Figure 1.
A diagram of three-layer (tripartite) network of drugs, biological functions, and adverse drug reactions (ADRs). This diagram includes two drugs (X and Y), where each drug may perturb biological functions. Drug X perturbs biological functions A and B, while drug Y perturbs biological functions D and E. Both drugs can also perturb function C. Each biological function perturbation may be associated with certain ADRs. Some ADRs are associated only with one drug (ADRs 1, 2, and 3 are only associated with drug X through biological function A, while ADR 6 is associated only with drug Y through biological function E). Some ADRs may be associated with both drugs. ADR 4 is associated with a function that may be perturbed by both drugs, an example of our “mode 1” model in this study. ADR 5 is associated with both drugs through different biological functions B and D, each of which is perturbed by drugs X and Y, respectively. ADR 5 is an example of our “mode 2” model in this study.
Figure 1.
A diagram of three-layer (tripartite) network of drugs, biological functions, and adverse drug reactions (ADRs). This diagram includes two drugs (X and Y), where each drug may perturb biological functions. Drug X perturbs biological functions A and B, while drug Y perturbs biological functions D and E. Both drugs can also perturb function C. Each biological function perturbation may be associated with certain ADRs. Some ADRs are associated only with one drug (ADRs 1, 2, and 3 are only associated with drug X through biological function A, while ADR 6 is associated only with drug Y through biological function E). Some ADRs may be associated with both drugs. ADR 4 is associated with a function that may be perturbed by both drugs, an example of our “mode 1” model in this study. ADR 5 is associated with both drugs through different biological functions B and D, each of which is perturbed by drugs X and Y, respectively. ADR 5 is an example of our “mode 2” model in this study.
Figure 2.
Tripartite Drug–GO–ADR network. Drugs are represented by purple diamonds, which are connected to Gene Ontology (GO) terms, represented by blue circles, which may be perturbed by the drug. In turn, GO terms are connected to those adverse drug reactions (ADRs), represented by red squares, that may manifest if said GO term is perturbed. In panel (A), the full network is shown. Panel (B) shows a subgraph of 10 (arbitrarily selected) drugs with their associated GO terms and ADRs.
Figure 2.
Tripartite Drug–GO–ADR network. Drugs are represented by purple diamonds, which are connected to Gene Ontology (GO) terms, represented by blue circles, which may be perturbed by the drug. In turn, GO terms are connected to those adverse drug reactions (ADRs), represented by red squares, that may manifest if said GO term is perturbed. In panel (A), the full network is shown. Panel (B) shows a subgraph of 10 (arbitrarily selected) drugs with their associated GO terms and ADRs.
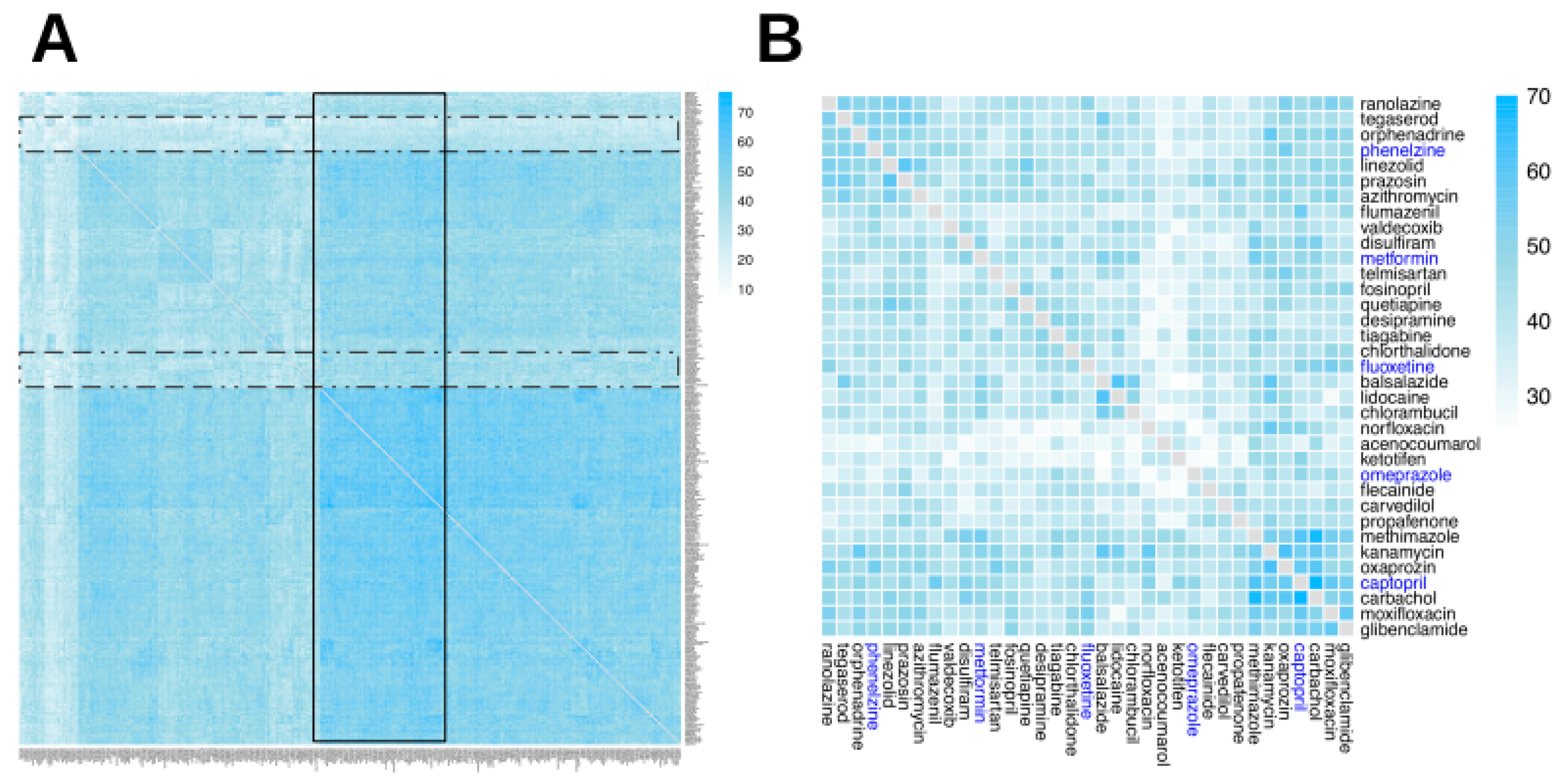
Figure 3.
Composite ADR heatmap. Heatmap of two-drug combination composite ADRs (cADRs). Composite ADRs are reactions that may be caused by any of the drugs in the combination. The heatmap is organized using a hierarchical clustering (a connectivity-based grouping method, in which a set of dissimilarities is generated from the original matrix data, and each drug is iteratively assigned to a cluster). (A) The complete heatmap, containing all 315 drugs; a band of drugs with more cADRs (highlighted in a solid line rectangle), as well as a narrow band of drugs with few cADRs (highlighted in a dotted rectangle) are shown. (B) A subset of the heatmap, containing 35 drugs: five drugs highlighted in blue, which are used in examples in the Discussion section, and the six drugs most similar to each of them (in terms of the number of cADRs) from Panel A.
Figure 3.
Composite ADR heatmap. Heatmap of two-drug combination composite ADRs (cADRs). Composite ADRs are reactions that may be caused by any of the drugs in the combination. The heatmap is organized using a hierarchical clustering (a connectivity-based grouping method, in which a set of dissimilarities is generated from the original matrix data, and each drug is iteratively assigned to a cluster). (A) The complete heatmap, containing all 315 drugs; a band of drugs with more cADRs (highlighted in a solid line rectangle), as well as a narrow band of drugs with few cADRs (highlighted in a dotted rectangle) are shown. (B) A subset of the heatmap, containing 35 drugs: five drugs highlighted in blue, which are used in examples in the Discussion section, and the six drugs most similar to each of them (in terms of the number of cADRs) from Panel A.
Figure 4.
Heatmap of two-drug combination cADRs via mode 1 configuration. The mode 1 configuration indicates that the two drugs in the combination may perturb the same GO term, which in turn may lead to cADR manifestation. The heatmap is organized using a hierarchical clustering. The heatmap indicates that most drug pairs have a large number of mode 1 configurations. (A) The complete heatmap, containing all 315 drugs; two narrow bands of drugs with few mode 1 configurations (dotted rectangles) and a wide band of drugs with many mode 1 configurations (solid line rectangle) are shown. (B) A subset of the heatmap, containing 35 drugs: five drugs highlighted in blue, which are used in examples in the Discussion section, and the six drugs most similar to each of them (in terms of the number of instances of mode 1 configurations) from Panel A.
Figure 4.
Heatmap of two-drug combination cADRs via mode 1 configuration. The mode 1 configuration indicates that the two drugs in the combination may perturb the same GO term, which in turn may lead to cADR manifestation. The heatmap is organized using a hierarchical clustering. The heatmap indicates that most drug pairs have a large number of mode 1 configurations. (A) The complete heatmap, containing all 315 drugs; two narrow bands of drugs with few mode 1 configurations (dotted rectangles) and a wide band of drugs with many mode 1 configurations (solid line rectangle) are shown. (B) A subset of the heatmap, containing 35 drugs: five drugs highlighted in blue, which are used in examples in the Discussion section, and the six drugs most similar to each of them (in terms of the number of instances of mode 1 configurations) from Panel A.
Figure 5.
Heatmap of two-drug combination cADRs via mode 2 configuration. The mode 2 configuration indicates that each drug in the combination may perturb a different GO term that is associated with cADR manifestation. The heatmap is organized using a hierarchical clustering. It can be seen that most of most drug pairs exhibit a large number of mode 2 configurations. (A) The complete heatmap, containing all 315 drugs; a band of drugs with the most mode 2 configurations is shown (inside the solid line rectangle). (B) A subset of the heatmap, containing 35 drugs: five drugs highlighted in blue, which are used in examples in the Discussion section, and the six drugs most similar to each of them (in terms of number of instances of mode 2 configurations) from Panel A.
Figure 5.
Heatmap of two-drug combination cADRs via mode 2 configuration. The mode 2 configuration indicates that each drug in the combination may perturb a different GO term that is associated with cADR manifestation. The heatmap is organized using a hierarchical clustering. It can be seen that most of most drug pairs exhibit a large number of mode 2 configurations. (A) The complete heatmap, containing all 315 drugs; a band of drugs with the most mode 2 configurations is shown (inside the solid line rectangle). (B) A subset of the heatmap, containing 35 drugs: five drugs highlighted in blue, which are used in examples in the Discussion section, and the six drugs most similar to each of them (in terms of number of instances of mode 2 configurations) from Panel A.
Figure 6.
Heatmap of two-drug combination composite risk modules (CRMs). A CRM is a set of GO terms and cADRs that are independently associated in such a way that the manifestation of a cADR in the CRM may only be associated with the perturbation of GO terms in the same CRM. The manifestation of more than one cADR from the same CRM may then be thought to be associated with the perturbation of the same set of GO terms. The heatmap is organized using a hierarchical clustering. (A) The complete heatmap, containing all 315 drugs. A narrow band of drugs that exhibit the highest number of CRMs is highlighted (inside a solid line rectangle), as well as a wide band of drugs with a low number of CRMs (inside the dotted line rectangle). (B) A subset of the heatmap, containing 35 drugs: five drugs highlighted in blue, which are used in examples in the Discussion section, and the six drugs most similar to each of them (in terms of number of CRMs) from Panel A.
Figure 6.
Heatmap of two-drug combination composite risk modules (CRMs). A CRM is a set of GO terms and cADRs that are independently associated in such a way that the manifestation of a cADR in the CRM may only be associated with the perturbation of GO terms in the same CRM. The manifestation of more than one cADR from the same CRM may then be thought to be associated with the perturbation of the same set of GO terms. The heatmap is organized using a hierarchical clustering. (A) The complete heatmap, containing all 315 drugs. A narrow band of drugs that exhibit the highest number of CRMs is highlighted (inside a solid line rectangle), as well as a wide band of drugs with a low number of CRMs (inside the dotted line rectangle). (B) A subset of the heatmap, containing 35 drugs: five drugs highlighted in blue, which are used in examples in the Discussion section, and the six drugs most similar to each of them (in terms of number of CRMs) from Panel A.
Figure 7.
Fluoxetine–phenelzine drug combination network visualization. This is a visualization of the subgraph containing the GO terms and ADRs associated with fluoxetine and phenelzine, two drugs that, in combination, may produce serotonin syndrome. The two drugs are represented by purple diamonds, the 107 GO terms as blue circles, and the 72 ADRs as red squares.
Figure 7.
Fluoxetine–phenelzine drug combination network visualization. This is a visualization of the subgraph containing the GO terms and ADRs associated with fluoxetine and phenelzine, two drugs that, in combination, may produce serotonin syndrome. The two drugs are represented by purple diamonds, the 107 GO terms as blue circles, and the 72 ADRs as red squares.
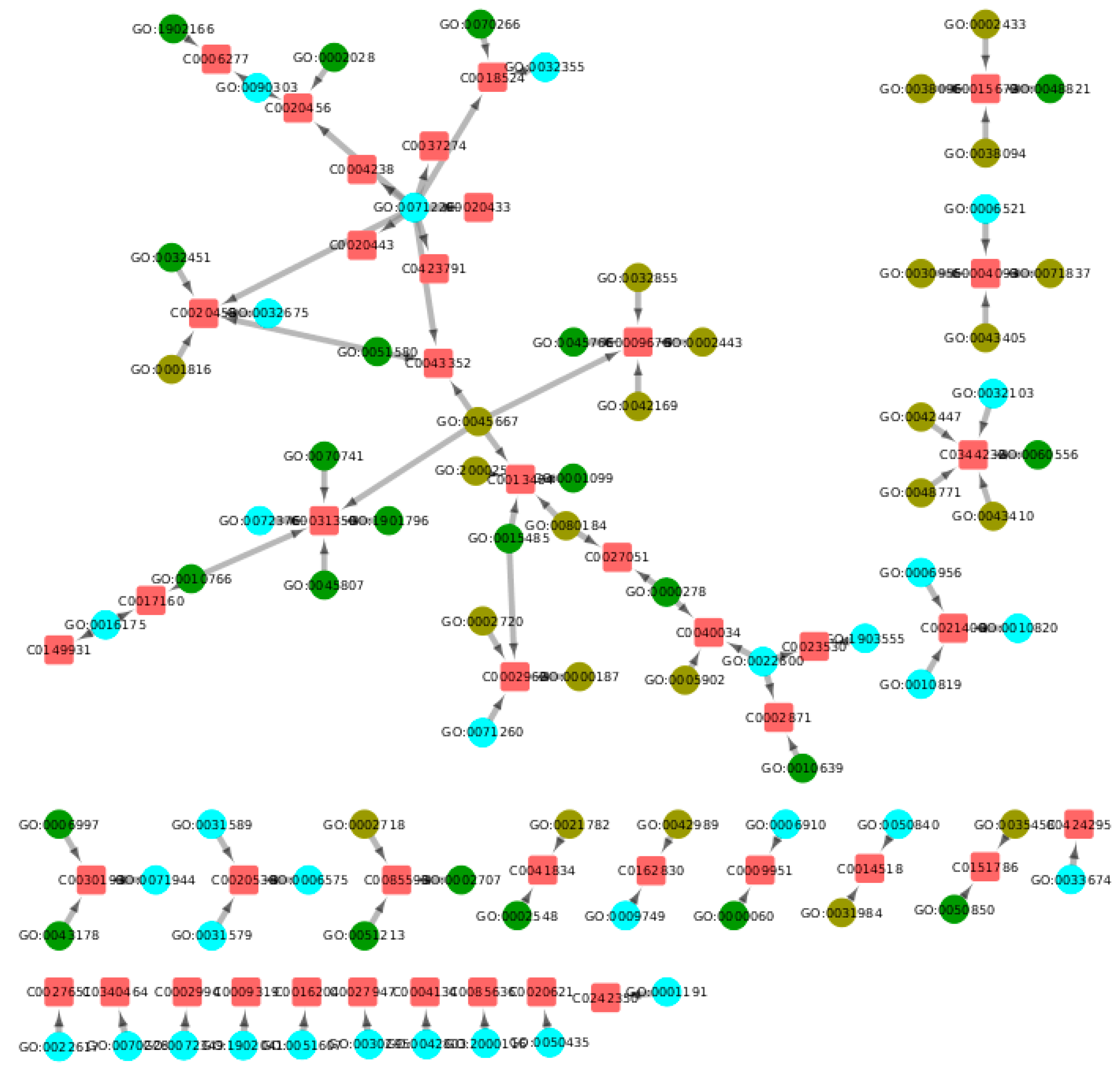
Figure 8.
Fluoxetine–phenelzine drug combination network cADR space. This is a visualization of the subgraph containing the cADRs and associated GO terms for the phenelzine and fluoxetine combination. The cADRs are represented as red squares. The two drugs are represented by a light brown and a dark green diamond, respectively. GO terms associated exclusively with phenelzine are represented as light brown circles, and those exclusively associated with fluoxetine as dark green circles, whereas GO terms associated with both drugs are colored blue.
Figure 8.
Fluoxetine–phenelzine drug combination network cADR space. This is a visualization of the subgraph containing the cADRs and associated GO terms for the phenelzine and fluoxetine combination. The cADRs are represented as red squares. The two drugs are represented by a light brown and a dark green diamond, respectively. GO terms associated exclusively with phenelzine are represented as light brown circles, and those exclusively associated with fluoxetine as dark green circles, whereas GO terms associated with both drugs are colored blue.
Figure 9.
Fluoxetine–phenelzine drug combination network CRMs. This is a visualization of the CRMs for the phenelzine–fluoxetine combination. In this visualization, those GO terms associated only with phenelzine are light brown, those associated only with fluoxetine are dark green, and those associated with both are blue. The red squares represent cADRs. The largest CRM contains 20 different cADRs. The remaining 23 cADRs are independent of each other, each belonging to its own small CRM.
Figure 9.
Fluoxetine–phenelzine drug combination network CRMs. This is a visualization of the CRMs for the phenelzine–fluoxetine combination. In this visualization, those GO terms associated only with phenelzine are light brown, those associated only with fluoxetine are dark green, and those associated with both are blue. The red squares represent cADRs. The largest CRM contains 20 different cADRs. The remaining 23 cADRs are independent of each other, each belonging to its own small CRM.
Figure 10.
A subgraph of fluoxetine and phenelzine with five pathways. This is an illustration of the manifestation of blurred vision as an ADR to the administration of phenelzine and fluoxetine. Phenelzine and fluoxetine may both perturb the positive regulation of the response to an external stimulus GO term in a mode 1 configuration. Additionally, mode 2 contributions may be observed, with fluoxetine being independently able to perturb the regulation of the vitamin D biosynthetic process and phenelzine being able to perturb the positive regulation of MAPK cascade, hormone catabolic processes, and tissue remodeling. The perturbation of any such GO terms may lead to the manifestation of blurred vision.
Figure 10.
A subgraph of fluoxetine and phenelzine with five pathways. This is an illustration of the manifestation of blurred vision as an ADR to the administration of phenelzine and fluoxetine. Phenelzine and fluoxetine may both perturb the positive regulation of the response to an external stimulus GO term in a mode 1 configuration. Additionally, mode 2 contributions may be observed, with fluoxetine being independently able to perturb the regulation of the vitamin D biosynthetic process and phenelzine being able to perturb the positive regulation of MAPK cascade, hormone catabolic processes, and tissue remodeling. The perturbation of any such GO terms may lead to the manifestation of blurred vision.
Figure 11.
Captopril, metformin, and omeprazole drug combination network visualization. This is a visualization of the subgraph containing the GO terms and ADRs associated with the three drugs. The drugs are represented as purple diamonds, the GO terms as blue circles, and the ADRs as red squares.
Figure 11.
Captopril, metformin, and omeprazole drug combination network visualization. This is a visualization of the subgraph containing the GO terms and ADRs associated with the three drugs. The drugs are represented as purple diamonds, the GO terms as blue circles, and the ADRs as red squares.
Figure 12.
Captopril, metformin, and omeprazole drug combination network CRMs. In this visualization, red squares represent cADRs, and blue circles represent GO terms.
Figure 12.
Captopril, metformin, and omeprazole drug combination network CRMs. In this visualization, red squares represent cADRs, and blue circles represent GO terms.
Figure 13.
A subgraph of omeprazole, captopril, and metformin and their GO term targets involved in the manifestation of the dry mouth ADR. It may be seen that there are nine different GO terms that, when perturbed by these drugs, may lead to the manifestation of the dry mouth ADR. Three of these GO terms are exclusively perturbed by omeprazole, four exclusively by metformin, and the rest may be perturbed by any of the drugs. Notice there is no GO term that is exclusively associated with captopril.
Figure 13.
A subgraph of omeprazole, captopril, and metformin and their GO term targets involved in the manifestation of the dry mouth ADR. It may be seen that there are nine different GO terms that, when perturbed by these drugs, may lead to the manifestation of the dry mouth ADR. Three of these GO terms are exclusively perturbed by omeprazole, four exclusively by metformin, and the rest may be perturbed by any of the drugs. Notice there is no GO term that is exclusively associated with captopril.
Table 1.
Topological parameters of the Drug–GO–ADR tripartite network.
Table 1.
Topological parameters of the Drug–GO–ADR tripartite network.
| Nodes and Edges | Counts |
|---|
| Drug Nodes | 3454 |
| GO Nodes | 323 |
| ADR Nodes | 111 |
| Drug to GO Edges | 258,793 |
| GO to ADR Edges | 419 |
Table 2.
Topological parameters of the fluoxetine–phenelzine drug combination network.
Table 2.
Topological parameters of the fluoxetine–phenelzine drug combination network.
| Parameter | Values |
|---|
| GO terms | 107 |
| ADRs | 72 |
| cADRs | 43 |
| GO nodes in mode 1 configurations | 32 |
| GO nodes in mode 2 configurations | 47 |
| CRMs | 24 |
| Size of largest CRM (ADR/GO) | 53 (20/33) |


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}