Diagnostic Roles of Postmortem cTn I and cTn T in Cardiac Death with Special Regard to Myocardial Infarction: A Systematic Literature Review and Meta-Analysis

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Included Literature
2.2. Characteristics of Involved Studies
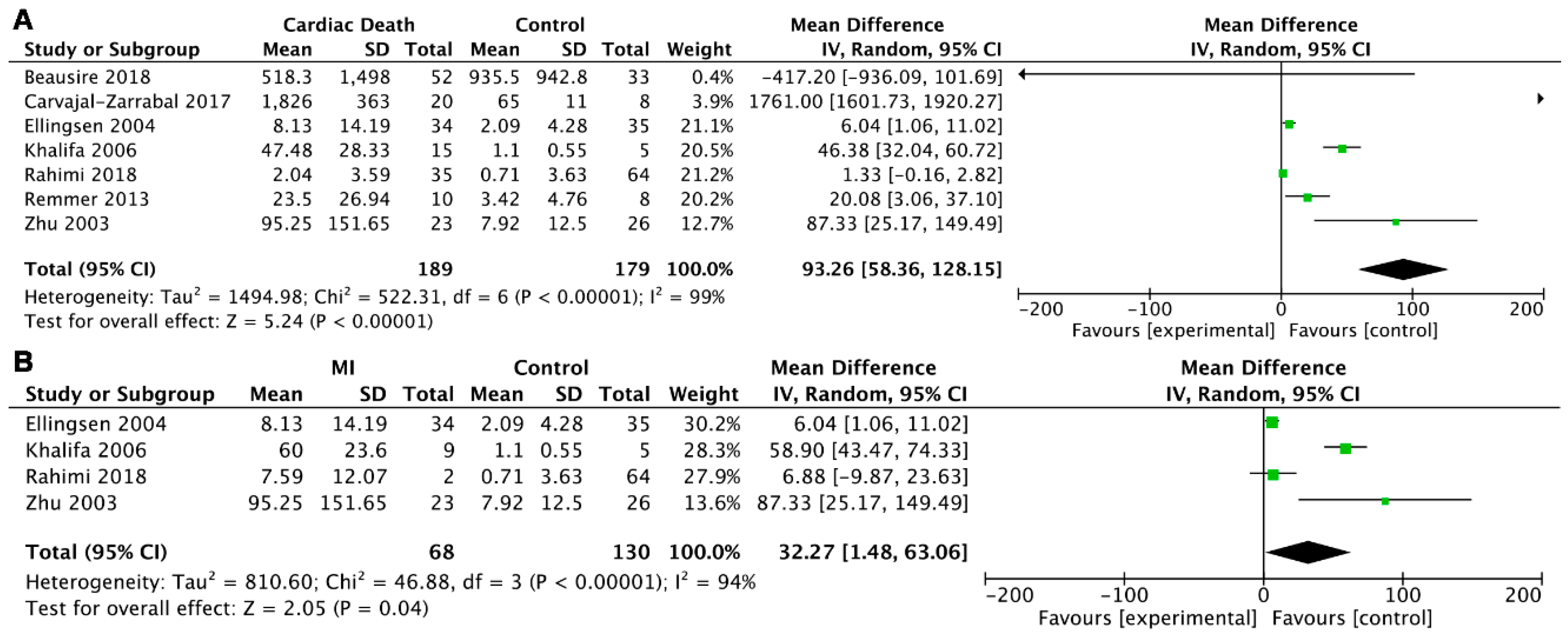
2.3. Meta-Analysis
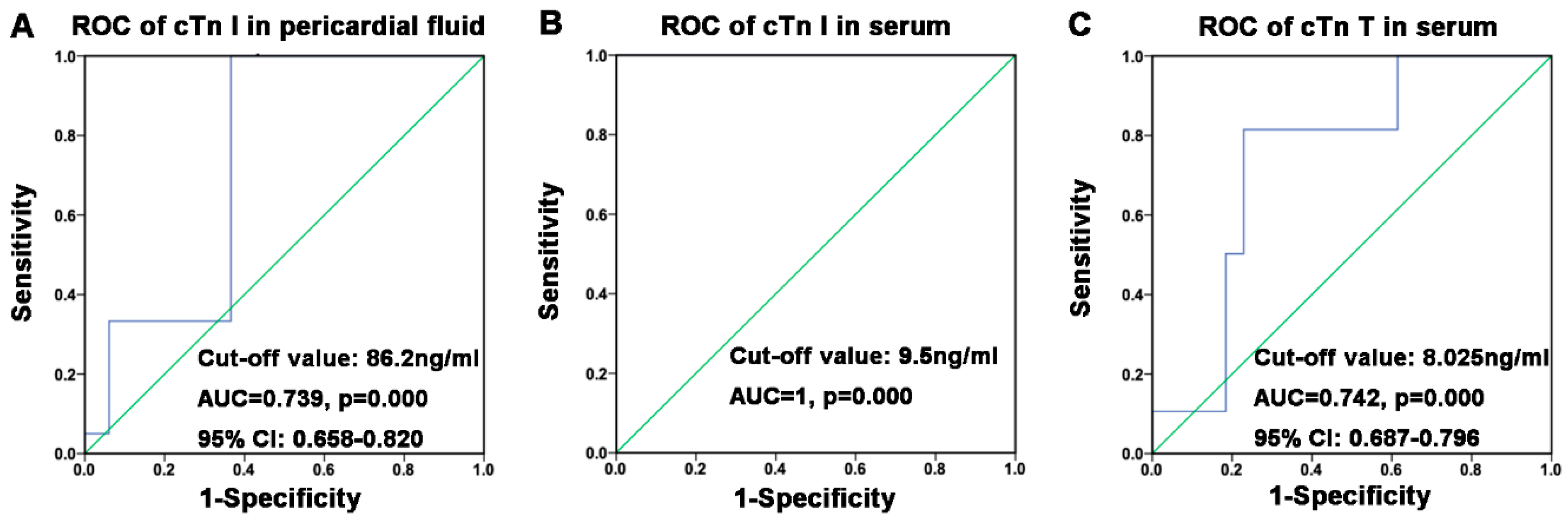
2.4. Speculation of Postmortem Cut-off Values of cTn I and cTn T by ROC
3. Discussion
3.1. The Concentration Changes of Cardiac Troponin in Antemortem and Postmortem Samples
3.2. Stability of Postmortem cTn I and cTn T with Regard to Cardiopulmonary Resuscitation, Age, Gender, and PMI
3.3. Cardiac Troponins in Different Sampling Sites
3.4. Cardiac Troponins in Cardiac Death
3.5. Cut-off Values of Postmortem cTn I and cTn T
3.6. Analysis Methods of Cardiac Troponins
4. Materials and Methods
4.1. Strategy of Literature Search
4.2. Inclusion Criteria
4.3. Exclusion Criteria
4.4. Data Abstraction and Quality Assessment
4.5. Statistical Analysis
5. Conclusions and Perspective
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| ACS | Acute coronary syndrome |
| AMI | Acute myocardial infarction |
| AUC | Area under the curve |
| NT-proBNP | N-terminal proBNP |
| CBM | China Biomedical Literature Database |
| CI | Confidence interval |
| CK-MB | Creatine kinase MB |
| CNKI | China National Knowledge Infrastructure |
| cTn I | Cardiac troponin I |
| cTn T | Cardiac troponin T |
| ELISA | Enzyme-linked immunosorbent assay |
| MI | Myocardial infarction |
| PMI | Postmortem interval |
| POCT | Point-of-care testing |
| ROC | Receiver operating characteristic curve |
| SCD | Sudden cardiac death |
| WMD | Weighted mean difference |
References
- Priori, S.G.; Blomstrom-Lundqvist, C.; Mazzanti, A.; Blom, N.; Borggrefe, M.; Camm, J.; Elliott, P.M.; Fitzsimons, D.; Hatala, R.; Hindricks, G.; et al. 2015 esc guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: The task force for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death of the european society of cardiology (esc). Endorsed by: Association for european paediatric and congenital cardiology (aepc). Eur. Heart J. 2015, 36, 2793–2867. [Google Scholar] [PubMed]
- Kuriachan, V.P.; Sumner, G.L.; Mitchell, L.B. Sudden cardiac death. Curr. Probl. Cardiol. 2015, 40, 133–200. [Google Scholar] [CrossRef] [PubMed]
- Kandala, J.; Oommen, C.; Kern, K.B. Sudden cardiac death. Br. Med. Bull. 2017, 122, 5–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cina, S.J.; Li, D.J.; Chan, D.W.; Boitnott, J.K.; Hruban, R.H.; Smialek, J.E. Serum concentrations of cardiac troponin i in sudden death: A pilot study. Am. J. Forensic Med. Pathol. 1998, 19, 324–328. [Google Scholar] [CrossRef]
- Campuzano, O.; Allegue, C.; Partemi, S.; Iglesias, A.; Oliva, A.; Brugada, R. Negative autopsy and sudden cardiac death. Int. J. Legal Med. 2014, 128, 599–606. [Google Scholar] [CrossRef] [PubMed]
- Cao, Z.P.; Zhang, Y.; Mi, L.; Luo, X.Y.; Tian, M.H.; Zhu, B.L. The expression of b-type natriuretic peptide after cacl2-induced arrhythmias in rats. Am. J. Forensic Med. Pathol. 2016, 37, 133–140. [Google Scholar] [PubMed]
- Madea, B.; Musshoff, F. Postmortem biochemistry. Forensic Sci. Int. 2007, 165, 165–171. [Google Scholar] [CrossRef]
- Maeda, H.; Ishikawa, T.; Michiue, T. Forensic biochemistry for functional investigation of death: Concept and practical application. Leg. Med. (Tokyo, Japan) 2011, 13, 55–67. [Google Scholar] [CrossRef]
- Sarko, J.; Pollack, C.V., Jr. Cardiac troponins. J. Emerg. Med. 2002, 23, 57–65. [Google Scholar] [CrossRef]
- Hoff, J.; Wehner, W.; Nambi, V. Troponin in cardiovascular disease prevention: Updates and future direction. Curr. Atheroscler. Rep. 2016, 18, 12. [Google Scholar] [CrossRef]
- Park, K.C.; Gaze, D.C.; Collinson, P.O.; Marber, M.S. Cardiac troponins: From myocardial infarction to chronic disease. Cardiovasc. Res. 2017, 113, 1708–1718. [Google Scholar] [CrossRef]
- Voss, E.M.; Sharkey, S.W.; Gernert, A.E.; Murakami, M.M.; Johnston, R.B.; Hsieh, C.C.; Apple, F.S. Human and canine cardiac troponin t and creatine kinase-mb distribution in normal and diseased myocardium. Infarct sizing using serum profiles. Arch. Pathol. Lab. Med. 1995, 119, 799–806. [Google Scholar] [PubMed]
- Jaffe, A.S.; Ordonez-Llanos, J. High sensitivity troponin in chest pain and acute coronary syndromes. A step forward? Rev. Esp. Cardiol. 2010, 63, 763–769. [Google Scholar] [CrossRef]
- Katus, H.A.; Remppis, A.; Scheffold, T.; Diederich, K.W.; Kuebler, W. Intracellular compartmentation of cardiac troponin t and its release kinetics in patients with reperfused and nonreperfused myocardial infarction. Am. J. Cardiol. 1991, 67, 1360–1367. [Google Scholar] [CrossRef]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Simoons, M.L.; Chaitman, B.R.; White, H.D.; Writing Group on behalf of the Joint ESC/ACCF/AHA/WHF Task Force for the Universal Definition of Myocardial Infarction. Third universal definition of myocardial infarction. Glob. Heart 2012, 7, 275–295. [Google Scholar] [CrossRef] [PubMed]
- Stone, N.J.; Robinson, J.G.; Lichtenstein, A.H.; Bairey Merz, C.N.; Blum, C.B.; Eckel, R.H.; Goldberg, A.C.; Gordon, D.; Levy, D.; Lloyd-Jones, D.M.; et al. 2013 acc/aha guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: A report of the american college of cardiology/american heart association task force on practice guidelines. Circulation 2014, 129, S1–S45. [Google Scholar] [CrossRef]
- Anderson, J.L.; Morrow, D.A. Acute myocardial infarction. N. Engl. J. Med. 2017, 376, 2053–2064. [Google Scholar] [CrossRef] [PubMed]
- Reinstadler, S.J.; Feistritzer, H.J.; Klug, G.; Mair, J.; Tu, A.M.; Kofler, M.; Henninger, B.; Franz, W.M.; Metzler, B. High-sensitivity troponin t for prediction of left ventricular function and infarct size one year following st-elevation myocardial infarction. Int. J. Cardiol. 2016, 202, 188–193. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.L.; Phan, J.A.; Hee, L.; Moses, D.A.; Otton, J.; Terreblanche, O.D.; Xiong, J.; Premawardhana, U.; Rajaratnam, R.; Juergens, C.P.; et al. High-sensitivity troponin t predicts infarct scar characteristics and adverse left ventricular function by cardiac magnetic resonance imaging early after reperfused acute myocardial infarction. Am. Heart J. 2015, 170, 715–725.e712. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.H.; Lee, J.S.; Kim, Y.H.; Kim, B.J.; Kim, Y.J.; Kang, D.W.; Kim, J.S.; Kwon, S.U. Prognostic significance of troponin elevation for long-term mortality after ischemic stroke. J. Stroke 2017, 19, 312–322. [Google Scholar] [CrossRef]
- Siasos, G.; Lazaros, G.; Oikonomou, E.; Zografos, T.; Athanasiou, D.; Vavuranakis, M.; Antonopoulos, A.; Tsigkou, V.; Stefanadis, C.; Papavassiliou, A.G.; et al. Different prognostic significance of cardiac troponin at presentation and peak cardiac troponin in patients with non-st segment elevation myocardial infarction. Cardiology 2016, 134, 384–388. [Google Scholar] [CrossRef] [PubMed]
- Barberi, C.; van den Hondel, K.E. The use of cardiac troponin t (ctnt) in the postmortem diagnosis of acute myocardial infarction and sudden cardiac death: A systematic review. Forensic Sci. Int. 2018, 292, 27–38. [Google Scholar] [CrossRef]
- Palmiere, C.; Tettamanti, C.; Bonsignore, A.; De Stefano, F.; Vanhaebost, J.; Rousseau, G.; Scarpelli, M.P.; Bardy, D. Cardiac troponins and nt-probnp in the forensic setting: Overview of sampling site, postmortem interval, cardiopulmonary resuscitation, and review of the literature. Forensic Sci. Int. 2018, 282, 211–218. [Google Scholar] [CrossRef]
- Rahimi, R.; Dahili, N.D.; Anuar Zainun, K.; Mohd Kasim, N.A.; Md Noor, S. Post mortem troponin t analysis in sudden death: Is it useful? Malays. J. Pathol. 2018, 40, 143–148. [Google Scholar] [PubMed]
- Zhu, B.L.; Ishida, K.; Taniguchi, M.; Quan, L.; Oritani, S.; Tsuda, K.; Kamikodai, Y.; Fujita, M.Q.; Maeda, H. Possible postmortem serum markers for differentiation between fresh-, saltwater drowning and acute cardiac death: A preliminary investigation. Legal Med. (Tokyo, Japan) 2003, 5, S298–S301. [Google Scholar] [CrossRef]
- Ellingsen, C.L.; Hetland, O. Serum concentrations of cardiac troponin t in sudden death. Am. J. Forensic Med. Pathol. 2004, 25, 213–215. [Google Scholar] [CrossRef] [PubMed]
- Perez-Carceles, M.D.; Noguera, J.; Jimenez, J.L.; Martinez, P.; Luna, A.; Osuna, E. Diagnostic efficacy of biochemical markers in diagnosis post-mortem of ischaemic heart disease. Forensic Sci. Int. 2004, 142, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Martinez Diaz, F.; Rodriguez-Morlensin, M.; Perez-Carceles, M.D.; Noguera, J.; Luna, A.; Osuna, E. Biochemical analysis and immunohistochemical determination of cardiac troponin for the postmortem diagnosis of myocardial damage. Histol. Histopathol. 2005, 20, 475–481. [Google Scholar] [PubMed]
- Khalifa, A.B.; Najjar, M.; Addad, F.; Turki, E.; Mghirbi, T. Cardiac troponin t (ctn t) and the postmortem diagnosis of sudden death. Am. J. Forensic Med. Pathol. 2006, 27, 175–177. [Google Scholar] [CrossRef]
- Batalis, N.I.; Marcus, B.J.; Papadea, C.N.; Collins, K.A. The role of postmortem cardiac markers in the diagnosis of acute myocardial infarction. J. Forensic Sci. 2010, 55, 1088–1091. [Google Scholar] [CrossRef]
- Sun, G.; Lin, X.; Guo, X.; Qu, Y. The blood biochemical value change of 20 patients with myocardial infarction after death. J. Kunming Med Univ. 2011, 32, 112–115, 125. [Google Scholar]
- Remmer, S.; Kuudeberg, A.; Tonisson, M.; Lepik, D.; Vali, M. Cardiac troponin t in forensic autopsy cases. Forensic Sci. Int. 2013, 233, 154–157. [Google Scholar] [CrossRef]
- Sapouna, R.; Gourgiotis, D.; Athanaselis, S.; Papadodima, S.; Spiliopoulou, C. Diagnostic value of cardiac troponin i in postmortem diagnosis of myocardial infarction. Am. J. Forensic Med. Pathol. 2013, 34, 139–141. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Herrera, L.; Valenzuela, A.; Ramos, V.; Blazquez, A.; Villanueva, E. Cardiac troponin t determination by a highly sensitive assay in postmortem serum and pericardial fluid. Forensic Sci. Med. Pathol. 2016, 12, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Carvajal-Zarrabal, O.; Hayward-Jones, P.M.; Nolasco-Hipolito, C.; Barradas-Dermitz, D.M.; Calderon-Garciduenas, A.L.; Lopez-Amador, N. Use of cardiac injury markers in the postmortem diagnosis of sudden cardiac death. J. Forensic Sci. 2017, 62, 1332–1335. [Google Scholar] [CrossRef]
- Beausire, T.; Faouzi, M.; Palmiere, C.; Fracasso, T.; Michaud, K. High-sensitive cardiac troponin hs-tnt levels in sudden deaths related to atherosclerotic coronary artery disease. Forensic Sci. Int. 2018, 289, 238–243. [Google Scholar] [CrossRef]
- Maeda, H.; Zhu, B.L.; Ishikawa, T.; Quan, L.; Michiue, T. Significance of postmortem biochemistry in determining the cause of death. Leg. Med. (Tokyo, Japan) 2009, 11, S46–S49. [Google Scholar] [CrossRef] [PubMed]
- Davies, S.J.; Gaze, D.C.; Collinson, P.O. Investigation of cardiac troponins in postmortem subjects: Comparing antemortem and postmortem levels. Am. J. Forensic Med. Pathol. 2005, 26, 213–215. [Google Scholar] [CrossRef] [PubMed]
- Cocariu, E.A.; Mageriu, V.; Staniceanu, F.; Bastian, A.; Socoliuc, C.; Zurac, S. Correlations between the autolytic changes and postmortem interval in refrigerated cadavers. Rom. J. Intern. Med. Rev. Roum. Med. Interne 2016, 54, 105–112. [Google Scholar] [CrossRef]
- Osuna, E.; Perez-Carceles, M.D.; Alvarez, M.V.; Noguera, J.; Luna, A. Cardiac troponin i (ctn i) and the postmortem diagnosis of myocardial infarction. Int. J. Leg. Med. 1998, 111, 173–176. [Google Scholar] [CrossRef]
- Cina, S.J.; Thompson, W.C.; Fischer, J.R., Jr.; Brown, D.K.; Titus, J.M.; Smialek, J.E. A study of various morphologic variables and troponin i in pericardial fluid as possible discriminators of sudden cardiac death. Am. J. of forensic Med. Pathol. 1999, 20, 333–337. [Google Scholar] [CrossRef]
- Wang, Q.; Michiue, T.; Ishikawa, T.; Zhu, B.L.; Maeda, H. Combined analyses of creatine kinase mb, cardiac troponin i and myoglobin in pericardial and cerebrospinal fluids to investigate myocardial and skeletal muscle injury in medicolegal autopsy cases. Leg. Med. (Tokyo, Japan) 2011, 13, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Aissaoui, A.; Haj Salem, N.; Zaqout, A.; Boughattas, M.; Belhaj, M.; Mosrati, M.A.; Chadly, A. Cardiac troponin i and the post-mortem diagnosis of myocardial damage. Ann. Cardiol. Angeiol. 2013, 62, 248–252. [Google Scholar] [CrossRef] [PubMed]
- Zhu, B.L.; Ishikawa, T.; Michiue, T.; Li, D.R.; Zhao, D.; Kamikodai, Y.; Tsuda, K.; Okazaki, S.; Maeda, H. Postmortem cardiac troponin t levels in the blood and pericardial fluid. Part 2: Analysis for application in the diagnosis of sudden cardiac death with regard to pathology. Leg. Med. 2006, 8, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Zhu, B.L.; Ishikawa, T.; Michiue, T.; Li, D.R.; Zhao, D.; Oritani, S.; Kamikodai, Y.; Tsuda, K.; Okazaki, S.; Maeda, H. Postmortem cardiac troponin t levels in the blood and pericardial fluid. Part 1. Analysis with special regard to traumatic causes of death. Leg. Med. (Tokyo) 2006, 8, 86–93. [Google Scholar] [CrossRef] [PubMed]
- Adams, J.E., 3rd; Abendschein, D.R.; Jaffe, A.S. Biochemical markers of myocardial injury. Is mb creatine kinase the choice for the 1990s? Circulation 1993, 88, 750–763. [Google Scholar] [CrossRef] [PubMed]
- Mao, R.M.; Zheng, P.P.; Zhu, C.R.; Zhu, B.L. The analysis of pericardial fluid in forensic practice. Fa Yi Xue Za Zhi 2010, 26, 202–205. [Google Scholar] [PubMed]
- Vogiatzidis, K.; Zarogiannis, S.G.; Aidonidis, I.; Solenov, E.I.; Molyvdas, P.A.; Gourgoulianis, K.I.; Hatzoglou, C. Physiology of pericardial fluid production and drainage. Front. Physiol. 2015, 6, 62. [Google Scholar] [CrossRef]
- Comment, L.; Reggiani Bonetti, L.; Mangin, P.; Palmiere, C. Measurement of beta-tryptase in postmortem serum, pericardial fluid, urine and vitreous humor in the forensic setting. Forensic Sci. Int. 2014, 240, 29–34. [Google Scholar] [CrossRef]
- Mizutani, T.; Yoshimoto, T.; Ishii, A. Pericardial fluid is suitable as an alternative specimen for the measurement of beta-hydroxybutyrate within 96h after death. Leg. Med. (Tokyo, Japan) 2018, 33, 53–54. [Google Scholar] [CrossRef]
- Cao, Z.; Jia, Y.; Zhu, B. Bnp and nt-probnp as diagnostic biomarkers for cardiac dysfunction in both clinical and forensic medicine. Int. J. Mol. Sci. 2019, 20, 1820. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.H.; Inamori-Kawamoto, O.; Michiue, T.; Ikeda, S.; Ishikawa, T.; Maeda, H. Cardiac biomarkers in blood, and pericardial and cerebrospinal fluids of forensic autopsy cases: A reassessment with special regard to postmortem interval. Leg. Med. (Tokyo, Japan) 2015, 17, 343–350. [Google Scholar] [CrossRef] [PubMed]
- Fathil, M.F.; Md Arshad, M.K.; Gopinath, S.C.; Hashim, U.; Adzhri, R.; Ayub, R.M.; Ruslinda, A.R.; Nuzaihan, M.N.M.; Azman, A.H.; Zaki, M.; et al. Diagnostics on acute myocardial infarction: Cardiac troponin biomarkers. Biosens. Bioelectron. 2015, 70, 209–220. [Google Scholar] [CrossRef] [PubMed]
- Cho, I.H.; Paek, E.H.; Kim, Y.K.; Kim, J.H.; Paek, S.H. Chemiluminometric enzyme-linked immunosorbent assays (elisa)-on-a-chip biosensor based on cross-flow chromatography. Anal. Chim. Acta 2009, 632, 247–255. [Google Scholar] [CrossRef] [PubMed]
- Hayes, M.A.; Petkus, M.M.; Garcia, A.A.; Taylor, T.; Mahanti, P. Demonstration of sandwich and competitive modulated supraparticle fluoroimmunoassay applied to cardiac protein biomarker myoglobin. Analyst 2009, 134, 533–541. [Google Scholar] [CrossRef]
- Dittmer, W.U.; Evers, T.H.; Hardeman, W.M.; Huijnen, W.; Kamps, R.; de Kievit, P.; Neijzen, J.H.; Nieuwenhuis, J.H.; Sijbers, M.J.; Dekkers, D.W.; et al. Rapid, high sensitivity, point-of-care test for cardiac troponin based on optomagnetic biosensor. Clin. Chim. Acta 2010, 411, 868–873. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.-Y.; Bian, Z.-P.; Wang, W.; Wang, W.; Zhu, J.-J. Pdms gold nanoparticle composite film-based silver enhanced colorimetric detection of cardiac troponin i. Sens. Actuators B Chem. 2010, 147, 298–303. [Google Scholar] [CrossRef]
- Liu, J.T.; Chen, C.J.; Ikoma, T.; Yoshioka, T.; Cross, J.S.; Chang, S.J.; Tsai, J.Z.; Tanaka, J. Surface plasmon resonance biosensor with high anti-fouling ability for the detection of cardiac marker troponin t. Anal. Chim. Acta 2011, 703, 80–86. [Google Scholar] [CrossRef]
- De Antonio, M.; Lupon, J.; Galan, A.; Vila, J.; Zamora, E.; Urrutia, A.; Diez, C.; Coll, R.; Altimir, S.; Bayes-Genis, A. Head-to-head comparison of high-sensitivity troponin t and sensitive-contemporary troponin i regarding heart failure risk stratification. Clin. Chim. Acta Int. J. Clin. Chem. 2013, 426, 18–24. [Google Scholar] [CrossRef]
- Tuteja, S.K.; Priyanka; Bhalla, V.; Deep, A.; Paul, A.K.; Suri, C.R. Graphene-gated biochip for the detection of cardiac marker troponin i. Anal. Chim. Acta 2014, 809, 148–154. [Google Scholar] [CrossRef]
- Bhalla, V.; Carrara, S.; Sharma, P.; Nangia, Y.; Raman Suri, C. Gold nanoparticles mediated label-free capacitance detection of cardiac troponin i. Sens. Actuators B Chem. 2012, 161, 761–768. [Google Scholar] [CrossRef]
- Bingisser, R.; Cairns, C.; Christ, M.; Hausfater, P.; Lindahl, B.; Mair, J.; Panteghini, M.; Price, C.; Venge, P. Cardiac troponin: A critical review of the case for point-of-care testing in the ed. Am. J. Emerg. Med. 2012, 30, 1639–1649. [Google Scholar] [CrossRef] [PubMed]
- Sun, K.J.; He, J.T.; Huang, H.Y.; Xue, Y.; Xie, X.L.; Wang, Q. Diagnostic role of serum tryptase in anaphylactic deaths in forensic medicine: A systematic review and meta-analysis. Forensic Sci. Med. Pathol. 2018, 14, 209–215. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Age | PMI (h) | Analyzed Sample(s) | Analyzed Biomarker(s) |
|---|---|---|---|---|---|
| Zhu et al. [25] | 2003 | 0–94 | <48 | Serum | Cardiac troponin T (cTn T) |
| Ellingsen et al. [26] | 2004 | 4–92 | 3–75 | Serum | cTn T |
| Pérez-Cárceles et al. [27] | 2004 | 14–87 | 1–29 | Pericardial fluid and serum | cardiac troponin I (cTn I) |
| Martínez Díaz et al. [28] | 2005 | 12–87 | 2–16 | Pericardial fluid and serum | cTn I |
| Khalifa et al. [29] | 2006 | — | 6–20 | Serum | cTn T |
| Batalis et al. [30] | 2010 | — | <24 | Pericardial fluid and serum | cTn I |
| Sun et al. [31] | 2011 | 0.5–76 | <288 | Serum | cTn I |
| Remmer et al. [32] | 2013 | 25–54 | 8–141 | Pericardial fluid and serum | cTn T |
| Sapouna et al. [33] | 2013 | 13–94 | 8–48 | Pericardial fluid | cTn I |
| González-Herrera et al. [34] | 2016 | 27–95 | 5–34 | Pericardial fluid and serum | cTn T (high-sensitivity assay) |
| Carvajal-Zarrabal et al. [35] | 2017 | 24–74 | <8 | Serum | cTn I and cTn T |
| Beausire et al. [36] | 2018 | 15–75 | <72 | Serum | cTn T (high-sensitivity assay) |
| Rahimi et al. [24] | 2018 | 18–50 | <24 | Serum | cTnT |
| Biomarker | Cause of Death | Included Studies | Weighted Mean Difference (WMD) (95% CI) | p | I2 | p-Value of Heterogeneity |
|---|---|---|---|---|---|---|
| cTn I in pericardial fluid | Cardiac death (myocardial infarction) | 4 | 181.99 (85.40, 278.58) | 0.0002 | 7% | 0.36 |
| cTn T in pericardial fluid | Cardiac death | 2 | 38.55 (−22.18, 99.29) | 0.21 | 83% | 0.02 |
| cTn I in serum | Cardiac death | 5 | 41.60 (13.08, 70.12) | 0.004 | 96% | <0.00001 |
| Myocardial infarction | 4 | 48.68 (−1.16, 98.52) | 0.06 | 96% | <0.00001 | |
| cTn T in serum | Cardiac death | 7 | 93.26 (58.36, 128.15) | <0.00001 | 99% | <0.00001 |
| Myocardial infarction | 4 | 32.27 (1.48, 63.06) | 0.04 | 94% | <0.00001 |
| Study | Quality indicators from the Newcastle–Ottawa Scale | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Selection | Comparable | Outcome Assessment | Scores | |||||||
| ① | ② | ③ | ④ | ⑤ | ⑥ | ⑦ | ⑧ | ⑨ | ||
| Zhu et al., 2003 [25] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 | |
| Ellingsen et al., 2004 [26] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 | ||
| Pérez-Cárceles et al., 2004 [27] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 | |
| Martínez Díaz et al., 2005 [28] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 | |
| Khalifa et al., 2006 [29] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 | |
| Batalis et al., 2010 [30] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 | |
| Sun et al., 2011 [31] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 | ||
| Remmer et al., 2013 [32] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 | ||
| Sapouna et al., 2013 [33] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 | |
| González-Herrera et al., 2016 [34] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 | |
| Carvajal-Zarrabal et al., 2017 [35] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 | |
| Beausire et al., 2018 [36] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 | ||
| Rahimi et al., 2018 [24] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cao, Z.; Zhao, M.; Xu, C.; Zhang, T.; Jia, Y.; Wang, T.; Zhu, B. Diagnostic Roles of Postmortem cTn I and cTn T in Cardiac Death with Special Regard to Myocardial Infarction: A Systematic Literature Review and Meta-Analysis. Int. J. Mol. Sci. 2019, 20, 3351. https://doi.org/10.3390/ijms20133351
Cao Z, Zhao M, Xu C, Zhang T, Jia Y, Wang T, Zhu B. Diagnostic Roles of Postmortem cTn I and cTn T in Cardiac Death with Special Regard to Myocardial Infarction: A Systematic Literature Review and Meta-Analysis. International Journal of Molecular Sciences. 2019; 20(13):3351. https://doi.org/10.3390/ijms20133351
Chicago/Turabian StyleCao, Zhipeng, Mengyang Zhao, Chengyang Xu, Tianyi Zhang, Yuqing Jia, Tianqi Wang, and Baoli Zhu. 2019. "Diagnostic Roles of Postmortem cTn I and cTn T in Cardiac Death with Special Regard to Myocardial Infarction: A Systematic Literature Review and Meta-Analysis" International Journal of Molecular Sciences 20, no. 13: 3351. https://doi.org/10.3390/ijms20133351
APA StyleCao, Z., Zhao, M., Xu, C., Zhang, T., Jia, Y., Wang, T., & Zhu, B. (2019). Diagnostic Roles of Postmortem cTn I and cTn T in Cardiac Death with Special Regard to Myocardial Infarction: A Systematic Literature Review and Meta-Analysis. International Journal of Molecular Sciences, 20(13), 3351. https://doi.org/10.3390/ijms20133351