
NAFLD and Chronic Kidney Disease

Abstract
:1. Introduction
2. Diagnosis and Screening
2.1. Imaging
2.2. Liver Enzymes and Biomarkers
3. Epidemiologic Evidence Linking Chronic Kidney Disease (CKD) to Non-Alcoholic Fatty Liver Disease (NAFLD)
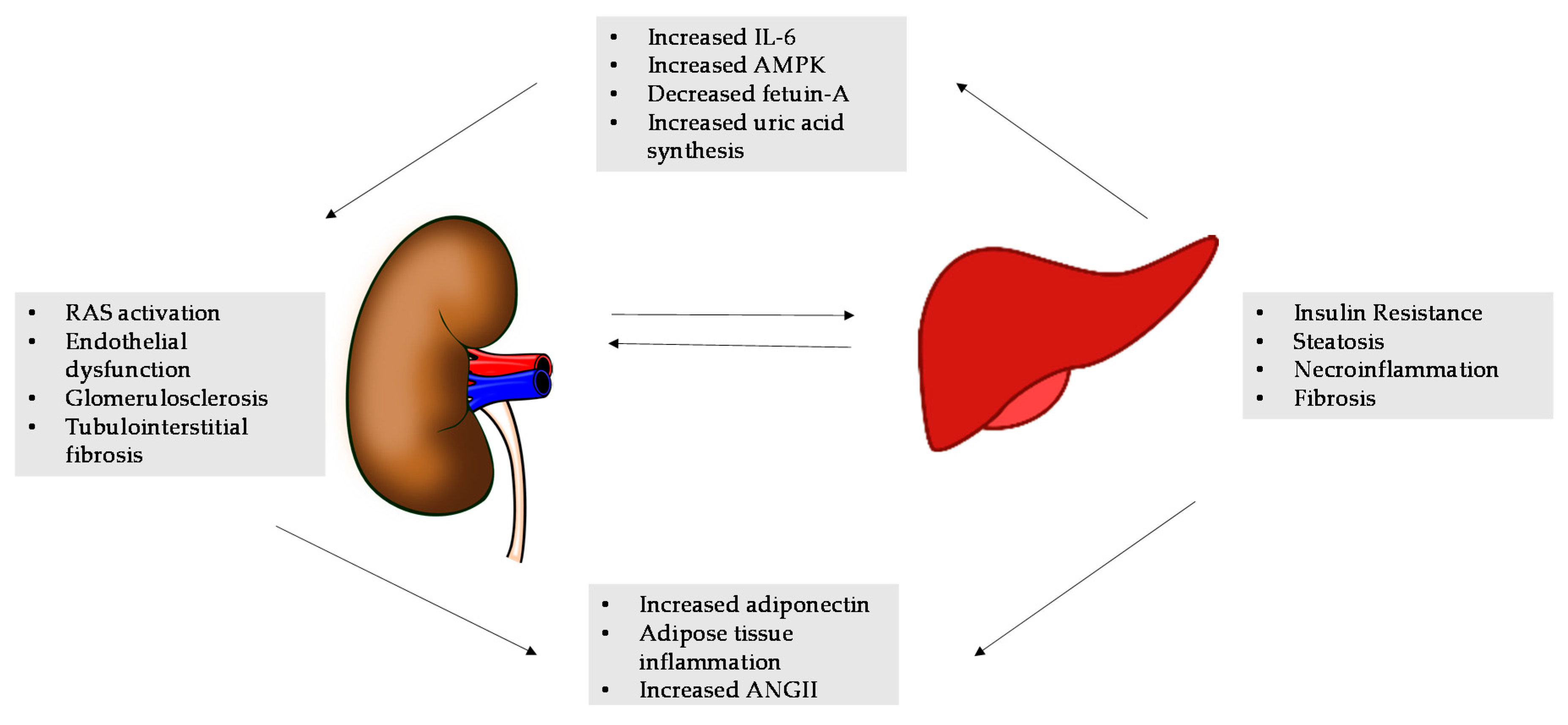
4. Mechanisms Linking NAFLD to CKD
4.1. AMPK, Fetuin-A, and Adiponectin
4.2. Renin-Angiotensin System (RAS) in NAFLD and CKD
4.3. Fructose Metabolism in NAFLD and CKD
4.4. Impaired Oxidative Stress
5. Therapeutic Interventions in NAFLD and CKD
6. Conclusions
Conflicts of Interest
Abbreviations
| DM | diabetes mellitus |
| HTN | hypertension |
| Tg | triglycerides |
| A1C% | hemoglobin A1C |
| eGFR | estimated glomerular filtration rate |
| MDRD | Modification of Diet in Renal Disease |
| CKD-EPI | Chronic Kidney Disease Epidemiology Collaboration |
| CRP | C-reactive protein |
| LFTs | liver function tests |
| HR | hazard ration |
| CI | confidence interval |
References
- Vernon, G.; Baranova, A.; Younossi, Z.M. Systematic review: The epidemiology and natural history of non-alcoholic fatty liver disease and non-alcoholic steatohepatitis in adults. Aliment. Pharmacol. Ther. 2011, 34, 274–285. [Google Scholar] [CrossRef] [PubMed]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Diehl, A.M.; Brunt, E.M.; Cusi, K.; Charlton, M.; Sanyal, A.J. The diagnosis and management of non-alcoholic fatty liver disease: Practice guideline by the American Association for the Study of Liver Diseases, American College of Gastroenterology, and the American Gastroenterological Association. Hepatology 2012, 55, 2005–2023. [Google Scholar]
- Loomba, R.; Sanyal, A.J. The global NAFLD epidemic. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 686–690. [Google Scholar] [CrossRef] [PubMed]
- McCullough, K.; Sharma, P.; Ali, T.; Khan, I.; Smith, W.C.; MacLeod, A.; Black, C. Measuring the population burden of chronic kidney disease: A systematic literature review of the estimated prevalence of impaired kidney function. Nephrol. Dial. Transplant. 2012, 27, 1812–1821. [Google Scholar] [CrossRef] [PubMed]
- Targher, G.; Chonchol, M.B.; Byrne, C.D. CKD and non-alcoholic fatty liver disease. AJKD 2014, 64, 638–652. [Google Scholar] [CrossRef] [PubMed]
- Black, C.; Sharma, P.; Scotland, G.; McCullough, K.; McGurn, D.; Robertson, L.; Fluck, N.; MacLeod, A.; McNamee, P.; Prescott, G.; et al. Early referral strategies for management of people with markers of renal disease: A systematic review of the evidence of clinical effectiveness, cost-effectiveness and economic analysis. Health Technol. Assess. 2010, 14, 1–184. [Google Scholar] [CrossRef] [PubMed]
- Athyros, V.; Tziomalos, K.; Katsiki, N.; Doumas, M.; Karagiannis, A.; Mikhailidis, D.P. Cardiovascular risk across the histological spectrum and the clinical manifestations of non-alcoholic fatty liver disease; an update. World J. Gastroenterol. 2015, 21, 6820–6834. [Google Scholar] [PubMed]
- Singal, A.K.; Salameh, H.; Kuo, Y.F.; Wiesner, R.H. Evolving frequency and outcomes of simultaneous liver kidney transplants based on liver disease etiology. Transplantation 2014, 98, 216–221. [Google Scholar] [CrossRef] [PubMed]
- Coresh, J.; Byrd-Holt, D.; Astor, B.C.; Briggs, J.P.; Eggers, P.W.; Lacher, D.A.; Hostetter, T.H. Chronic kidney disease awareness, prevalence, and trends among US adults, 1999 to 2000. J. Am. Soc. Nephrol. 2005, 16, 180–188. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Kim, W.R.; Kim, H.J.; Therneau, T.M. Association between noninvasive fibrosis markers and mortality among adults with nonalcoholic fatty liver disease in the United States. Hepatology 2013, 57, 1357–1365. [Google Scholar] [CrossRef] [PubMed]
- Hernaez, R.; Lazo, M.; Bonekamp, S.; Kamel, I.; Brancati, F.L.; Guallar, E.; Clark, J.M. Diagnostic accuracy and reliability of ultrasonography for the detection of fatty liver: A meta-analysis. Hepatology 2011, 54, 1082–1090. [Google Scholar] [CrossRef] [PubMed]
- Anstee, Q.M.; Targher, G.; Day, C.P. Progression of NAFLD to diabetes mellitus, cardiovascular disease or cirrhosis. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 330–344. [Google Scholar] [CrossRef] [PubMed]
- Dowman, J.K.; Tomlinson, J.W.; Newsome, P.N. Systematic review; the diagnosis and staging of non-alcoholic fatty liver disease and non-alcoholic steatohepatitis. Aliment. Pharmacol. Ther. 2011, 33, 525–540. [Google Scholar] [CrossRef] [PubMed]
- Mikolasevic, I.; Racki, S.; Bubic, I.; Jelic, I.; Stimac, D.; Orlic, L. Chronic kidney disease and nonalcoholic fatty liver disease proven by transient elastography. Kidney Blood Press Res. 2013, 37, 305–310. [Google Scholar] [CrossRef] [PubMed]
- Mikolasevic, I.; Orlic, L.; Zaputovic, L.; Racki, S.; Cubranic, Z.; Anic, K.; Devcic, B.; Stimac, D. Usefulness of liver test and controlled attenuation parameter in detection of nonalcoholic fatty liver disease in patients with chronic renal failure and coronary heart disease. Wien. Klin. Wochenschr. 2015, 127, 451–458. [Google Scholar] [CrossRef] [PubMed]
- Satapathy, S.K.; Garg, S.; Chauhan, R.; Sakhuja, P.; Malhotra, V.; Sharma, B.C.; Sarin, S.K. Beneficial effects of tumor necrosis factor-α inhibition by pentoxyfilline on clinical, biochemical, and metabolic parameters of patients with nonalcoholic steatohepatitis. Am. J. Gastroenterol. 2004, 99, 1946–1952. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, W.M.; Voelker, M.; Thiel, R.; Becka, M.; Burt, A.; Schuppan, D.; Hubscher, S.; Roskams, T.; Pinzani, M.; Arthur, M.J. European Liver Fibrosis Group: Serum markers detect the presence of liver fibrosis: A cohort study. Gastroenterology 2004, 127, 1704–1713. [Google Scholar] [CrossRef] [PubMed]
- Ratziu, V.; Gira, P.; Charlotte, F.; Bruckert, E.; Thibault, V.; Theodorou, I.; Khalil, L.; Turpin, G.; Opolon, P.; Poynard, T. Liver fibrosis in overweight patient. Gastroenterology 2000, 118, 1117–1123. [Google Scholar] [CrossRef]
- Ratziu, V.; Massard, J.; Charlotte, F.; Messous, D.; Imbert-Bismut, F.; Bonyhay, L.; Tahiri, M.; Munteanu, M.; Thabut, D.; Cadranel, J.F.; et al. Diagnostic value of biochemical markers (FibroTest-FibroSURE) for the prediction of liver fibrosis in patients with non-alcoholic fatty liver disease. BMC Gastroenterol. 2006, 6, 6. [Google Scholar] [CrossRef] [PubMed]
- Angulo, P.; Keach, J.C.; Batts, K.P.; Lindor, K.D. Independent predictor of liver fibrosis in patients with nonalcoholic steatohepatitis. Hepatology 1999, 30, 1356–1362. [Google Scholar] [CrossRef] [PubMed]
- Harrison, S.A.; Oliver, D.; Arnod, H.L.; Gogia, S.; Neuschwander-Tetri, B.A. Development and validation of a simple NAFLD clinical scoring system for identifying patients without advanced disease. Gut 2008, 57, 1441–1447. [Google Scholar] [CrossRef] [PubMed]
- Cales, P.; Laine, F.; Boursier, J.; Deugnier, Y.; Moal, V.; Oberti, F.; Hunault, G.; Rousselet, M.C.; Hubert, I.; Laafi, J.; et al. Comparison of blood tests for liver fibrosis specific or not to NAFLD. J. Hepatol. 2009, 50, 165–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, A.; Lydecker, A.; Murray, K.; Tetri, B.N.; Contos, M.J.; Sanyal, A.J. Nash Clinical Research Network. Comparison of noninvasive markers of fibrosis in patients with nonalcoholic fatty liver disease. Clin. Gastroenterol. Hepatol. 2009, 7, 1104–1112. [Google Scholar] [CrossRef] [PubMed]
- Sumida, Y.; Yoneda, M.; Hyogo, H.; Yamaguchi, K.; Ono, M.; Fujii, H.; Eguchi, Y.; Suzuki, Y.; Imai, S.; Kanemasa, K.; et al. Japan Study Group of Nonalcoholic Fatty Liver Disease (JSG-NAFLD): A simple clinical scoring system using ferritin, fasting insulin, and type IV collagen 7S for predicting steatohepatitis in nonalcoholic fatty liver disease. J. Gastroenterol. 2011, 46, 257–268. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.; Page, S.; Rafiq, N.; Birerdinc, A.; Stepanova, M.; Hossain, N.; Afendy, A.; Younoszai, Z.; Goodman, Z.; Baranova, A. A biomarker panel for non-alcoholic steatohepatitis (NASH) and NASH-related fibrosis. Obes. Surg. 2011, 21, 431–439. [Google Scholar] [CrossRef] [PubMed]
- Pearce, S.G.; Thosani, N.C.; Pan, J. Noninvasive biomarkers for the diagnosis of steatohepatitis and advanced fibrosis in NAFLD. Biomark. Res. 2013, 1, 7. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.W.; Hsu, Y.C.; Chang, C.H.; Wei, K.L.; Lin, C.L. High FIB-4 index as an independent risk factor of prevalent chronic kidney disease in patients with nonalcoholic fatty liver disease. Hepatol. Int. 2016, 10, 340–346. [Google Scholar] [CrossRef] [PubMed]
- Musso, G.; Gambino, R.; Tabibian, J.H.; Ekstedt, M.; Kechagias, S.; Hamaguchi, M.; Hultcrantz, R.; Hagström, H.; Yoon, S.K.; Charatcharoenwitthaya, P.; et al. Association of non-alcoholic fatty liver disease with chronic kidney disease: A systematic review and meta-analysis. PLoS Med. 2014, 11, e1001680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Targher, G.; Bertolini, L.; Rodella, S.; Zoppini, G.; Lippi, G.; Day, C.; Muggeo, M. Non-alcoholic fatty liver disease is independently associated with an increased prevalence of chronic kidney disease and proliferative/laser-treated retinopathy in type 2 diabetic patients. Diabetologia 2008, 51, 444–450. [Google Scholar] [CrossRef] [PubMed]
- Campos, G.M.; Bambha, K.; Vittinghoff, E.; Rabl, C.; Posselt, A.M.; Ciovica, R.; Tiwari, U.; Ferrel, L.; Pabst, M.; Bass, N.M.; et al. A clinical scoring system for predicting nonalcoholic steatohepatitis in morbidly obese patients. Hepatology 2008, 47, 1916–1923. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.; Ryu, S.; Sung, E.; Woo, H.Y.; Oh, E.; Cha, K.; Jung, E.; Kim, W.S. Nonalcoholic fatty liver disease predicts chronic kidney disease in nonhypertensive and nondiabetic Korean men. Metabolism 2008, 57, 569–576. [Google Scholar] [CrossRef] [PubMed]
- Targher, G.; Chonchol, M.; Bertolini, L.; Rodella, S.; Zenari, L.; Ciovica, R.; Tiwari, U.; Ferrel, L.; Pabst, M.; Bass, N.M.; et al. Increased risk of CKD among type 2 diabetics with nonalcoholic fatty liver disease. J. Am. Soc. Nephrol. 2008, 19, 1564–1570. [Google Scholar] [CrossRef] [PubMed]
- Targher, G.; Bertolini, L.; Chonchol, M.; Rodella, S.; Zoppini, G.; Lippi, G. Nonalcoholic fatty liver disease is independently associated with an increased prevalence of chronic kidney disease and retinopathy in type 1 diabetic patients. Diabetologia 2010, 53, 1341–1348. [Google Scholar] [CrossRef] [PubMed]
- Targher, G.; Bertolini, L.; Rodella, S.; Lippi, G.; Zoppini, G.; Chonchol, M. Relationship between kidney function and liver histology in subjects with nonalcoholic steatohepatitis. Clin. J. Am. Soc. Nephrol. 2010, 5, 2166–2171. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, Y.; Alahdab, Y.O.; Yonal, O.; Kurt, R.; Kedrah, A.E.; Celikel, C.A.; Ozdogan, O.; Duman, D.; Imeryuz, N.; Avsar, E.; et al. Microalbuminuria in nondiabetic patients with nonalcoholic fatty liver disease: Association with liver fibrosis. Metabolism 2010, 59, 1327–1330. [Google Scholar] [CrossRef] [PubMed]
- Söderberg, C.; Stål, P.; Askling, J.; Glaumann, H.; Lindberg, G.; Marmur, J.; Hultcrantz, R. Decreased survival of subjects with elevated liver function tests during a 28-year follow-up. Hepatology 2010, 51, 595–602. [Google Scholar] [CrossRef] [PubMed]
- Wong, V.W.; Wong, G.L.; Choi, P.C.; Chan, A.W.; Li, M.K.; Chan, H.Y.; Chim, A.M.; Yu, J.; Sung, J.J.; Chan, H.L. Disease progression of non-alcoholic fatty liver disease: A prospective study with paired liver biopsies at 3 years. Gut 2010, 59, 969–974. [Google Scholar] [CrossRef] [PubMed]
- Lau, K.; Lorbeer, R.; Haring, R.; Schmidt, C.O.; Wallaschofski, H.; Nauck, M.; John, U.; Baumeister, S.E.; Völzke, H. The association between fatty liver disease and blood pressure in a population-based prospective longitudinal study. J. Hypertens. 2010, 28, 1829–1835. [Google Scholar] [CrossRef] [PubMed]
- Yasui, K.; Sumida, Y.; Mori, Y.; Mitsuyoshi, H.; Minami, M.; Itoh, Y.; Kanemasa, K.; Matsubara, H.; Okanoue, T.; Yoshikawa, T. Nonalcoholic steatohepatitis and increased risk of chronic kidney disease. Metabolism 2011, 60, 735–739. [Google Scholar] [CrossRef] [PubMed]
- Machado, M.V.; Gonçalves, S.; Carepa, F.; Coutinho, J.; Costa, A.; Cortez-Pinto, H. Impaired renal function in morbid obese patients with nonalcoholic fatty liver disease. Liver Int. 2012, 32, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Targher, G.; Pichiri, I.; Zoppini, G.; Trombetta, M.; Bonora, E. Increased prevalence of chronic kidney disease in patients with Type 1 diabetes and non-alcoholic fatty liver. Diabet. Med. 2012, 29, 220–226. [Google Scholar] [CrossRef] [PubMed]
- Sirota, J.C.; McFann, K.; Targher, G.; Chonchol, M.; Jalal, D.I. Association between nonalcoholic liver disease and chronic kidney disease: An ultrasound analysis from NHANES 1988–1994. Am. J. Nephrol. 2012, 36, 466–471. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, M.J.; Houlihan, D.D.; Bentham, L.; Shaw, J.C.; Cramb, R.; Olliff, S.; Gill, P.S.; Neuberger, J.M.; Lilford, R.J.; Newsome, P.N. Presence and severity of non-alcoholic fatty liver disease in a large prospective primary care cohort. J. Hepatol. 2012, 56, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Musso, G.; Cassader, M.; de Michieli, F.; Rosina, F.; Orlandi, F.; Gambino, R. Nonalcoholic steatohepatitis versus steatosis: Adipose tissue insulin resistance and dysfunctional response to fat ingestion predict liver injury and altered glucose and lipoprotein. Metab. Hepatol. 2012, 56, 933–942. [Google Scholar] [CrossRef] [PubMed]
- Francque, S.M.; Verrijken, A.; Mertens, I.; Hubens, G.; van Marck, E.; Pelckmans, P.; Michielsen, P.; van Gaal, L. Noninvasive assessment of nonalcoholic fatty liver disease in obese or overweight patients. Clin. Gastroenterol. Hepatol. 2012, 10, 1162–1168. [Google Scholar] [CrossRef] [PubMed]
- Casoinic, F.; Sâmpelean, D.; Bădău, C.; Prună, L. Nonalcoholic fatty liver disease–A risk factor for microalbuminuria in type 2 diabetic patients. Rom. J. Int. Med. 2009, 47, 55–59. [Google Scholar]
- Xia, M.F.; Lin, H.D.; Li, X.M.; Yan, H.M.; Bian, H.; Chang, X.X.; He, W.Y.; Jeekel, J.; Hofman, A.; Gao, X. Renal function-dependent association of serum uric acid with metabolic syndrome and hepatic fat content in a middle-aged and elderly Chinese population. Clin. Exp. Pharmacol. Physiol. 2012, 39, 930–937. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.S.; Jung, E.S.; Hur, W.; Bae, S.H.; Choi, J.Y.; Chang, X.X.; He, W.Y.; Jeekel, J.; Hofman, A.; Gao, X. Noninvasive predictors of nonalcoholic steatohepatitis in Korean patients with histologically proven nonalcoholic fatty liver disease. Clin. Mol. Hepatol. 2013, 19, 120–130. [Google Scholar] [CrossRef] [PubMed]
- Angulo, P.; Bugianesi, E.; Bjornsson, E.S.; Charatcharoenwitthaya, P.; Mills, P.R.; Barrera, F.; Haflidadottir, S.; Day, C.P.; George, J. Simple noninvasive systems predict long-term outcomes of patients with nonalcoholic fatty liver disease. Gastroenterology 2013, 145, 782–789. [Google Scholar] [CrossRef] [PubMed]
- El Azeem, H.A.; Khalek, E.A.; El-Akabawy, H.; Naeim, H.; Khalik, H.A.; Alfifi, A.A. Association between nonalcoholic fatty liver disease and the incidence of cardiovascular and renal events. J. Saudi. Heart Assoc. 2013, 25, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Musso, G.; Cassader, M.; Cohney, S.; Pinach, S.; Saba, F.; Gambino, R. Emerging liver–kidney interactions in nonalcoholic fatty liver disease. Trends Mol. Med. 2015, 21, 645–662. [Google Scholar] [CrossRef] [PubMed]
- Ogden, C.L.; Carroll, M.D.; Kit, B.K.; Flegal, K.M. Prevalence of childhood and adult obesity in the United States, 2011–2012. JAMA 2014, 311, 806–814. [Google Scholar] [CrossRef] [PubMed]
- Ix, J.H.; Sharma, K. Mechanisms linking obesity, chronic kidney disease, and fatty liver disease: The roles of fetuin-A, adiponectin, and AMPK. J. Am. Soc. Nephrol. 2010, 21, 406–412. [Google Scholar] [CrossRef] [PubMed]
- Hamaguchi, M.; Kojima, T.; Takeda, N.; Nakagawa, T.; Taniguchi, H.; Fujii, K.; Omatsu, T.; Nakajima, T.; Sarui, H.; Shimazaki, M.; et al. The metabolic syndrome as a predictor of nonalcoholic fatty liver disease. Ann. Intern. Med. 2005, 143, 722–728. [Google Scholar] [CrossRef] [PubMed]
- Mathews, S.T.; Rakhade, S.; Zhou, X.; Parker, G.C.; Coscina, D.V.; Grunberger, G. Fetuin-null mice are protected against obesity and insulin resistance associated with aging. Biochem. Biophys. Res. Commun. 2006, 350, 437–443. [Google Scholar] [CrossRef] [PubMed]
- Ix, J.H.; Chertow, G.M.; Shlipak, M.G.; Brandenburg, V.M.; Ketteler, M.; Whooley, M.A. Fetuin-A and kidney function in persons with coronary artery disease—Data from the Heart and Soul Study. Nephrol. Dial. Transplant. 2006, 21, 2144–2151. [Google Scholar] [CrossRef] [PubMed]
- De Vries, A.P.; Ruggenenti, P.; Ruan, X.Z.; Praga, M.; Cruzado, J.M.; Bajema, I.M.; D'Agati, V.D.; Lamb, H.J.; Pongrac Barlovic, D.; Hojs, R.; et al. Fatty kidney: Emerging role of ectopic lipid in obesity-related renal disease. Lancet Diabetes Endocrinol. 2014, 2, 417–426. [Google Scholar] [CrossRef]
- Osterreicher, C.H.; Taura, K.; de Minicis, S.; Seki, E.; Penz-Osterreicher, M.; Kodama, Y.; Kluwe, J.; Schuster, M.; Oudit, G.Y.; Penninger, J.M.; et al. Angiotensin-converting-enzyme 2 inhibits liver fibrosis in mice. Hepatology 2009, 50, 929–938. [Google Scholar] [CrossRef] [PubMed]
- Vos, M.; Kimmons, J.; Gillespie, C.; Welsh, J.; Blanck, H. Dietary fructose consumption among US children and adults: The Third National Health and Nutrition Examination Survey. Medscape J. Med. 2008, 10, 160. [Google Scholar] [PubMed]
- Osterreicher, C.H.; Taura, K.; de Minicis, S.; Seki, E.; Penz-Osterreicher, M.; Kodama, Y.; Kluwe, J.; Schuster, M.; Oudit, G.Y.; Penninger, J.M.; et al. Betaine supplementation protects against high-fructose-induced renal injury in rats. J. Nutr. Biochem. 2014, 25, 353–362. [Google Scholar]
- Abdelmalek, M.F.; Suzuki, A.; Guy, C.; Unalp-Arida, A.; Colvin, R.; Johnson, R.J.; Diehl, A.M. Nonalcoholic Steatohepatitis Clinical Research Network. Increased fructose consumption is associated with fibrosis severity in patients with nonalcoholic fatty liver disease. Hepatology 2010, 51, 1961–1971. [Google Scholar] [CrossRef] [PubMed]
- Cheungpasitporn, W.; Thongprayoon, C.; O'Corragain, O.A.; Edmonds, P.J.; Kittanamongkolchai, W.; Erickson, S.B. Associations of sugar and artificially sweetened soda and chronic kidney disease: A systematic review and meta-analysis. Nephrology 2014, 19, 791–797. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Cui, Y.; Li, C.; Zhang, Y.; Xu, S.; Li, X.; Li, H.; Zhang, X. Nrf2 deletion causes “benign” simple steatosis to develop into nonalcoholic steatohepatitis in mice fed a high-fat diet. Lipids Health Dis. 2013, 12, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Pergola, P.E.; Raskin, P.; Toto, R.D.; Meyer, C.J.; Huff, W.; Grossman, E.B.; Krauth, M.A.B.; Ruiz, S.; Audhya, P.; Christ-Schmidt, H.; et al. Bardoxolone methyl and kidney function in CKD with type 2 diabetes. N. Engl. J. Med. 2011, 365, 327–336. [Google Scholar] [CrossRef] [PubMed]
- De Zeeuw, D.; Akizawa, T.; Agarwal, R.; Audhya, P.; Bakris, G.L.; Chin, M.; Krauth, M.; Lambers Heerspink, H.J.; Meyer, C.J.; McMurray, J.J.; et al. Rationale and trial design of bardoxolone methyl evaluation in patients with chronic kidney disease and type 2 diabetes: The occurrence of renal events (BEACON). Am. J. Nephrol. 2013, 37, 212–222. [Google Scholar] [CrossRef] [PubMed]
- Hirata, T.; Tomita, K.; Kawai, T.; Yokoyama, H.; Shimada, A.; Kikuchi, M.; Hirose, H.; Ebinuma, H.; Irie, J.; Ojiro, K.; et al. Effect of telmisartan or losartan for treatment of nonalcoholic fatty liver disease: Fatty Liver Protection Trial by Telmisartan or Losartan Study (FANTASY). Int. J. Endocrinol. 2013, 2013, 587140. [Google Scholar] [CrossRef] [PubMed]
- Bain, R.; Rohde, R.; Hunsicker, L.G.; McGill, J.; Kobrin, S.; Lewis, E.J. A controlled clinical trial of angiotensin-converting enzyme inhibition in type I diabetic nephropathy: Study design and patient characteristics. The Collaborative Study Group. J. Am. Soc. Nephrol. 1992, 3, S97–S103. [Google Scholar] [PubMed]
- Orlic, L.; Mikolasevic, I.; Lukenda, V.; Anic, K.; Jelic, I.; Racki, S. Nonalcoholic fatty liver disease and the renin-angiotensin system blockers in the patients with chronic kidney disease. Wien. Klin. Wochenschr. 2015, 127, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Khera, R.; Allen, A.M.; Murad, H.; Loomba, R. Comparative effectiveness of pharmacologic interventions for non-alcoholic steatohepatitis: A systemic review and network meta-analysis. Hepatology 2015, 62, 1417–1432. [Google Scholar] [CrossRef] [PubMed]
- Athyros, V.G.; Tziomalos, K.; Gossios, T.D.; Griva, T.; Anagnostis, P.; Kargiotis, K.; Pagourelias, E.D.; Theocharidou, E.; Karagiannis, A.; Mikhailidis, D.P. Safety and efficacy of long-term statin treatment for cardiovascular events in patients with coronary heart disease and abnormal liver tests in the Greek Atorvastatin and Coronary Heart Disease Evaluation (GREACE) Study: A post-hoc analysis. Lancet 2010, 376, 1916–1922. [Google Scholar] [CrossRef]
- Tikkanen, M.J.; Fayyad, R.; Faergeman, O.; Olsson, A.G.; Wun, C.C.; Laskey, R.; Kastelein, J.J.; Holme, I.; Pedersen, T.R. Effect of intensive lipid lowering with atorvastatin on cardiovascular outcomes in coronary heart disease patients with mild-to-moderate baseline elevations in alanine aminotransferase levels. Int. J. Cardiol. 2013, 168, 3846–3852. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Reference | Test | Components | PPV% | NPV% |
|---|---|---|---|---|
| Rosenberg [17] | Original European Liver Fibrosis Panel | age, HA, TIMP1, PIIINP for score ≤1 | 80 | 98 |
| Ratziu [18] | BAAT score | BMI ≥ 28 kg/m2 age ≥ 50 years, ALT ≥ 2 × ULN triglycerides ≥ 1.7 mmol/L | 33 | 100 |
| Ratziu [19] | Fibrotest | α2 macroglobulin, haptoglobin, GGT, Total bilirubin, apolipoprotein A1 | 54 | 90 |
| Angulo [20] | NAFLD Fibrosis Score | age, hyperglycemia, BMI, platelet count, albumin, AAR | 56 | 93 |
| Harrison [21] | BARD | BMI ≥ 28 kg/m2, AAR ≥ 0.8, diabetes | 43 | 96 |
| Cales [22] | Fibrometer NAFLD | glucose, AST, ferritin, ALT, body weight, age | 87.9 | 92.1 |
| Shah [23] | FIB4 index | age, ALT, AST, platelet count | 43 | 90 |
| Sumida [24] | NAFIC score | serum ferritin (≥200 ng/mL for female, ≥300 ng/mL for male), fasting insulin ≥ 10 | 32 | 96 |
| Younossi [25] | NAFLD Diagnostic Panel | diabetes, gender, BMI, triglycerides, apoptotic and necrotic CK18 fragments | 57.7 | 85 |
| Study | Characteristics | CKD Diagnosis and Prevalence | Liver Disease Diagnosis and Prevalence | Risk Factors Adjusted in Analysis |
|---|---|---|---|---|
| Targher, 2008 [29] | Outpatient; n = 103; HTN 63% | eGFR < 60 mL/min/1.73 m2 (CKD-EPI) and/or overt proteinuria; 15% | Ultrasound; 48% | Age, sex, BMI, waist circumference, HTN, alcohol consumption, diabetes duration, HbA1c, LDL cholesterol, Tg |
| Campos, 2008 [30] | Hospital; n = 197; HTN 56%, DM 26% | eGFR < 60 mL/min/1.73 m2 (CKD-EPI); 10% | Liver biopsy: NAFLD 63%, NASH 32% | Age, gender, BMI, waist circumference, HTN |
| Chang, 2008 [31] | Population; n = 8329; DM 0%, HTN 0%, metabolic syndrome 6% | eGFR < 60 mL/min/1.73 m2 (MDRD) or morning proteinuria >1+; 4% | Ultrasound; 73% | Age, eGFR, dyslipidemia, BMI, CRP, sys BP |
| Targher, 2008 [32] | Population; n = 1760; DM 100%, HTN 65%, metabolic syndrome 55% | eGFR < 60 mL/min/1.73 m2 (MDRD) or ACR = 300 mg/g; 31% | Ultrasound; 30% | Age, gender, BMI, waist circumference, BP, LDL-C, Tg, smoking, DM duration, medications |
| Targher, 2010 [33] | Outpatient; n = 202 adults; HTN 35%, DM 0% | eGFR < 60 mL/min/1.73 m2 and/or ACR ≥ 30 mg/g; 37.8% | Ultrasound | Age, sex, BMI, systolic BP, alcohol consumption, diabetes duration, HbA1c, Tg, medication use |
| Targher, 2010 [34] | Hospital; n = 160; DM 6%, HTN 60%, metabolic syndrome 29% | eGFR < 60 mL/min/1.73 m2 (CKD-EPI) or ACR = 30 mg/g; 14% | Biopsy; NASH 100% | Age, sex, BMI, waist circumference, smoking, systolic BP, insulin resistance |
| Yilmaz, 2010 [35] | Hospital; n = 87; DM 0%, HTN 30%, metabolic syndrome 27% | eGFR < 60 mL/min/1.73 m2 (CKD-EPI) or ACE 30–300 mg/d; 16% | Biopsy; NAFLD 100%, NASH 67% | Age, gender, BMI, waist circumference, BP, lipids, smoking, insulin resistance, metabolic syndrome |
| Soderberg, 2010 [36] | Hospital; n = 125; DM 24%, HTN 37%, metabolic syndrome 31% | eGFR < 60 mL/min/1.73 m2 (CKD-EPI); 27% | Biopsy; NAFLD 67%, NASH 33% | Age, BMI, HTN, smoking, DM, metabolic syndrome |
| Wong 2010 [37] | Hospital; n = 51; DM 50%, HTN 37%, metabolic syndrome 65% | eGFR < 60 mL/min/1.73 m2 (CKD-EPI) or ACR > 30mg/g; 8% | Biopsy; NAFLD 100%, NASH 33% | Age, BMI, DM, HTN, waist circumference, metabolic syndrome, smoking |
| Lau 2010 [38] | Population; n = 2858; DM 8.9%, HTN 47%; metabolic syndrome 24% | eGFR < 60 mL/min/1.73 m2 (CKD-EPI) or ACR > 30 mg/g; 8% | Ultrasound; 30% | Age, BMI, metabolic syndrome, HTN, dyslipidemia, smoking |
| Yasui 2011 [39] | Hospital; n = 169; DM 31%, HTN 34%, metabolic syndrome 30% | eGFR < 60 mL/min/1.73 m2 (CKD-EPI) or am proteinuria 1+; 14% | Biopsy; NAFLD 100%, NASH 53% | BMI, HTN, waist circumference, dyslipidemia, smoking, DM |
| Machado 2012 [40] | Hospital; n = 148; HTN 67% | eGFR < 60 mL/min/1.73 m2; 8% | Biopsy; NAFLD 100% | Age, sex, HTN, DM, dyslipidemia |
| Targher 2012 [41] | Hospital; n = 343; DM 100%, HTN 43%, metabolic syndrome 46% | eGFR < 60 mL/min/1.73 m2 (MDRD) or ACR > 30 mg/g; 40% | Ultrasound 53% | Age, gender, BMI, family history, systolic BP, dyslipidemia, smoking DM, medications, microalbuminuria |
| Sirota 2012 [42] | Population; n = 11469; HTN 24% | eGFR < 60 mL/min/1.73 m2 and/or ACR > 30 mg/g; 42% | Ultrasound | Age, sex, race, HTN, diabetes, waist circumference, dyslipidemia, insulin resistance |
| Armstrong 2012 [43] | Population; n = 146; DM 0%, HTN 36% | eGFR < 60 mL/min/1.73 m2 (CKD-EPI); 25% | Ultrasound; 50% | BMI, HTN |
| Musso 2012 [44] | Hospital; n = 80; DM 0%, HTN 52%, metabolic syndrome 31% | eGFR < 60 mL/min/1.73 m2 (CKD-EPI) or ACR > 30 mg/d; 20% | Biopsy; NAFLD 50%, NASH 20% | Age, gender, BMI, waist circumference, HTN, smoking, metabolic syndrome |
| Francque 2012 [45] | Hospital; n = 230; DM 0%, HTN 50%, metabolic syndrome 47% | eGFR < 60 mL/min/1.73 m2 (CKD-EPI) or proteinuria > 300 mg/d; 9% | Biopsy; NAFLD 100%, NASH 52% | Age, BMI, HTN, waist circumference, smoking, metabolic syndrome |
| Casoinic 2012 [46] | Hospital; n = 145; DM 100%; HTN 55%; metabolic syndrome 80% | eGFR < 60 mL/min/1.73 m2 (CKD-EPI) or ACE 30–300 mg/g; 10% | Ultrasound; 51% | Age, gender, CRP |
| Xia 2012 [47] | Population; n = 1141; DM 0%, HTN 38%, metabolic syndrome 32% | eGFR < 60 mL/min/1.73 m2 (mDRD) or ACR > 30 mg/g; 12% | Ultrasound; 41% | Age, BMI, smoking, HTN, metabolic syndrome, uric acid |
| Kim 2013 [48] | Hospital; n = 96; DM 100%, HTN 66%, metabolic syndrome 56% | eGFR < 60 mL/min/1.73 m2 (MDRD) or proteinuria > 1+ am; 25% | Biopsy: NAFLD 100%, NASH 56% | Age, BMI, HTN, waist circumference, smoking, metabolic syndrome, dyslipidemia |
| Angulo 2013 [49] | Hospital; n = 191; DM 17%, HTN 32%, metabolic syndrome 25% | eGFR < 60 mL/min/1.73 m2 (CKD-EPI) or am proteinuria >1+; 18% | Biopsy | Age, BMI, DM, HTN, smoking, dyslipidemia, metabolic syndrome |
| El Azeem 2013 [50] | Population; n = 747; DM 57%, HTN 32%, metabolic syndrome 67% | eGFR < 60 mL/min/1.73 m2 (MDRD) or ACE > 30 mg/g; 29% | Ultrasound 35% | Age, BMI, HTN, dyslipidemia, smoking, metabolic syndrome |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marcuccilli, M.; Chonchol, M. NAFLD and Chronic Kidney Disease. Int. J. Mol. Sci. 2016, 17, 562. https://doi.org/10.3390/ijms17040562
Marcuccilli M, Chonchol M. NAFLD and Chronic Kidney Disease. International Journal of Molecular Sciences. 2016; 17(4):562. https://doi.org/10.3390/ijms17040562
Chicago/Turabian StyleMarcuccilli, Morgan, and Michel Chonchol. 2016. "NAFLD and Chronic Kidney Disease" International Journal of Molecular Sciences 17, no. 4: 562. https://doi.org/10.3390/ijms17040562
APA StyleMarcuccilli, M., & Chonchol, M. (2016). NAFLD and Chronic Kidney Disease. International Journal of Molecular Sciences, 17(4), 562. https://doi.org/10.3390/ijms17040562