
Focus on Pivotal Role of Dietary Intake (Diet and Supplement) and Blood Levels of Tocopherols and Tocotrienols in Obtaining Successful Aging

 ,
,
Abstract
:1. Introduction
2. Methods


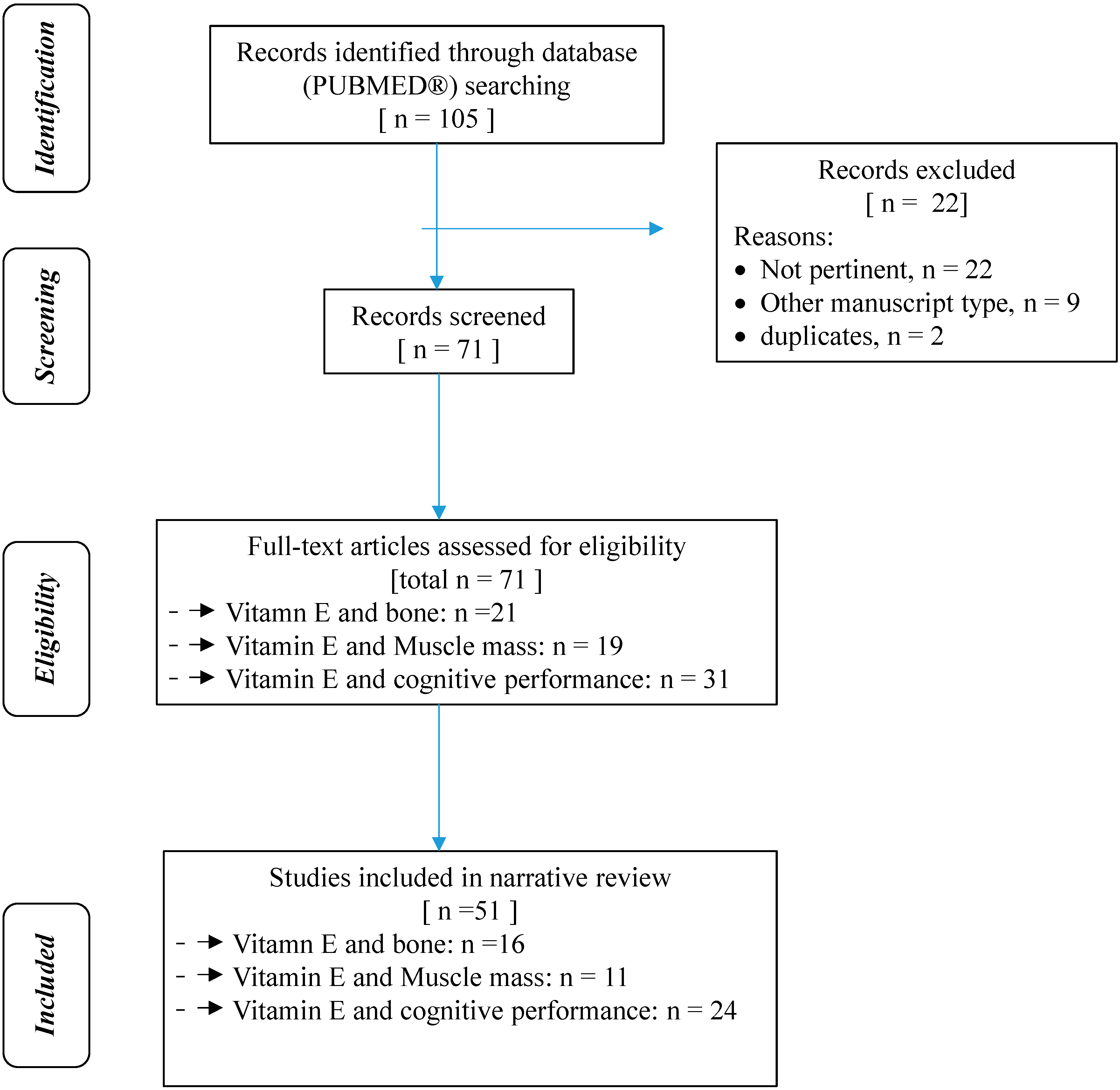{kind=link}
| Step | General Activities | Specific Activities |
|---|---|---|
| Step 1 | configuration of a working group | Three operators skilled in clinical nutrition: one operator acting as a methodological operator two participating as clinical operators |
| Step 2 | formulation of the revision question | Evaluation of the state of the art on metabolic and nutritional correlates (osteoporosis, bone mineral density, sarcopenia, muscle mass, Alzheimerʼs disease, mild cognitive impairment, cognitive performance) of vitamin E deficiency in elderly and their nutritional treatment |
| Step 3 | identification of relevant studies on Pub Med | Suitable for the systematic review were human studies of any design, which considered elderly (over 65 years). In vitro or animals studies are given in the paper only if useful to better explain a result in humans, but are not considered in the tables |
| Step 4 | analysis and presentation of the outcomes | The data extrapolated from the revised studies was carried out in the form of a narrative review of the reports and were collocated in tables |
3. Vitamin E and Bone Health
| Author | Type of Study | Subjects Studied | Primary Endpoint | Main Results of the Study | ||||
|---|---|---|---|---|---|---|---|---|
| Michaëlsson, K., 2014 [37] | Two cohort studies: The Swedish Mammography Cohort (SMC) and the Uppsala Longitudinal Study of Adult Men (ULSAM) | (SMC; n = 61,433 women); (ULSAM; n = 1138 men) | To determine whether α-tocopherol intake or serum concentration are associated with fracture risk in older women and men. | Low intakes and low serum concentrations of α-tocopherol are associated with an increased rate of fracture in elderly women and men. | ||||
| Holvik, K., 2014 [38] | Case-cohort study | 21,774 men and women aged 65–79 years who participated in four community-based health studies in Norway 1994–2001 | To investigate the association between serum α-tocopherol concentrations and risk of hip fracture during up to 11 years of follow-up. | Low serum concentrations of α-tocopherol were associated with increased risk of hip fracture in older Norwegians. | ||||
| D’Adamo, C.R., 2011 [39] | Observational study | 148 women with hip fracture, from the fourth cohort of the Baltimore Hip Studies (BHS4) | To examine how serum α tocopherol and γ-tocopherol concentrations change throughout the year after hip fracture. | Highly cognitively and physically functioning hip fracture patients demonstrated higher vitamin E concentrations. | ||||
| D’Adamo, C.R., 2012 [40] | Observational study | 148 hip fracture patients | To assess whether post-fracture concentration of vitamin E and the carotenoids were associated with lower levels of IL-6 and the soluble receptor of TNF-α. | Higher post-fracture concentrations of vitamin E and the carotenoids were associated with lower levels of inflammatory markers. | ||||
| D’Adamo, C.R., 2011 [41] | Observational study | 148 female hip fracture patients from the Baltimore Hip Studies cohort 4 (BHS4) | To assess the association between serum concentrations of vitamin E with decline in phisical function among older adults. | Serum concentrations of both α- and γ-tocopherol were associated with better physical function after hip fracture. | ||||
| Dietary Supplemtation | ||||||||
| Chuin, A., 2009 [26] | Randomized controlled trial | 34 postmenopausal women randomized in 4 groups (placebo, n = 7; antioxidants, n = 8; exercise and placebo, n = 11; exercise and antioxidants, n = 8) | To evaluate the effects of antioxidants supplementation (α-tocopherol 600 mg/die and vit C 1000 mg/die) combined to resistance training on BMD in healthy elderly women. | Significant decrease in the placebo group for lumbar spine BMD, while it remained stable in all other groups. No changes were observed for femoral neck BMD. | ||||
| Pasco, J.A., 2006 [27] | observational study | 533 community-dwelling non-smoking postmenopausal women (subjects were described as antioxidant supplement users if they were current users of vitamins C and/or E at the time of the assessment) | To assess the association among the use of antioxidant supplements, (vitamins C and E) and serum levels of biochemical markers of bone turnover. | The use of antioxidant supplements was inversely associated with the bone resorption marker C terminal telopeptide in serum, but not with whole body BMD. | ||||
4. Vitamin E and Loss of Muscle Mass and Power
| Author | Type of Study | Subjects Studied | Primary Endpoint | Main Results of the Study |
|---|---|---|---|---|
| Semba 2003 [50] | Cross-sectional analyses | 669 non-disabled to severely disabled community-dwelling women aged 70 to 79 who participated in the Women’s Health and Aging Studies | To assess the association between dietary carotenoids and α-tocopherol with sarcopenia, as indicated by low grip, hip, and knee strength. | Higher carotenoid and α-tocopherol status were independently associated with higher strength measures. |
| Ble 2006 [51] | Epidemiological study | 827 older (65 years) persons (women, 54%) | To evaluate the association between circulating levels of vitamin E and the presence of frailty. | Low plasma levels of Vit. E (α-tocopherol) are associated with frailty syndrome in older persons free from dementia and disability. |
| Bartali 2008 [54] | Longitudinal study | 698 community-living persons (≥65 years) | To determine whether a low serum concentration of micronutrients (Vitamin E, B6, B12, Folic acid, D and Iron) are associated with subsequent decline in physical function among older men and women living in the community. | A low serum concentration of vitamin E is associated with subsequent decline in physical function among community-living older adults. |
| Dietary Supplementation | ||||
| Meydani 1993 [55] | Double-blind study | Nine young (22–29 years) and 12 older (55–74 years) sedentary male subjects | To measure the changes in oxidative products and antioxidants (α-tocopherol and γ-tocopherol) in skeletal muscle of young and old subjects after an eccentric exercise that causes delayed-onset muscle soreness and damage and then compare the antioxidant status of urine and plasma of older vs. younger. | All vitamin E-supplemented subjects excreted less (p < 0.05) urinary thiobarbituric acid adducts after the exercise bout than placebo subjects at 12 days post-exercise. |
| Sacheck 2003 [56] | Randomized clinical trial | Sixteen young (26.4 ± 3.3 years) and 16 older (71.1 ± 4.0 years) healthy men | To investigate the effects of an extended bout of downhill running on oxidative stress response and antioxidant status in healthy young and older men, and whether supplementation with vit, E could negate any observed differences. | Vitamin E supplementation (1000 IU α-tocopherol in soybean oil) induced modest changes eccentric exercise-induced oxidative stress, although differentially between the young and older subjects, while age had no direct influence on these responses among this group of physically fit subjects. |
5. Vitamin E and Cognitive Performance
| Author | Type of Study | Subjects Studied | Primary Endpoint | Main Results of the Study |
|---|---|---|---|---|
| Devore 2010 [59] | prospective cohort study | 5395 participants, aged 55+ years, who were free of dementia | To assess consumption of major dietary antioxidants in relation to long-term risk of dementia. | In multivariate models adjusted for age, education, APOE ε4 genotype, total energy intake, alcohol intake, smoking habits, body-mass index (BMI), and supplement use, higher intake of vitamin E at baseline was associated with a lower long-term risk of dementia (p-trend = 0.02). Higher intake of foods rich in vitamin E may modestly reduce long-term risk of dementia and AD. |
| Mangialasche 2010 [60] | Observational study | A dementia-free sample of 232 subjects aged 80+ years, derived from the Kungsholmen Project, was followed-up to 6 years to detect incident AD | To evaluate the association between plasma levels of eight congeners of vitamin E and incidence of Alzheimer’s disease (AD) among oldest-old individuals in a population-based setting. | The neuroprotective effect of vitamin E seems to be related to the combination of different congeners, rather than to α-tocopherol alone. |
| Morris 2005 [61] | Observational study | 6158 community residents aged ≥65 years. | To assess the food intakes of vitamin E, α-tocopherol equivalents (a measure of the relative biologic activity of tocopherols and tocotrienols), or individual tocopherols protect against incident Alzheimer disease and cognitive decline over 6 y in participants of the Chicago Health and Aging Project. | Various tocopherol congeners rather than α-tocopherol alone may be important in the vitamin E protective association with Alzheimer disease. |
| Bourdel-Marchasson 2001 [62] | Case-control | 20 patients with AD and 23 elderly control subjects living at home and free from disease | To investigate oxidative stress (plasma\erythrocyte malondialdehyde) and enzymatic and non-enzymatic antioxidants (α-tocopherol, retinol, GPx-peroxidase, superoxide dismutase) in normally nourished elderly with AD. | Lower plasma concentrations of α-tocopherol and retinol in normally nourished elderly patients with AD than in controls. |
| Perkins 1999 [63] | Cross-sectional | 4809 non-Hispanic White, non-Hispanic Black, and Mexican-American elderly who visited the Mobile Examination Center during the Third National Health and Nutrition Examination Survey | To evaluate association between serum antioxidant (vitamins E, C, A, carotenoids, selenium) levels and poor memory performance in an elderly, multiethnic sample of the United States. | Decreasing serum levels of vitamin E per unit of cholesterol were consistently associated with increasing levels of poor memory after adjustment for age, education, income, vascular risk factors, and other trace elements and minerals. Serum levels of vitamins A and C, 3-carotene, and selenium were not associated with poor memory performance in this study. |
| Rinaldi 2003 [65] | Case-control | 25 patients with MCI, 63 AD patients and 53 controls | To estimate peripheral levels and activities of Vitamin C, A, E, uric acid, carotenoids including lutein, zeaxanthin, α-cryptoxanthin, lycopene, α- and β-carotene as well as activities of plasma and red blood cell (RBC) superoxide dismutase (SOD) and of plasma glutathione peroxidase (GPx). | MCI patients showed significantly decreased plasma levels of vitamin C, E, A, uric acid, lutein, zeaxanthin, and α- carotene as compared to controls and significant lower activities of plasma and RBC SOD and of plasma GPx. |
| Kang 2008 [72] | Prospective study | 858 female participants of the Nurses’ Health Study, aged 70+ years | To assess the association between plasma antioxidants (carotenoids and tocopherols) and cognition assessed by Telephone Interview for Cognitive Status-TICS (a telephone adaptation of MMSE), East Boston Memory test-EBMT, test of category fluency (name of animals in 1 min), digit span-back words. | In this population of generally well-nourished and healthy aging women, plasma carotenoid and tocopherol levels measured were not associated with their cognitive function or decline ten years later. |
| Schmidt 1998 [73] | Evaluation of cross-sectional data from a cohort study | A total of 1769 subjects aged 50 to 75 years, with no history or signs of neuropsychiatric disease, selected randomly from the community register | To evaluate the association between cognitive status and plasma concentrations of various antioxidants (lutein/zeaxanthin, cryptoxanthin, canthaxanthin, lycopene, alpha-carotene, beta-carotene, retinol, gamma-tocopherol, alpha-tocopherol) in middle-aged and older individuals without neuropsychiatric disease. | Only alpha-tocopherol remained significantly associated with cognitive functioning when logistic regression analysis was used to adjust for possible confounders including age, sex, month of blood sampling, years of education, smoking, lipid status, and major risk factors for stroke. |
| Ravaglia 2008 [74] | Cohort study | 761 elderly Italian subjects from a population based cohort assessed in 1999–2000 for mild cognitive impairment (MCI) and dementia. In 2003–2004, information about cognitive status was collected for 615 of the 666 subjects without baseline cognitive impairment | To investigate plasma concentrations of the natural tocopherols and the tocopherol oxidation markers α-tocopherylquinone (αTQ) and 5-nitro-α-tocopherol (5NGT) in relation to cognitive function in the elderly. | Plasma concentrations of some non-α-tocopherol congeners of vitamin E are associated with cognitive impairment in elderly people. However, the associations depend on concurrent cholesterol concentration and need further investigation. |
| Mangialasche 2012 [75] | Observational study | 168 AD cases, 166 MCI, and 187 cognitively normal (CN) people | To assess the relation of all plasma vitamin E congeners and markers of vitamin E damage (α-tocopherylquinone, 5-nitro-γ-tocopherol) with mild cognitive impairment (MCI) and Alzheimer’s disease (AD). | Both disorders were associated with increased vitamin E damage. Low plasma tocopherols and tocotrienols levels are associated with increased odds of MCI and AD. |
| Mangialasche 2013 [76] | Longitudinal retrospective case-control study | 140 non-cognitively impaired elderly | To investigate the association between serum levels of tocopherols and tocotrienols, markers of vitamin E oxidative/nitrosative damage (α-tocopherylquinone, 5-nitro-γ-tocopherol) and incidence of cognitive impairment. | Elevated levels of tocopherol and tocotrienol congeners are associated with reduced risk of cognitive impairment in older adults. The association is modulated by concurrent cholesterol concentration. |
| Dietary Supplementation | ||||
| Dysken 2014 [77] | Double-blind, placebo-controlled, parallel-group, randomized clinical trial | 613 patients with mild to moderate AD | To determine if supplementation with vitamin E (2000 IU/d of α-tocopherol), memantine (20 mg/die), or both slow progression of mild to moderate AD in patients taking an acetylcholinesterase inhibitor. | Among patients with mild to moderate AD, 2000 IU/d of α-tocopherol compared with placebo resulted in slower functional decline. There were no significant differences in the groups receiving memantine alone or memantine plus α-tocopherol. |
6. Discussion
| Food | mg/100 g | Food | mg/100g |
|---|---|---|---|
| Wheat germ oil | 136.70 | tomato paste | 5.37 |
| sunflower oil | 49.20 | pistachios | 5.21 |
| seed oil corn | 34.50 | sticks and crackers integral | 3.92 |
| extra virgin olive oil | 21.42 | muesli | 3.20 |
| Hazelnut | 24.98 | hen egg, yolk | 3.11 |
| Sweet almond | 23.96 | chickpeas (dry) | 2.61 |
| peanuts (not roasted) | 10.09 | butter | 2.40 |
| Caviar | 7 | chicory | 2.26 |
| Eel river | 5.55 | low-fat milk | 0.04 |
| Vitamin E mg/100 g | Corn Oil | Peanut Oil | Sesame Oil | Sunflower Oil | Walnut Oil | Milk | Milk Cream |
|---|---|---|---|---|---|---|---|
| α-tocopherol | 13 ± 0.3 | 20 ± 1 | 4 ± 0.2 | 46 ± 4 | 8 ± 1 | 0.07 ± 0.01 | 0.5 ± 0.04 |
| β-tocopherol | - | - | - | - | - | - | 0.05 ± 0.004 |
| γ-tocopherol | 87 ± 8 | 15 ± 0.6 | 0.3 ± 0.02 | - | 29 ± 0.3 | - | - |
| γ-tocopherol | - | - | - | - | 5.0 ± 0.6 | - | - |
| α-tocotrienol | - | - | - | - | - | - | - |
| β-tocotrienol | - | - | - | - | - | - | - |
| γ-tocotrienol | - | - | - | - | - | - | - |
| δ-tocotrienol | - | - | 30 ± 7 | - | - | - | - |
| Vitamin E mg/100 g | Badengold | Luteus | Kombo | Macaroni | Rotkorn | Tommi |
|---|---|---|---|---|---|---|
| α-tocopherol | 0.02 ± 0.002 | 0.04 ± 0.003 | 0.07 ± 0.01 | 0.02 ± 0.003 | 0.03 ± 0.01 | 0.05 ± 0.01 |
| β-tocopherol | 0.3 ± 0.02 | - | 0.2 ± 0.01 | 0.06 ± 0.002 | 0.25 ± 0.01 | 0.3 ± 0.1 |
| γ-tocophero | - | - | - | - | - | - |
| δ-tocopherol | - | 0.01 ± 0.001 | - | - | - | - |
| α-tocotrienol | <LOQ | <LOQ | 0.1 ± 0.01 | 0.01 ± 0.003 | <LOQ | 0.03 ± 0.01 |
| β-tocotrienol | 1.7 ± 0.1 | 1.2 ± 0.1 | 2.9 ± 0.01 | 0.9 ± 0.04 | 1.6 ± 0.1 | 2.3 ± 0.3 |
| γ-tocotrienol | 0.01 ± 0.001 | 0.01 ± 0.001 | 0.02 ± 0.001 | - | <LOQ | <LOQ |
| δ-tocotrienol | - | 0.01 ± 0.001 | <LOQ | - | - | <LOQ |
7. Conclusions
Author Contributions
Conflicts of Interest
References
- Marian, M.; Sacks, G. Micronutrients and older adults. Nutr. Clin. Pract. 2009, 24, 179–195. [Google Scholar] [CrossRef] [PubMed]
- Ames, B.N. Low micronutrient intake may accelerate the degenerative dis-eases of aging through allocation of scarce micronutrients by triage. Proc. Natl. Acad. Sci. USA 2006, 103, 17589–17594. [Google Scholar] [CrossRef] [PubMed]
- Maras, J.E.; Bermudez, O.I.; Qiao, N.; Bakun, P.J.; Boody-Alter, E.L.; Tucker, K.L. Intake of alpha-tocopherol is limited among US adults. J. Am. Diet. Assoc. 2004, 104, 567–575. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.; Wilde, P.E.; Lichtenstein, A.H.; Bermudez, O.I.; Tucker, K.L. The maximal amount of dietary alpha-tocopherol intake in U.S. adults (NHANES 2001–2002). J. Nutr. 2006, 136, 1021–1026. [Google Scholar] [PubMed]
- Krebs-Smith, S.M.; Guenther, P.M.; Subar, A.F.; Kirkpatrick, S.I.; Dodd, K.W. Americans do not meet federal dietary recommendations. J. Nutr. 2010, 140, 1832–1838. [Google Scholar] [CrossRef] [PubMed]
- Granado-Lorencio, F.; Blanco-Navarro, I.; Perez-Sacrista, B.; Milla, I.; Donoso-Navarro, E.; Silvestre-Mardomingo, R.A. Determinants of fat-soluble vitamin status in patients aged 65 years and over. Eur. J. Clin. Nutr. 2013, 67, 1325–1327. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Hernandez, J.; Planas Vila, M.; Leon-Sanz, M.; Garcıa de Lorenzo, A.; Celaya-Perez, S.; Garcıa-Lorda, P.; Araujo, K.; Sarto Guerri, B. Prevalence and costs of malnutrition in hospitalized patients; the PREDyCESs Study. Nutr. Hosp. 2012, 27, 1049–1059. [Google Scholar] [PubMed]
- Fisberg, R.M.; Marchioni, D.M.; Castro, M.A.; Verly, E., Jr.; Araújo, M.C.; Bezerra, I.N.; Pereira, R.A.; Sichieri, R. Inadequate nutrient intake among the Brazilian elderly: National Dietary Survey 2008–2009. Rev. Saude Publica 2013, 47, 222S–230S. [Google Scholar] [CrossRef] [PubMed]
- Anlasik, T.; Sies, H.; Griffiths, H.R.; Mecocci, P.; Stahl, W.; Polidori, M.C. Dietary habits are major determinants of the plasma antioxidant status in healthy elderly subjects. Br. J. Nutr. 2005, 94, 639–642. [Google Scholar] [CrossRef] [PubMed]
- Food and Nutrition Board. Dietary Reference Intakes for Vitamin C, Vitamin E, Selenium, and Carotenoids; National Academies Press: Washington, DC, USA, 2000. [Google Scholar]
- Martin, A.; Youdim, K.; Szprengiel, A.; Shukitt-Hale, B.; Joseph, J. Roles of vitamins E and C on neurodegenerative diseases and cognitive performance. Nutr. Rev. 2002, 60, 308–326. [Google Scholar] [CrossRef] [PubMed]
- McCullough, M.L.; Feskanich, D.; Stampfer, M.J.; Giovannucci, E.L.; Rimm, E.B.; Hu, F.B.; Spiegelman, D.; Hunter, D.J.; Colditz, G.A.; Willett, W.C. Diet quality and major chronic disease risk in men and women: Moving toward improved dietary guidance. Am. J. Clin. Nutr. 2002, 76, 1261–1271. [Google Scholar] [PubMed]
- Mayer-Davis, E.J.; Costacou, T.; King, I.; Zaccaro, D.J.; Bell, R.A. Plasma and dietary vitamin E in relation to incidence of type 2 diabetes: The Insulin Resistance and Atherosclerosis Study (IRAS). Diabetes Care 2002, 25, 2172–2177. [Google Scholar] [CrossRef] [PubMed]
- Kuwabara, A.; Nakade, M.; Tamai, H.; Tsuboyama-Kasaoka, N.; Tanaka, K. The association between vitamin E intake and hypertension: Results from the re-analysis of the National Health and Nutrition Survey. J. Nutr. Sci. Vitaminol. 2014, 60, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Mecocci, P.; Polidori, M.C.; Troiano, L.; Cherubini, A.; Cecchetti, R.; Pini, G.; Straatman, M.; Monti, D.; Stahl, W.; Sies, H.; et al. Plasma antioxi-dants and longevity: A study on healthy centenarians. Free Radic. Biol. Med. 2000, 28, 1243–1248. [Google Scholar] [CrossRef]
- Poljsak, B.; Milisav, I. The neglected significance of “antioxidative stress”. Oxid. Med. Cell Longev. 2012, 480895–480907. [Google Scholar] [CrossRef] [PubMed]
- Liochev, S.I. Reactive oxygen species and the free radical theory of aging. Free Radic Biol. Med. 2013, 60, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Burton, G.W.; Cheeseman, K.H.; Doba, T.; Ingold, K.U.; Slater, T.F. Vitamin E asan antioxidant in vitro and in vivo. Ciba Found Symp. 1983, 101, 4–18. [Google Scholar] [PubMed]
- Palace, V.P.; Hill, M.F.; Farahmand, F.; Singal, P.K. Mobilization of antioxidantvitamin pools and hemodynamic function after myocardial infarction. Circulation 1999, 99, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Palace, V.; Kumar, D.; Hill, M.F.; Khaper, N.; Singal, P.K. Regional differencesin non-enzymatic antioxidants in the heart under control and oxidative stressconditions. J. Mol. Cell. Cardiol. 1999, 31, 193–202. [Google Scholar] [CrossRef] [PubMed]
- Burton, G.W.; Cheng, S.C.; Webb, A.; Ingold, K.U. Vitamin E in young and oldhuman red blood cells. Biochem. Biophys. Acta 1986, 860, 84–90. [Google Scholar] [CrossRef]
- Pae, M.; Meydani, S.N.; Wu, D. The role of nutrition in enhancing immunity inaging. Aging Dis. 2012, 3, 91–129. [Google Scholar] [PubMed]
- Claycombe, K.J.; Meydani, S.N. Vitamin E and genome stability. Mutat. Res. 2001, 475, 37–44. [Google Scholar] [CrossRef]
- Azzi, A.; Gysin, R.; Kempná, P.; Munteanu, A.; Negis, Y.; Villacorta, L.; Visarius, T.; Zingg, J.M. Vitamin E mediates cell signaling and regulation of gene expression. Ann. N. Y. Acad. Sci. 2004, 1031, 86–95. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Smith, G.D.; Altman, D.G. Systematic Reviews in Health Care: Meta-Analysis in Context, 2nd ed.; BMJ Publishing Group: London, UK, 2001; pp. 3–68. [Google Scholar]
- Chuin, A.; Labonté, M.; Tessier, D.; Khalil, A.; Bobeuf, F.; Doyon, C.Y.; Rieth, N.; Dionne, I.J. Effect of antioxidants combined to resistance training on BMD in elderly women: A pilot study. Osteoporos. Int. 2009, 20, 1253–1258. [Google Scholar] [CrossRef] [PubMed]
- Pasco, J.A.; Henry, M.J.; Wilkinson, L.K.; Nicholson, G.C.; Schneider, H.G.; Kotowicz, M.A. Antioxidant vitamin supplements and markers of bone turnover in a community sample of non-smoking women. J. Womens Health 2006, 15, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Manolagas, S.C.; Parfitt, A.M. What old means to bone. Trends Endocrinol. Metab. 2010, 21, 369–374. [Google Scholar] [CrossRef] [PubMed]
- Cerullo, F.; Gambassi, G.; Cesari, M. Rationale for antioxidant supplementation in sarcopenia. J. Aging Res. 2012, 2012, 316943. [Google Scholar] [CrossRef] [PubMed]
- Meng, S.J.; Yu, L.J. Oxidative stress, molecular inflammation and sarcopenia. Int. J. Mol. Sci 2010, 11, 1509–1526. [Google Scholar] [CrossRef] [PubMed]
- Marshall, D.; Johnell, O.; Wedel, H. Meta-analysis of how well measures of bone mineral density predict occurrence of osteoporotic fractures. BMJ 1996, 312, 1254–1259. [Google Scholar] [CrossRef] [PubMed]
- Jarvinen, T.L.; Sievanen, H.; Khan, K.M.; Heinonen, A.; Kannus, P. Shifting the focus in fracture prevention from osteoporosis to falls. BMJ 2008, 336, 124–126. [Google Scholar] [CrossRef] [PubMed]
- Fiatarone, M.A.; Singh, N.A.; Hansen, R.D.; Finnegan, T.P.; Allen, B.J.; Diamond, T.H.; Diwan, A.D.; Lloyd, B.D.; Williamson, D.A.; Smith, E.U.; et al. Methodology and baseline characteristics for the Sarcopenia and Hip Fracture study: A 5-year prospective study. J. Gerontol. A Biol. Sci. Med. Sci. 2009, 64, 568–574. [Google Scholar] [CrossRef] [PubMed]
- Shuid, A.N.; Mohamad, S.; Muhammad, N.; Fadzilah, F.M.; Mokhtar, S.A.; Mohamed, N.; Soelaiman, I.N. Effects of alpha-tocopherol on the early phase of osteoporotic fracture healing. J. Orthop. Res. 2011, 29, 1732–1738. [Google Scholar] [CrossRef] [PubMed]
- Mehat, M.Z.; Shuid, A.N.; Mohamed, N.; Muhammad, N.; Soelaiman, I.N. Beneficial effects of vitamin E isomer supplementation on static and dynamic bone histomorphometry parameters in normal male rats. J. Bone Miner Metab. 2010, 28, 503–509. [Google Scholar] [CrossRef] [PubMed]
- Nieves, J.W. Skeletal effects of nutrients and nutraceuticals, beyond calcium and vitamin D. Osteoporos. Int. 2013, 24, 771–786. [Google Scholar] [CrossRef] [PubMed]
- Michaëlsson, K.; Wolk, A.; Byberg, L.; Ärnlöv, J.; Melhus, H. Intake and serum concentrations of α-tocopherol in relation to fractures in elderly women and men: 2 cohort studies. Am. J. Clin. Nutr. 2014, 99, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Holvik, K.; Gjesdal, C.G.; Tell, G.S.; Grimnes, G.; Schei, B.; Apalset, E.M.; Samuelsen, S.O.; Blomhoff, R.; Michaëlsson, K.; Meyer, H.E. Low serum concentrations of alpha-tocopherol are associated with increased risk of hip fracture. A NOREPOS study. Osteoporos. Int. 2014, 25, 2545–2554. [Google Scholar] [CrossRef] [PubMed]
- D’Adamo, C.R.; Shardell, M.D.; Hicks, G.E.; Orwig, D.L.; Hochberg, M.C.; Semba, R.D.; Yu-Yahiro, J.A.; Ferrucci, L.; Magaziner, J.S.; Miller, R.R. Serum vitamin E concentrations among highly functioning hip fracture patients are higher than in nonfracture controls. Nutr. Res. 2011, 31, 205–214. [Google Scholar] [CrossRef] [PubMed]
- D’Adamo, C.R.; Miller, R.R.; Shardell, M.D.; Orwig, D.L.; Hochberg, M.C.; Ferrucci, L.; Semba, R.D.; Yu-Yahiro, J.A.; Magaziner, J.; Hicks, G.E. Higher serum concentrations of dietary antioxidants are associated with lower levels of inflammatory biomarkers during the year after hip fracture. Clin. Nutr. 2012, 31, 659–665. [Google Scholar] [CrossRef] [PubMed]
- D’Adamo, C.R.; Miller, R.R.; Hicks, G.E.; Orwig, D.L.; Hochberg, M.C.; Semba, R.D.; Yu-Yahiro, J.A.; Ferrucci, L.; Magaziner, J.; Shardell, M.D. Serum vitamin E concentrations and recovery of physical function during the year after hip fracture. J. Gerontol. A Biol. Sci. Med. Sci. 2011, 66, 784–793. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European working group on Sarcopenia in older people. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [PubMed]
- Van Kan, G.A. Epidemiology 16 and consequences of sarcopenia. J. Nutr. Health Aging 2009, 13, 708–712. [Google Scholar] [CrossRef]
- International Osteoporosis Foundation. Available online: http://www.iofbonehealth.org (accessed on 25 September 2015).
- Schwartz, R.S.; Weindruch, C.; Weindruch, R. Interventions based on the possibility that oxidative stress contributes to sarcopenia. J. Gerontol. A Biol. Sci. Med. Sci. 1995, 50, 157–161. [Google Scholar] [CrossRef]
- McKenzie, D.; Bua, E.; McKiernan, S.; Cao, Z.; Wanagat, J.; Aiken, J.M. Mitochondrial DNA deletion mutations: A causal role in sarcopenia. Eur. J. Biochem. 2002, 269, 2010–2015. [Google Scholar] [CrossRef] [PubMed]
- Carmeli, E.; Coleman, R.; Reznick, A.Z. The biochemistry of aging muscle. Exp. Gerontol. 2002, 37, 477–489. [Google Scholar] [CrossRef]
- Morley, J.E.; Baumgartner, R.N. Cytokine-related aging process. J. Gerontol. A Biol. Sci. Med. Sci. 2004, 59, M924–M929. [Google Scholar] [CrossRef] [PubMed]
- Schaap, L.A.; Pluijm, S.M.F.; Deeg, D.J.H.; Visser, M. Inflammatory markers and loss of muscle mass (sarcopenia) and strength. Am. J. Med. 2006, 119, 526.e9–526.e17. [Google Scholar] [CrossRef] [PubMed]
- Semba, R.D.; Blaum, C.; Guralnik, J.M.; Moncrief, D.T.; Ricks, M.O.; Fried, L.P. Carotenoid and vitamin E status are associated with indicators of sarcopenia among older women living in the community. Aging Clin. Exp. Res. 2003, 15, 482–487. [Google Scholar] [CrossRef] [PubMed]
- Ble, A.; Cherubini, A.; Volpato, S.; Bartali, B.; Walston, J.D.; Windham, B.G.; Bandinelli, S.; Lauretani, F.; Guralnik, J.M.; Ferrucci, L. Lower plasma vitamin E levels are associated with the frailty syndrome: The InCHIANTI study. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 61, 278–283. [Google Scholar] [CrossRef] [PubMed]
- Pette, D.; Spamer, C. Metabolic properties of muscle fibers. Fed. Proc. 1986, 45, 2910–2914. [Google Scholar] [PubMed]
- Evans, W.J. Vitamin E, vitamin C, and exercise. Am. J. Clin. Nutr. 2000, 72, 647S–652S. [Google Scholar] [PubMed]
- Bartali, B.; Frongillo, E.A.; Guralnik, J.M.; Stipanuk, M.H.; Allore, H.G.; Cherubini, A.; Bandinelli, S.; Ferrucci, L.; Gill, T.M. Serum micronutrient concentrations and decline in physical function among older persons. JAMA 2008, 299, 308–315. [Google Scholar] [CrossRef] [PubMed]
- Meydani, M.; Evans, W.J.; Handelman, G.; Biddle, L.; Fielding, R.A.; Meydani, S.N.; Burrill, J.; Fiatarone, M.A.; Blumberg, J.B.; Cannon, J.G. Protective effect of vitamin E on exercise-induced oxidative damage in young and older adults. Am. J. Physiol. Regul. Integr. Comp. Physiol. 1993, 264, R992–R998. [Google Scholar]
- Sacheck, J.M.; Milbury, P.E.; Cannon, J.G.; Roubenoff, R.; Blumberg, J.B. Effect of vitamin E and eccentric exercise on selected biomarkers of oxidative stress in young and elderly men. Free Radic. Biol. Med. 2003, 34, 1575–1588. [Google Scholar] [CrossRef]
- Devi, S.A.; Prathim, S.; Subramanyam, M.V.V. Dietary vitamin E and physical exercise: I. Altered endurance capacity and plasma lipid profile in ageing rats. Exp. Gerontol. 2003, 38, 285–290. [Google Scholar] [CrossRef]
- Lee, S.P.; Mar, G.Y.; Ng, L.T. Effects of tocotrienol-rich fraction on exercise endurance capacity and oxidative stress in forced swimming rats. Eur. J. Appl. Physiol. 2009, 107, 587–595. [Google Scholar] [CrossRef] [PubMed]
- Devore, E.E.; Grodstein, F.; van Rooij, F.J.; Hofman, A.; Stampfer, M.J.; Witteman, J.C.; Breteler, M.M. Dietary antioxidants and longterm risk of dementia. Arch. Neurol. 2010, 67, 819–825. [Google Scholar] [CrossRef] [PubMed]
- Mangialasche, F.; Kivipelto, M.; Mecocci, P.; Rizzuto, D.; Palmer, K.; Winblad, B.; Fratiglioni, L. High plasma levels of vitamin E forms and reduced Alzheimer’s disease risk in advanced age. J. Alzheimers Dis. 2010, 20, 1029–1037. [Google Scholar] [PubMed]
- Morris, M.C.; Evans, D.A.; Tangney, C.C.; Bienias, J.L.; Wilson, R.S.; Aggarwal, N.T.; Scherr, P.A. Relation of the tocopherol forms to incident Alzheimer disease and to cognitive change. Am. J. Clin. Nutr. 2005, 81, 508–514. [Google Scholar] [PubMed]
- Bourdel-Marchasson, I.; Delmas-Beauvieux, M.C.; Peuchant, E.; Richard-Harston, S.; Decamps, A.; Reignier, B.; Emeriau, J.P.; Rainfray, M. Antioxidant defences and oxidative stress markers in erythrocytes and plasma from normally nourished elderly Alzheimer patients. Age Ageing 2001, 30, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Perkins, A.J.; Hendrie, H.C.; Callahan, C.M.; Gao, S.; Unverzagt, F.W.; Xu, Y.; Hall, K.S.; Hui, S.L. Association of antioxidants with memory in a multiethnic elderly sample using the Third National Health and Nutrition Examination Survey. Am. J. Epidemiol. 1999, 150, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Praticò, D.; Sung, S. Lipid peroxidation and oxidative imbalance: Early functional events in Alzheimer’s disease. J. Alzheimers Dis. 2004, 6, 171–175. [Google Scholar] [PubMed]
- Rinaldi, P.; Polidori, M.C.; Metastasio, A.; Mariani, E.; Mattioli, P.; Cherubini, A.; Catani, M.; Cecchetti, R.; Senin, U.; Mecocci, P. Plasma antioxidants are similarly depleted in mild cognitive impairment and in Alzheimer’s disease. Neurobiol. Aging 2003, 24, 915–919. [Google Scholar] [CrossRef]
- Parks, E.; Traber, M.G. Mechanisms of vitamin E regulation: Research over the past decade and focus on the future. Antioxid. Redox Signal. 2000, 2, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Muller, D.P.; Goss-Sampson, M.A. Neurochemical, neurophysiological, and neuropathological studies in vitamin E deficiency. Crit. Rev. Neurobiol. 1990, 5, 239–263. [Google Scholar] [PubMed]
- Mangialasche, F.; Polidori, M.C.; Monastero, R.; Ercolani, S.; Camarda, C.; Cecchetti, R.; Mecocci, P. Biomarkers of oxidative and nitrosative damage in Alzheimer’s disease and mild cognitive impairment. Ageing Res. Rev. 2009, 8, 285–305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reddy, P.H. Mitochondrial dysfunction in aging and Alzheimer’s disease: Strategies to protect neurons. Antioxid. Redox Signal. 2007, 9, 1647–1658. [Google Scholar] [CrossRef] [PubMed]
- Ricciarelli, R.; Argellati, F.; Pronzato, M.A.; Domenicotti, C. Vitamin E and neurodegenerative diseases. Mol. Asp. Med. 2007, 28, 591–606. [Google Scholar] [CrossRef] [PubMed]
- Sen, C.K.; Khanna, S.; Rink, C.; Roy, S. Tocotrienols: The emerging face of natural vitamin E. Vitam. Horm. 2007, 76, 203–261. [Google Scholar] [PubMed]
- Kang, J.H.; Grodstein, F. Plasma carotenoids and tocopherols and cognitive function: A prospective study. Neurobiol. Aging 2008, 29, 1394–1403. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, R.; Hayn, M.; Reinhart, B.; Roob, G.; Schmidt, H.; Schumacher, M.; Watzinger, N.; Launer, L.J. Plasma antioxidants and cognitive performance in middle-aged and older adults: Results of the Austrian Stroke Prevention Study. J. Am. Geriatr. Soc. 1998, 46, 1407–1410. [Google Scholar] [CrossRef] [PubMed]
- Ravaglia, G.; Forti, P.; Lucicesare, A.; Pisacane, N.; Rietti, E.; Mangialasche, F.; Cecchetti, R.; Patterson, C.; Mecocci, P. Plasma tocopherols and risk of cognitive impairment in an elderly Italian cohort. Am. J. Clin. Nutr. 2008, 87, 1306–1313. [Google Scholar] [PubMed]
- Mangialasche, F.; Xu, W.; Kivipelto, M.; Costanzi, E.; Ercolani, S.; Pigliautile, M.; Cecchetti, R.; Baglioni, M.; Simmons, A.; Soininen, H.; et al. Tocopherols and tocotrienols plasma levels are associated with cognitive impairment. Neurobiol. Aging 2012, 33, 2282–2290. [Google Scholar] [CrossRef] [PubMed]
- Mangialasche, F.; Solomon, A.; Kåreholt, I.; Hooshmand, B.; Cecchetti, R.; Fratiglioni, L.; Soininen, H.; Laatikainen, T.; Mecocci, P.; Kivipelto, M. Serum levels of vitamin E forms and risk of cognitive impairment in a Finnish cohort of older adults. Exp. Gerontol. 2013, 48, 1428–1435. [Google Scholar] [CrossRef] [PubMed]
- Dysken, M.W.; Sano, M.; Asthana, S.; Vertrees, J.E.; Pallaki, M.; Llorente, M.; Love, S.; Schellenberg, G.D.; McCarten, J.R.; Malphurs, J.; et al. Effect of vitamin E and memantine on functional decline in Alzheimer disease. JAMA 2014, 311, 33–44. [Google Scholar] [CrossRef] [PubMed]
- Mocchegiani, E.; Costarelli, L.; Giacconi, R.; Malavolta, M.; Basso, A.; Piacenza, F.; Ostan, R.; Cevenini, E.; Gonos, E.S.; Franceschi, C.; et al. Vitamin E-gene interactions in aging and inflammatory age-related diseases: Implications for treatment. A systematic review. Ageing Res. Rev. 2014, 14, 81–101. [Google Scholar] [CrossRef] [PubMed]
- Schürks, M.; Glynn, R.J.; Rist, P.M.; Tzourio, C.; Kurth, T. Effects of vitamin E on stroke subtypes: Meta-analysis of randomised controlled trials. BMJ 2010, 341, c5702. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.Y.; Appel, L.J. Supplementation of diets with alpha-tocopherol reduces serum concentrations of gamma- and delta-tocopherol in humans. J. Nutr. 2003, 133, 3137–3140. [Google Scholar] [PubMed]
- Khanna, S.; Patel, V.; Rink, C.; Roy, S.; Sen, C.K. Delivery of orally supplemented alpha-tocotrienol to vital organs of rats and tocopherol-transport protein deficient mice. Free Radic. Biol. Med. 2005, 39, 1310–1319. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.C.; Kanekiyo, T.; Xu, H.; Bu, G. Apolipoprotein E and Alzheimer disease: Risk, mechanisms and therapy. Nat. Rev. Neurol. 2013, 9, 106–118. [Google Scholar] [CrossRef] [PubMed]
- Karmowski, J.; Hintze, V.; Kschonsek, J.; Killenberg, M.; Böhm, V. Antioxidant activities of tocopherols/tocotrienols and lipophilic antioxidant capacity of wheat, vegetable oils, milk and milk cream by using photochemiluminescence. Food Chem. 2015, 175, 593–600. [Google Scholar] [CrossRef] [PubMed]
- Shammugasamy, B.; Ramakrishnan, Y.; Ghazali, H.M.; Muhammad, K. Tocopherol and tocotrienol contents of different varieties of rice in Malaysia. J. Sci. Food Agric. 2015, 95, 672–678. [Google Scholar] [CrossRef] [PubMed]
- Vivekananthan, D.P.; Penn, M.S.; Sapp, S.K.; Hsu, A.; Topol, E.J. Use of antioxidant vitamins for the prevention of cardiovascular disease: Meta-analysis of randomised trials. Lancet 2003, 361, 2017–2023. [Google Scholar] [CrossRef]
- Bjelakovic, G.; Nikolova, D.; Simonetti, R.G.; Gluud, C. Antioxidant supplements for prevention of gastrointestinal cancers: A systematic review and meta-analysis. Lancet 2004, 364, 1219–1228. [Google Scholar] [CrossRef]
- Miller, E.R.; Pastor-Barriuso, R.; Dalal, D.; Riemersma, R.A.; Appel, L.J.; Guallar, E. Meta-analysis: High-dosage vitamin E supplementation may increase all-cause mortality. Ann. Intern. Med. 2005, 142, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Shekelle, P.G.; Morton, S.C.; Jungvig, L.K.; Udani, J.; Spar, M.; Tu, W.; Suttorp, M.; Coulter, I.; Newberry, S.J.; Hardy, M. Effect of supplemental vitamin E for the prevention and treatment of cardiovascular disease. J. Gen. Intern. Med. 2004, 19, 380–389. [Google Scholar] [CrossRef] [PubMed]
- Bjelakovic, G.; Nikolova, D.; Gluud, L.L.; Simonetti, R.G.; Gluud, C. Antioxidant supplements for prevention of mortality in healthy participants and patients with various diseases. Cochrane Database Syst. Rev. 2012, 14, CD007176. [Google Scholar]
- Roberts, H.J. Perspective on vitamin E as therapy. JAMA 1981, 246, 129–131. [Google Scholar] [CrossRef] [PubMed]
- Berry, D.; Wathen, J.K.; Newell, M. Bayesian model averaging in meta-analysis: Vitamin E supplementation and mortality. Clin. Trials 2009, 6, 28–41. [Google Scholar] [CrossRef] [PubMed]
- Biesalski, H.K.; Grune, T.; Tinz, J.; Zöllner, I.; Blumberg, J.B. Reexamination of a meta-analysis of the effect of antioxidant supplementation on mortality and health in randomized trials. Nutrients 2010, 2, 929–949. [Google Scholar] [CrossRef] [PubMed]
- Banca Dati Di Composizione Degli Alimenti per Studi Epidemiologici in Italia. Available online: http://www.bda-ieo.it (accessed on 25 September 2015).
- Yoshida, Y.; Niki, E.; Noguchi, N. Comparative study on the action of tocopherols and tocotrienols as antioxidant: Chemical and physical effects. Chem. Phys. Lipids 2003, 123, 63–75. [Google Scholar] [CrossRef]
- Aggarwal, B.B.; Sundaram, C.; Prasad, S.; Kannappan, R. Tocotrienols, the vitamin E of the 21st century: Its potential against cancer and other chronic diseases. Biochem. Pharmacol. 2010, 80, 1613–1631. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Q.; Christen, S.; Shigenaga, M.K.; Ames, B.N. gamma-tocopherol, the major form of vitamin E in the US diet, deserves more attention. Am. J. Clin. Nutr. 2001, 74, 714–722. [Google Scholar] [PubMed]
- Brigelius-Flohé, R.; Kelly, F.J.; Salonen, J.T.; Neuzil, J.; Zingg, J.M.; Azzi, A. The European perspective on vitamin E: Current knowledge and future research. Am. J. Clin. Nutr. 2002, 76, 703–716. [Google Scholar] [PubMed]
- Wu, D.; Meydani, S.N. Age-associated changes in immune and inflammatory responses: Impact of vitamin E intervention. J. Leukoc. Biol. 2008, 84, 900–914. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rondanelli, M.; Faliva, M.A.; Peroni, G.; Moncaglieri, F.; Infantino, V.; Naso, M.; Perna, S. Focus on Pivotal Role of Dietary Intake (Diet and Supplement) and Blood Levels of Tocopherols and Tocotrienols in Obtaining Successful Aging. Int. J. Mol. Sci. 2015, 16, 23227-23249. https://doi.org/10.3390/ijms161023227
Rondanelli M, Faliva MA, Peroni G, Moncaglieri F, Infantino V, Naso M, Perna S. Focus on Pivotal Role of Dietary Intake (Diet and Supplement) and Blood Levels of Tocopherols and Tocotrienols in Obtaining Successful Aging. International Journal of Molecular Sciences. 2015; 16(10):23227-23249. https://doi.org/10.3390/ijms161023227
Chicago/Turabian StyleRondanelli, Mariangela, Milena Anna Faliva, Gabriella Peroni, Francesca Moncaglieri, Vittoria Infantino, Maurizio Naso, and Simone Perna. 2015. "Focus on Pivotal Role of Dietary Intake (Diet and Supplement) and Blood Levels of Tocopherols and Tocotrienols in Obtaining Successful Aging" International Journal of Molecular Sciences 16, no. 10: 23227-23249. https://doi.org/10.3390/ijms161023227
APA StyleRondanelli, M., Faliva, M. A., Peroni, G., Moncaglieri, F., Infantino, V., Naso, M., & Perna, S. (2015). Focus on Pivotal Role of Dietary Intake (Diet and Supplement) and Blood Levels of Tocopherols and Tocotrienols in Obtaining Successful Aging. International Journal of Molecular Sciences, 16(10), 23227-23249. https://doi.org/10.3390/ijms161023227