Recent Understandings of Biology, Prophylaxis and Treatment Strategies for Hypertrophic Scars and Keloids


Abstract
:1. Introduction
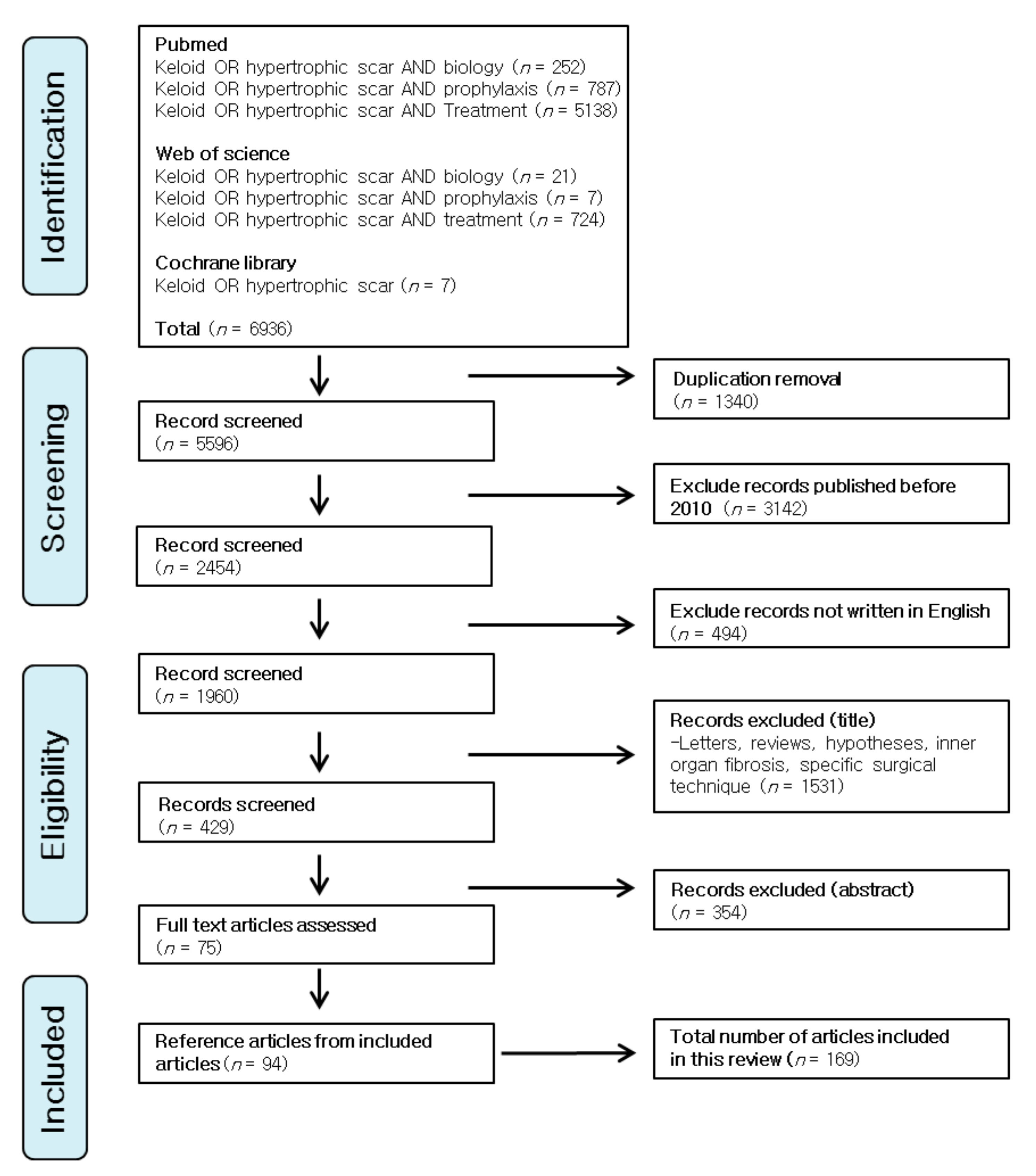
2. Methods
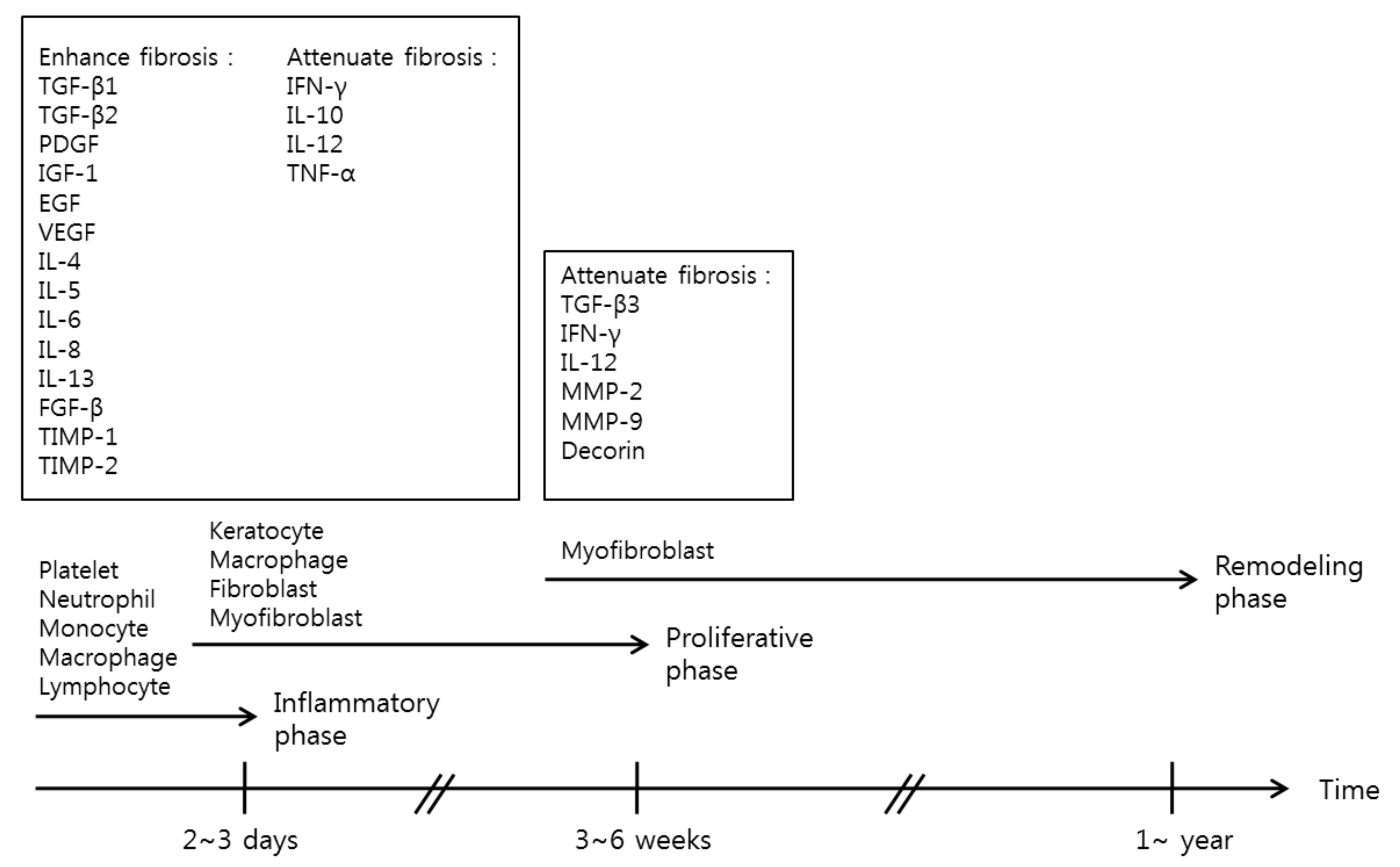
3. Classical Concepts of Wound Healing
4. Important Proteins and Cytokines in the Wound Healing Processes
4.1. Inflammatory and Proliferative Phase
4.2. Remodeling Phase
5. Recent Findings of Scar Biology
5.1. Hypoxia
5.2. Periostin
5.3. MicroRNAs
6. Preventions and Treatment Strategies for Hypertrophic Scars and Keloids
6.1. Prevention
6.1.1. Tension-Free Primary Closure
6.1.2. Passive Mechanical Stabilization
6.1.3. Flavonoids
6.1.4. Pressure Therapy
6.2. Current Treatment Strategies
6.2.1. Corticosteroids
6.2.2. Scar Revision Surgery
6.2.3. Cryotherapy
6.2.4. Radiotherapy
6.2.5. Laser Therapy
6.2.6. 5-Fluorouracil
6.3. Emerging Therapies
6.3.1. Mesenchymal Stem Cell Therapy
6.3.2. Fat Grafting
6.3.3. Interferon
6.3.4. Transforming Growth Factor-β
6.3.5. Botulinum Toxin A
6.3.6. Bleomycin
7. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Sund, B. New Development in Wound Care; PJB Publications: London, UK, 2000; pp. 1–255. [Google Scholar]
- Ogawa, R. Keloid and Hypertrophic Scars Are the Result of Chronic Inflammation in the Reticular Dermis. Int. J. Mol. Sci. 2017, 18, 606. [Google Scholar] [CrossRef] [PubMed]
- Chiang, R.S.; Borovikova, A.A.; King, K.; Banyard, D.A.; Lalezari, S.; Toranto, J.D.; Paydar, K.Z.; Wirth, G.A.; Evans, G.R.; Widgerow, A.D. Current concepts related to hypertrophic scarring in burn injuries. Wound Repair Regen. 2016, 24, 466–477. [Google Scholar] [CrossRef] [PubMed]
- Tredget, E.E.; Nedelec, B.; Scott, P.G.; Ghahary, A. Hypertrophic scars, keloids, and contractures. The cellular and molecular basis for therapy. Surg. Clin. N. Am. 1997, 77, 701–730. [Google Scholar] [CrossRef]
- Imhof, B.A.; Jemelin, S.; Ballet, R.; Vesin, C.; Schapira, M.; Karaca, M.; Emre, Y. CCN1/CYR61-mediated meticulous patrolling by Ly6Clow monocytes fuels vascular inflammation. Proc. Natl. Acad. Sci. USA 2016, 113, E4847–E4856. [Google Scholar] [CrossRef] [PubMed]
- Grose, R.; Werner, S. Wound-healing studies in transgenic and knockout mice. Mol. Biotechnol. 2004, 28, 147–166. [Google Scholar] [CrossRef]
- Werner, S.; Krieg, T.; Smola, H. Keratinocyte-fibroblast interactions in wound healing. J. Investig. Dermatol. 2007, 127, 998–1008. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Z.; Ding, J.; Tredget, E.E. The molecular basis of hypertrophic scars. Burns Trauma 2016, 4, 2. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Jiang, L.Z.; Xue, B. Recombinant human endostatin reduces hypertrophic scar formation in rabbit ear model through down-regulation of VEGF and TIMP-1. Afr. Health Sci. 2016, 16, 542–553. [Google Scholar] [CrossRef] [PubMed]
- Tuan, T.L.; Nichter, L.S. The molecular basis of keloid and hypertrophic scar formation. Mol. Med. Today 1998, 4, 19–24. [Google Scholar] [CrossRef]
- Ishihara, H.; Yoshimoto, H.; Fujioka, M.; Murakami, R.; Hirano, A.; Fujii, T.; Ohtsuru, A.; Namba, H.; Yamashita, S. Keloid fibroblasts resist ceramide-induced apoptosis by overexpression of insulin-like growth factor I receptor. J. Investig. Dermatol. 2000, 115, 1065–1071. [Google Scholar] [CrossRef] [PubMed]
- Butler, P.D.; Longaker, M.T.; Yang, G.P. Current progress in keloid research and treatment. J. Am. Coll. Surg. 2008, 206, 731–741. [Google Scholar] [CrossRef] [PubMed]
- Ladak, A.; Tredget, E.E. Pathophysiology and management of the burn scar. Clin. Plast. Surg. 2009, 36, 661–674. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Thibeault, S.L. Role of tumor necrosis factor-α in wound repair in human vocal fold fibroblasts. Laryngoscope 2010, 120, 1819–1825. [Google Scholar] [CrossRef] [PubMed]
- Mariani, T.J.; Sandefur, S.; Roby, J.D.; Pierce, R.A. Collagenase-3 induction in rat lung fibroblasts requires the combined effects of tumor necrosis factor-α and 12-lipoxygenase metabolites: A model of macrophage-induced, fibroblast driven extracellular matrix remodeling during inflammatory lung injury. Mol. Biol. Cell 1998, 9, 1411–1424. [Google Scholar] [CrossRef] [PubMed]
- Yan, C.; Grimm, W.A.; Garner, W.L.; Qin, L.; Travis, T.; Tan, N.; Han, Y.P. Epithelial to mesenchymal transition in human skin wound healing is induced by tumor necrosis factor-α through bone morphogenic protein-2. Am. J. Pathol. 2010, 176, 2247–2258. [Google Scholar] [CrossRef] [PubMed]
- Armour, A.; Scott, P.G.; Tredget, E.E. Cellular and molecular pathology of HTS: Basis for treatment. Wound Repair Regen. 2007, 15 (Suppl. S1), S6–S17. [Google Scholar] [CrossRef] [PubMed]
- Doucet, C.; Brouty-Boye, D.; Pottin-Clemenceau, C.; Canonica, G.W.; Jasmin, C.; Azzarone, B. Interleukin (IL) 4 and IL-13 act on human lung fibroblasts. Implication in asthma. J. Clin. Investig. 1998, 101, 2129–2139. [Google Scholar] [CrossRef] [PubMed]
- Wynn, T.A. Fibrotic disease and the Th1/Th2 paradigm. Nat. Rev. Immunol. 2004, 4, 583–594. [Google Scholar] [CrossRef] [PubMed]
- Van den Broek, L.J.; van der Veer, W.M.; de Jong, E.H.; Gibbs, S.; Niessen, F.B. Suppressed inflammatory gene expression during human hypertrophic scar compared to normotrophic scar formation. Exp. Dermatol. 2015, 24, 623–629. [Google Scholar] [CrossRef] [PubMed]
- Namazi, M.R.; Fallahzadeh, M.K.; Schwartz, R.A. Strategies for prevention of scars: What can we learn from fetal skin? Int. J. Dermatol. 2011, 50, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Liechty, K.W.; Kim, H.B.; Adzick, N.S.; Crombleholme, T.M. Fetal wound repair results in scar formation in interleukin-10-deficient mice in a syngeneic murine model of scarless fetal wound repair. J. Pediatr. Surg. 2000, 35, 866–872. [Google Scholar] [CrossRef] [PubMed]
- Bock, O.; Yu, H.; Zitron, S.; Bayat, A.; Ferguson, M.W.; Mrowietz, U. Studies of transforming growth factors β 1–3 and their receptors I and II in fibroblast of keloids and hypertrophic scars. Acta Derm. Venereol. 2005, 85, 216–220. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.Y.; Chin, G.S.; Kim, W.J.; Chau, D.; Gittes, G.K.; Longaker, M.T. Expression of transforming growth factor β 1, 2, and 3 proteins in keloids. Ann. Plast. Surg. 1999, 43, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Xia, W.; Phan, T.T.; Lim, I.J.; Longaker, M.T.; Yang, G.P. Complex epithelial-mesenchymal interactions modulate transforming growth factor-β expression in keloid-derived cells. Wound Repair Regen. 2004, 12, 546–556. [Google Scholar] [CrossRef] [PubMed]
- Lu, L.; Saulis, A.S.; Liu, W.R.; Roy, N.K.; Chao, J.D.; Ledbetter, S.; Mustoe, T.A. The temporal effects of anti-TGF-β1, 2, and 3 monoclonal antibody on wound healing and hypertrophic scar formation. J. Am. Coll. Surg. 2005, 201, 391–397. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, M.; Muragaki, Y.; Ooshima, A. Keloid-derived fibroblasts show increased secretion of factors involved in collagen turnover and depend on matrix metalloproteinase for migration. Br. J. Dermatol. 2005, 153, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Ghahary, A.; Ghaffari, A. Role of keratinocyte-fibroblast cross-talk in development of hypertrophic scar. Wound Repair Regen. 2007, 15 (Suppl. S1), S46–S53. [Google Scholar] [CrossRef] [PubMed]
- Mauviel, A. Cytokine regulation of metalloproteinase gene expression. J. Cell. Biochem. 1993, 53, 288–295. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; McCluskey, K.; Fujii, K.; Wahl, L.M. Differential regulation of monocyte matrix metalloproteinase and TIMP-1 production by TNF-α, granulocyte-macrophage CSF, and IL-1 β through prostaglandin-dependent and -independent mechanisms. J. Immunol. 1998, 161, 3071–3076. [Google Scholar] [PubMed]
- McQuibban, G.A.; Gong, J.H.; Tam, E.M.; McCulloch, C.A.; Clark-Lewis, I.; Overall, C.M. Inflammation dampened by gelatinase A cleavage of monocyte chemoattractant protein-3. Science 2000, 289, 1202–1206. [Google Scholar] [CrossRef] [PubMed]
- McQuibban, G.A.; Gong, J.H.; Wong, J.P.; Wallace, J.L.; Clark-Lewis, I.; Overall, C.M. Matrix metalloproteinase processing of monocyte chemoattractant proteins generates CC chemokine receptor antagonists with anti-inflammatory properties in vivo. Blood 2002, 100, 1160–1167. [Google Scholar] [PubMed]
- Rohani, M.G.; Parks, W.C. Matrix remodeling by MMPs during wound repair. Matrix Biol. 2015, 44, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Krumdieck, R.; Hook, M.; Rosenberg, L.C.; Volanakis, J.E. The proteoglycan decorin binds C1q and inhibits the activity of the C1 complex. J. Immunol. 1992, 149, 3695–3701. [Google Scholar] [PubMed]
- Scott, P.G.; Dodd, C.M.; Tredget, E.E.; Ghahary, A.; Rahemtulla, F. Chemical characterization and quantification of proteoglycans in human post-burn hypertrophic and mature scars. Clin. Sci. 1996, 90, 417–425. [Google Scholar] [CrossRef] [PubMed]
- Jarvelainen, H.; Sainio, A.; Wight, T.N. Pivotal role for decorin in angiogenesis. Matrix Biol. 2015, 43, 15–26. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Garron, T.M.; Li, X.J.; Liu, Y.; Zhang, X.; Li, Y.Y.; Xu, W.S. Recombinant human decorin inhibits TGF-β1-induced contraction of collagen lattice by hypertrophic scar fibroblasts. Burns 2009, 35, 527–537. [Google Scholar] [CrossRef] [PubMed]
- Mukhopadhyay, A.; Wong, M.Y.; Chan, S.Y.; Do, D.V.; Khoo, A.; Ong, C.T.; Cheong, H.H.; Lim, I.J.; Phan, T.T. Syndecan-2 and decorin: Proteoglycans with a difference—Implications in keloid pathogenesis. J. Trauma 2010, 68, 999–1008. [Google Scholar] [CrossRef] [PubMed]
- Sen, C.K.; Roy, S. Oxygenation state as a driver of myofibroblast differentiation and wound contraction: Hypoxia impairs wound closure. J. Investig. Dermatol. 2010, 130, 2701–2703. [Google Scholar] [CrossRef] [PubMed]
- Nauta, T.D.; van Hinsbergh, V.W.; Koolwijk, P. Hypoxic signaling during tissue repair and regenerative medicine. Int. J. Mol. Sci. 2014, 15, 19791–19815. [Google Scholar] [CrossRef] [PubMed]
- Ueda, K.; Yasuda, Y.; Furuya, E.; Oba, S. Inadequate blood supply persists in keloids. Scand. J. Plast. Reconstr. Surg. Hand Surg. 2004, 38, 267–271. [Google Scholar] [CrossRef] [PubMed]
- Steinbrech, D.S.; Mehrara, B.J.; Chau, D.; Rowe, N.M.; Chin, G.; Lee, T.; Saadeh, P.B.; Gittes, G.K.; Longaker, M.T. Hypoxia upregulates VEGF production in keloid fibroblasts. Ann. Plast. Surg. 1999, 42, 514–519. [Google Scholar] [CrossRef] [PubMed]
- Zhao, B.; Guan, H.; Liu, J.Q.; Zheng, Z.; Zhou, Q.; Zhang, J.; Su, L.L.; Hu, D.H. Hypoxia drives the transition of human dermal fibroblasts to a myofibroblast-like phenotype via the TGF-β1/Smad3 pathway. Int. J. Mol. Med. 2017, 39, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Horiuchi, K.; Amizuka, N.; Takeshita, S.; Takamatsu, H.; Katsuura, M.; Ozawa, H.; Toyama, Y.; Bonewald, L.F.; Kudo, A. Identification and characterization of a novel protein, periostin, with restricted expression to periosteum and periodontal ligament and increased expression by transforming growth factor β. J. Bone Miner. Res. 1999, 14, 1239–1249. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.M.; Wang, J.; Elliott, C.; Wen, W.; Hamilton, D.W.; Conway, S.J. Spatiotemporal expression of periostin during skin development and incisional wound healing: Lessons for human fibrotic scar formation. J. Cell Commun. Signal. 2010, 4, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Crawford, J.; Nygard, K.; Gan, B.S.; O’Gorman, D.B. Periostin induces fibroblast proliferation and myofibroblast persistence in hypertrophic scarring. Exp. Dermatol. 2015, 24, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Elliott, C.G.; Wang, J.; Guo, X.; Xu, S.W.; Eastwood, M.; Guan, J.; Leask, A.; Conway, S.J.; Hamilton, D.W. Periostin modulates myofibroblast differentiation during full-thickness cutaneous wound repair. J. Cell Sci. 2012, 125, 121–132. [Google Scholar] [CrossRef] [PubMed]
- Conway, S.J.; Izuhara, K.; Kudo, Y.; Litvin, J.; Markwald, R.; Ouyang, G.; Arron, J.R.; Holweg, C.T.; Kudo, A. The role of periostin in tissue remodeling across health and disease. Cell. Mol. Life Sci. 2014, 71, 1279–1288. [Google Scholar] [CrossRef] [PubMed]
- Jackson-Boeters, L.; Wen, W.; Hamilton, D.W. Periostin localizes to cells in normal skin, but is associated with the extracellular matrix during wound repair. J. Cell Commun. Signal. 2009, 3, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Nie, F.; Kang, C.; Chen, B.; Qin, Z.; Ma, J.; Ma, Y.; Zhao, X. Increased periostin expression affects the proliferation, collagen synthesis, migration and invasion of keloid fibroblasts under hypoxic conditions. Int. J. Mol. Med. 2014, 34, 253–261. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Nie, F.; Chen, X.; Qin, Z.; Kang, C.; Chen, B.; Ma, J.; Pan, B.; Ma, Y. Upregulated periostin promotes angiogenesis in keloids through activation of the ERK 1/2 and focal adhesion kinase pathways, as well as the upregulated expression of VEGF and angiopoietin1. Mol. Med. Rep. 2015, 11, 857–864. [Google Scholar] [CrossRef] [PubMed]
- Kashiyama, K.; Mitsutake, N.; Matsuse, M.; Ogi, T.; Saenko, V.A.; Ujifuku, K.; Utani, A.; Hirano, A.; Yamashita, S. miR-196a downregulation increases the expression of type I and III collagens in keloid fibroblasts. J. Investig. Dermatol. 2012, 132, 1597–1604. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Yang, D.; Xiao, Z.; Zhang, M. miRNA expression profiles in keloid tissue and corresponding normal skin tissue. Aesthet. Plast. Surg. 2012, 36, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Lovendorf, M.B.; Skov, L. miRNAs in inflammatory skin diseases and their clinical implications. Expert Rev. Clin. Immunol. 2015, 11, 467–477. [Google Scholar] [CrossRef] [PubMed]
- Luan, Y.; Liu, Y.; Liu, C.; Lin, Q.; He, F.; Dong, X.; Xiao, Z. Serum miRNAs Signature Plays an Important Role in Keloid Disease. Curr. Mol. Med. 2016, 16, 504–514. [Google Scholar] [CrossRef] [PubMed]
- Yao, X.; Cui, X.; Wu, X.; Xu, P.; Zhu, W.; Chen, X.; Zhao, T. Tumor suppressive role of miR-1224-5p in keloid proliferation, apoptosis and invasion via the TGF-β1/Smad3 signaling pathway. Biochem. Biophys. Res. Commun. 2017, 495, 713–720. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.Y.; Lu, L.; Liang, J.; Guo, X.R.; Zhang, P.H.; Luo, S.J. Keloid microRNA expression analysis and the influence of miR-199a-5p on the proliferation of keloid fibroblasts. Genet. Mol. Res. 2014, 13, 2727–2738. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Wang, X.; Yang, D.; Xiao, Z.; Chen, X. MicroRNA-21 affects proliferation and apoptosis by regulating expression of PTEN in human keloid fibroblasts. Plast. Reconstr. Surg. 2014, 134, 561e–573e. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zhang, J.; Lei, Y.; Lyu, L.; Zuo, R.; Chen, T. MicroRNA-21 in Skin Fibrosis: Potential for Diagnosis and Treatment. Mol. Diagn. Ther. 2017, 21, 633–642. [Google Scholar] [CrossRef] [PubMed]
- Zhou, R.; Wang, C.; Wen, C.; Wang, D. miR-21 promotes collagen production in keloid via Smad7. Burns 2017, 43, 555–561. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Li, Y.; Li, N.; Teng, W.; Wang, M.; Zhang, Y.; Xiao, Z. TGF-β1 promotes scar fibroblasts proliferation and transdifferentiation via up-regulating microRNA-21. Sci. Rep. 2016, 6, 32231. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Lu, C.L.; Cui, L.P.; Hu, Y.L.; Yu, Q.; Jiang, Y.; Ma, T.; Jiao, D.K.; Wang, D.; Jia, C.Y. MicroRNA-146a modulates TGF-β1-induced phenotypic differentiation in human dermal fibroblasts by targeting SMAD4. Arch. Dermatol. Res. 2012, 304, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Xu, D.; Li, N.; Li, Y.; He, Y.; Hu, X.; Lyu, L.; He, L. Downregulation of microRNA-31 inhibits proliferation and induces apoptosis by targeting HIF1AN in human keloid. Oncotarget 2017, 8, 74623–74634. [Google Scholar] [CrossRef] [PubMed]
- Bond, J.S.; Duncan, J.A.; Mason, T.; Sattar, A.; Boanas, A.; O’Kane, S.; Ferguson, M.W. Scar redness in humans: How long does it persist after incisional and excisional wounding? Plast. Reconstr. Surg. 2008, 121, 487–496. [Google Scholar] [CrossRef] [PubMed]
- Mutalik, S. Treatment of keloids and hypertrophic scars. Indian J. Dermatol. Venereol. Leprol. 2005, 71, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Wong, V.W.; Akaishi, S.; Longaker, M.T.; Gurtner, G.C. Pushing back: Wound mechanotransduction in repair and regeneration. J. Investig. Dermatol. 2011, 131, 2186–2196. [Google Scholar] [CrossRef] [PubMed]
- Gurtner, G.C.; Dauskardt, R.H.; Wong, V.W.; Bhatt, K.A.; Wu, K.; Vial, I.N.; Padois, K.; Korman, J.M.; Longaker, M.T. Improving cutaneous scar formation by controlling the mechanical environment: Large animal and phase I studies. Ann. Surg. 2011, 254, 217–225. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, J.A.; McKenna, K.T.; Barnett, A.G.; McGrath, D.J.; Rudd, M. A randomized, controlled trial to determine the efficacy of paper tape in preventing hypertrophic scar formation in surgical incisions that traverse Langer’s skin tension lines. Plast. Reconstr. Surg. 2005, 116, 1648–1656. [Google Scholar] [CrossRef] [PubMed]
- Daya, M.; Nair, V. Traction-assisted dermatogenesis by serial intermittent skin tape application. Plast. Reconstr. Surg. 2008, 122, 1047–1054. [Google Scholar] [CrossRef] [PubMed]
- Fulton, J.E., Jr. Silicone gel sheeting for the prevention and management of evolving hypertrophic and keloid scars. Dermatol. Surg. 1995, 21, 947–951. [Google Scholar] [CrossRef] [PubMed]
- Sawada, Y.; Sone, K. Hydration and occlusion treatment for hypertrophic scars and keloids. Br. J. Plast. Surg. 1992, 45, 599–603. [Google Scholar] [CrossRef]
- Reish, R.G.; Eriksson, E. Scar treatments: Preclinical and clinical studies. J. Am. Coll. Surg. 2008, 206, 719–730. [Google Scholar] [CrossRef] [PubMed]
- Beuth, J.; Hunzelmann, N.; van Leendert, R.; Basten, R.; Noehle, M.; Schneider, B. Safety and efficacy of local administration of contractubex to hypertrophic scars in comparison to corticosteroid treatment. Results of a multicenter, comparative epidemiological cohort study in Germany. In Vivo 2006, 20, 277–283. [Google Scholar] [PubMed]
- Chung, V.Q.; Kelley, L.; Marra, D.; Jiang, S.B. Onion extract gel versus petrolatum emollient on new surgical scars: Prospective double-blinded study. Dermatol. Surg. 2006, 32, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Ho, W.S.; Ying, S.Y.; Chan, P.C.; Chan, H.H. Use of onion extract, heparin, allantoin gel in prevention of scarring in chinese patients having laser removal of tattoos: A prospective randomized controlled trial. Dermatol. Surg. 2006, 32, 891–896. [Google Scholar] [CrossRef] [PubMed]
- Jackson, B.A.; Shelton, A.J. Pilot study evaluating topical onion extract as treatment for postsurgical scars. Dermatol. Surg. 1999, 25, 267–269. [Google Scholar] [CrossRef] [PubMed]
- Phan, T.T.; Lim, I.J.; Sun, L.; Chan, S.Y.; Bay, B.H.; Tan, E.K.; Lee, S.T. Quercetin inhibits fibronectin production by keloid-derived fibroblasts. Implication for the treatment of excessive scars. J. Dermatol. Sci. 2003, 33, 192–194. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.W.; Cho, S.Y.; Lee, S.R.; Lee, K.S. Onion extract and quercetin induce matrix metalloproteinase-1 in vitro and in vivo. Int. J. Mol. Med. 2010, 25, 347–352. [Google Scholar] [PubMed]
- Atiyeh, B.S. Nonsurgical management of hypertrophic scars: Evidence-based therapies, standard practices, and emerging methods. Aesthet. Plast. Surg. 2007, 31, 468–492. [Google Scholar] [CrossRef] [PubMed]
- Baur, P.S.; Larson, D.L.; Stacey, T.R.; Barratt, G.F.; Dobrkovsky, M. Ultrastructural analysis of pressure-treated human hypertrophic scars. J. Trauma 1976, 16, 958–967. [Google Scholar] [CrossRef] [PubMed]
- Kelly, A.P. Medical and surgical therapies for keloids. Dermatol. Ther. 2004, 17, 212–218. [Google Scholar] [CrossRef] [PubMed]
- Macintyre, L.; Baird, M. Pressure garments for use in the treatment of hypertrophic scars—An evaluation of current construction techniques in NHS hospitals. Burns 2005, 31, 11–14. [Google Scholar] [CrossRef] [PubMed]
- Macintyre, L.; Baird, M. Pressure garments for use in the treatment of hypertrophic scars—A review of the problems associated with their use. Burns 2006, 32, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Macintyre, L.; Ferguson, R. Pressure garment design tool to monitor exerted pressures. Burns 2013, 39, 1073–1082. [Google Scholar] [CrossRef] [PubMed]
- Reno, F.; Sabbatini, M.; Lombardi, F.; Stella, M.; Pezzuto, C.; Magliacani, G.; Cannas, M. In vitro mechanical compression induces apoptosis and regulates cytokines release in hypertrophic scars. Wound Repair Regen. 2003, 11, 331–336. [Google Scholar] [CrossRef] [PubMed]
- Van den Kerckhove, E.; Stappaerts, K.; Fieuws, S.; Laperre, J.; Massage, P.; Flour, M.; Boeckx, W. The assessment of erythema and thickness on burn related scars during pressure garment therapy as a preventive measure for hypertrophic scarring. Burns 2005, 31, 696–702. [Google Scholar] [CrossRef] [PubMed]
- Rauscher, G.E.; Kolmer, W.L. Treatment of recurrent earlobe keloids. Cutis 1986, 37, 67–68. [Google Scholar] [PubMed]
- Boyadjiev, C.; Popchristova, E.; Mazgalova, J. Histomorphologic changes in keloids treated with Kenacort. J. Trauma 1995, 38, 299–302. [Google Scholar] [CrossRef] [PubMed]
- Cruz, N.I.; Korchin, L. Inhibition of human keloid fibroblast growth by isotretinoin and triamcinolone acetonide in vitro. Ann. Plast. Surg. 1994, 33, 401–405. [Google Scholar] [CrossRef] [PubMed]
- Robles, D.T.; Berg, D. Abnormal wound healing: Keloids. Clin. Dermatol. 2007, 25, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Wong, T.S.; Li, J.Z.; Chen, S.; Chan, J.Y.; Gao, W. The Efficacy of Triamcinolone Acetonide in Keloid Treatment: A Systematic Review and Meta-analysis. Front. Med. 2016, 3, 71. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, R.; Akaishi, S.; Huang, C.; Dohi, T.; Aoki, M.; Omori, Y.; Koike, S.; Kobe, K.; Akimoto, M.; Hyakusoku, H. Clinical applications of basic research that shows reducing skin tension could prevent and treat abnormal scarring: The importance of fascial/subcutaneous tensile reduction sutures and flap surgery for keloid and hypertrophic scar reconstruction. J. Nippon Med. Sch. 2011, 78, 68–76. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, R.; Akaishi, S.; Kuribayashi, S.; Miyashita, T. Keloids and Hypertrophic Scars Can Now Be Cured Completely: Recent Progress in Our Understanding of the Pathogenesis of Keloids and Hypertrophic Scars and the Most Promising Current Therapeutic Strategy. J. Nippon Med. Sch. 2016, 83, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Leventhal, D.; Furr, M.; Reiter, D. Treatment of keloids and hypertrophic scars: A meta-analysis and review of the literature. Arch. Facial Plast. Surg. 2006, 8, 362–368. [Google Scholar] [CrossRef] [PubMed]
- Muir, I.F. On the nature of keloid and hypertrophic scars. Br. J. Plast. Surg. 1990, 43, 61–69. [Google Scholar] [CrossRef]
- Mustoe, T.A.; Cooter, R.D.; Gold, M.H.; Hobbs, F.D.; Ramelet, A.A.; Shakespeare, P.G.; Stella, M.; Teot, L.; Wood, F.M.; Ziegler, U.E.; et al. International clinical recommendations on scar management. Plast. Reconstr. Surg. 2002, 110, 560–571. [Google Scholar] [CrossRef] [PubMed]
- Har-Shai, Y.; Zouboulis, C.C. Intralesional Cryotherapy for the Treatment of Keloid Scars: A Prospective Study. Plast. Reconstr. Surg. 2015, 136, 397e–398e. [Google Scholar] [CrossRef] [PubMed]
- Boutli-Kasapidou, F.; Tsakiri, A.; Anagnostou, E.; Mourellou, O. Hypertrophic and keloidal scars: An approach to polytherapy. Int. J. Dermatol. 2005, 44, 324–327. [Google Scholar] [CrossRef] [PubMed]
- Jaros, E.; Priborsky, J.; Klein, L. Treatment of keloids and hypertrophic scars with cryotherapy. Acta Med. 1999, 42, 61–63. [Google Scholar]
- Yosipovitch, G.; Widijanti Sugeng, M.; Goon, A.; Chan, Y.H.; Goh, C.L. A comparison of the combined effect of cryotherapy and corticosteroid injections versus corticosteroids and cryotherapy alone on keloids: A controlled study. J. Dermatol. Treat. 2001, 12, 87–90. [Google Scholar] [CrossRef] [PubMed]
- Har-Shai, Y.; Amar, M.; Sabo, E. Intralesional cryotherapy for enhancing the involution of hypertrophic scars and keloids. Plast. Reconstr. Surg. 2003, 111, 1841–1852. [Google Scholar] [CrossRef] [PubMed]
- Rusciani, L.; Paradisi, A.; Alfano, C.; Chiummariello, S.; Rusciani, A. Cryotherapy in the treatment of keloids. J. Drugs Dermatol. 2006, 5, 591–595. [Google Scholar] [CrossRef] [PubMed]
- Rusciani, L.; Rossi, G.; Bono, R. Use of cryotherapy in the treatment of keloids. J. Dermatol. Surg. Oncol. 1993, 19, 529–534. [Google Scholar] [CrossRef] [PubMed]
- Zouboulis, C.C.; Blume, U.; Buttner, P.; Orfanos, C.E. Outcomes of cryosurgery in keloids and hypertrophic scars. A prospective consecutive trial of case series. Arch. Dermatol. 1993, 129, 1146–1151. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, R.; Mitsuhashi, K.; Hyakusoku, H.; Miyashita, T. Postoperative electron-beam irradiation therapy for keloids and hypertrophic scars: Retrospective study of 147 cases followed for more than 18 months. Plast. Reconstr. Surg. 2003, 111, 547–553. [Google Scholar] [CrossRef] [PubMed]
- Ji, J.; Tian, Y.; Zhu, Y.Q.; Zhang, L.Y.; Ji, S.J.; Huan, J.; Zhou, X.Z.; Cao, J.P. Ionizing irradiation inhibits keloid fibroblast cell proliferation and induces premature cellular senescence. J. Dermatol. 2015, 42, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Keeling, B.H.; Whitsitt, J.; Liu, A.; Dunnick, C.A. Keloid removal by shave excision with adjuvant external beam radiation therapy. Dermatol. Surg. 2015, 41, 989–992. [Google Scholar] [CrossRef] [PubMed]
- McKeown, S.R.; Hatfield, P.; Prestwich, R.J.; Shaffer, R.E.; Taylor, R.E. Radiotherapy for benign disease; assessing the risk of radiation-induced cancer following exposure to intermediate dose radiation. Br. J. Radiol. 2015, 88, 20150405. [Google Scholar] [CrossRef] [PubMed]
- Shen, J.; Lian, X.; Sun, Y.; Wang, X.; Hu, K.; Hou, X.; Sun, S.; Yan, J.; Yu, L.; Sun, X.; et al. Hypofractionated electron-beam radiation therapy for keloids: Retrospective study of 568 cases with 834 lesions. J. Radiat. Res. 2015, 56, 811–817. [Google Scholar] [CrossRef] [PubMed]
- Vivante, H.; Salgueiro, M.J.; Ughetti, R.; Nicolini, J.; Zubillaga, M. 32P-patch contact brachyradiotherapy in the management of recalcitrant keloids and hypertrophic scars. Indian J. Dermatol. Venereol. Leprol. 2007, 73, 336–339. [Google Scholar] [PubMed]
- Bhusari, P.; Shukla, J.; Kumar, M.; Vatsa, R.; Chhabra, A.; Palarwar, K.; Rathore, Y.; De, D.; Kumaran, S.; Handa, S.; et al. Noninvasive treatment of keloid using customized Re-188 skin patch. Dermatol. Ther. 2017, 30. [Google Scholar] [CrossRef] [PubMed]
- Apfelberg, D.B.; Maser, M.R.; Lash, H.; White, D.; Weston, J. Preliminary results of argon and carbon dioxide laser treatment of keloid scars. Lasers Surg. Med. 1984, 4, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Alster, T.S.; Handrick, C. Laser treatment of hypertrophic scars, keloids, and striae. Semin. Cutan. Med. Surg. 2000, 19, 287–292. [Google Scholar] [CrossRef] [PubMed]
- Tanzi, E.L.; Alster, T.S. Laser treatment of scars. Skin Ther. Lett. 2004, 9, 4–7. [Google Scholar]
- Koike, S.; Akaishi, S.; Nagashima, Y.; Dohi, T.; Hyakusoku, H.; Ogawa, R. Nd:YAG Laser Treatment for Keloids and Hypertrophic Scars: An Analysis of 102 Cases. Plast. Reconstr. Surg. Glob. Open 2014, 2, e272. [Google Scholar] [CrossRef] [PubMed]
- Akaishi, S.; Koike, S.; Dohi, T.; Kobe, K.; Hyakusoku, H.; Ogawa, R. Nd:YAG Laser Treatment of Keloids and Hypertrophic Scars. Eplasty 2012, 12, e1. [Google Scholar] [PubMed]
- Alster, T. Laser scar revision: Comparison study of 585-nm pulsed dye laser with and without intralesional corticosteroids. Dermatol. Surg. 2003, 29, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Chan, H.H.; Wong, D.S.; Ho, W.S.; Lam, L.K.; Wei, W. The use of pulsed dye laser for the prevention and treatment of hypertrophic scars in chinese persons. Dermatol. Surg. 2004, 30, 987–994. [Google Scholar] [PubMed]
- Fiskerstrand, E.J.; Svaasand, L.O.; Volden, G. Pigmentary changes after pulsed dye laser treatment in 125 northern European patients with port wine stains. Br. J. Dermatol. 1998, 138, 477–479. [Google Scholar] [CrossRef] [PubMed]
- Hermanns, J.F.; Petit, L.; Hermanns-Le, T.; Pierard, G.E. Analytic quantification of phototype-related regional skin complexion. Skin Res. Technol. 2001, 7, 168–171. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, R.E. Treatment of inflamed hypertrophic scars using intralesional 5-FU. Dermatol. Surg. 1999, 25, 224–232. [Google Scholar] [CrossRef] [PubMed]
- Nanda, S.; Reddy, B.S. Intralesional 5-fluorouracil as a treatment modality of keloids. Dermatol. Surg. 2004, 30, 54–56. [Google Scholar] [PubMed]
- Khan, M.A.; Bashir, M.M.; Khan, F.A. Intralesional triamcinolone alone and in combination with 5-fluorouracil for the treatment of Keloid and Hypertrophic scars. J. Pak. Med. Assoc. 2014, 64, 1003–1007. [Google Scholar] [PubMed]
- Darougheh, A.; Asilian, A.; Shariati, F. Intralesional triamcinolone alone or in combination with 5-fluorouracil for the treatment of keloid and hypertrophic scars. Clin. Exp. Dermatol. 2009, 34, 219–223. [Google Scholar] [CrossRef] [PubMed]
- Bijlard, E.; Steltenpool, S.; Niessen, F.B. Intralesional 5-fluorouracil in keloid treatment: A systematic review. Acta Derm. Venereol. 2015, 95, 778–782. [Google Scholar] [CrossRef] [PubMed]
- Le Blanc, K. Immunomodulatory effects of fetal and adult mesenchymal stem cells. Cytotherapy 2003, 5, 485–489. [Google Scholar] [CrossRef] [PubMed]
- Le Blanc, K.; Mougiakakos, D. Multipotent mesenchymal stromal cells and the innate immune system. Nat. Rev. Immunol. 2012, 12, 383–396. [Google Scholar] [CrossRef] [PubMed]
- Ortiz, L.A.; Gambelli, F.; McBride, C.; Gaupp, D.; Baddoo, M.; Kaminski, N.; Phinney, D.G. Mesenchymal stem cell engraftment in lung is enhanced in response to bleomycin exposure and ameliorates its fibrotic effects. Proc. Natl. Acad. Sci. USA 2003, 100, 8407–8411. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Guan, J.; Niu, X.; Hu, G.; Guo, S.; Li, Q.; Xie, Z.; Zhang, C.; Wang, Y. Exosomes released from human induced pluripotent stem cells-derived MSCs facilitate cutaneous wound healing by promoting collagen synthesis and angiogenesis. J. Transl. Med. 2015, 13, 49. [Google Scholar] [CrossRef] [PubMed]
- Lee, R.H.; Pulin, A.A.; Seo, M.J.; Kota, D.J.; Ylostalo, J.; Larson, B.L.; Semprun-Prieto, L.; Delafontaine, P.; Prockop, D.J. Intravenous hMSCs improve myocardial infarction in mice because cells embolized in lung are activated to secrete the anti-inflammatory protein TSG-6. Cell Stem Cell 2009, 5, 54–63. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.S.; Zhou, L.; Sagayaraj, A.; Jumat, N.H.; Choolani, M.; Chan, J.K.; Biswas, A.; Wong, P.C.; Lim, S.G.; Dan, Y.Y. Hepatic differentiation of human amniotic epithelial cells and in vivo therapeutic effect on animal model of cirrhosis. J. Gastroenterol. Hepatol. 2015, 30, 1673–1682. [Google Scholar] [CrossRef] [PubMed]
- Prockop, D.J. Concise review: Two negative feedback loops place mesenchymal stem/stromal cells at the center of early regulators of inflammation. Stem Cells 2013, 31, 2042–2046. [Google Scholar] [CrossRef] [PubMed]
- Prockop, D.J. Inflammation, fibrosis, and modulation of the process by mesenchymal stem/stromal cells. Matrix Boil. 2016, 51, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Prockop, D.J.; Oh, J.Y. Mesenchymal stem/stromal cells (MSCs): Role as guardians of inflammation. Mol. Ther. 2012, 20, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Reinders, M.E.; de Fijter, J.W.; Rabelink, T.J. Mesenchymal stromal cells to prevent fibrosis in kidney transplantation. Curr. Opin. Organ Transplant. 2014, 19, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Shafiq, M.; Lee, S.H.; Jung, Y.; Kim, S.H. Strategies for recruitment of stem cells to treat myocardial infarction. Curr. Pharm. Des. 2015, 21, 1584–1597. [Google Scholar] [CrossRef] [PubMed]
- Seo, B.F.; Jung, S.N. The Immunomodulatory Effects of Mesenchymal Stem Cells in Prevention or Treatment of Excessive Scars. Stem Cells Int. 2016, 2016, 6937976. [Google Scholar] [CrossRef] [PubMed]
- Altman, A.M.; Matthias, N.; Yan, Y.; Song, Y.H.; Bai, X.; Chiu, E.S.; Slakey, D.P.; Alt, E.U. Dermal matrix as a carrier for in vivo delivery of human adipose-derived stem cells. Biomaterials 2008, 29, 1431–1442. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.P.; Hsu, C.C.; Chang, S.C.; Wang, C.H.; Deng, S.C.; Dai, N.T.; Chen, T.M.; Chan, J.Y.; Chen, S.G.; Huang, S.M. Adipose-derived stem cells seeded on acellular dermal matrix grafts enhance wound healing in a murine model of a full-thickness defect. Ann. Plast. Surg. 2012, 69, 656–662. [Google Scholar] [CrossRef] [PubMed]
- Lam, M.T.; Nauta, A.; Meyer, N.P.; Wu, J.C.; Longaker, M.T. Effective delivery of stem cells using an extracellular matrix patch results in increased cell survival and proliferation and reduced scarring in skin wound healing. Tissue Eng. A 2013, 19, 738–747. [Google Scholar] [CrossRef] [PubMed]
- Zonari, A.; Martins, T.M.; Paula, A.C.; Boeloni, J.N.; Novikoff, S.; Marques, A.P.; Correlo, V.M.; Reis, R.L.; Goes, A.M. Polyhydroxybutyrate-co-hydroxyvalerate structures loaded with adipose stem cells promote skin healing with reduced scarring. Acta Biomater. 2015, 17, 170–181. [Google Scholar] [CrossRef] [PubMed]
- Kaigler, D.; Krebsbach, P.H.; Polverini, P.J.; Mooney, D.J. Role of vascular endothelial growth factor in bone marrow stromal cell modulation of endothelial cells. Tissue Eng. 2003, 9, 95–103. [Google Scholar] [CrossRef] [PubMed]
- Liotta, F.; Angeli, R.; Cosmi, L.; Fili, L.; Manuelli, C.; Frosali, F.; Mazzinghi, B.; Maggi, L.; Pasini, A.; Lisi, V.; et al. Toll-like receptors 3 and 4 are expressed by human bone marrow-derived mesenchymal stem cells and can inhibit their T-cell modulatory activity by impairing Notch signaling. Stem Cells 2008, 26, 279–289. [Google Scholar] [CrossRef] [PubMed]
- Waterman, R.S.; Tomchuck, S.L.; Henkle, S.L.; Βncourt, A.M. A new mesenchymal stem cell (MSC) paradigm: Polarization into a pro-inflammatory MSC1 or an Immunosuppressive MSC2 phenotype. PLoS ONE 2010, 5, e10088. [Google Scholar] [CrossRef] [PubMed]
- Yan, H.; Wu, M.; Yuan, Y.; Wang, Z.Z.; Jiang, H.; Chen, T. Priming of Toll-like receptor 4 pathway in mesenchymal stem cells increases expression of B cell activating factor. Biochem. Biophys. Res. Commun. 2014, 448, 212–217. [Google Scholar] [CrossRef] [PubMed]
- Bruno, A.; Delli Santi, G.; Fasciani, L.; Cempanari, M.; Palombo, M.; Palombo, P. Burn scar lipofilling: Immunohistochemical and clinical outcomes. J. Craniofac. Surg. 2013, 24, 1806–1814. [Google Scholar] [CrossRef] [PubMed]
- Negenborn, V.L.; Groen, J.W.; Smit, J.M.; Niessen, F.B.; Mullender, M.G. The Use of Autologous Fat Grafting for Treatment of Scar Tissue and Scar-Related Conditions: A Systematic Review. Plast. Reconstr. Surg. 2016, 137, 31e–43e. [Google Scholar] [CrossRef] [PubMed]
- Piccolo, N.S.; Piccolo, M.S.; Piccolo, M.T. Fat grafting for treatment of burns, burn scars, and other difficult wounds. Clin. Plast. Surg. 2015, 42, 263–283. [Google Scholar] [CrossRef] [PubMed]
- Al-Khawajah, M.M. Failure of interferon-α 2b in the treatment of mature keloids. Int. J. Dermatol. 1996, 35, 515–517. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Kim, S.E.; Lee, A.Y. Effects of interferon-α2b on keloid treatment with triamcinolone acetonide intralesional injection. Int. J. Dermatol. 2008, 47, 183–186. [Google Scholar] [CrossRef] [PubMed]
- Schrementi, M.E.; Ferreira, A.M.; Zender, C.; DiPietro, L.A. Site-specific production of TGF-β in oral mucosal and cutaneous wounds. Wound Repair Regen. 2008, 16, 80–86. [Google Scholar] [CrossRef] [PubMed]
- O'Kane, S.; Ferguson, M.W. Transforming growth factor βs and wound healing. Int. J. Biochem. Cell Biol. 1997, 29, 63–78. [Google Scholar] [CrossRef]
- Shah, M.; Foreman, D.M.; Ferguson, M.W. Neutralisation of TGF-β1 and TGF-β2 or exogenous addition of TGF-β3 to cutaneous rat wounds reduces scarring. J. Cell Sci. 1995, 108 Pt 3, 985–1002. [Google Scholar] [PubMed]
- So, K.; McGrouther, D.A.; Bush, J.A.; Durani, P.; Taylor, L.; Skotny, G.; Mason, T.; Metcalfe, A.; O’Kane, S.; Ferguson, M.W. Avotermin for scar improvement following scar revision surgery: A randomized, double-blind, within-patient, placebo-controlled, phase II clinical trial. Plast. Reconstr. Surg. 2011, 128, 163–172. [Google Scholar] [CrossRef] [PubMed]
- Occleston, N.L.; O’Kane, S.; Laverty, H.G.; Cooper, M.; Fairlamb, D.; Mason, T.; Bush, J.A.; Ferguson, M.W. Discovery and development of avotermin (recombinant human transforming growth factor β3): A new class of prophylactic therapeutic for the improvement of scarring. Wound Repair Regen. 2011, 19 (Suppl. S1), s38–s48. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, M.W.; Duncan, J.; Bond, J.; Bush, J.; Durani, P.; So, K.; Taylor, L.; Chantrey, J.; Mason, T.; James, G.; et al. Prophylactic administration of avotermin for improvement of skin scarring: Three double-blind, placebo-controlled, phase I/II studies. Lancet 2009, 373, 1264–1274. [Google Scholar] [CrossRef]
- Zhibo, X.; Miaobo, Z. Botulinum toxin type A affects cell cycle distribution of fibroblasts derived from hypertrophic scar. J. Plast. Reconstr. Aesthet. Surg. 2008, 61, 1128–1129. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Z.; Zhang, M.; Liu, Y.; Ren, L. Botulinum toxin type a inhibits connective tissue growth factor expression in fibroblasts derived from hypertrophic scar. Aesthet. Plast. Surg. 2011, 35, 802–807. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Z.; Zhang, F.; Lin, W.; Zhang, M.; Liu, Y. Effect of botulinum toxin type A on transforming growth factor β1 in fibroblasts derived from hypertrophic scar: A preliminary report. Aesthet. Plast. Surg. 2010, 34, 424–427. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Z.; Zhang, F.; Cui, Z. Treatment of hypertrophic scars with intralesional botulinum toxin type A injections: A preliminary report. Aesthet. Plast. Surg. 2009, 33, 409–412. [Google Scholar] [CrossRef] [PubMed]
- Gassner, H.G.; Sherris, D.A.; Otley, C.C. Treatment of facial wounds with botulinum toxin A improves cosmetic outcome in primates. Plast. Reconstr. Surg. 2000, 105, 1948–1953. [Google Scholar] [CrossRef] [PubMed]
- Elhefnawy, A.M. Assessment of intralesional injection of botulinum toxin type A injection for hypertrophic scars. Indian J. Dermatol. Venereol. Leprol. 2016, 82, 279–283. [Google Scholar] [CrossRef] [PubMed]
- Shaarawy, E.; Hegazy, R.A.; Abdel Hay, R.M. Intralesional botulinum toxin type A equally effective and better tolerated than intralesional steroid in the treatment of keloids: A randomized controlled trial. J. Cosmet. Dermatol. 2015, 14, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Zhibo, X.; Miaobo, Z. Intralesional botulinum toxin type A injection as a new treatment measure for keloids. Plast. Reconstr. Surg. 2009, 124, 275e–277e. [Google Scholar] [CrossRef] [PubMed]
- Jones, C.D.; Guiot, L.; Samy, M.; Gorman, M.; Tehrani, H. The Use of Chemotherapeutics for the Treatment of Keloid Scars. Dermatol. Rep. 2015, 7, 5880. [Google Scholar] [CrossRef] [PubMed]
- Espana, A.; Solano, T.; Quintanilla, E. Bleomycin in the treatment of keloids and hypertrophic scars by multiple needle punctures. Dermatol. Surg. 2001, 27, 23–27. [Google Scholar] [PubMed]
- Saray, Y.; Gulec, A.T. Treatment of keloids and hypertrophic scars with dermojet injections of bleomycin: A preliminary study. Int. J. Dermatol. 2005, 44, 777–784. [Google Scholar] [CrossRef] [PubMed]
- Hendricks, T.; Martens, M.F.; Huyben, C.M.; Wobbes, T. Inhibition of basal and TGF β-induced fibroblast collagen synthesis by antineoplastic agents. Implications for wound healing. Br. J. Cancer 1993, 67, 545–550. [Google Scholar] [CrossRef] [PubMed]
- Yeowell, H.N.; Marshall, M.K.; Walker, L.C.; Ha, V.; Pinnell, S.R. Regulation of lysyl oxidase mRNA in dermal fibroblasts from normal donors and patients with inherited connective tissue disorders. Arch. Biochem. Biophys. 1994, 308, 299–305. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Categories | Modalities | Suggested Mechanisms | Use |
|---|---|---|---|
| Prophylaxis | Tension-free closure | -Reduce inflammation by reducing mechanotransduction | -Debridement of inviable tissues, adequate hemostasis -Rapid tension free primary closure |
| Taping or silicone sheeting | -Reduce inflammation by reducing mechanotransduction: occlusion and hydration | -Start 2 weeks after primary wound treatment -12 h a day for at least 2 months | |
| Flavonoids | -Induction of MMPs -Inhibition of SMADs expression | -Start 2 weeks after primary wound treatment -Generally twice daily for 4 to 6 months | |
| Pressure therapy | -Occlusion of blood vessels -Inducing apoptosis | -Pressure of 15 to 40 mmHg -More than 23 h a day for at least 6 months | |
| Treatment (current) | Corticosteroids | -Reducing inflammation and proliferation -Vasoconstriction | -Intralesional injection: triamcinolone 10 to 40 mg/mL -1 to 2 sessions a month (2 to 3 sessions, but can be extended) -Tapes/plasters, ointments are available -Combination is common |
| Scar revision | -Direct reduction of scar volume | -At least 1 year after primary wound treatment -Combination is recommended | |
| Cryotherapy | -Scar tissue necrosis | -Deliver liquid nitrogen using spray, contact or intralesional needle cryoprobe -10 to 20 s freeze-thaw cycles -Combination is common | |
| Radiotherapy | -Anti-angiogenesis -Anti-inflammation | -Adjuvant after scar revision -24–48 h after scar revision surgery -Total of 40 Gray or less, over several divided sessions | |
| Laser therapy | -Vaporize blood vessel -Anti-inflammation | -585-nm pulsed dye laser: 6.0–7.5 J/cm2 (7 mm spot) or 4.5–5.5 J/cm2 (10 mm spot) -1064-nm Nd:YAG laser: 14 J/cm2 (5 mm spot) -2 to 6 sessions, every 3–4 weeks | |
| 5-Fluorouracil | -Anti-angiogenesis -Anti-inflammation | -Intralesional injection: 50 mg/mL -Weekly for 12 weeks -Combination is common | |
| Treatment (Emerging) | MSC * therapy | -Modulation of proinflammatory cell activity -Anti-fibrosis -Promote normal angiogenetic activity | -Systemic injection -Local injection (at the wound) -Engineered MSC-seeded tissue scaffold |
| Fat grafting | -Deliver adipose-tissue derived MSCs | -Fat injection or fat tissue grafting underneath or into the wound | |
| Interferon | -Downregulating TGF-β1 -Attenuates collagen synthesis and fibroblast proliferation | -Intralesional injection: 1.5 × 106 IU, twice daily over 4 days | |
| Human recombinant TGF-β3/TGF-β1 or 2 neutralizing antibody | -Adjust TGF-β3: TGF-β1 or 2 ratio | Not available currently | |
| Botulinum toxin type A | -Reduce muscle tension during wound healing -Arrest cell cycle in non-proliferative stage -Influence TGF-β1 expression | -Intralesional injection: 70~140 U, 1 or 3 months interval, 3 sessions | |
| Bleomycin | -Decreasing collagen synthesis -Reduce lysyl-oxidase levels -Induce apoptosis | -Intralesional injection: 1.5 IU/mL, 2 to 6 sessions at monthly interval |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, H.J.; Jang, Y.J. Recent Understandings of Biology, Prophylaxis and Treatment Strategies for Hypertrophic Scars and Keloids. Int. J. Mol. Sci. 2018, 19, 711. https://doi.org/10.3390/ijms19030711
Lee HJ, Jang YJ. Recent Understandings of Biology, Prophylaxis and Treatment Strategies for Hypertrophic Scars and Keloids. International Journal of Molecular Sciences. 2018; 19(3):711. https://doi.org/10.3390/ijms19030711
Chicago/Turabian StyleLee, Ho Jun, and Yong Ju Jang. 2018. "Recent Understandings of Biology, Prophylaxis and Treatment Strategies for Hypertrophic Scars and Keloids" International Journal of Molecular Sciences 19, no. 3: 711. https://doi.org/10.3390/ijms19030711
APA StyleLee, H. J., & Jang, Y. J. (2018). Recent Understandings of Biology, Prophylaxis and Treatment Strategies for Hypertrophic Scars and Keloids. International Journal of Molecular Sciences, 19(3), 711. https://doi.org/10.3390/ijms19030711