
Histogram Analysis of Diffusion Weighted Imaging at 3T is Useful for Prediction of Lymphatic Metastatic Spread, Proliferative Activity, and Cellularity in Thyroid Cancer

 , ,
, ,
Abstract
:1. Introduction
2. Results
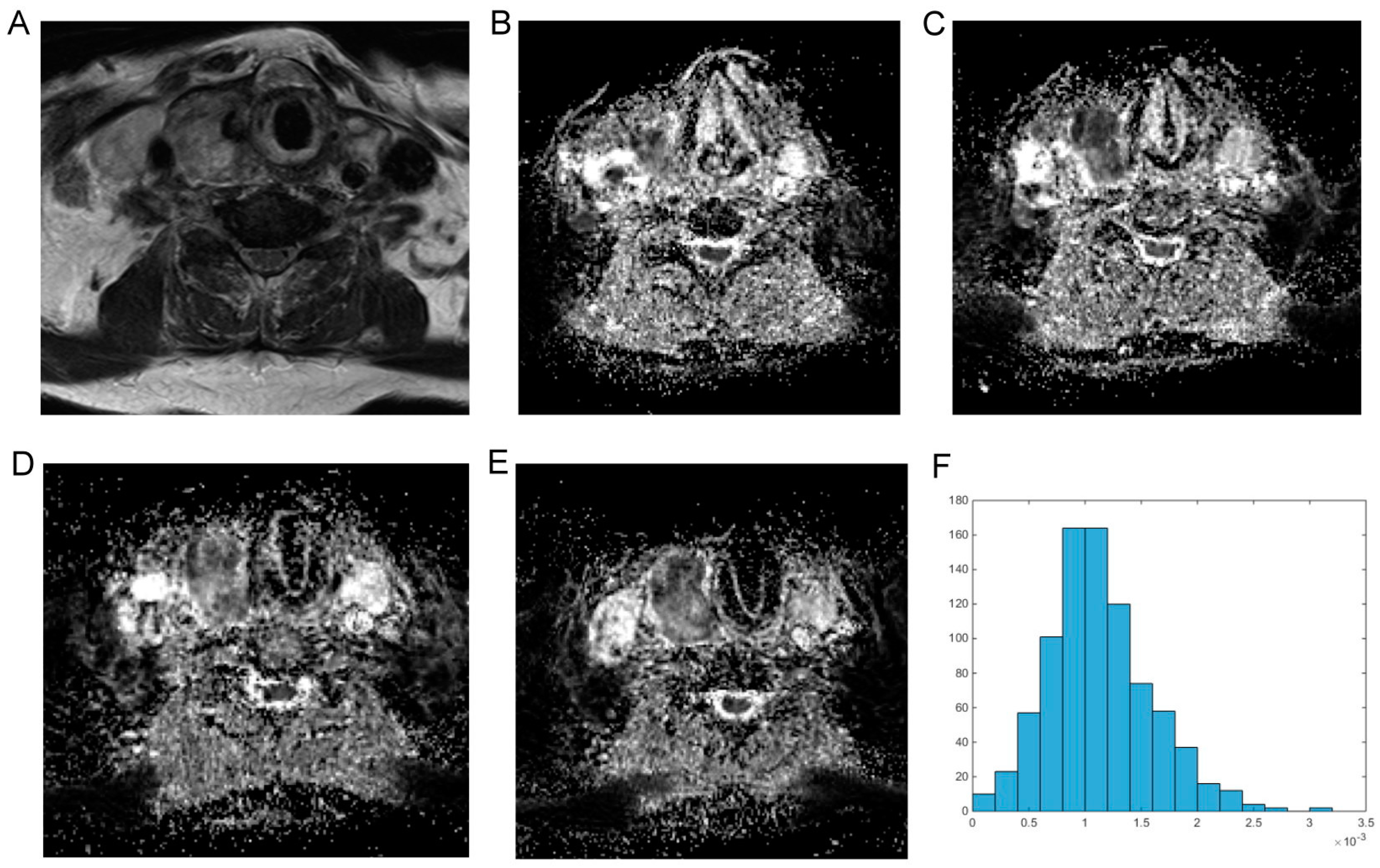
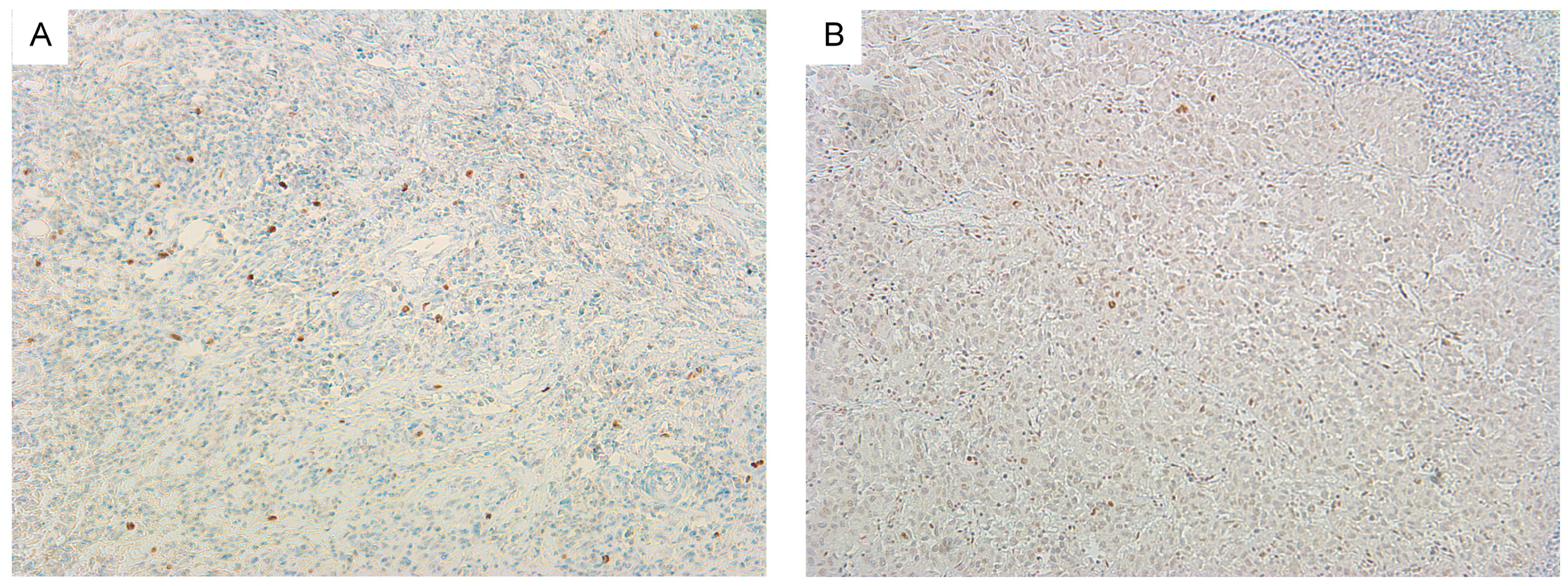
2.1. Diffusion Weighted Imaging and Immunohistopathology of Thyroid Carcinoma
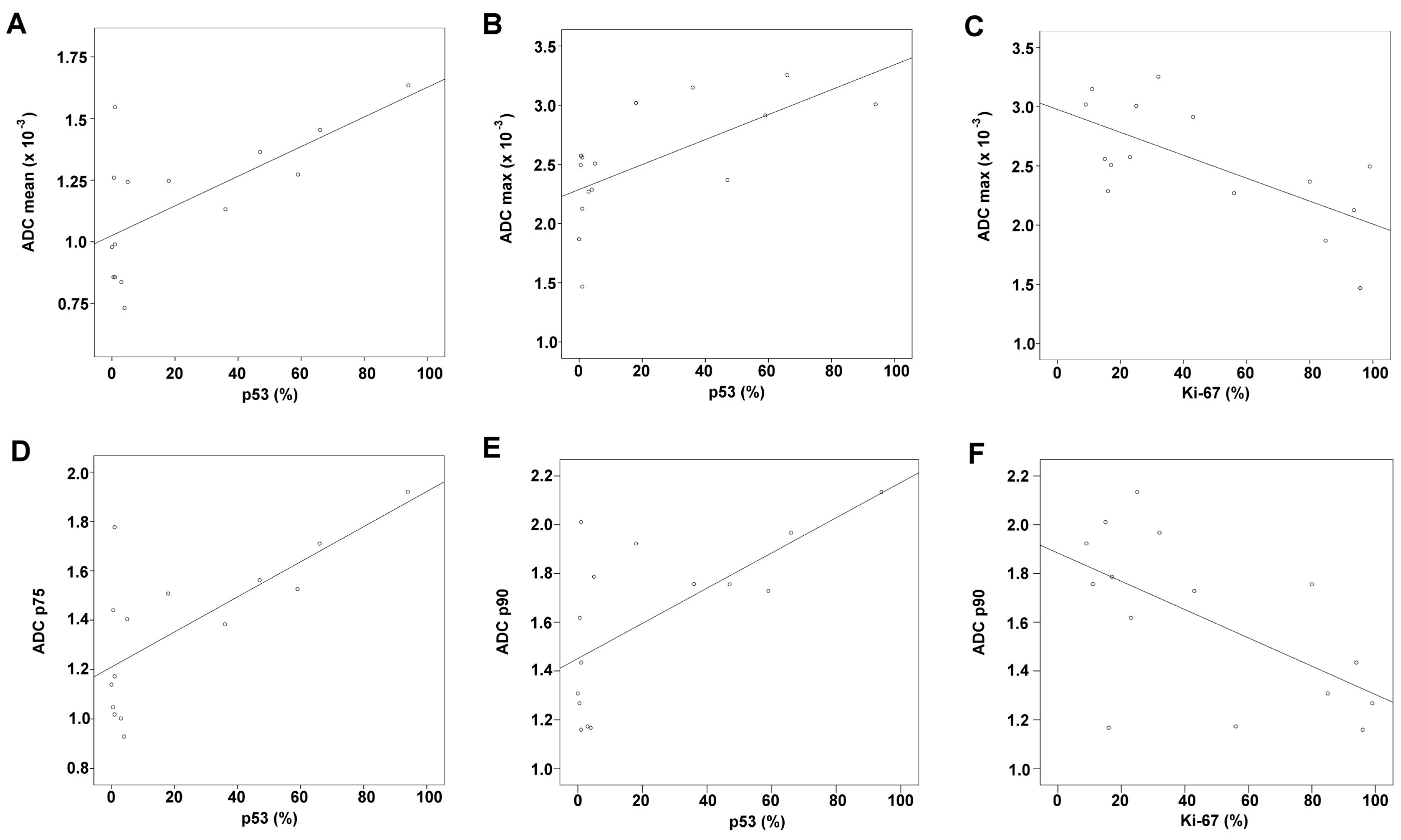
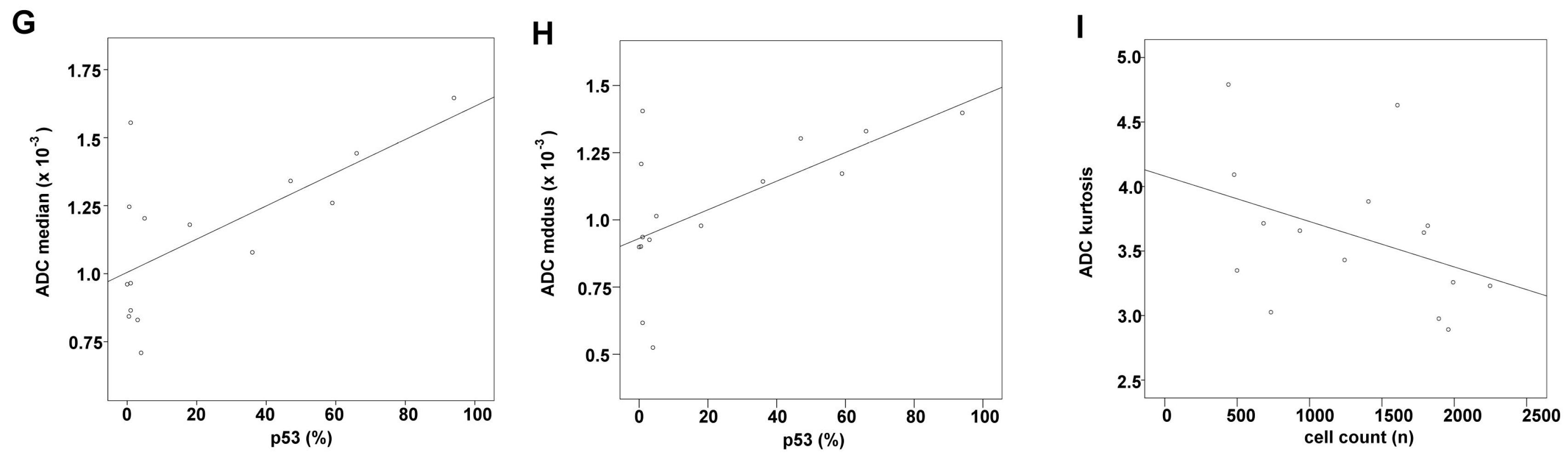
2.2. Correlation Analysis
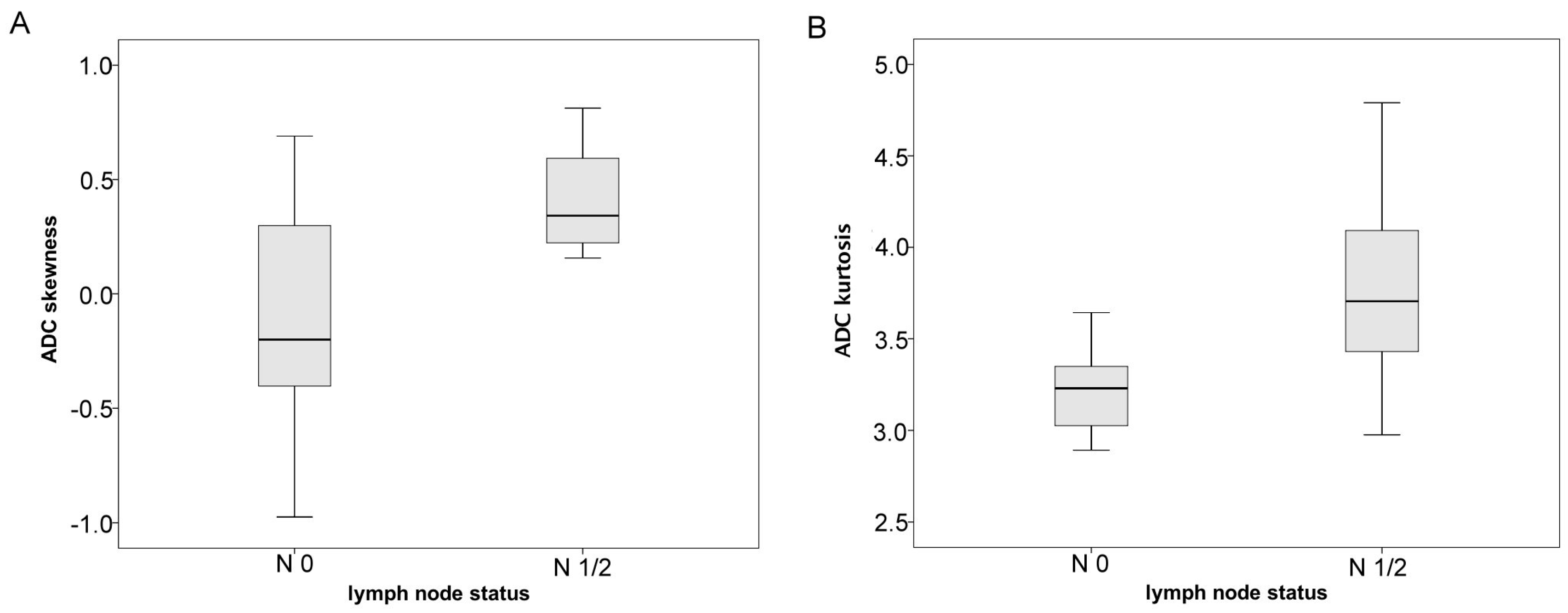
2.3. Group Comparisons
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. MRI
- axial T2 weighted (T2w) turbo spin echo (TSE) sequence (TR/TE: 4000/69, flip angle: 150°, slice thickness: 4 mm, acquisition matrix: 200 × 222, field of view: 100 mm);
- axial T1 weighted (T1w) turbo spin echo (TSE ) sequences (TR/TE: 765/9.5, flip angle: 150°, slice thickness: 5 mm, acquisition matrix: 200 × 222, field of view: 100 mm) before and after intravenous application of contrast medium (gadopentate dimeglumine, Magnevist®, Bayer Schering Pharma, Leverkusen, Germany);
- axial DWI (readout-segmented, multi-shot EPI sequence; TR/TE: 5400/69, flip angle 180°, slice thickness: 4 mm, acquisition matrix: 200 × 222, field of view: 100 mm) with b values of 0, 400 and 800 s/mm2. ADC maps were generated automatically by the implemented software package and analyzed as described previously [28].
4.3. Histogram Analysis of ADC Values
4.4. Histopathology and Immunohistochemistry
4.5. Statistical Analysis
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| MDPI | Multidisciplinary Digital Publishing Institute |
| DOAJ | Directory of Open Access Journals |
| TLA | Three Letter Acronym |
| LD | linear Dichroism |
References
- Katoh, H.; Yamashita, K.; Enomoto, T.; Watanabe, M. Classification and general considerations of thyroid cancer. Ann. Clin. Pathol. 2015, 3, 1–9. [Google Scholar]
- Dralle, H.; Machens, A.; Basa, J.; Fatourechi, V.; Franceschi, S.; Hay, I.D.; Nikiforov, Y.E.; Pacini, F.; Pasieka, J.L.; Sherman, S.I. Follicular cell-derived thyroid cancer. Nat. Rev. Dis. Prim. 2015, 1, 15077. [Google Scholar] [CrossRef] [PubMed]
- Paschke, R.; Lincke, T.; Müller, S.P.; Kreissl, M.C.; Dralle, H.; Fassnacht, M. The treatment of well-differentiated thyroid carcinoma. Dtsch. Arztebl. Int. 2015, 112, 452–458. [Google Scholar] [PubMed]
- Nixon, I.J.; Shaha, A.R. Management of regional nodes in thyroid cancer. Oral Oncol. 2013, 49, 671–675. [Google Scholar] [CrossRef] [PubMed]
- Shaha, A.R. Recurrent differentiated thyroid cancer. Endocr. Pract. 2012, 18, 600–603. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, S.M.; Fallahi, P.; Politti, U.; Materazzi, G.; Baldini, E.; Ulisse, S.; Miccoli, P.; Antonelli, A. Molecular targeted therapies of aggressive thyroid cancer. Front Endocrinol. 2015, 6, 176. [Google Scholar] [CrossRef] [PubMed]
- Cabanillas, M.E.; Dadu, R.; Hu, M.I.; Lu, C.; Gunn, G.B.; Grubbs, E.G.; Lai, S.Y.; Williams, M.D. Thyroid gland malignancies. Hematol. Oncol. Clin. N. Am. 2015, 29, 1123–1143. [Google Scholar] [CrossRef] [PubMed]
- Wendler, J.; Kroiss, M.; Gast, K.; Kreissl, M.C.; Allelein, S.; Lichtenauer, U.; Blaser, R.; Spitzweg, C.; Fassnacht, M.; Schott, M.; et al. Clinical presentation, treatment and outcome of anaplastic thyroid carcinoma: Results of a multicenter study in Germany. Eur. J. Endocrinol. 2016, 175, 521–529. [Google Scholar] [CrossRef] [PubMed]
- Asimakopoulos, P.; Nixon, I.J.; Shaha, A.R. Differentiated and medullary thyroid cancer: Surgical management of cervical lymph nodes. Clin. Oncol. 2017, 29, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Mizrachi, A.; Shaha, A.R. Lymph node dissection for differentiated thyroid cancer. Mol. Imaging Radionucl. Ther. 2016, 26, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Schob, S.; Meyer, J.; Gawlitza, M.; Frydrychowicz, C.; Müller, W.; Preuss, M.; Bure, L.; Quäschling, U.; Hoffmann, K.-T.; Surov, A. Diffusion-weighted MRI reflects proliferative activity in primary CNS lymphoma. PLoS ONE 2016, 11, e0161386. [Google Scholar] [CrossRef] [PubMed]
- Surov, A.; Stumpp, P.; Meyer, H.J.; Gawlitza, M.; Höhn, A.-K.; Boehm, A.; Sabri, O.; Kahn, T.; Purz, S. Simultaneous 18F-FDG-PET/MRI: Associations between diffusion, glucose metabolism and histopathological parameters in patients with head and neck squamous cell carcinoma. Oral Oncol. 2016, 58, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Khizer, A.T.; Raza, S.; Slehria, A.-U.-R. Diffusion-weighted MR imaging and ADC mapping in differentiating benign from malignant thyroid nodules. J. Coll. Physicians Surg. Pak. 2015, 25, 785–788. [Google Scholar] [PubMed]
- Lu, Y.; Moreira, A.L.; Hatzoglou, V.; Stambuk, H.E.; Gonen, M.; Mazaheri, Y.; Deasy, J.O.; Shaha, A.R.; Tuttle, R.M.; Shukla-Dave, A. Using diffusion-weighted MRI to predict aggressive histological features in papillary thyroid carcinoma: A novel tool for pre-operative risk stratification in thyroid cancer. Thyroid 2015, 25, 672–680. [Google Scholar] [CrossRef] [PubMed]
- Porter, D.A.; Heidemann, R.M. High resolution diffusion-weighted imaging using readout-segmented echo-planar imaging, parallel imaging and a two-dimensional navigator-based reacquisition. Magn. Reson. Med. 2009, 62, 468–475. [Google Scholar] [CrossRef] [PubMed]
- Schob, S.; Voigt, P.; Bure, L.; Meyer, H.J.; Wickenhauser, C.; Behrmann, C.; Höhn, A.; Kachel, P.; Dralle, H.; Hoffmann, K.-T.; Surov, A. Diffusion-weighted imaging using a readout-segmented, multishot EPI sequence at 3T distinguishes between morphologically differentiated and undifferentiated subtypes of thyroid carcinoma—A preliminary study. Transl. Oncol. 2016, 9, 403–410. [Google Scholar] [CrossRef] [PubMed]
- Just, N. Improving tumour heterogeneity MRI assessment with histograms. Br. J. Cancer 2014, 111, 2205–2213. [Google Scholar] [CrossRef] [PubMed]
- Hao, Y.; Pan, C.; Chen, W.; Li, T.; Zhu, W.; Qi, J. Differentiation between malignant and benign thyroid nodules and stratification of papillary thyroid cancer with aggressive histological features: Whole-lesion diffusion-weighted imaging histogram analysis. J. Magn. Reson. Imaging 2016, 44, 1546–1555. [Google Scholar] [CrossRef] [PubMed]
- Kierans, A.S.; Rusinek, H.; Lee, A.; Shaikh, M.B.; Triolo, M.; Huang, W.C.; Chandarana, H. Textural differences in apparent diffusion coefficient between low- and high-stage clear cell renal cell carcinoma. Am. J. Roentgenol. 2014, 203, W637–W644. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Liu, Y.; Xu, L.; Li, Z.; Lv, H.; Dong, N.; Li, W.; Yang, Z.; Wang, Z.; Jin, E. Application of texture analysis based on apparent diffusion coefficient maps in discriminating different stages of rectal cancer. J. Magn. Reson. Imaging 2016. [Google Scholar] [CrossRef] [PubMed]
- Nowosielski, M.; Recheis, W.; Goebel, G.; Güler, O.; Tinkhauser, G.; Kostron, H.; Schocke, M.; Gotwald, T.; Stockhammer, G.; Hutterer, M. ADC histograms predict response to anti-angiogenic therapy in patients with recurrent high-grade glioma. Neuroradiology 2011, 53, 291–302. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Liu, M.; Bao, J.; Xia, Y.; Zhang, J.; Zhang, L.; Huang, X.; Wang, J. The correlation between apparent diffusion coefficient and tumor cellularity in patients: A meta-analysis. PLoS ONE 2013, 8, e79008. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Sun, Y. Targeting p53 for novel anticancer therapy. Transl. Oncol. 2010, 3, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Godballe, C.; Asschenfeldt, P.; Jørgensen, K.E.; Bastholt, L.; Clausen, P.P.; Hansen, T.P.; Hansen, O.; Bentzen, S.M. Prognostic factors in papillary and follicular thyroid carcinomas: P53 expression is a significant indicator of prognosis. Laryngoscope 1998, 108, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Bachmann, K.; Pawliska, D.; Kaifi, J.; Schurr, P.; Zörb, J.; Mann, O.; Kahl, H.J.; Izbicki, J.R.; Strate, T. P53 is an independent prognostic factor for survival in thyroid cancer. Anticancer Res. 2006, 27, 3993–3997. [Google Scholar]
- Padhani, A.R.; Liu, G.; Mu-Koh, D.; Chenevert, T.L.; Thoeny, H.C.; Takahara, T.; Dzik-Jurasz, A.; Ross, B.D.; Van Cauteren, M.; Collins, D.; et al. Diffusion-weighted magnetic resonance imaging as a cancer biomarker: Consensus and recommendations. Neoplasia 2009, 11, 102–125. [Google Scholar] [CrossRef] [PubMed]
- Schlüter, C.; Duchrow, M.; Wohlenberg, C. The cell proliferation-associated antigen of antibody Ki-67: A very large, ubiquitous nuclear protein with numerous repeated elements, representing a new kind of cell cycle-maintaining proteins. J. Cell Biol. 1993, 123, 1–10. [Google Scholar] [CrossRef]
- Surov, A.; Caysa, H.; Wienke, A.; Spielmann, R.P.; Fiedler, E. Correlation between different ADC fractions, cell count, Ki-67, total nucleic areas and average nucleic areas in meningothelial meningiomas. Anticancer Res. 2015, 35, 6841–6846. [Google Scholar] [PubMed]
- Chen, L.; Zhang, J.; Chen, Y.; Wang, W.; Zhou, X.; Yan, X.; Wang, J. Relationship between apparent diffusion coefficient and tumour cellularity in lung cancer. PLoS ONE 2014, 9, e99865. [Google Scholar] [CrossRef] [PubMed]
- Chandarana, H.; Rosenkrantz, A.B.; Mussi, T.C.; Kim, S.; Ahmad, A.A.; Raj, S.D.; McMenamy, J.; Melamed, J.; Babb, J.S.; Kiefer, B.; et al. Histogram analysis of whole-lesion enhancement in differentiating clear cell from papillary subtype of renal cell cancer. Radiology 2012, 265, 790–798. [Google Scholar] [CrossRef] [PubMed]
- Surov, A.; Gottschling, S.; Mawrin, C.; Prell, J.; Spielmann, R.P.; Wienke, A.; Fiedler, E. Diffusion-weighted imaging in meningioma: Prediction of tumor grade and association with histopathological parameters. Transl. Oncol. 2015, 8, 517–523. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| DWI Related Parameters | Median | Range | Minimum–Maximum |
|---|---|---|---|
| ADCmean, ×10−5 mm2·s−1 | 124.30 | 90 | 73–163 |
| ADCmin, ×10−5 mm2·s−1 | 14.90 | 53 | 0.2–53 |
| ADCmax, ×10−5 mm2·s−1 | 250.70 | 179 | 147–325 |
| P10 ADC, ×10−5 mm2·s−1 | 72.10 | 85 | 30–114 |
| P25 ADC, ×10−5 mm2·s−1 | 91.90 | 84 | 52–136 |
| P75 ADC, ×10−5 mm2·s−1 | 140.40 | 99 | 93–192 |
| P90 ADC, ×10−5 mm2·s−1 | 172.82 | 116 | 97–213 |
| Median ADC, ×10−5 mm2·s−1 | 118.00 | 94 | 71–165 |
| Mode ADC, ×10−5 mm2·s−1 | 101.40 | 88 | 53–141 |
| Kurtosis | 3.64 | 1.90 | 2.89–4.79 |
| Skewness | 0.30 | 1.79 | −0.97–0.81 |
| Entropy | 3.27 | 1.98 | 2.75–4.72 |
| Parameters | Median | Range | Minimum–Maximum |
|---|---|---|---|
| Cell count, n | 1407 | 1808 | 439–2247 |
| Ki 67, % | 32.0 | 90 | 9–99 |
| p53, % | 4.0 | 94 | 0–94 |
| Total nuclear area, µm2 | 71,735 | 148,620 | 14,649–163,269 |
| Average nuclear area, µm2 | 53.0 | 61 | 33–94 |
| ADC Parameters and Histogram Values | Cell Count | p53 | Ki-67 | Total Nuclear Area | Average Nuclear Area |
|---|---|---|---|---|---|
| ADCmean, ×10−3 mm2·s−1 | r = 0.429 | r = 0.548 | r = −0.325 | r = 0.389 | r = 0.034 |
| p = 0.111 | p = 0.034 | p = 0.237 | p = 0.152 | p = 0.904 | |
| ADCmin, ×10−3 mm2·s−1 | r = 0.256 | r = 0.244 | r = −0.241 | r = 0.163 | r = −0.208 |
| p = 0.358 | p = 0.381 | p =0.386 | p = 0.562 | p = 0.456 | |
| ADCmax, ×10−3 mm2 s−1 | r = 0.372 | r = 0.645 | r = −0.646 | r = 0.461 | r = 0.155 |
| p = 0.173 | p = 0.009 | p = 0.009 | p = 0.084 | p = 0.580 | |
| ADC p10, ×10−3 mm2·s−1 | r = 0.361 | r = 0.409 | r = 0.289 | r = 0.275 | r = −0.079 |
| p = 0.187 | p =0.130 | p = 0.296 | p = 0.321 | p = 0.781 | |
| ADC p25, ×10−3 mm2·s−1 | r = 0.375 | r = 0.509 | r = 0.361 | r = 0.311 | r = −0.064 |
| p = 0.168 | p = 0.053 | p = 0.187 | p = 0.260 | p = 0.820 | |
| ADC p75, ×10−3 mm2·s−1 | r = 0.450 | r = 0.537 | r = −0.343 | r = 0.411 | r = 0.055 |
| p = 0.092 | p = 0.025 | p =0.211 | p =0.128 | p = 0.845 | |
| ADC p90, ×10−3 mm2·s−1 | r = 0.289 | r = 0.588 | r = −0.568 | r = 0.300 | r = 0.075 |
| p = 0.296 | p = 0.021 | p = 0.027 | p = 0.277 | p = 0.790 | |
| Median ADC, ×10−3 mm2·s−1 | r = 0.414 | r = 0.556 | r = −0.314 | r = 0.361 | r = −0.020 |
| p = 0.125 | p = 0.032 | p = 0.254 | p = 0.187 | p = 0.945 | |
| Mode ADC, ×10−3 mm2·s−1 | r = 0.496 | r = 0.534 | r = −0.357 | r = 0.432 | r = −0.149 |
| p = 0.060 | p = 0.040 | p = 0.191 | p = 0.108 | p = 0.682 | |
| Kurtosis | r = −0.571 | r = −0.262 | r = −0.314 | r = −0.411 | r = −0.182 |
| p = 0.026 | p =0.346 | p = 0.254 | p = 0.128 | p = 0.516 | |
| Skewness | r = −0.229 | r = −0.004 | r = −0.389 | r = 0.011 | r = 0.186 |
| p = 0.413 | p = 0.990 | p = 0.152 | p = 0.970 | p = 0.507 | |
| Entropy | r = 0.243 | r = −0.240 | r = 0.289 | r = 0.225 | r = 0.316 |
| p = 0.383 | p = 0.389 | p = 0.296 | p = 0.420 | p = 0.251 |
| ADC Parameters and Histogram Values | N0 Mean ± SD | N1/2 Mean ± SD | Group Comparison: p-Values | ||
|---|---|---|---|---|---|
| ADCmean, ×10−5 mm2·s−1 | 125.25 | 34.1 | 111.41 | 25.00 | 0.513 |
| ADCmin, ×10−5 mm2·s−1 | 28.26 | 17.30 | 14.02 | 16.90 | 0.075 |
| ADCmax, ×10−5 mm2·s−1 | 238.44 | 69.40 | 259.43 | 38.50 | 0.768 |
| P10 ADC, ×10−5 mm2·s−1 | 82.15 | 26.17 | 69.14 | 23.50 | 0.371 |
| P25 ADC, ×10−5 mm2·s−1 | 102.25 | 30.00 | 89.19 | 23.30 | 0.440 |
| P75 ADC, ×10−5 mm2·s−1 | 147.26 | 39.14 | 131.75 | 26.43 | 0.440 |
| P90 ADC, ×10−5 mm2·s−1 | 170.69 | 44.15 | 156.55 | 28.50 | 0.440 |
| Median ADC, ×10−5 mm2·s−1 | 124.14 | 34.86 | 109.19 | 25.50 | 0.513 |
| Mode ADC, ×10−5 mm2·s−1 | 112.32 | 25.56 | 101.39 | 27.50 | 0.594 |
| Kurtosis | 3.23 | 0.29 | 3.81 | 0.57 | 0.028 |
| Skewness | −0.12 | 0.64 | 0.41 | 0.21 | 0.031 |
| Entropy | 3.56 | 0.66 | 3.5 | 0.71 | 0.768 |
| Case | Age | Gender | Histological Subtype | Infiltration Pattern | M Stage | N Stage |
|---|---|---|---|---|---|---|
| 1 | 91 | female | anaplastic | trachea | 0 | 1 |
| 2 | 60 | female | papillary | trachea | 0 | 1 |
| 3 | 73 | male | papillary | trachea, esophagus | 0 | 1 |
| 4 | 68 | female | papillary | trachea, esophagus internal jugular vein | 0 | 0 |
| 5 | 73 | female | papillary | trachea | 0 | 1 |
| 6 | 67 | female | anaplastic | Trachea internal jugular vein | 1 | 2 |
| 7 | 73 | female | anaplastic | trachea, esophagus | 0 | 0 |
| 8 | 41 | female | follicular | trachea | 0 | 1 |
| 9 | 72 | female | anaplastic | none | 0 | 1 |
| 10 | 59 | female | anaplastic | trachea | 0 | 1 |
| 11 | 83 | female | papillary | trachea | 0 | 0 |
| 12 | 77 | female | follicular | trachea | 0 | 1 |
| 13 | 52 | female | anaplastic | trachea | 0 | 0 |
| 14 | 51 | female | follicular | trachea | 0 | 0 |
| 15 | 66 | female | anaplastic | trachea | 0 | 1 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schob, S.; Meyer, H.J.; Dieckow, J.; Pervinder, B.; Pazaitis, N.; Höhn, A.K.; Garnov, N.; Horvath-Rizea, D.; Hoffmann, K.-T.; Surov, A. Histogram Analysis of Diffusion Weighted Imaging at 3T is Useful for Prediction of Lymphatic Metastatic Spread, Proliferative Activity, and Cellularity in Thyroid Cancer. Int. J. Mol. Sci. 2017, 18, 821. https://doi.org/10.3390/ijms18040821
Schob S, Meyer HJ, Dieckow J, Pervinder B, Pazaitis N, Höhn AK, Garnov N, Horvath-Rizea D, Hoffmann K-T, Surov A. Histogram Analysis of Diffusion Weighted Imaging at 3T is Useful for Prediction of Lymphatic Metastatic Spread, Proliferative Activity, and Cellularity in Thyroid Cancer. International Journal of Molecular Sciences. 2017; 18(4):821. https://doi.org/10.3390/ijms18040821
Chicago/Turabian StyleSchob, Stefan, Hans Jonas Meyer, Julia Dieckow, Bhogal Pervinder, Nikolaos Pazaitis, Anne Kathrin Höhn, Nikita Garnov, Diana Horvath-Rizea, Karl-Titus Hoffmann, and Alexey Surov. 2017. "Histogram Analysis of Diffusion Weighted Imaging at 3T is Useful for Prediction of Lymphatic Metastatic Spread, Proliferative Activity, and Cellularity in Thyroid Cancer" International Journal of Molecular Sciences 18, no. 4: 821. https://doi.org/10.3390/ijms18040821
APA StyleSchob, S., Meyer, H. J., Dieckow, J., Pervinder, B., Pazaitis, N., Höhn, A. K., Garnov, N., Horvath-Rizea, D., Hoffmann, K. -T., & Surov, A. (2017). Histogram Analysis of Diffusion Weighted Imaging at 3T is Useful for Prediction of Lymphatic Metastatic Spread, Proliferative Activity, and Cellularity in Thyroid Cancer. International Journal of Molecular Sciences, 18(4), 821. https://doi.org/10.3390/ijms18040821