Update on the Impact of Omega 3 Fatty Acids on Inflammation, Insulin Resistance and Sarcopenia: A Review


Abstract
:1. Introduction
2. Results
2.1. Metabolic and Lipid Profile in Healthy, Elderly and Chronic Renal Failure
2.2. Metabolic and Lipid Profile in Impaired Glucose Metabolism (IGM) and T2DM
2.3. Inflammation and Oxidative Stress in in Healthy, Elderly and Chronic Renal Failure
2.4. Inflammation and Oxidative Stress in IGM, Diabetes, and Metabolic Syndrome
2.5. Muscle Mass and Function, and Whole-Body Energetics in Healthy, Elderly and Chronic Renal Failure
3. Discussion
3.1. Lipid and Metabolic Profile
3.2. Inflammatory Status and Oxidative Stress
3.3. Muscle Mass and Function, and Whole-Body Energetics
3.4. Limitations and Future Perspectives
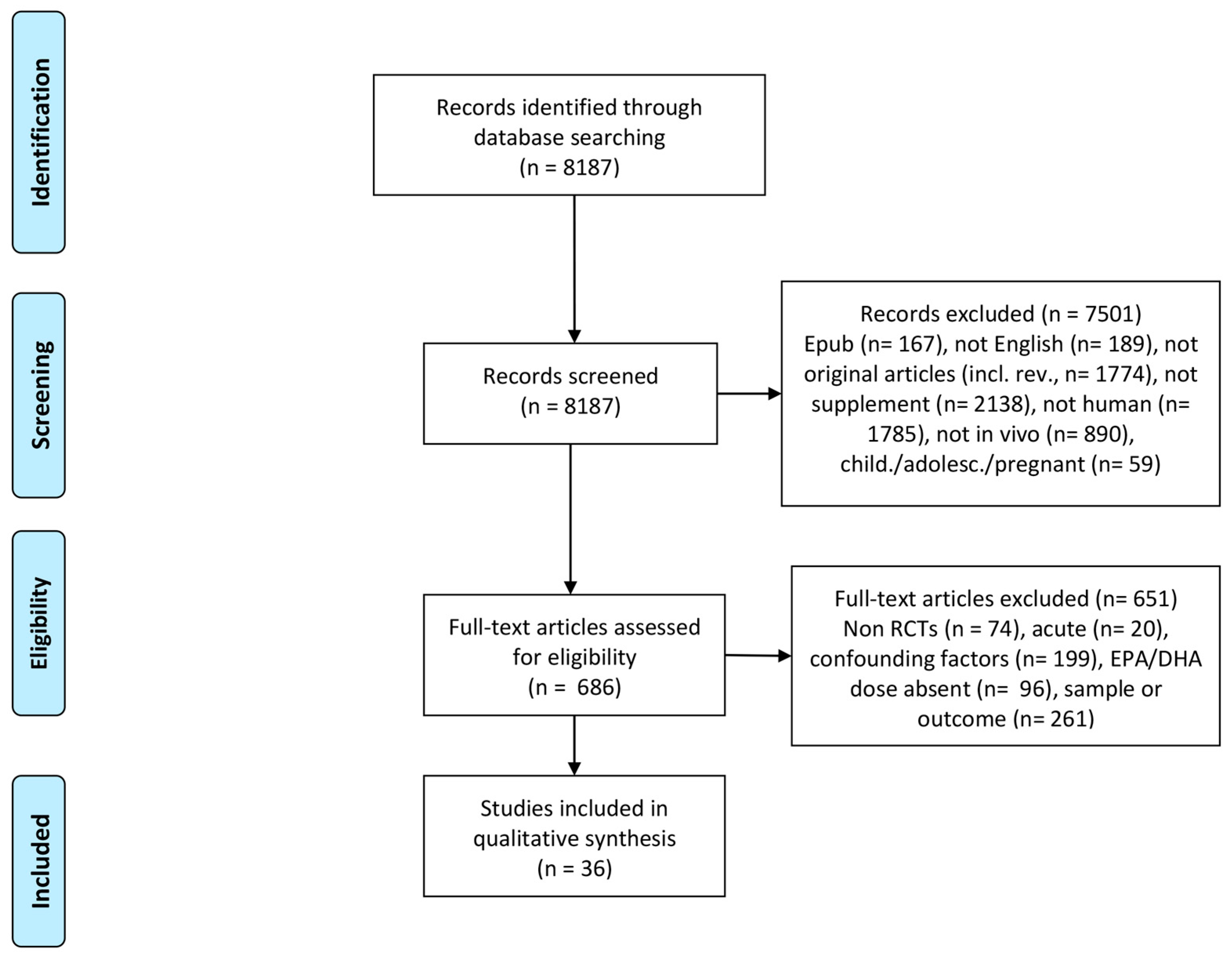
4. Methods
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Sinclair, A.J.; Abdelhafiz, A.H.; Rodriguez-Manas, L. Frailty and sarcopenia—Newly emerging and high impact complications of diabetes. J. Diabetes Complicat. 2017, 31, 1465–1473. [Google Scholar] [CrossRef] [PubMed]
- Chow, L.S.; Nair, K.S. Sarcopenia of male aging. Endocrinol. Metab. Clin. N. Am. 2005, 34, 833–852. [Google Scholar] [CrossRef] [PubMed]
- Johns, N.; Stephens, N.A.; Fearon, K.C.H. Muscle wasting in cancer. Int. J. Biochem. Cell Biol. 2013, 45, 2215–2229. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Nathan, J.A.; Goldberg, A.L. Muscle wasting in disease: Molecular mechanisms and promising therapies. Nat. Rev. Drug Discov. 2015, 14, 58–74. [Google Scholar] [CrossRef] [PubMed]
- Jo, E.; Lee, S.-R.; Park, B.-S.; Kim, J.-S. Potential mechanisms underlying the role of chronic inflammation in age-related muscle wasting. Aging Clin. Exp. Res. 2012, 24, 412–422. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Ballantyne, C.M. Skeletal muscle inflammation and insulin resistance in obesity. J. Clin. Investig. 2017, 127, 43–54. [Google Scholar] [CrossRef] [PubMed]
- Jackson, M.J. Reactive oxygen species in sarcopenia: Should we focus on excess oxidative damage or defective redox signalling? Mol. Asp. Med. 2016, 50, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Oh, S.-L.; Lee, S.-R.; Kim, J.-S. Effects of conjugated linoleic acid/n-3 and resistance training on muscle quality and expression of atrophy-related ubiquitin ligases in middle-aged mice with high-fat dietinduced obesity. J. Exerc. Nutr. Biochem. 2017, 21, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.I.; Atherton, P.; Reeds, D.N.; Mohammed, B.S.; Rankin, D.; Rennie, M.J.; Mittendorfer, B. Omega-3 polyunsaturated fatty acids augment the muscle protein anabolic response to hyperinsulinaemia-hyperaminoacidaemia in healthy young and middle-aged men and women. Clin. Sci. 2011, 121, 267–278. [Google Scholar] [CrossRef] [PubMed]
- Di Girolamo, F.G.; Situlin, R.; Mazzucco, S.; Valentini, R.; Toigo, G.; Biolo, G. Omega-3 fatty acids and protein metabolism: Enhancement of anabolic interventions for sarcopenia. Curr. Opin. Clin. Nutr. Metab. Care 2014, 17, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Farias, J.G.; Molina, V.M.; Carrasco, R.A.; Zepeda, A.B.; Figueroa, E.; Letelier, P.; Castillo, R.L. Antioxidant Therapeutic Strategies for Cardiovascular Conditions Associated with Oxidative Stress. Nutrients 2017, 9. [Google Scholar] [CrossRef] [PubMed]
- Calder, P.C. Omega-3 fatty acids and inflammatory processes: From molecules to man. Biochem. Soc. Trans. 2017, 45, 1105–1115. [Google Scholar] [CrossRef] [PubMed]
- Lucero, D.; Olano, C.; Bursztyn, M.; Morales, C.; Stranges, A.; Friedman, S.; Macri, E.V.; Schreier, L.; Zago, V. Supplementation with n-3, n-6, n-9 fatty acids in an insulin-resistance animal model: Does it improve VLDL quality? Food Funct. 2017, 8, 2053–2061. [Google Scholar] [CrossRef] [PubMed]
- Asztalos, I.B.; Gleason, J.A.; Sever, S.; Gedik, R.; Asztalos, B.F.; Horvath, K.V.; Dansinger, M.L.; Lamon-Fava, S.; Schaefer, E.J. Effects of eicosapentaenoic acid and docosahexaenoic acid on cardiovascular disease risk factors: A randomized clinical trial. Metabolism 2016, 65, 1636–1645. [Google Scholar] [CrossRef] [PubMed]
- Polus, A.; Zapala, B.; Razny, U.; Gielicz, A.; Kiec-Wilk, B.; Malczewska-Malec, M.; Sanak, M.; Childs, C.E.; Calder, P.C.; Dembinska-Kiec, A. Omega-3 fatty acid supplementation influences the whole blood transcriptome in women with obesity, associated with pro-resolving lipid mediator production. Biochim. Biophys. Acta 2016, 1861, 1746–1755. [Google Scholar] [CrossRef] [PubMed]
- Logan, S.L.; Spriet, L.L. Omega-3 Fatty Acid Supplementation for 12 Weeks Increases Resting and Exercise Metabolic Rate in Healthy Community-Dwelling Older Females. PLoS ONE 2015, 10, e0144828. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.I.; Julliand, S.; Reeds, D.N.; Sinacore, D.R.; Klein, S.; Mittendorfer, B. Fish oil-derived n-3 PUFA therapy increases muscle mass and function in healthy older adults. Am. J. Clin. Nutr. 2015, 102, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Alves Luzia, L.; Mendes Aldrighi, J.; Teixeira Damasceno, N.R.; Rodrigues Sampaio, G.; Aparecida Manolio Soares, R.; Tande Silva, I.; De Queiroz Mello, A.P.; Ferreira Carioca, A.A.; Ferraz da Silva Torres, E.A. Fish oil and vitamin e change lipid profiles and anti-LDL-antibodies in two different ethnic groups of women transitioning through menopause. Nutr. Hosp. 2015, 32, 165–174. [Google Scholar] [CrossRef] [PubMed]
- Moeinzadeh, F.; Shahidi, S.; Mortazavi, M.; Dolatkhah, S.; Kajbaf, M.; Haghjooy Javanmard, S.; Moghtaderi, A. Effects of Omega-3 Fatty Acid Supplementation on Serum Biomarkers, Inflammatory Agents, and Quality of Life of Patients on Hemodialysis. Iran. J. Kidney Dis. 2016, 10, 381–387. [Google Scholar] [PubMed]
- Kajbaf, M.H.; Khorvash, F.; Mortazavi, M.; Shahidi, S.; Moeinzadeh, F.; Farajzadegan, Z.; Tirani, S.A. Does Omega-3 supplementation decrease carotid intima-media thickening in hemodialysis patients? J. Res. Pharm. Pract. 2016, 5, 252–256. [Google Scholar] [CrossRef] [PubMed]
- Gharekhani, A.; Dashti-Khavidaki, S.; Lessan-Pezeshki, M.; Khatami, M.-R. Potential Effects of Omega-3 Fatty Acids on Insulin Resistance and Lipid Profile in Maintenance Hemodialysis Patients: A Randomized Placebo-Controlled Trial. Iran. J. Kidney Dis. 2016, 10, 310–318. [Google Scholar] [PubMed]
- Deger, S.M.; Hung, A.M.; Ellis, C.D.; Booker, C.; Bian, A.; Chen, G.; Abumrad, N.N.; Ikizler, T.A. High Dose Omega-3 Fatty Acid Administration and Skeletal Muscle Protein Turnover in Maintenance Hemodialysis Patients. Clin. J. Am. Soc. Nephrol. 2016, 11, 1227–1235. [Google Scholar] [CrossRef] [PubMed]
- Omrani, H.R.; Pasdar, Y.; Raisi, D.; Najafi, F.; Esfandiari, A. The effect of omega-3 on serum lipid profile in hemodialysis patients. J. Ren. Inj. Prev. 2015, 4, 68–72. [Google Scholar] [CrossRef] [PubMed]
- Naini, A.E.; Asiabi, R.E.K.; Keivandarian, N.; Moeinzadeh, F. Effect of omega-3 supplementation on inflammatory parameters in patients on chronic ambulatory peritoneal dialysis. Adv. Biomed. Res. 2015, 4, 167. [Google Scholar] [CrossRef] [PubMed]
- Taheri, S.; Keyvandarian, N.; Moeinzadeh, F.; Mortazavi, M.; Naini, A.E. The effect of omega-3 fatty acid supplementation on oxidative stress in continuous ambulatory peritoneal dialysis patients. Adv. Biomed. Res. 2014, 3, 143. [Google Scholar] [CrossRef] [PubMed]
- Naini, A.E.; Keyvandarian, N.; Mortazavi, M.; Taheri, S.; Hosseini, S.M. Effect of Omega-3 fatty acids on blood pressure and serum lipids in continuous ambulatory peritoneal dialysis patients. J. Res. Pharm. Pract. 2015, 4, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Sawada, T.; Tsubata, H.; Hashimoto, N.; Takabe, M.; Miyata, T.; Aoki, K.; Yamashita, S.; Oishi, S.; Osue, T.; Yokoi, K.; et al. Effects of 6-month eicosapentaenoic acid treatment on postprandial hyperglycemia, hyperlipidemia, insulin secretion ability, and concomitant endothelial dysfunction among newly-diagnosed impaired glucose metabolism patients with coronary artery disease. A. Cardiovasc. Diabetol. 2016, 15, 121. [Google Scholar] [CrossRef] [PubMed]
- Clark, L.F.; Thivierge, M.C.; Kidd, C.A.; McGeoch, S.C.; Abraham, P.; Pearson, D.W.M.; Horgan, G.W.; Holtrop, G.; Thies, F.; Lobley, G.E. Fish oil supplemented for 9 months does not improve glycaemic control or insulin sensitivity in subjects with impaired glucose regulation: A parallel randomised controlled trial. Br. J. Nutr. 2016, 115, 75–86. [Google Scholar] [CrossRef] [PubMed]
- Poreba, M.; Mostowik, M.; Siniarski, A.; Golebiowska-Wiatrak, R.; Malinowski, K.P.; Haberka, M.; Konduracka, E.; Nessler, J.; Undas, A.; Gajos, G. Treatment with high-dose n-3 PUFAs has no effect on platelet function, coagulation, metabolic status or inflammation in patients with atherosclerosis and type 2 diabetes. Cardiovasc. Diabetol. 2017, 16, 50. [Google Scholar] [CrossRef] [PubMed]
- Toorang, F.; Djazayery, A.; Djalali, M. Effects of Omega-3 Fatty Acids Supplement on Antioxidant Enzymes Activity in Type 2 Diabetic Patients. Iran. J. Public Health 2016, 45, 340–345. [Google Scholar] [PubMed]
- Farahbakhsh-Farsi, P.; Djazayery, A.; Eshraghian, M.R.; Koohdani, F.; Zarei, M.; Javanbakht, M.H.; Derakhshanian, H.; Djalali, M. Effect of Omega-3 Supplementation on Lipocalin 2 and Retinol-Binding Protein 4 in Type 2 Diabetic Patients. Iran. J. Public Health 2016, 45, 179–185. [Google Scholar] [PubMed]
- Veleba, J.; Kopecky, J.J.; Janovska, P.; Kuda, O.; Horakova, O.; Malinska, H.; Kazdova, L.; Oliyarnyk, O.; Skop, V.; Trnovska, J.; et al. Combined intervention with pioglitazone and n-3 fatty acids in metformin-treated type 2 diabetic patients: Improvement of lipid metabolism. Nutr. Metab. 2015, 12, 52. [Google Scholar] [CrossRef] [PubMed]
- Dasarathy, S.; Dasarathy, J.; Khiyami, A.; Yerian, L.; Hawkins, C.; Sargent, R.; McCullough, A.J. Double-blind randomized placebo-controlled clinical trial of omega 3 fatty acids for the treatment of diabetic patients with nonalcoholic steatohepatitis. J. Clin. Gastroenterol. 2015, 49, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.C.; Ivester, P.; Hester, A.G.; Sergeant, S.; Case, L.D.; Morgan, T.; Kouba, E.O.; Chilton, F.H. The impact of polyunsaturated fatty acid-based dietary supplements on disease biomarkers in a metabolic syndrome/diabetes population. Lipids Health Dis. 2014, 13, 196. [Google Scholar] [CrossRef] [PubMed]
- Venturini, D.; Simao, A.N.C.; Urbano, M.R.; Dichi, I. Effects of extra virgin olive oil and fish oil on lipid profile and oxidative stress in patients with metabolic syndrome. Nutrition 2015, 31, 834–840. [Google Scholar] [CrossRef] [PubMed]
- Simao, A.N.C.; Lozovoy, M.A.B.; Dichi, I. Effect of soy product kinako and fish oil on serum lipids and glucose metabolism in women with metabolic syndrome. Nutrition 2014, 30, 112–115. [Google Scholar] [CrossRef] [PubMed]
- Muldoon, M.F.; Laderian, B.; Kuan, D.C.H.; Sereika, S.M.; Marsland, A.L.; Manuck, S.B. Fish oil supplementation does not lower C-reactive protein or interleukin-6 levels in healthy adults. J. Intern. Med. 2016, 279, 98–109. [Google Scholar] [CrossRef] [PubMed]
- Flock, M.R.; Skulas-Ray, A.C.; Harris, W.S.; Gaugler, T.L.; Fleming, J.A.; Kris-Etherton, P.M. Effects of supplemental long-chain omega-3 fatty acids and erythrocyte membrane fatty acid content on circulating inflammatory markers in a randomized controlled trial of healthy adults. Prostaglandins Leukot. Essent. Fatty Acids 2014, 91, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Bo, Y.; Zhang, X.; Wang, Y.; You, J.; Cui, H.; Zhu, Y.; Pang, W.; Liu, W.; Jiang, Y.; Lu, Q. The n-3 Polyunsaturated Fatty Acids Supplementation Improved the Cognitive Function in the Chinese Elderly with Mild Cognitive Impairment: A Double-Blind Randomized Controlled Trial. Nutrients 2017, 9. [Google Scholar] [CrossRef] [PubMed]
- Gharekhani, A.; Khatami, M.-R.; Dashti-Khavidaki, S.; Razeghi, E.; Noorbala, A.-A.; Hashemi-Nazari, S.-S.; Mansournia, M.-A. The effect of omega-3 fatty acids on depressive symptoms and inflammatory markers in maintenance hemodialysis patients: A randomized, placebo-controlled clinical trial. Eur. J. Clin. Pharmacol. 2014, 70, 655–665. [Google Scholar] [CrossRef] [PubMed]
- Gharekhani, A.; Khatami, M.-R.; Dashti-Khavidaki, S.; Razeghi, E.; Abdollahi, A.; Hashemi-Nazari, S.-S.; Mansournia, M.-A. Potential effects of omega-3 fatty acids on anemia and inflammatory markers in maintenance hemodialysis patients. DARU J. Pharm. Sci. 2014, 22, 11. [Google Scholar] [CrossRef] [PubMed]
- Asemi, Z.; Soleimani, A.; Shakeri, H.; Mazroii, N.; Esmaillzadeh, A. Effects of omega-3 fatty acid plus alpha-tocopherol supplementation on malnutrition-inflammation score, biomarkers of inflammation and oxidative stress in chronic hemodialysis patients. Int. Urol. Nephrol. 2016, 48, 1887–1895. [Google Scholar] [CrossRef] [PubMed]
- Barden, A.; O’Callaghan, N.; Burke, V.; Mas, E.; Beilin, L.J.; Fenech, M.; Irish, A.B.; Watts, G.F.; Puddey, I.B.; Huang, R.-C.; et al. n-3 Fatty Acid Supplementation and Leukocyte Telomere Length in Patients with Chronic Kidney Disease. Nutrients 2016, 8, 175. [Google Scholar] [CrossRef] [PubMed]
- Azizi-Soleiman, F.; Jazayeri, S.; Eghtesadi, S.; Rajab, A.; Heidari, I.; Vafa, M.R.; Gohari, M.R. Effects of pure eicosapentaenoic and docosahexaenoic acids on oxidative stress, inflammation and body fat mass in patients with type 2 diabetes. Int. J. Prev. Med. 2013, 4, 922–928. [Google Scholar] [PubMed]
- Mocking, R.J.T.; Assies, J.; Bot, M.; Jansen, E.H.J.M.; Schene, A.H.; Pouwer, F. Biological effects of add-on eicosapentaenoic acid supplementation in diabetes mellitus and co-morbid depression: A randomized controlled trial. PLoS ONE 2012, 7, e49431. [Google Scholar] [CrossRef] [PubMed]
- Bostock, E.L.; Morse, C.I.; Winwood, K.; McEwan, I.M.; Onambele, G.L. Omega-3 Fatty Acids and Vitamin D in Immobilisation: Part B- Modulation of Muscle Functional, Vascular and Activation Profiles. J. Nutr. Health Aging 2017, 21, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Bostock, E.L.; Morse, C.I.; Winwood, K.; McEwan, I.M.; Onambélé-Pearson, G.L. Omega-3 fatty acids and vitamin D in immobilisation: Part A—Modulation of appendicular mass content, composition and structure. J. Nutr. Health Aging 2017, 21, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Gerling, C.J.; Whitfield, J.; Mukai, K.; Spriet, L.L. Variable effects of 12 weeks of omega-3 supplementation on resting skeletal muscle metabolism. Appl. Physiol. Nutr. Metab. 2014, 39, 1083–1091. [Google Scholar] [CrossRef] [PubMed]
- Krzyminska-Siemaszko, R.; Czepulis, N.; Lewandowicz, M.; Zasadzka, E.; Suwalska, A.; Witowski, J.; Wieczorowska-Tobis, K. The Effect of a 12-Week Omega-3 Supplementation on Body Composition, Muscle Strength and Physical Performance in Elderly Individuals with Decreased Muscle Mass. Int. J. Environ. Res. Public Health 2015, 12, 10558–10574. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Rimm, E.B. Fish intake, contaminants, and human health: Evaluating the risks and the benefits. JAMA 2006, 296, 1885–1899. [Google Scholar] [CrossRef] [PubMed]
- Sharp, R.P.; Gales, B.J.; Sirajuddin, R. Comparing the Impact of Prescription Omega-3 Fatty Acid Products on Low-Density Lipoprotein Cholesterol. Am. J. Cardiovasc. Drugs 2017. [Google Scholar] [CrossRef] [PubMed]
- Wei, M.Y.; Jacobson, T.A. Effects of eicosapentaenoic acid versus docosahexaenoic acid on serum lipids: A systematic review and meta-analysis. Curr. Atheroscler. Rep. 2011, 13, 474–483. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, T.A.; Glickstein, S.B.; Rowe, J.D.; Soni, P.N. Effects of eicosapentaenoic acid and docosahexaenoic acid on low-density lipoprotein cholesterol and other lipids: A review. J. Clin. Lipidol. 2012, 6, 5–18. [Google Scholar] [CrossRef] [PubMed]
- Mori, T.A.; Burke, V.; Puddey, I.B.; Watts, G.F.; O’Neal, D.N.; Best, J.D.; Beilin, L.J. Purified eicosapentaenoic and docosahexaenoic acids have differential effects on serum lipids and lipoproteins, LDL particle size, glucose, and insulin in mildly hyperlipidemic men. Am. J. Clin. Nutr. 2000, 71, 1085–1094. [Google Scholar] [PubMed]
- Abbott, K.A.; Burrows, T.L.; Thota, R.N.; Acharya, S.; Garg, M.L. Do omega-3 PUFAs affect insulin resistance in a sex-specific manner? A systematic review and meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 2016, 104, 1470–1484. [Google Scholar] [CrossRef] [PubMed]
- Endres, S.; Ghorbani, R.; Kelley, V.E.; Georgilis, K.; Lonnemann, G.; van der Meer, J.W.; Cannon, J.G.; Rogers, T.S.; Klempner, M.S.; Weber, P.C. The effect of dietary supplementation with n-3 polyunsaturated fatty acids on the synthesis of interleukin-1 and tumor necrosis factor by mononuclear cells. N. Engl. J. Med. 1989, 320, 265–271. [Google Scholar] [CrossRef] [PubMed]
- Akchurin, O.M.; Kaskel, F. Update on inflammation in chronic kidney disease. Blood Purif. 2015, 39, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Yoshino, J.; Smith, G.I.; Kelly, S.C.; Julliand, S.; Reeds, D.N.; Mittendorfer, B. Effect of dietary n-3 PUFA supplementation on the muscle transcriptome in older adults. Physiol. Rep. 2016, 4. [Google Scholar] [CrossRef] [PubMed]
- Jankowska, M.; Cobo, G.; Lindholm, B.; Stenvinkel, P. Inflammation and Protein-Energy Wasting in the Uremic Milieu. Contrib. Nephrol. 2017, 191, 58–71. [Google Scholar] [CrossRef] [PubMed]
- Rice, H.B.; Bernasconi, A.; Maki, K.C.; Harris, W.S.; von Schacky, C.; Calder, P.C. Conducting omega-3 clinical trials with cardiovascular outcomes: Proceedings of a workshop held at ISSFAL 2014. Prostaglandins Leukot. Essent. Fatty Acids 2016, 107, 30–42. [Google Scholar] [CrossRef] [PubMed]
- Jeromson, S.; Gallagher, I.J.; Galloway, S.D.R.; Hamilton, D.L. Omega-3 Fatty Acids and Skeletal Muscle Health. Mar. Drugs 2015, 13, 6977–7004. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study | Sample (n) | Protocol | Key Findings |
|---|---|---|---|
| Asztalos et al., 2016 [14] | Healthy (121) | 600 EPA mg vs. 1800 mg EPA vs. 600 mg DHA daily vs. placebo, 6 weeks | High dose EPA decreased TRL fasted (−14.6%) and TRL post prandial (−12.6%) DHA decreased postprandial TG (−20.0%), and increased fasting and postprandial LDL (18.4%) No effect of low dose EPA |
| Polus et al., 2016 [15] | Obese women (59) | 360 mg EPA and 1290 mg DHA daily vs. placebo, 3 months | Decreased fasting TG (−17.6%) and insulin (−12.1%) No effect on NEFA, TC, HDL, LDL, FBG |
| Logan & Spriet, 2015 [16] | Elderly women (24) | 360 mg EPA + 1290 mg DHA daily vs. placebo, 12 weeks | Decreased TG (−29%) No effect on insulin or FBG |
| Smith et al., 2015 [17] | Elderly (60) | 1860 mg EPA + 1500 mg DHA daily vs. placebo, 6 months | No effect on TG, HDL, LDL, FBG |
| Alves Luzia et al., 2015 [18] | Menopause women (74) | 540 mg EPA + 360 mg DHA + 400 vit E (or placebo) daily vs. placebo, 3 months | Decreased TC in omega 3 group (−5.4%), omega 3 + vit E (−7.5%) and control (−1.0%). Decreased LDL in omega 3 (−8.4%) and omega 3 + vit E (−7.3%), increased LDL in control (8.3%) |
| Moeinzadeh et al., 2016 [19] | Hemodialysis (52) | 540 mg EPA + 360 mg DHA daily vs. placebo, 6 months | No effect on serum albumin, LDL, TC, and TG |
| Kajbaf et al., 2016 [20] | Hemodialysis (54) | 540 mg EPA + 360 mg DHA daily vs. placebo, 6 months | Increased HDL (27.5%) and increased urea reduction ratio (1.54%) No effect on serum albumin, LDL, TC, and TG |
| Gharekhani et al., 2016 [21] | Hemodialysis (54) | 1080 mg EPA + 720 mg DHA daily vs. placebo, 4 months | Decreased serum TC (−5.37%) and HDL (−30.9%). TG reduced only compared to placebo No effect on insulin, leptin, adiponectin, FPG, LDL, HOMA-IR |
| Deger et al., 2016 [22] | Hemodialysis (20) | 1914 mg EPA + 957 mg DHA daily vs. placebo, 12 weeks | No effect on FBG and HOMA-IR |
| Omrani et al., 2015 [23] | Hemodialysis (60) | 80 mg EPA + 120 mg DHA daily vs. placebo, 10 weeks | Reduced TC in both experimental (−23.9%) and control (−7.7%) group No effect on HDL, LDL, and TG |
| Naini et al., 2015 [26] | CAPD (90) | 540 mg EPA + 360 mg DHA daily vs. placebo, 8 weeks | No effect on serum TG, TC, HDL, and LDL |
| Taheri et al., 2014 [25] | CAPD (90) | 540 mg EPA + 360 mg DHA daily vs. placebo, 8 weeks | No effect on lipid profile |
| Study | Sample (n) | Protocol | Key Findings |
|---|---|---|---|
| Sawada et al., 2016 [27] | IGM (107) | 1800 mg EPA daily vs. placebo, 6 months | Increased HDL (5.1%) and reduced fasting TG (−25.3%) No effect on HbA1c and FBG |
| Clark et al., 2016 [28] | IGM (36) | 2388 mg EPA + 1530 mg DHA daily vs. placebo, 9 months | Increased total protein disposal (9.6%) and endogenous whole-body protein turnover (10.4%) under insulin-stimulated conditions No effect on FBG, insulin, HOMA-IR. No effect on total glucose disposal during hyperinsulinaemic-euglycaemic-euaminoacidaemic clamp |
| Poreba et al., 2017 [29] | T2DM (74) | 1000 mg EPA + 1000 mg DHA daily vs. placebo, 3 months | No effect on insulin, HbA1c, adiponectin, leptin, and lipid levels |
| Toorang et al., 2016 [30] | T2DM (90) | 1548 mg EPA + 828 mg DHA daily vs. placebo, 2 months | Decreased HbA1c (−8.2%) |
| Farahbakhsh-Farsi et al., 2016 [31] | T2DM (45) | 310 mg EPA + 210 mg DHA daily vs. placebo, 10 weeks | Reduced retinol-binding protein 4 (−42.5%) |
| Veleba et al., 2015 [32] | T2DM (60) | 750 mg EPA and 2000 mg DHA + 15 mg Pio (or PLACEBO) daily vs. 15 mg Pio daily vs. PLACEBO, 24 weeks | Increased HbA1c (14.7%) and FBG (17.0%) No effect on TG, TC, HDL, LDL, NEFA, Leptin, Adiponectin |
| Dasarthy et al., 2015 [33] | T2DM with NASH (37) | 2160 mg EPA + 1440 mg DHA daily vs. placebo,48 weeks | Increased FBG (15.8%), HOMA (34.2%), and HbA1c (6.4%) No effect on TG, HDL and TC |
| Lee et al., 2014 [34] | MetS (59) | 3580 mg EPA + 2440 mg DHA daily vs. placebo, 8 weeks | Reduced TG (−16.0%) and HbA1c (−3.0%), increased insulin (29.8%) and HDL (7.1%) |
| Venturini et al., 2015 [35] | MetS (102) | 1800 mg EPA + 1200 mg DHA + 10 mL extra virgin oil (or PLACEBO) daily vs. 10 mL extra virgin oil daily vs. placebo, 90 days | No effect on TG, TC, HDL, LDL, FBG, insulin, HOMA-IR |
| Simao et al., 2014 [36] | MetS (65) | 1800 mg EPA + 1200 mg DHA + 29 g kinako (or PLACEBO) daily vs. 29 g kinako daily vs. placebo, 90 days | Decreased TG (−20.0%), increased TC (7.7%), LDL (18.6%), FBG (10.5%), fasting insulin (18.3%), and HOMA-IR (13.4%) No effect on HDL |
| Author (Year) | Sample (n) | Treatment | Key Findings |
|---|---|---|---|
| Asztalos et al., 2016 [14] | Healthy (121) | 600 mg EPA vs. 1800 mg EPA vs. 600 mg DHA daily vs. placebo, 6 weeks | High dose EPA reduced Lp-PLA2 (−14.1%) No effect of low dose EPA or DHA |
| Muldoon et al., 2016 [37] | Healthy (261) | 1000 mg EPA + 400 mg DHA daily vs. placebo, 18 weeks | No effect on serum CRP and IL-6 |
| Flock et al., 2014 [38] | Healthy (125) | 300 mg EPA + DHA vs. 600 mg EPA + DHA vs. 900 mg EPA + DHA vs. 1800 mg EPA + DHA daily vs. placebo, 5 months | No dose-response effect on IL-6, TNF-α and CRP |
| Polus et al., 2016 [15] | Obese women (59) | 360 mg EPA and 1290 mg DHA daily vs. placebo, 3 months | Decreased sVCAM-1 (−4.1%), sPECAM-1 (−8.4%) and hsCRP (−20.3%) No effect on IL-6 |
| Bo et al., 2017 [39] | Elderly with mild cognitive impairment (86) | 720 mg EPA + 480 mg DHA daily vs. placebo, 6 months | Decreased IL-6 (−29.0%), TNF-α (−31.1%), and sPLA2 activity (−11.3%) No effect on IL-10, COX and LOX |
| Alves Luzia et al., 2015 [18] | Menopause women (74) | 540 mg EPA + 360 mg DHA + 400 mg vit E (or placebo) daily vs. placebo, 3 months | Increased TBARS (125%) |
| Moeinzadeh et al., 2016 [19] | Hemodialysis (52) | 540 mg EPA + 360 mg DHA daily vs. placebo, 6 months | Decreased VCAM (−37.5%) |
| Gharekhani et al., 2016 [21] | Hemodialysis (54) | 1080 mg EPA + 720 mg DHA daily vs. placebo, 4 months | No effect on CRP |
| Deger et al., 2016 [22] | Hemodialysis (20) | 1914 mg EPA + 957 mg DHA daily vs. placebo, 12 months | No effect on serum hsCRP and IL-6 |
| Gharekhani et al., 2014 [41] | Hemodialysis (54) | 1080 mg EPA + 720 mg DHA daily vs. placebo, 4 months | Increased IL10 to IL-6 ratio (48.5%), reduced IL-6 (−5.2%) |
| Asemi et al., 2016 [42] | Hemodialysis (120) | 1600 mg EPA + 300 mg DHA + 400 IU Alphatocopherol (or placebo) daily vs. placebo, 12 weeks | Increased NO (59.3%) and TAC (4.77%) No effect on albumin, hsCRP, GSH, and MDA |
| Barden et al., 2016 [43] | CKD (85) | 1840 mg EPA + 1520 mg DHA + 200 mg CoQ (or PLACEBO) daily vs. placebo, 8 weeks | Reduced F2-isoprostanes (−29.1%) |
| Naini et al., 2015 [24] | CAPD (40) | 540 mg EPA + 360 mg DHA daily vs. placebo, 2 months | No effect on CRP and IL-6 |
| Taheri et al., 2014 [25] | CAPD (90) | 540 mg EPA + 360 mg DHA daily vs. placebo, 8 weeks | No effect on SOD and GSH |
| Author (Year) | Sample (n) | Treatment | Key Findings |
|---|---|---|---|
| Sawada et al., 2016 [27] | IGM (2016) | 1800 mg EPA daily vs. placebo, 6 months | Reduced CRP (−10%), similar effects in placebo |
| Clark et al., 2016 [28] | IGM (36) | 2388 mg EPA + 1530 mg DHA daily vs. placebo, 9 months | No effect in IL-1B, IL-6, hsCRP, sICAM and VCAM |
| Poreba et al., 2017 [29] | T2DM (74) | 1000 mg EPA + 1000 mg DHA daily vs. placebo, 3 months | No effect on markers of systemic inflammation |
| Azizi-Soleiman et al., 2013 [44] | T2DM (60) | 1000 mg EPA vs. 1000 mg DHA daily vs. placebo, 12 weeks | No effect on serum CRP and MDA |
| Mocking et al., 2012 [45] | T2DM (24) | 900 mg EPA daily vs. placebo, 12 weeks | No effect on oxidative stress and inflammatory parameters |
| Veleba et al., 2015 [32] | T2DM (60) | 2800 mg EPA + DHA + 15 mg Pio (or placebo) vs. 15 mg Pio daily vs. placebo, 24 weeks | No effect on SOD, TBARS, GSSG/GSH |
| Venturini et al., 2015 [35] | MetS (102) | 1800 mg EPA + 1200 mg DHA + 10 mL extra virgin oil (or placebo) vs. 10 mL extra viring oil daily vs. placebo, 90 days | No effect on CRP and oxidative stress parameters |
| Author (Year) | Sample (n) | Treatment | Key findings |
|---|---|---|---|
| Bostock et al., 2017a and 2017b [46,47] | Healthy (24) | 1770 mg EPA + 390 mg DHA vs. 1000 IU vit D daily vs. placebo, 2 weeks | No effect on declines in muscle thickness and torque associated with immobilisation |
| Gerling et al., 2014 [48] | Healthy (30) | 2000 mg EPA + 1000 mg DHA daily vs. placebo, 12 weeks | Increased long form of UCP3 (11%) No effect on whole muscle, sarcolemmal, or mitochondrial FAT/CD36, FABPpm, FATP1 and FATP4, or mitochondrial electron chain and PDH proteins |
| Logan and Spriet, 2015 [16] | Elderly women (24) | 360 mg EPA + 1290 mg DHA daily vs. placebo, 12 weeks | Increased resting metabolic rate (14%), energy expenditure during exercise (10%), rate of fat oxidation during rest (19%) and during exercise (27%), increased lean body mass (4%) and functional capacity (7%) |
| Smith et al., 2015 [17] | Elderly (60) | 1860 mg EPA + 1500 mg DHA daily vs. placebo, 6 months | Increased thigh muscle volume (3.6%), handgrip strength (6.6%), and 1-RM muscle strength (4.0%) |
| Lrzyminska-Siemaszko et al., 2015 [49] | Elderly (53) | 660 mg EPA + 440 mg DHA + 10 mg vit E vs. placebo + 10 mg vit E, 12 weeks | No effect on muscle mass, hand grip, and TUG |
| Deger et al., 2016 [22] | Hemodialysis (20) | 1914 mg EPA + 957 mg DHA daily vs. placebo, 12 weeks | Decreased forearm muscle protein breakdown (−42.5%) No effect on forearm muscle net protein balance or synthesis, and whole-body protein synthesis or breakdown |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buoite Stella, A.; Gortan Cappellari, G.; Barazzoni, R.; Zanetti, M. Update on the Impact of Omega 3 Fatty Acids on Inflammation, Insulin Resistance and Sarcopenia: A Review. Int. J. Mol. Sci. 2018, 19, 218. https://doi.org/10.3390/ijms19010218
Buoite Stella A, Gortan Cappellari G, Barazzoni R, Zanetti M. Update on the Impact of Omega 3 Fatty Acids on Inflammation, Insulin Resistance and Sarcopenia: A Review. International Journal of Molecular Sciences. 2018; 19(1):218. https://doi.org/10.3390/ijms19010218
Chicago/Turabian StyleBuoite Stella, Alex, Gianluca Gortan Cappellari, Rocco Barazzoni, and Michela Zanetti. 2018. "Update on the Impact of Omega 3 Fatty Acids on Inflammation, Insulin Resistance and Sarcopenia: A Review" International Journal of Molecular Sciences 19, no. 1: 218. https://doi.org/10.3390/ijms19010218
APA StyleBuoite Stella, A., Gortan Cappellari, G., Barazzoni, R., & Zanetti, M. (2018). Update on the Impact of Omega 3 Fatty Acids on Inflammation, Insulin Resistance and Sarcopenia: A Review. International Journal of Molecular Sciences, 19(1), 218. https://doi.org/10.3390/ijms19010218