Imaging of Metastatic Cancer Cells in Sentinel Lymph Nodes using Affibody Probes and Possibility of a Theranostic Approach

 ,
,  ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
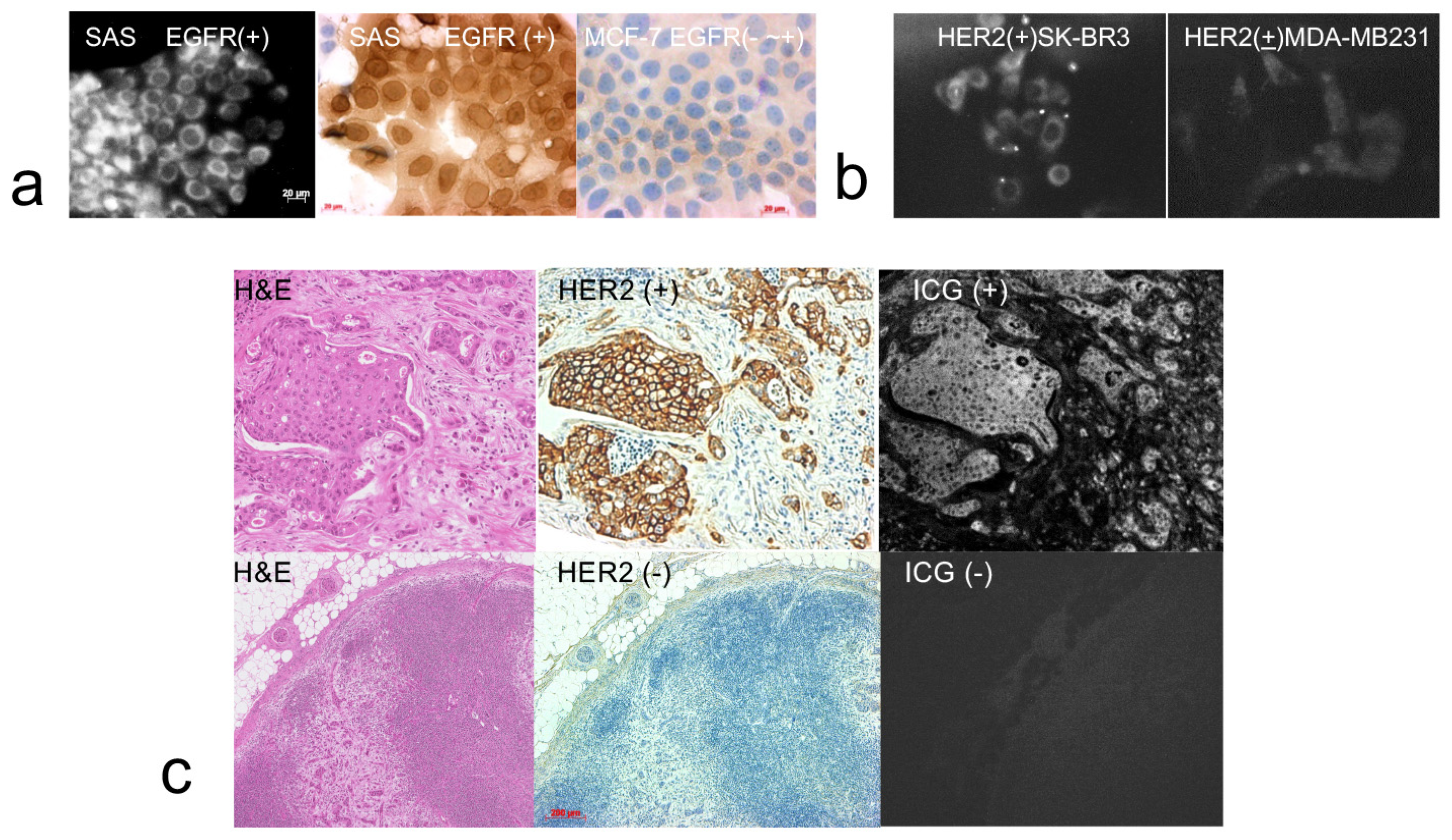
2.1. Cell Culture
2.2. Section Analysis
2.3. Combined Imaging
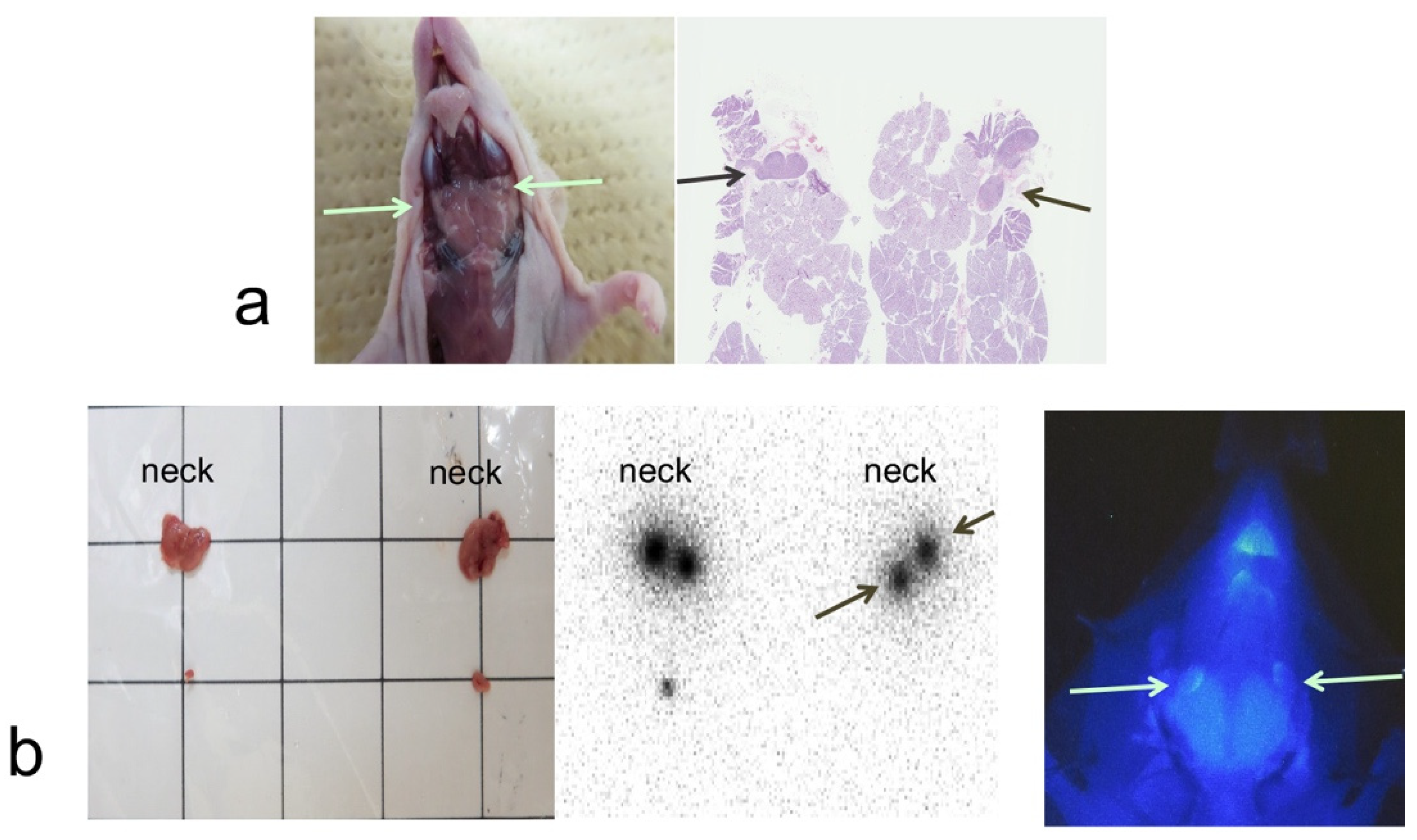
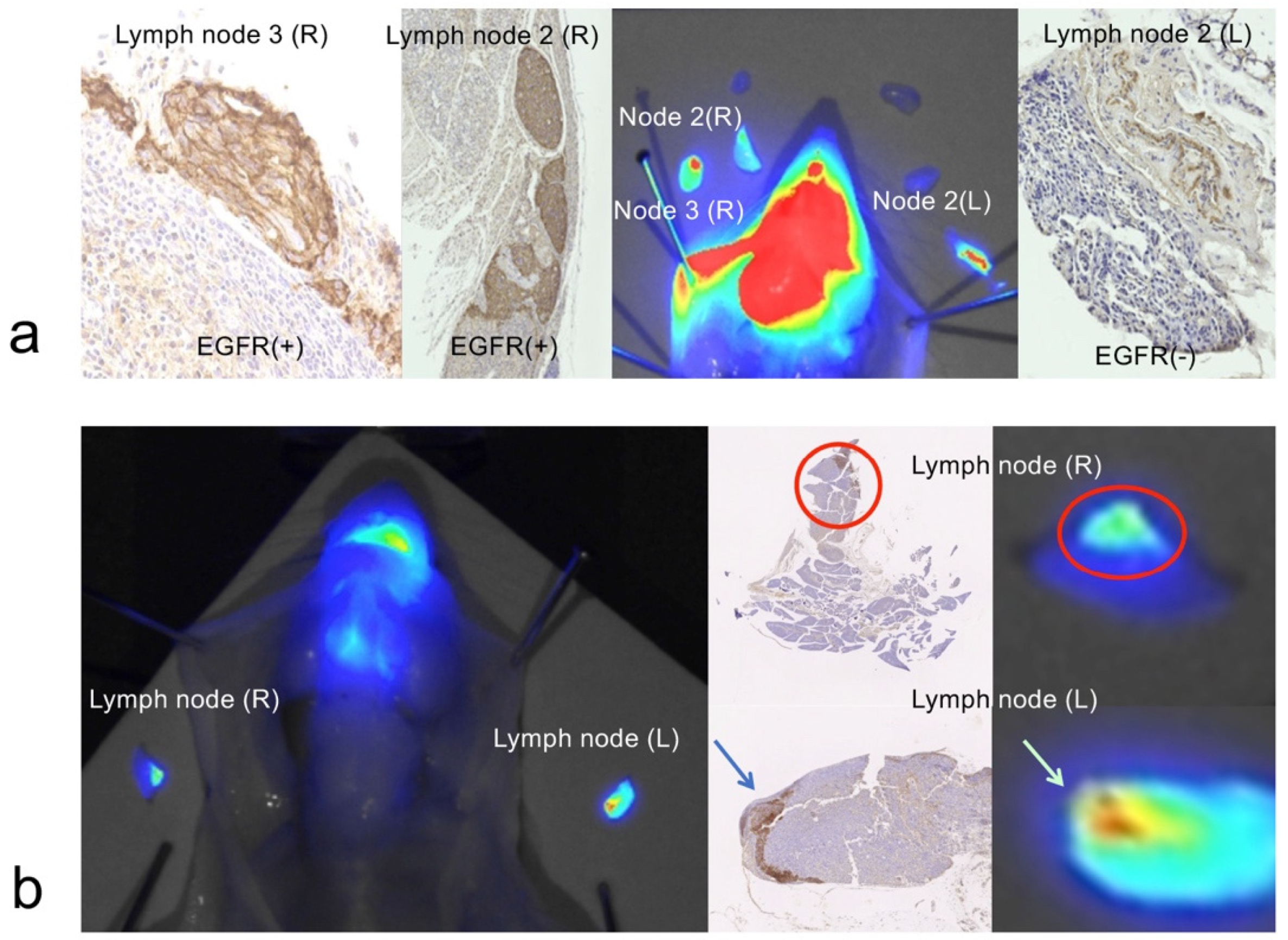
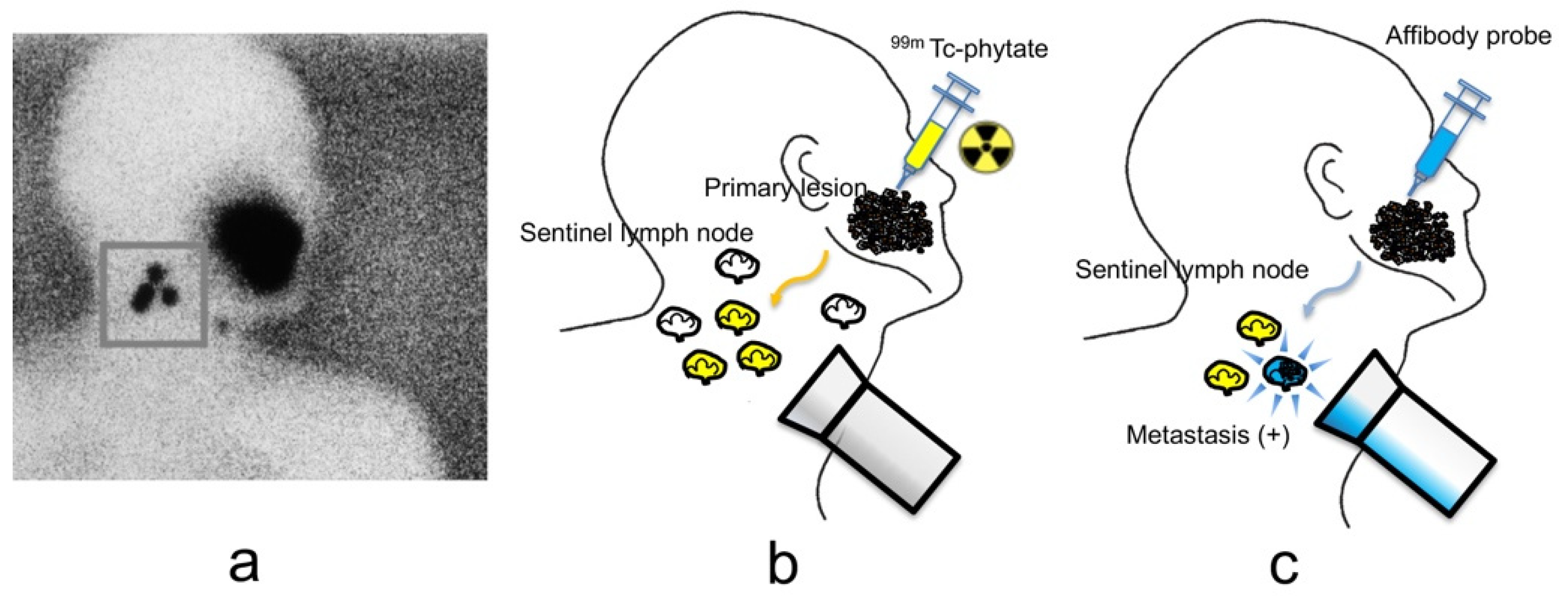
2.4. NIR Fluorescence Imaging of Cancer Cells in Lymph Nodes
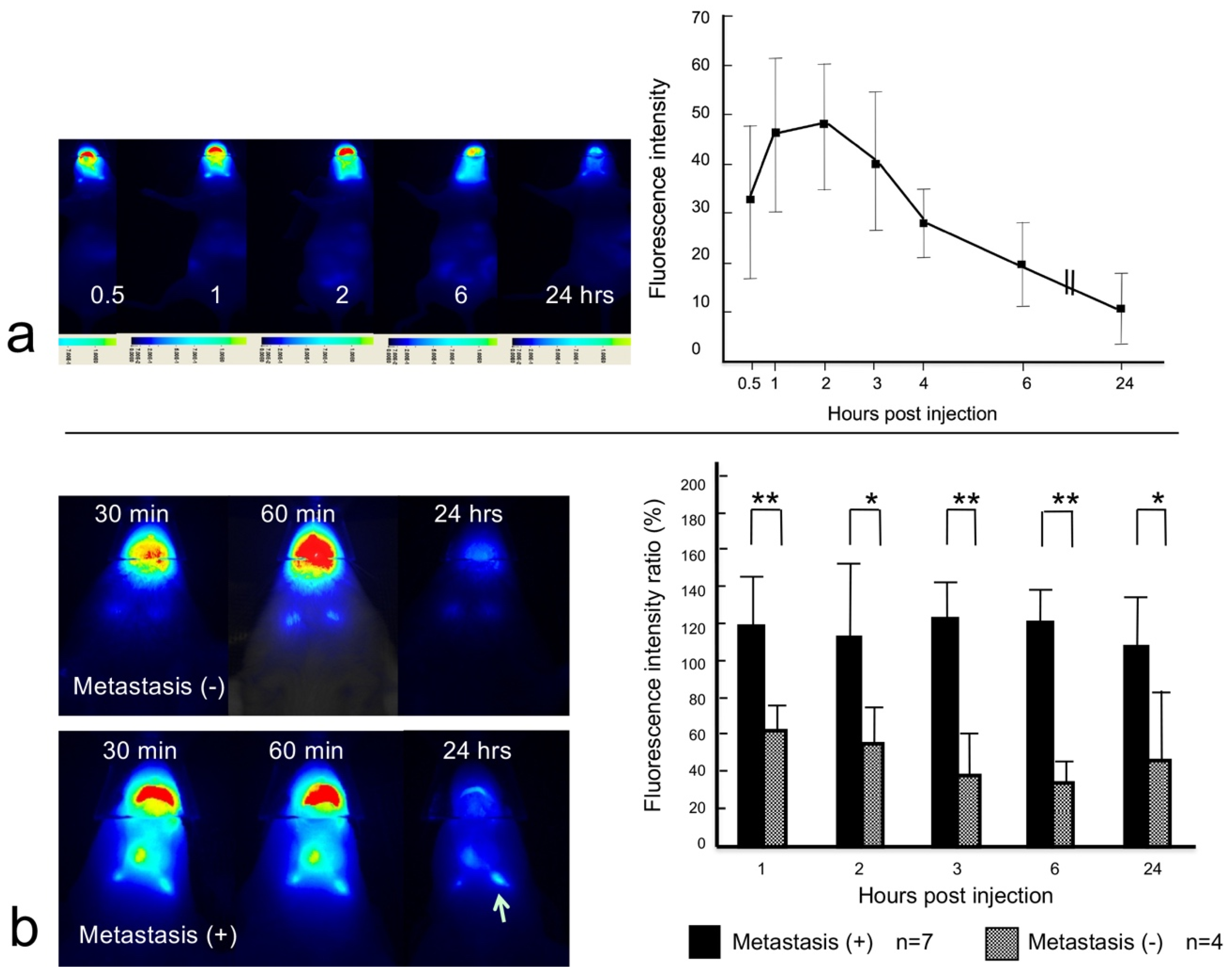
2.5. Dynamic NIR Fluorescence Imaging
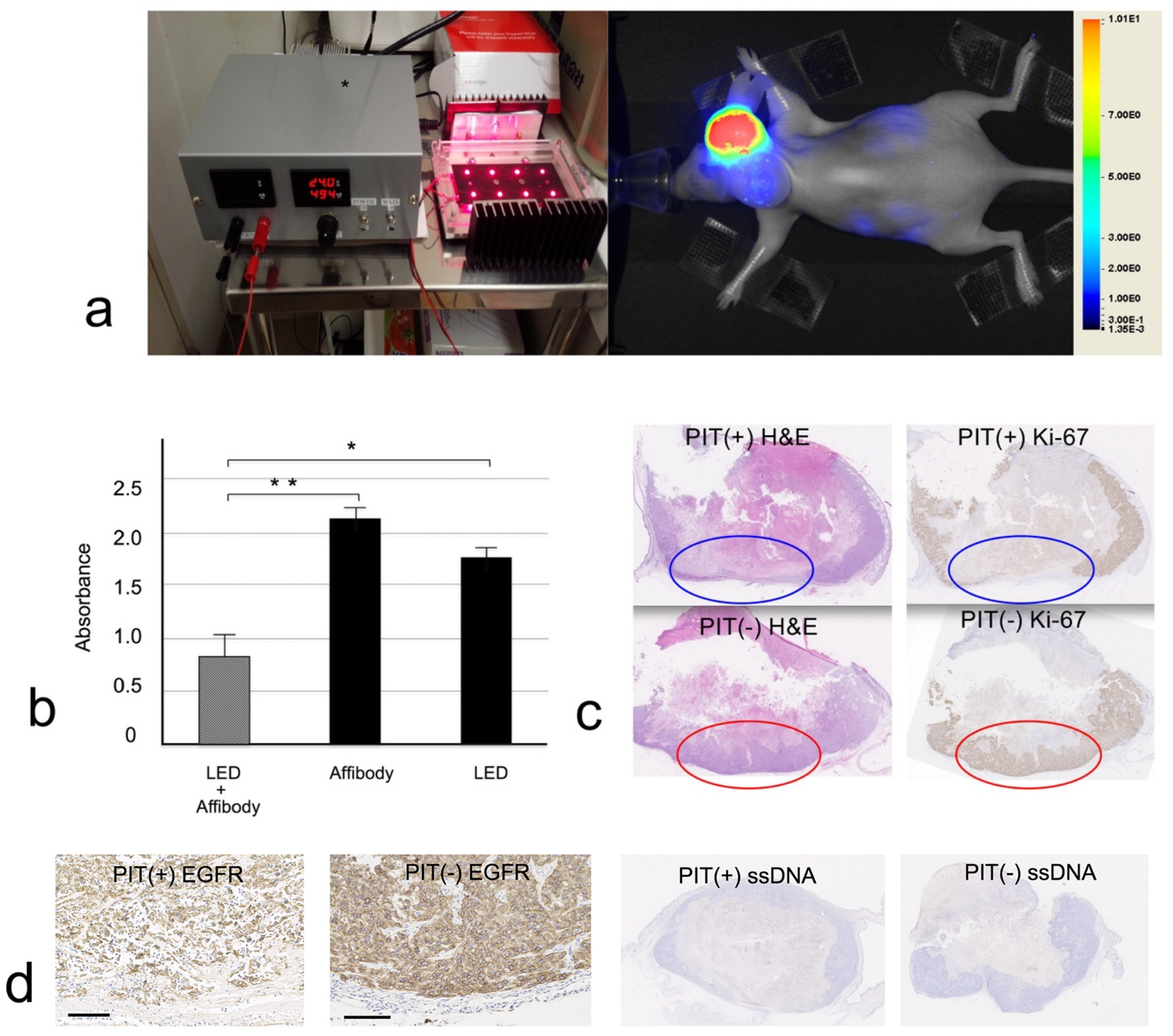
2.6. In Vitro PIT
2.7. In Vivo PIT
3. Discussion
4. Materials and Methods
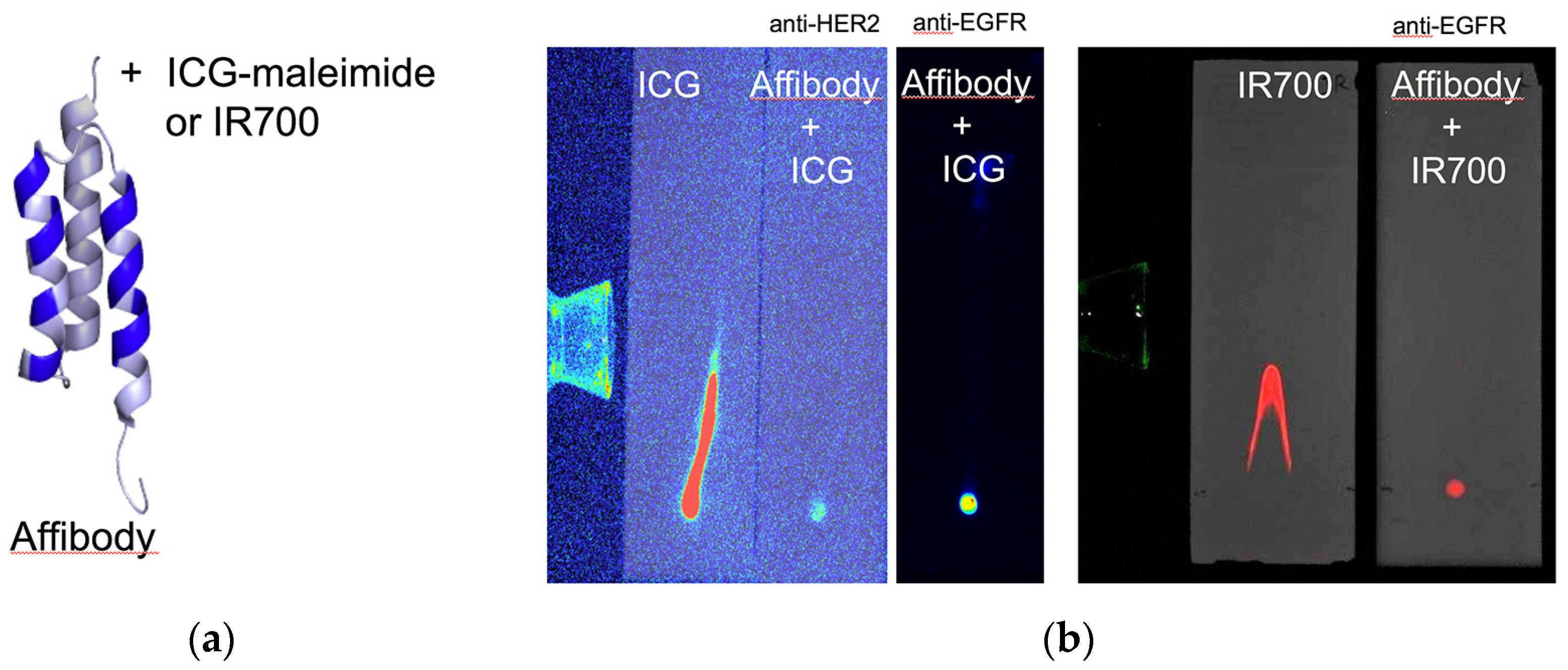
4.1. Affibody Fluorescence Imaging Probes
4.2. Cell Culture
4.3. Analysis of Metastasis Lymph Node Sections from Breast Cancer Patients
4.3.1. Immunohistochemical Examination
4.3.2. Anti-HER2 Affibody Fluorescence Imaging Probe
4.4. Animal Imaging
4.4.1. Metastatic Oral Cancer Mouse Model
4.4.2. 99mTc-phytate Lymph Node Imaging
4.4.3. NIR Imaging
4.4.4. Dynamic NIR Fluorescence Imaging
4.4.5. Combined Imaging Method
4.4.6. Immunohistochemical Examination
4.5. PIT
4.5.1. Affibody PIT Probe
4.5.2. In Vitro PIT
4.5.3. In Vivo PIT
4.6. Statistical Analysis
5. Conclusions
Ethics Approval
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| cRGDY | cyclic arginine-glycine-aspartic acid-tyrosine |
| CT | computed tomography |
| DMSO | dimethyl sulfoxide |
| DTT | dithiothreitol |
| EGFR | epidermal growth factor receptor |
| FDA | U.S. Food and Drug Administration |
| HER2 | human epidermal growth factor receptor 2 |
| ICG | indocyanine green |
| NIR | near-infrared |
| mAbs | monoclonal antibodies |
| MRI | magnetic resonance imaging |
| PBS | phosphate-buffered saline |
| PEG | polyethylene glycol |
| PET | positron emission tomography |
| PIT | photoimmunotherapy |
| SCC | squamous cell carcinoma |
| ssDNA | single-stranded deoxyribonucleic acid |
| SLN | sentinel lymph node |
| TEM | transmission electron microscopy |
| TLC | thin-layer chromatography |
References
- Mariani, G.; Moresco, L.; Viale, G.; Villa, G.; Bagnasco, M.; Canavese, G.; Buscombe, J.; Strauss, H.W.; Paganelli, G. Radioguided sentinel lymph node biopsy in breast cancer surgery. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2001, 42, 1198–1215. [Google Scholar]
- Mariani, G.; Gipponi, M.; Moresco, L.; Villa, G.; Bartolomei, M.; Mazzarol, G.; Bagnara, M.C.; Romanini, A.; Cafiero, F.; Paganelli, G.; et al. Radioguided sentinel lymph node biopsy in malignant cutaneous melanoma. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2002, 43, 811–827. [Google Scholar]
- Cheng, G.; Kurita, S.; Torigian, D.A.; Alavi, A. Current status of sentinel lymph-node biopsy in patients with breast cancer. Eur. J. Nucl. Med. Mol. Imaging 2011, 38, 562–575. [Google Scholar] [CrossRef] [PubMed]
- Thompson, C.F.; St John, M.A.; Lawson, G.; Grogan, T.; Elashoff, D.; Mendelsohn, A.H. Diagnostic value of sentinel lymph node biopsy in head and neck cancer: A meta-analysis. Eur. Arch. Oto-Rhino-Laryngol. 2013, 270, 2115–2122. [Google Scholar] [CrossRef] [PubMed]
- Tsuchimochi, M.; Hayama, K.; Oda, T.; Togashi, M.; Sakahara, H. Evaluation of the efficacy of a small CdTe gamma-camera for sentinel lymph node biopsy. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2008, 49, 956–962. [Google Scholar]
- Tsuchimochi, M.; Hayama, K. Intraoperative gamma cameras for radioguided surgery: Technical characteristics, performance parameters, and clinical applications. Phys. Med. 2013, 29, 126–138. [Google Scholar] [CrossRef] [PubMed]
- Stoffels, I.; Leyh, J.; Poppel, T.; Schadendorf, D.; Klode, J. Evaluation of a radioactive and fluorescent hybrid tracer for sentinel lymph node biopsy in head and neck malignancies: Prospective randomized clinical trial to compare ICG-(99m)Tc-nanocolloid hybrid tracer versus (99m)Tc-nanocolloid. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 1631–1638. [Google Scholar] [CrossRef]
- Seim, N.B.; Wright, C.L.; Agrawal, A. Contemporary use of sentinel lymph node biopsy in the head and neck. World J. Otorhinolaryngol. Head Neck Surg. 2016, 2, 117–125. [Google Scholar] [CrossRef] [Green Version]
- Agrawal, A.; Civantos, F.J.; Brumund, K.T.; Chepeha, D.B.; Hall, N.C.; Carroll, W.R.; Smith, R.B.; Zitsch, R.P.; Lee, W.T.; Shnayder, Y.; et al. [99mTc]Tilmanocept Accurately Detects Sentinel Lymph Nodes and Predicts Node Pathology Status in Patients with Oral Squamous Cell Carcinoma of the Head and Neck: Results of a Phase III Multi-institutional Trial. Ann. Surg. Oncol. 2015, 22, 3708–3715. [Google Scholar] [CrossRef]
- Benezra, M.; Penate-Medina, O.; Zanzonico, P.B.; Schaer, D.; Ow, H.; Burns, A.; DeStanchina, E.; Longo, V.; Herz, E.; Iyer, S.; et al. Multimodal silica nanoparticles are effective cancer-targeted probes in a model of human melanoma. J. Clin. Investig. 2011, 121, 2768–2780. [Google Scholar] [CrossRef]
- Bradbury, M.S.; Phillips, E.; Montero, P.H.; Cheal, S.M.; Stambuk, H.; Durack, J.C.; Sofocleous, C.T.; Meester, R.J.; Wiesner, U.; Patel, S. Clinically-translated silica nanoparticles as dual-modality cancer-targeted probes for image-guided surgery and interventions. Integr. Biol. 2013, 5, 74–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phillips, E.; Penate-Medina, O.; Zanzonico, P.B.; Carvajal, R.D.; Mohan, P.; Ye, Y.; Humm, J.; Gonen, M.; Kalaigian, H.; Schoder, H.; et al. Clinical translation of an ultrasmall inorganic optical-PET imaging nanoparticle probe. Sci. Transl. Med. 2014, 6, 260ra149. [Google Scholar] [CrossRef] [PubMed]
- Bradbury, M.S.; Pauliah, M.; Zanzonico, P.; Wiesner, U.; Patel, S. Intraoperative mapping of sentinel lymph node metastases using a clinically translated ultrasmall silica nanoparticle. Wiley Interdiscip. Reviews. Nanomed. Nanobiotechnol. 2016, 8, 535–553. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Ma, R.; Cao, H.; Wang, Z.; Jing, C.; Sun, Y.; Zhang, Y.; Yang, Z.; Hoffman, R.M.; Tang, J. Intraoperative imaging of metastatic lymph nodes using a fluorophore-conjugated antibody in a HER2/neu-expressing orthotopic breast cancer mouse model. Anticancer Res. 2013, 33, 419–424. [Google Scholar] [PubMed]
- Yang, X.; Wang, Z.; Zhang, F.; Zhu, G.; Song, J.; Teng, G.J.; Niu, G.; Chen, X. Mapping Sentinel Lymph Node Metastasis by Dual-probe Optical Imaging. Theranostics 2017, 7, 153–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beard, P. Biomedical photoacoustic imaging. Interface Focus 2011, 1, 602–631. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stoffels, I.; Morscher, S.; Helfrich, I.; Hillen, U.; Leyh, J.; Burton, N.C.; Sardella, T.C.; Claussen, J.; Poeppel, T.D.; Bachmann, H.S.; et al. Metastatic status of sentinel lymph nodes in melanoma determined noninvasively with multispectral optoacoustic imaging. Sci. Transl. Med. 2015, 7, 317ra199. [Google Scholar] [CrossRef] [PubMed]
- Luke, G.P.; Myers, J.N.; Emelianov, S.Y.; Sokolov, K.V. Sentinel lymph node biopsy revisited: Ultrasound-guided photoacoustic detection of micrometastases using molecularly targeted plasmonic nanosensors. Cancer Res. 2014, 74, 5397–5408. [Google Scholar] [CrossRef]
- Luke, G.P.; Emelianov, S.Y. Label-free Detection of Lymph Node Metastases with US-guided Functional Photoacoustic Imaging. Radiology 2015, 277, 435–442. [Google Scholar] [CrossRef]
- Lofblom, J.; Feldwisch, J.; Tolmachev, V.; Carlsson, J.; Stahl, S.; Frejd, F.Y. Affibody molecules: Engineered proteins for therapeutic, diagnostic and biotechnological applications. FEBS Lett. 2010, 584, 2670–2680. [Google Scholar] [CrossRef] [Green Version]
- Frejd, F.Y.; Kim, K.T. Affibody molecules as engineered protein drugs. Exp. Mol. Med. 2017, 49, e306. [Google Scholar] [CrossRef] [PubMed]
- Stahl, S.; Graslund, T.; Eriksson Karlstrom, A.; Frejd, F.Y.; Nygren, P.A.; Lofblom, J. Affibody Molecules in Biotechnological and Medical Applications. Trends Biotechnol. 2017, 35, 691–712. [Google Scholar] [CrossRef] [PubMed]
- Baum, R.P.; Prasad, V.; Muller, D.; Schuchardt, C.; Orlova, A.; Wennborg, A.; Tolmachev, V.; Feldwisch, J. Molecular imaging of HER2-expressing malignant tumors in breast cancer patients using synthetic 111In- or 68Ga-labeled affibody molecules. J. Nucl. Med. 2010, 51, 892–897. [Google Scholar] [CrossRef] [PubMed]
- Sexton, K.; Tichauer, K.; Samkoe, K.S.; Gunn, J.; Hoopes, P.J.; Pogue, B.W. Fluorescent affibody peptide penetration in glioma margin is superior to full antibody. PLoS ONE 2013, 8, e60390. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, J.; Velikyan, I.; Sandberg, D.; Wennborg, A.; Feldwisch, J.; Tolmachev, V.; Orlova, A.; Sandstrom, M.; Lubberink, M.; Olofsson, H.; et al. Measuring HER2-Receptor Expression In Metastatic Breast Cancer Using [68Ga]ABY-025 Affibody PET/CT. Theranostics 2016, 6, 262–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Souza, A.L.; Marra, K.; Gunn, J.; Samkoe, K.S.; Hoopes, P.J.; Feldwisch, J.; Paulsen, K.D.; Pogue, B.W. Fluorescent Affibody Molecule Administered In Vivo at a Microdose Level Labels EGFR Expressing Glioma Tumor Regions. Mol. Imaging Biol. 2017, 19, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Krasniqi, A.; D’Huyvetter, M.; Devoogdt, N.; Frejd, F.Y.; Sorensen, J.; Orlova, A.; Keyaerts, M.; Tolmachev, V. Same-Day Imaging Using Small Proteins: Clinical Experience and Translational Prospects in Oncology. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2018, 59, 885–891. [Google Scholar] [CrossRef]
- Railkar, R.; Krane, L.S.; Li, Q.Q.; Sanford, T.; Siddiqui, M.R.; Haines, D.; Vourganti, S.; Brancato, S.J.; Choyke, P.L.; Kobayashi, H.; et al. Epidermal Growth Factor Receptor (EGFR)-targeted Photoimmunotherapy (PIT) for the Treatment of EGFR-expressing Bladder Cancer. Mol. Cancer Ther. 2017, 16, 2201–2214. [Google Scholar] [CrossRef] [Green Version]
- Ogata, F.; Nagaya, T.; Nakamura, Y.; Sato, K.; Okuyama, S.; Maruoka, Y.; Choyke, P.L.; Kobayashi, H. Near-infrared photoimmunotherapy: A comparison of light dosing schedules. Oncotarget 2017, 8, 35069–35075. [Google Scholar] [CrossRef]
- Tsuchimochi, M.; Hayama, K.; Toyama, M.; Sasagawa, I.; Tsubokawa, N. Dual-modality imaging with 99mTc and fluorescent indocyanine green using surface-modified silica nanoparticles for biopsy of the sentinel lymph node: An animal study. EJNMMI Res. 2013, 3, 33. [Google Scholar] [CrossRef]
- Frangioni, J.V. New technologies for human cancer imaging. J. Clin. Oncol. 2008, 26, 4012–4021. [Google Scholar] [CrossRef] [PubMed]
- Wu, A.M.; Senter, P.D. Arming antibodies: Prospects and challenges for immunoconjugates. Nat. Biotechnol. 2005, 23, 1137–1146. [Google Scholar] [CrossRef] [PubMed]
- Feldwisch, J.; Tolmachev, V. Engineering of affibody molecules for therapy and diagnostics. Methods Mol. Biol. 2012, 899, 103–126. [Google Scholar] [PubMed]
- Ardeshirpour, Y.; Sackett, D.L.; Knutson, J.R.; Gandjbakhche, A.H. Using in vivo fluorescence lifetime imaging to detect HER2-positive tumors. EJNMMI Res. 2018, 8, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, K.; Chen, H.; Jenkins, C.H.; Zhang, G.; Zhao, W.; Zhang, Z.; Han, F.; Fung, J.; Yang, M.; Jiang, Y.; et al. Synthesis, Characterization, and Biomedical Applications of a Targeted Dual-Modal Near-Infrared-II Fluorescence and Photoacoustic Imaging Nanoprobe. ACS Nano 2017, 11, 12276–12291. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Ballou, B.; Schmidt, B.F.; Andreko, S.; St Croix, C.M.; Watkins, S.C.; Bruchez, M.P. Affibody-targeted fluorogen activating protein for in vivo tumor imaging. Chem. Commun. 2017, 53, 2001–2004. [Google Scholar] [CrossRef] [PubMed]
- Szuba, A.; Shin, W.S.; Strauss, H.W.; Rockson, S. The third circulation: Radionuclide lymphoscintigraphy in the evaluation of lymphedema. J. Nucl. Med. 2003, 44, 43–57. [Google Scholar]
- Lux, A.; Yu, X.; Scanlan, C.N.; Nimmerjahn, F. Impact of immune complex size and glycosylation on IgG binding to human FcgammaRs. J. Immunol. 2013, 190, 4315–4323. [Google Scholar] [CrossRef]
- Lucas, A.; Price, L.; Schorzman, A.; Storrie, M.; Piscitelli, J.; Razo, J.; Zamboni, W. Factors Affecting the Pharmacology of Antibody–Drug Conjugates. Antibodies 2018, 7, 10. [Google Scholar] [CrossRef]
- Keizer, R.J.; Huitema, A.D.; Schellens, J.H.; Beijnen, J.H. Clinical pharmacokinetics of therapeutic monoclonal antibodies. Clin. Pharmacokinet. 2010, 49, 493–507. [Google Scholar] [CrossRef]
- Mitsunaga, M.; Ogawa, M.; Kosaka, N.; Rosenblum, L.T.; Choyke, P.L.; Kobayashi, H. Cancer cell-selective in vivo near infrared photoimmunotherapy targeting specific membrane molecules. Nat. Med. 2011, 17, 1685–1691. [Google Scholar] [CrossRef] [PubMed]
- Moore, L.S.; de Boer, E.; Warram, J.M.; Tucker, M.D.; Carroll, W.R.; Korb, M.L.; Brandwein-Gensler, M.S.; van Dam, G.M.; Rosenthal, E.L. Photoimmunotherapy of residual disease after incomplete surgical resection in head and neck cancer models. Cancer Med. 2016, 5, 1526–1534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kishimoto, S.; Oshima, N.; Yamamoto, K.; Munasinghe, J.; Ardenkjaer-Larsen, J.H.; Mitchell, J.B.; Choyke, P.L.; Krishna, M.C. Molecular imaging of tumor photoimmunotherapy: Evidence of photosensitized tumor necrosis and hemodynamic changes. Free Rad.Biol. Med. 2018, 116, 1–10. [Google Scholar] [CrossRef]
- Clinicaltrials. 2018. Available online: https://clinicaltrials.gov/ct2/show/NCT02422979 (accessed on 15 October 2018).
- Burley, T.A.; Maczynska, J.; Shah, A.; Szopa, W.; Harrington, K.J.; Boult, J.K.R.; Mrozek-Wilczkiewicz, A.; Vinci, M.; Bamber, J.C.; Kaspera, W.; et al. Near-infrared photoimmunotherapy targeting EGFR-Shedding new light on glioblastoma treatment. Int. J. Cancer 2018, 142, 2363–2374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wallberg, H.; Grafstrom, J.; Cheng, Q.; Lu, L.; Martinsson Ahlzen, H.S.; Samen, E.; Thorell, J.O.; Johansson, K.; Dunas, F.; Olofsson, M.H.; et al. HER2-positive tumors imaged within 1 hour using a site-specifically 11C-labeled Sel-tagged affibody molecule. J. Nucl. Med. 2012, 53, 1446–1453. [Google Scholar] [CrossRef] [PubMed]







© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsuchimochi, M.; Yamaguchi, H.; Hayama, K.; Okada, Y.; Kawase, T.; Suzuki, T.; Tsubokawa, N.; Wada, N.; Ochiai, A.; Fujii, S.; et al. Imaging of Metastatic Cancer Cells in Sentinel Lymph Nodes using Affibody Probes and Possibility of a Theranostic Approach. Int. J. Mol. Sci. 2019, 20, 427. https://doi.org/10.3390/ijms20020427
Tsuchimochi M, Yamaguchi H, Hayama K, Okada Y, Kawase T, Suzuki T, Tsubokawa N, Wada N, Ochiai A, Fujii S, et al. Imaging of Metastatic Cancer Cells in Sentinel Lymph Nodes using Affibody Probes and Possibility of a Theranostic Approach. International Journal of Molecular Sciences. 2019; 20(2):427. https://doi.org/10.3390/ijms20020427
Chicago/Turabian StyleTsuchimochi, Makoto, Haruka Yamaguchi, Kazuhide Hayama, Yasuo Okada, Tomoyuki Kawase, Takamasa Suzuki, Norio Tsubokawa, Noriaki Wada, Atsushi Ochiai, Satoshi Fujii, and et al. 2019. "Imaging of Metastatic Cancer Cells in Sentinel Lymph Nodes using Affibody Probes and Possibility of a Theranostic Approach" International Journal of Molecular Sciences 20, no. 2: 427. https://doi.org/10.3390/ijms20020427
APA StyleTsuchimochi, M., Yamaguchi, H., Hayama, K., Okada, Y., Kawase, T., Suzuki, T., Tsubokawa, N., Wada, N., Ochiai, A., Fujii, S., & Fujii, H. (2019). Imaging of Metastatic Cancer Cells in Sentinel Lymph Nodes using Affibody Probes and Possibility of a Theranostic Approach. International Journal of Molecular Sciences, 20(2), 427. https://doi.org/10.3390/ijms20020427