Wisteria floribunda Agglutinin-Positive Mac-2 Binding Protein but not α-fetoprotein as a Long-Term Hepatocellular Carcinoma Predictor

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
Association between WFA±M2BP and Fibrosis Stage
2.2. Prediction of HCC Development Using WFA±M2BP and AFP at SVR24
2.3. Prediction of HCC Development as Per WFA±M2BP and AFP at 1 Year after SVR24
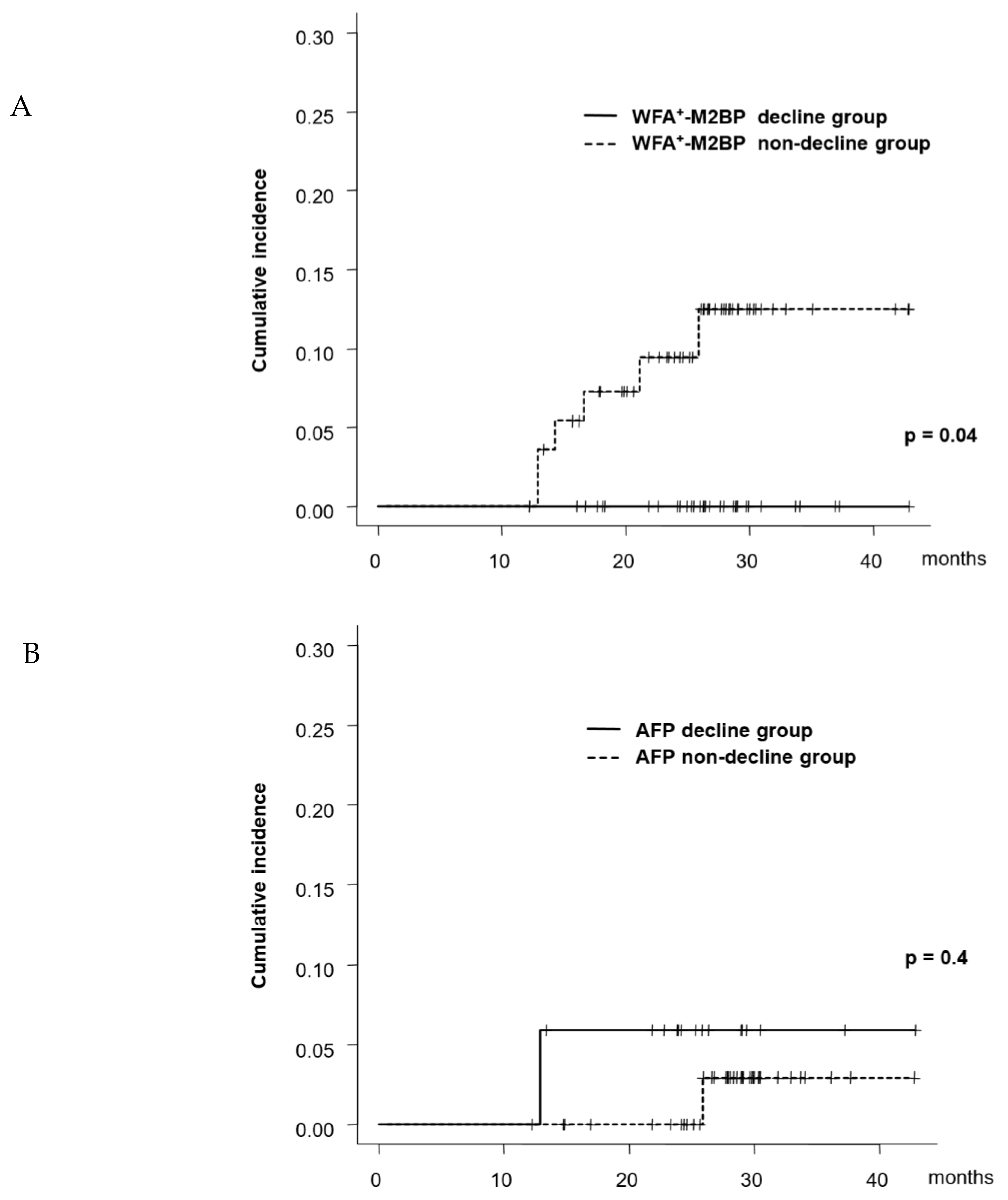
2.4. Time-Course Changes in WFA±M2BP and AFP and HCC Risk
2.5. Association between AFP and LR3/4 nodule
2.6. Multivariable Analysis of Factors at SVR24 Associated with HCC Development
2.7. Multivariable Analysis of Factors at 1 Year after SVR24 Associated with HCC Development
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Clinical and Laboratory Data
4.3. HCC Surveillance and Diagnosis
Histological Evaluation
4.4. Statistical Analyses
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| DAAs | direct-acting antivirals |
| SVR | sustained virological responses |
| HCC | hepatocellular carcinoma |
| AFP | α-fetoprotein |
| SVR24 | 24 weeks after the end of treatment |
| WFA±M2BP | Wisteria floribunda agglutinin-positive mac-2 binding protein |
| ROC | receiver operating characteristic |
| AST | aspartate aminotransferase |
| ALT | alanine aminotransferase |
| LR | the liver imaging reporting and data system |
| HR | hazard ratio |
| CI | 95% confidence interval |
References
- Tsuji, K.; Kurosaki, M.; Itakura, J.; Mori, N.; Takaki, S.; Hasebe, C.; Akahane, T.; Joko, K.; Yagisawa, H.; Takezawa, J.; et al. Real-world efficacy and safety of ledipasvir and sofosbuvir in patients with hepatitis C virus genotype 1 infection: A nationwide multicenter study by the Japanese Red Cross Liver Study Group. J. Gastroenterol. 2018, 53, 1142–1150. [Google Scholar] [CrossRef] [PubMed]
- Suda, G.; Ogawa, K.; Yamamoto, Y.; Katagiri, M.; Furuya, K.; Kumagai, K.; Konno, J.; Kimura, M.; Kawagishi, N.; Ohara, M.; et al. Retreatment with sofosbuvir, ledipasvir, and add-on ribavirin for patients who failed daclatasvir and asunaprevir combination therapy. J. Gastroenterol. 2017, 52, 1122–1129. [Google Scholar] [CrossRef] [PubMed]
- Izumi, N.; Takehara, T.; Chayama, K.; Yatsuhashi, H.; Takaguchi, K.; Ide, T.; Kurosaki, M.; Ueno, Y.; Toyoda, H.; Kakizaki, S.; et al. Sofosbuvir-velpatasvir plus ribavirin in Japanese patients with genotype 1 or 2 hepatitis C who failed direct-acting antivirals. Hepatol. Int. 2018, 12, 356–367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujii, H.; Kimura, H.; Kurosaki, M.; Hasebe, C.; Akahane, T.; Yagisawa, H.; Kato, K.; Yoshida, H.; Itakura, J.; Sakita, S.; et al. Efficacy of daclatasvir plus asunaprevir in patients with hepatitis C virus infection undergoing and not undergoing hemodialysis. Hepatol. Res. 2018, 48, 746–756. [Google Scholar] [CrossRef] [PubMed]
- Akahane, T.; Kurosaki, M.; Itakura, J.; Tsuji, K.; Joko, K.; Kimura, H.; Nasu, A.; Ogawa, C.; Kojima, Y.; Hasebe, C.; et al. Real-world efficacy and safety of sofosbuvir + ribavirin for hepatitis C genotype 2: A nationwide multicenter study by the Japanese Red Cross Liver Study Group. Hepatol. Res. 2019, 49, 264–270. [Google Scholar] [CrossRef] [PubMed]
- Sho, T.; Suda, G.; Nagasaka, A.; Yamamoto, Y.; Furuya, K.; Kumagai, K.; Uebayashi, M.; Terashita, K.; Kobayashi, T.; Tsunematsu, I.; et al. Safety and efficacy of sofosbuvir and ribavirin for genotype 2 hepatitis C Japanese patients with renal dysfunction. Hepatol. Res. 2018, 48, 529–538. [Google Scholar] [CrossRef]
- Kanwal, F.; Kramer, J.; Asch, S.M.; Chayanupatkul, M.; Cao, Y.; El-Serag, H.B. Risk of hepatocellular cancer in HCV patients treated with direct-acting antiviral agents. Gastroenterology 2017, 153, 996–1005. [Google Scholar] [CrossRef] [Green Version]
- Higuchi, M.; Tamaki, N.; Kurosaki, M.; Watakabe, K.; Osawa, L.; Wang, W.; Okada, M.; Shimizu, T.; Takaura, K.; Takada, H.; et al. Prediction of hepatocellular carcinoma after sustained virological responses using magnetic resonance elastography. Clin. Gastroenterol. Hepatol. 2018, 28, 31323–31325. [Google Scholar] [CrossRef]
- Asahina, Y.; Tsuchiya, K.; Nishimura, T.; Muraoka, M.; Suzuki, Y.; Tamaki, N.; Yasui, Y.; Hosokawa, T.; Ueda, K.; Nakanishi, H.; et al. α-fetoprotein levels after interferon therapy and risk of hepatocarcinogenesis in chronic hepatitis C. Hepatology 2013, 58, 1253–1262. [Google Scholar] [CrossRef]
- Asahina, Y.; Tsuchiya, K.; Nishimura, T.; Muraoka, M.; Suzuki, Y.; Tamaki, N.; Yasui, Y.; Hosokawa, T.; Ueda, K.; Nakanishi, H.; et al. Genetic variation near interleukin 28B and the risk of hepatocellular carcinoma in patients with chronic hepatitis C. J. Gastroenterol. 2014, 49, 1152–1162. [Google Scholar] [CrossRef]
- Tada, T.; Kumada, T.; Toyoda, H.; Kiriyama, S.; Tanikawa, M.; Hisanaga, Y.; Kanamori, A.; Kitabatake, S.; Yama, T.; Tanaka, J. Post-treatment levels of α-fetoprotein predict long-term hepatocellular carcinoma development after sustained virological response in patients with hepatitis C. Hepatol. Res. 2017, 47, 1021–1031. [Google Scholar] [CrossRef] [PubMed]
- Yamada, R.; Hiramatsu, N.; Oze, T.; Urabe, A.; Tahata, Y.; Morishita, N.; Kodama, T.; Hikita, H.; Sakamori, R.; Yakushijin, T.; et al. Incidence and risk factors of hepatocellular carcinoma change over time in patients with hepatitis C virus infection who achieved sustained virologic response. Hepatol. Res. 2019, 49, 570–578. [Google Scholar] [CrossRef] [PubMed]
- Tamaki, N.; Higuchi, M.; Kurosaki, M.; Kirino, S.; Osawa, L.; Watakabe, K.; Wang, W.; Okada, M.; Shimizu, T.; Takaura, K.; et al. Risk assessment of hepatocellular carcinoma development by magnetic resonance elastography in chronic hepatitis C patients who achieved sustained virological responses by direct-acting antivirals. J. Viral Hepat. 2019, 26, 893–899. [Google Scholar] [CrossRef] [PubMed]
- Kuno, A.; Ikehara, Y.; Tanaka, Y.; Ito, K.; Matsuda, A.; Sekiya, S.; Hige, S.; Sakamoto, M.; Kage, M.; Mizokami, M.; et al. A serum “sweet-doughnut” protein facilitates fibrosis evaluation and therapy assessment in patients with viral hepatitis. Sci. Rep. 2013, 3, 1065. [Google Scholar] [CrossRef]
- Tamaki, N.; Kurosaki, M.; Kuno, A.; Korenaga, M.; Togayachi, A.; Gotoh, M.; Nakakuki, N.; Takada, H.; Matsuda, S.; Hattori, N.; et al. Wisteria floribundaagglutinin positive human Mac-2-binding protein as a predictor of hepatocellular carcinoma development in chronic hepatitis C patients. Hepatol. Res. 2015, 45, E82–E88. [Google Scholar] [CrossRef]
- Nagata, H.; Nakagawa, M.; Asahina, Y.; Sato, A.; Asano, Y.; Tsunoda, T.; Miyoshi, M.; Kaneko, S.; Otani, S.; Kawai-Kitahata, F.; et al. Effect of interferon-based and -free therapy on early occurrence and recurrence of hepatocellular carcinoma in chronic hepatitis C. J. Hepatol. 2017, 67, 933–939. [Google Scholar] [CrossRef]
- Yasui, Y.; Kurosaki, M.; Komiyama, Y.; Takada, H.; Tamaki, N.; Watakabe, K.; Okada, M.; Wang, W.; Shimizu, T.; Kubota, Y.; et al. Wisteria floribunda agglutinin-positive Mac-2 binding protein predicts early occurrence of hepatocellular carcinoma after sustained virologic response by direct-acting antivirals for hepatitis C virus. Hepatol. Res. 2018, 48, 1131–1139. [Google Scholar] [CrossRef]
- Shiratori, Y.; Imazeki, F.; Moriyama, M.; Yano, M.; Arakawa, Y.; Yokosuka, O.; Kuroki, T.; Nishiguchi, S.; Sata, M.; Yamada, G.; et al. Histologic improvement of fibrosis in patients with hepatitis C who have sustained response to interferon therapy. Ann. Intern. Med. 2000, 132, 517–524. [Google Scholar] [CrossRef]
- Tamaki, N.; Kurosaki, M.; Tanaka, K.; Suzuki, Y.; Hoshioka, Y.; Kato, T.; Yasui, Y.; Hosokawa, T.; Ueda, K.; Tsuchiya, K.; et al. Noninvasive estimation of fibrosis progression overtime using the FIB-4 index in chronic hepatitis C. J. Viral Hepat. 2013, 20, 72–76. [Google Scholar] [CrossRef]
- Tamaki, N.; Kurosaki, M.; Matsuda, S.; Muraoka, M.; Yasui, Y.; Suzuki, S.; Hosokawa, T.; Ueda, K.; Tsuchiya, K.; Nakanishi, H.; et al. Non-invasive prediction of hepatocellular carcinoma development using serum fibrosis marker in chronic hepatitis C patients. J. Gastroenterol. 2014, 49, 1495–1503. [Google Scholar] [CrossRef]
- Elsayes, K.M.; Hooker, J.; Agrons, M.M.; Kielar, A.Z.; Tang, A.; Fowler, K.J.; Chernyak, V.; Bashir, M.R.; Kono, Y.; Do, R.K.; et al. 2017 version of LI-RADS for CT and MR imaging: An update. Radiographics 2017, 37, 1994–2017. [Google Scholar] [CrossRef] [PubMed]
- Toyoda, H.; Tada, T.; Tsuji, K.; Hiraoka, A.; Tachi, Y.; Itobayashi, E.; Takaguchi, K.; Senoh, T.; Takizawa, D.; Ishikawa, T.; et al. Characteristics and prognosis of hepatocellular carcinoma detected in patients with chronic hepatitis C after the eradication of hepatitis C virus: A multicenter study from Japan. Hepatol. Res. 2016, 46, 734–742. [Google Scholar] [CrossRef] [PubMed]
- Toyoda, H.; Kumada, T.; Tada, T.; Mizuno, K. Imaging basis of AFP and WFA(+)M2BP as indicators of the risk of HCC after SVR. J. Hepatol. 2018, 68, 606–607. [Google Scholar] [CrossRef] [PubMed]
- Toyoda, H.; Kumada, T.; Tada, T.; Mizuno, K.; Sone, Y.; Kaneoka, Y.; Maeda, A.; Akita, T.; Tanaka, J. Impact of previously cured hepatocellular carcinoma (HCC) on new development of HCC after eradication of hepatitis C infection with non-interferon-based treatments. Aliment. Pharmacol. Ther. 2018, 48, 664–670. [Google Scholar] [CrossRef] [PubMed]
- Ioannou, G.; Beste, L.A.; Green, P.K.; Singal, A.G.; Tapper, E.B.; Waljee, A.K.; Sterling, R.K.; Feld, J.J.; Kaplan, D.E.; Taddei, T.H.; et al. Increased risk for hepatocellular carcinoma persists up to 10 years after HCV eradication in patients with baseline cirrhosis or high FIB-4 scores. Gastroenterology 2019, 157, 1264–1278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roberts, L.R.; Sirlin, C.B.; Zaiem, F.; Almasri, J.; Prokop, L.J.; Heimbach, J.K.; Murad, M.H.; Mohammed, K. Imaging for the diagnosis of hepatocellular carcinoma: A systematic review and meta-analysis. Hepatology 2018, 67, 401–421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kokudo, N.; Hasegawa, K.; Akahane, M.; Igaki, H.; Izumi, N.; Ichida, T.; Uemoto, S.; Kaneko, S.; Kawasaki, S.; Ku, Y.; et al. Evidence-based clinical practice guidelines for hepatocellular carcinoma: The Japan society of hepatology 2013 update (3rd JSH-HCC guidelines). Hepatol. Res. 2015, 45, 12464. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| At Entry (SVR24) | 1 Year after SVR24 | |
|---|---|---|
| n = 734 | n = 501 | |
| Age (years) | 65.9 ± 12 | 67.1 ± 12 |
| Sex (male/female) | 291/443 | 194/307 |
| Albumin (g/dL) | 4.32 ± 0.4 | 4.30 ± 0.4 |
| Bilirubin (mg/dL) | 0.67 ± 0.3 | 0.73 ± 0.3 |
| AST (IU/L) | 24.7 ± 8.1 | 23.7 ± 8.0 |
| ALT (IU/L) | 17.6 ± 9.0 | 17.5 ± 9.0 |
| Platelet counts (×104/μL) | 17.0 ± 5.6 | 17.7 ± 5.6 |
| WFA±M2BP (COI) | 1.52 ± 1.4 | 1.28 ± 1.1 |
| AFP (ng/mL) | 3.99 ± 3.4 | 3.51 ± 2.2 |
| Presence of LR3/4 nodules | 21 (2.9%) | 9 (1.8%) |
| Histological fibrosis stage (1/2/3/4) | 64/75/88/30 |
| At SVR24 | ||||||
| Univariate | Multivariate | |||||
| HR | 95%CI | p value | HR | 95%CI | p value | |
| Age (every 10 years) | 1.90 | 1.20–2.99 | 0.006 | |||
| Sex (male) | 1.31 | 0.59–2.93 | 0.5 | |||
| Albumin (g/dL) | 0.22 | 0.09–0.56 | 0.001 | |||
| Bilirubin (mg/dL) | 2.34 | 0.69–7.98 | 0.2 | |||
| AST (every 30 IU/L) | 4.40 | 1.69–11.4 | 0.002 | |||
| ALT (every 30 IU/L) | 3.42 | 1.40–8.35 | 0.007 | |||
| Platelet counts (×104/μL) | 0.87 | 0.80–0.94 | <0.001 | |||
| WFA±M2BP ≥ 1.85 (COI) | 9.43 | 3.91–22.7 | <0.001 | 5.29 | 2.07–13.0 | <0.001 |
| AFP ≥ 6.0 (ng/mL) | 8.17 | 3.63–18.4 | <0.001 | 4.27 | 1.84–9.94 | <0.001 |
| Presence of LR3/4 nodules | 15.4 | 6.06–39.2 | <0.001 | 8.49 | 3.29–21.9 | <0.001 |
| 1 Year after SVR24 | ||||||
| Univariate | Multivariate | |||||
| HR | 95%CI | p value | HR | 95%CI | p value | |
| Age (every 10 years) | 2.40 | 0.91–6.31 | 0.08 | |||
| Sex (male) | 0.64 | 0.12–3.30 | 0.6 | |||
| Albumin (g/dL) | 0.17 | 0.04–0.65 | 0.01 | |||
| Bilirubin (mg/dL) | 2.12 | 0.27–16.6 | 0.5 | |||
| AST (every 30 IU/L) | 2.52 | 0.46–13.7 | 0.3 | |||
| ALT (every 30 IU/L) | 1.18 | 0.11–12.1 | 0.9 | |||
| Platelet counts (×104/μL) | 0.81 | 0.69–0.94 | 0.005 | |||
| WFA±M2BP ≥ 1.85 (COI) | 35.3 | 4.25–293 | <0.001 | 23.5 | 2.68–205 | 0.004 |
| AFP ≥ 6.0 (ng/mL) | 1.23 | 0.15–10.2 | 0.9 | |||
| Presence of LR3/4 nodules | 60.1 | 13.2–273 | <0.001 | 24.1 | 5.02–116 | <0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Osawa, L.; Tamaki, N.; Kurosaki, M.; Kirino, S.; Watakabe, K.; Wang, W.; Okada, M.; Shimizu, T.; Higuchi, M.; Takaura, K.; et al. Wisteria floribunda Agglutinin-Positive Mac-2 Binding Protein but not α-fetoprotein as a Long-Term Hepatocellular Carcinoma Predictor. Int. J. Mol. Sci. 2020, 21, 3640. https://doi.org/10.3390/ijms21103640
Osawa L, Tamaki N, Kurosaki M, Kirino S, Watakabe K, Wang W, Okada M, Shimizu T, Higuchi M, Takaura K, et al. Wisteria floribunda Agglutinin-Positive Mac-2 Binding Protein but not α-fetoprotein as a Long-Term Hepatocellular Carcinoma Predictor. International Journal of Molecular Sciences. 2020; 21(10):3640. https://doi.org/10.3390/ijms21103640
Chicago/Turabian StyleOsawa, Leona, Nobuharu Tamaki, Masayuki Kurosaki, Sakura Kirino, Keiya Watakabe, Wan Wang, Mao Okada, Takao Shimizu, Mayu Higuchi, Kenta Takaura, and et al. 2020. "Wisteria floribunda Agglutinin-Positive Mac-2 Binding Protein but not α-fetoprotein as a Long-Term Hepatocellular Carcinoma Predictor" International Journal of Molecular Sciences 21, no. 10: 3640. https://doi.org/10.3390/ijms21103640
APA StyleOsawa, L., Tamaki, N., Kurosaki, M., Kirino, S., Watakabe, K., Wang, W., Okada, M., Shimizu, T., Higuchi, M., Takaura, K., Takada, H., Kaneko, S., Yasui, Y., Tsuchiya, K., Nakanishi, H., Itakura, J., Takahashi, Y., Enomoto, N., & Izumi, N. (2020). Wisteria floribunda Agglutinin-Positive Mac-2 Binding Protein but not α-fetoprotein as a Long-Term Hepatocellular Carcinoma Predictor. International Journal of Molecular Sciences, 21(10), 3640. https://doi.org/10.3390/ijms21103640