; Long, H.; Schwarzenboeck, A.; Schmidt-Taenzer, W.; Genthner, A.; Wolff, A.; Frenzel, C.; Schulze, J.; Eickhoff, A. Traditional Chinese Medicine and herbal hepatotoxicity:A tabular compilation of reported cases. Ann. Hepatol. 2015, 14, 7–19. [Google Scholar] [CrossRef]
- Teschke, R.; Larrey, D.; Melchart, D.; Danan, G. Traditional Chinese medicine (TCM) and herbal hepatotoxicity: RUCAM and the role of novel diagnostic biomarkers such as microRNAs. Medicines 2016, 3, 18. [Google Scholar] [CrossRef] [Green Version]
- COMMISSION DECISION. 1999. Available online: https://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=CONSLEG:1999D0217:20090227:EN:PDF (accessed on 27 October 2021).
- EAFUS: A Food Additive Database.1998. Available online: http://www.usc.es/caa/EdulcWeb/EAFUS.pdf (accessed on 27 October 2021).
- Poivre, M.; Duez, P. Biological activity and toxicity of the Chinese herb Magnolia officinalis Rehder & E. Wilson (Houpo) and its constituents. J. Zhejiang Univ. Sci. B. 2017, 18, 194–214. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Researcher | Study Design | Doses of Treatment | Main Results | References |
|---|---|---|---|---|
| da Silva Lima et al. (2013) | Model: Swiss mice (22–28 g) Disease model: CFA paw edema | Treatment: 50 mg/kg, 100 mg/kg CAR, 40 min before CFA Type of administration: IP | ↓IL-1β ↓PGE2 ⟷ TNF-α local levels ↓COX-2 ↓IL-1β mRNA expression ↑IL-10 ↑IL-10 mRNA expression | [114] |
| Tabibzadeh Dezfuli et al. (2017) | Model: Rats Disease model: STZ induced DM | Treatment: 5 mg/kg, 10 mg/kg, 15 mg/kg BW CAR Type of administration: OG |
↓
IL-1β ↓ IL-6 ↓ TNF-α | [120] |
| de Carvalho et al. (2020) | Model: Animals or humans Disease model: Pulmonary injury | Treatment: Different doses of CAR Type of administration: IP/ diluted in water/ PO/ capsule | ↓IL-1β ↓IL-4 ↓IL-8 ⟷ IL-6 ⟷ TNF-α | [121] |
| Xiao et al. (2018) | Model: Human articular cartilage (8 patients, age 24–41 years), chondrocyte culture Disease model: Articular cartilage with degenerative changes, osteoarthritis Treatment: Various concentrations of CAR (0 µg/mL, 1 µg/mL, 5 µg/mL and 10 µg/mL), for 2 h Type of administration: in vitro | Treatment: Various concentrations of CAR (0 µg/mL, 1 µg/mL, 5 µg/mL and 10 µg/mL), for 2 h Type of administration: in vitro | inhibits IL-1β-induced NO inhibits PGE2 ↓iNOS ↓COX-2 expression suppressed IL-1β-induced MMP-3 and MMP-13 expression inhibits the activation of NF-κB signaling pathway in chondrocytes | [122] |
| Lai et al. (2011) | Model: RAW 264.7 cells, derived from murine macrophages, induced by LPS Disease model: Inflammation | Treatment: 5–15 μM MAG dissolved in DMSO were added together with LPS Type of administration: in vitro |
significantly inhibited LPS stimulated iNOS and COX-2 protein and gene expression | [123] |
| Lu et al. (2015) | Model: RAW 264.7 macrophages Disease model: Inflammation | Treatment: 5–20 μM MAG Type of administration: in vitro | ↓production of pro-inflammatory nitrates ↓PGE2 ↓iNOS ↓COX-2 expression activated NF-κB ↑Nrf2 ↑HO | [124] |
| Lin el al. (2015) | Model: Male Sprague–Dawley rats (200–230 g) Disease model: Acute lung injury | Treatment: 10 mg/kg, 20 mg/kg BW MAG, for 1 h Type of administration: IP | ↓iNOS expression ↓COX-2 expression ↓NF-κB activation ↑PPAR-γ expression | [125] |
| Yang et al. (2016) | Model: Neonatal C57BL/6J mice Disease model: Oxygen-induced retinopathy | Treatment: 25 mg/kg MAG, once a day Type of administration: IP | ↓inflammatory cytokines | [126] |
| Lu et al. (2013) | Model: Male Sprague–Dawley rats (250–350 g) Disease model: Ligature induced periodontitis | Treatment: 100 mg/kg MAG, for 9 days, starting 1 day before ligature Type of administration: OG |
inhibited neutrophil migration in gingival tissue inhibited MPO activity in gingival tissue inhibited COX-2 expression in gingival tissue inhibited iNOS in gingival tissue | [104] |
| Lee et al. (2005) | Model: Human monocyte THP-1 cell line Disease model: Acne | Treatment: 10–15 μM MAG and 10–15 μM honokiol dissolved in 10% DMSO Type of administration: in vitro |
inhibit NF-κB from COX-2, IL-8 and TNF-α promoters ↓ IL-8 ↓ TNF-α ↓ COX-2 | [127] |
| Periodontal Pathogens | CAR | References | |
|---|---|---|---|
| MIC | MBC | ||
| A. actinomycetemcomitans | 200 µg/mL | 200 µg/mL | [151] |
| E. coli | 400 µg/mL | 400 µg/mL | [151] |
| F. nucleatum | 0.002% | 0.002% | [152] |
| MRSA | 400 µg/mL | 600 µg/mL | [151] |
| P. gingivalis | 0.007% | 0.007% | [152] |
| S. mutans | 400 µg/mL | 600 µg/mL | [151] |
| Periodontal Pathogens | MAG | References | |
|---|---|---|---|
| MIC | MBC | ||
| A. actinomycetemcomitans | 10 µg/mL, 25 µg/mL | 20 µg/mL | [145,153] |
| B. subtilis | 25 µg/mL | [145] | |
| E. coli | >100 µg/mL | >100 µg/mL | [153] |
| F. nucleatum | 25 µg/mL | [145] | |
| M. luteus | 25 µg/mL | [145] | |
| MRSA | 10 µg/mL | 30 µg/mL | [153] |
| P. gingivalis | 25 µg/mL | [145] | |
| P. intermedia | 25 µg/mL | [145] | |
| S. mutans | 10 µg/mL | 20 µg/mL | [153] |
| Researcher | Study Design | Doses of Treatment | Main Results | References |
|---|---|---|---|---|
| Bayramoglu et al. (2014) | Animals: Adult Sprague–Dawley rats (195–215 g) Disease model: STZ-induced DM | Treatment: 25 mg/kg, 50 mg/kg BW CAR for 7 days Type of administration: PO | ↓in serum glucose ↓TC ↓AST ↓ALT ↓LDH protection against liver enzymes | [162] |
| Li et al. (2020) | Animals: Adult male C57BL/6 mice (20.0 ± 2.0 g) Disease model: STZ-induced IDDM | Treatment: 10 mg/kg, 20 mg/kg, 40 mg/kg BW CAR, once a day, for 2 weeks Type of administration: IP | ↓plasma glucose levels ↓level of fasting plasma glucose improved glucose tolerance ↓the level of TG ⟷ on the serum level of AST, ALT or ALP no effect on the serum level of AST, ALT, or ALP no effect on the serum level of AST, ALT, or ALP no effect on the serum level of AST, ALT, or ALP no effect on the serum level of AST, ALT, or A ↓LDH plasma levels ↓reduced significantly the activity of hepatic enzymes | [163] |
| Ezhumalai et al. (2014) | Animals: Male C57BL/6J mice (20–30 g) Disease model: NIDDM + HFD | Treatment: 20 mg/kg BW CAR + 4 mg/kg BW RSG, daily, for 35 days Type of administration: IG | antihyperglycemic effects improving carbohydrate metabolism ↓plasma glucose ↓activity of hepatic marker enzymes | [164] |
| Wang et al. (2014) | Animals: Male C57BL/6J mice (20–30 g) Disease model: STZ-induced DM + HFD | Treatment: 25 mg × kg(–1) × d(–1), 50 mg × kg(–1) × d(–1), 100 mg × kg(–1) × d(–1) MAG, for 10 days Type of administration: PO | ↓TC levels ↓TG levels ↓LDL levels ↓hepatic CYP2E1 activity ↓MDA ↑CAT ↑GSH | [167] |
| Sun et al. (2015) | Animals: Male Chinese Kunming mice (18–22 g) Disease model: STZ-induced NIDDM | Treatment: Honokiol 200 mg/kg, once a day, for 8 weeks Type of administration: OG | ↓fasting blood glucose ↓blood glucose levels ameliorates body weight disorder enhances insulin signaling | [168] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cicalău, G.I.P.; Babes, P.A.; Calniceanu, H.; Popa, A.; Ciavoi, G.; Iova, G.M.; Ganea, M.; Scrobotă, I. Anti-Inflammatory and Antioxidant Properties of Carvacrol and Magnolol, in Periodontal Disease and Diabetes Mellitus. Molecules 2021, 26, 6899. https://doi.org/10.3390/molecules26226899
Cicalău GIP, Babes PA, Calniceanu H, Popa A, Ciavoi G, Iova GM, Ganea M, Scrobotă I. Anti-Inflammatory and Antioxidant Properties of Carvacrol and Magnolol, in Periodontal Disease and Diabetes Mellitus. Molecules. 2021; 26(22):6899. https://doi.org/10.3390/molecules26226899
Chicago/Turabian StyleCicalău, Georgiana Ioana Potra, Petru Aurel Babes, Horia Calniceanu, Adelina Popa, Gabriela Ciavoi, Gilda Mihaela Iova, Mariana Ganea, and Ioana Scrobotă. 2021. "Anti-Inflammatory and Antioxidant Properties of Carvacrol and Magnolol, in Periodontal Disease and Diabetes Mellitus" Molecules 26, no. 22: 6899. https://doi.org/10.3390/molecules26226899
APA StyleCicalău, G. I. P., Babes, P. A., Calniceanu, H., Popa, A., Ciavoi, G., Iova, G. M., Ganea, M., & Scrobotă, I. (2021). Anti-Inflammatory and Antioxidant Properties of Carvacrol and Magnolol, in Periodontal Disease and Diabetes Mellitus. Molecules, 26(22), 6899. https://doi.org/10.3390/molecules26226899