A Signature of Four Circulating microRNAs as Potential Biomarkers for Diagnosing Early-Stage Breast Cancer


 , , and
, , and
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
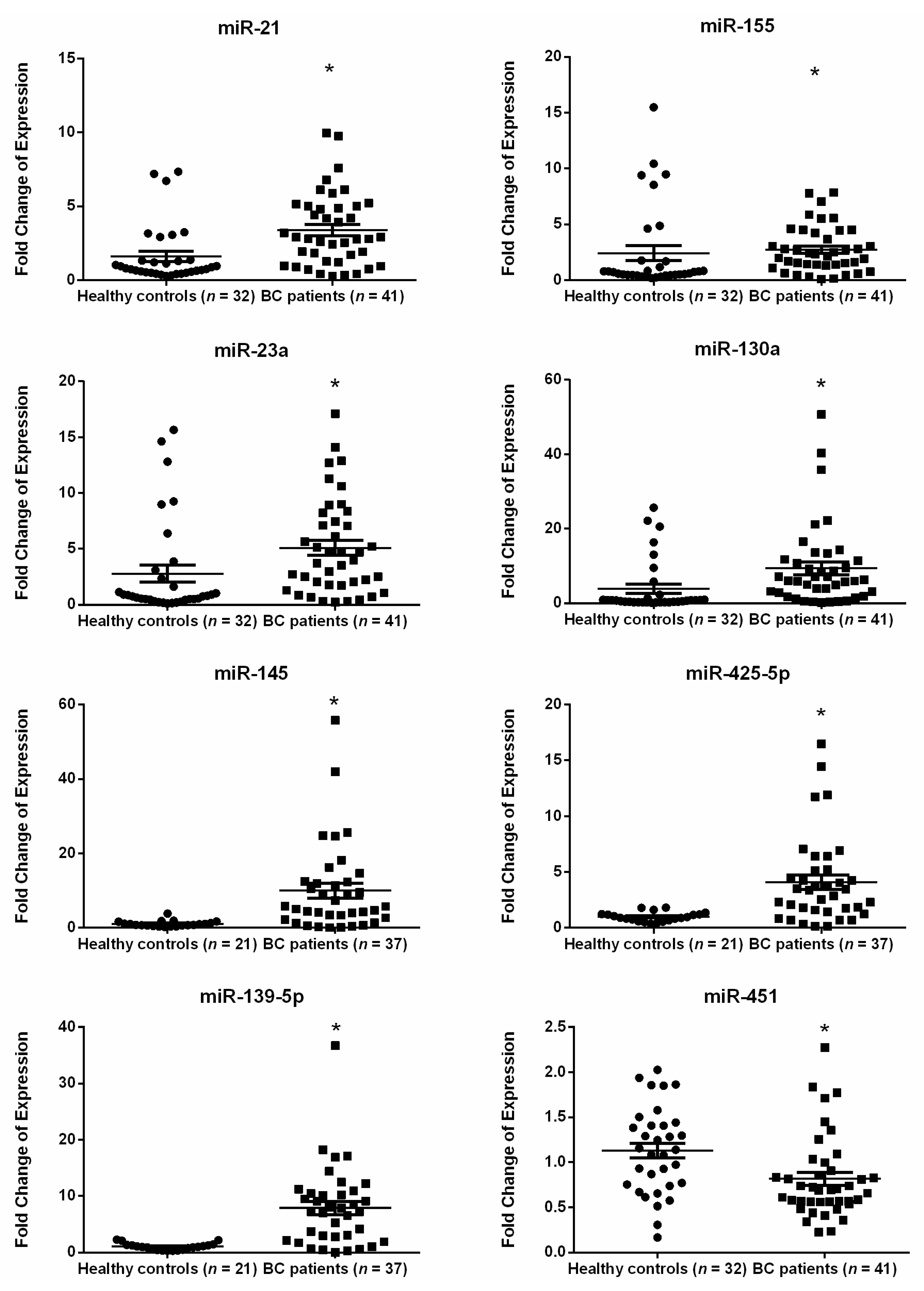
2.2. MiRNA Expression in the Plasma of Breast Cancer Patients as Compared with Healthy Subjects
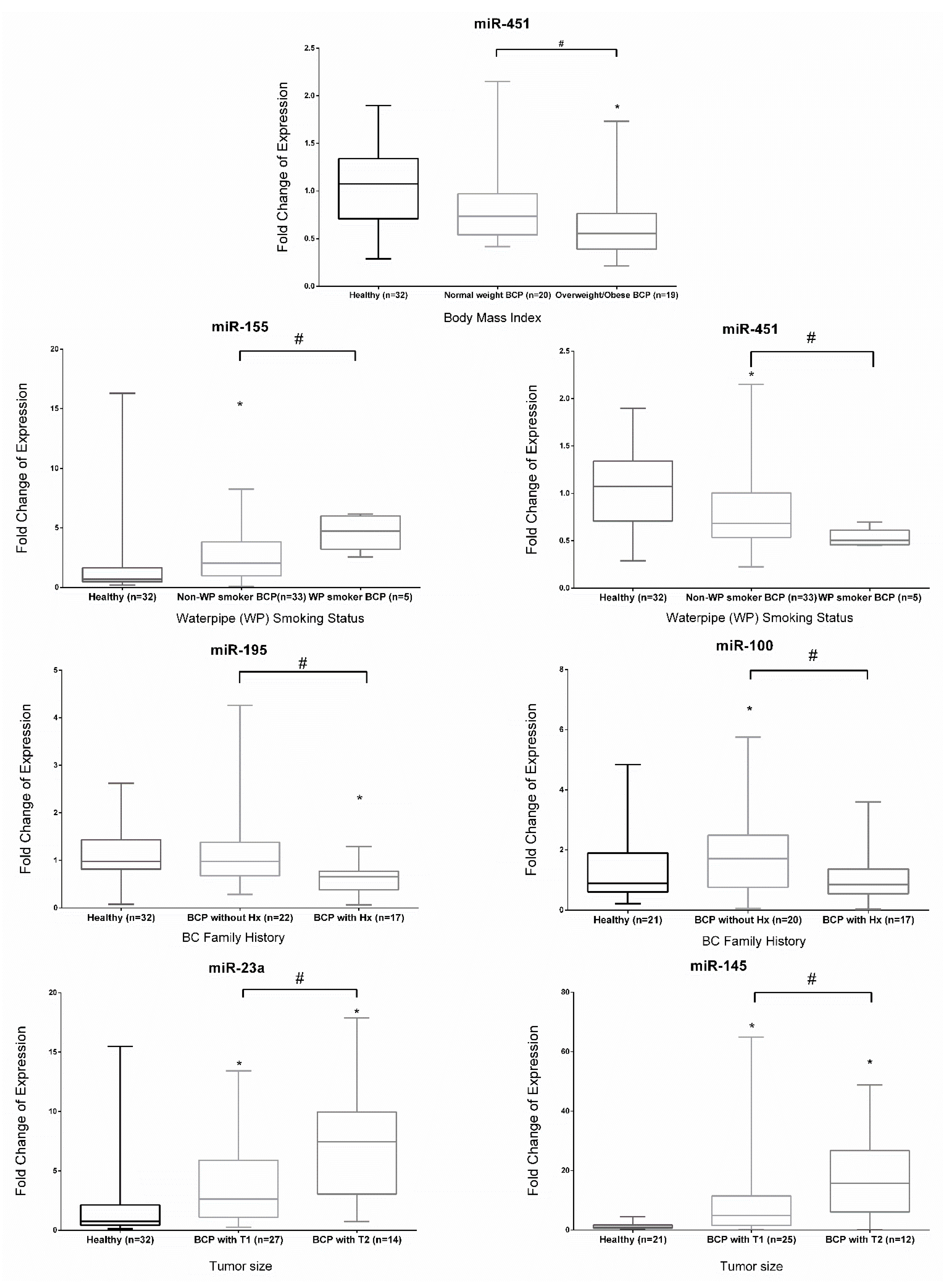
2.3. Expression of miRNAs in Early Stage BC Patients with Different Clinicopathological Features
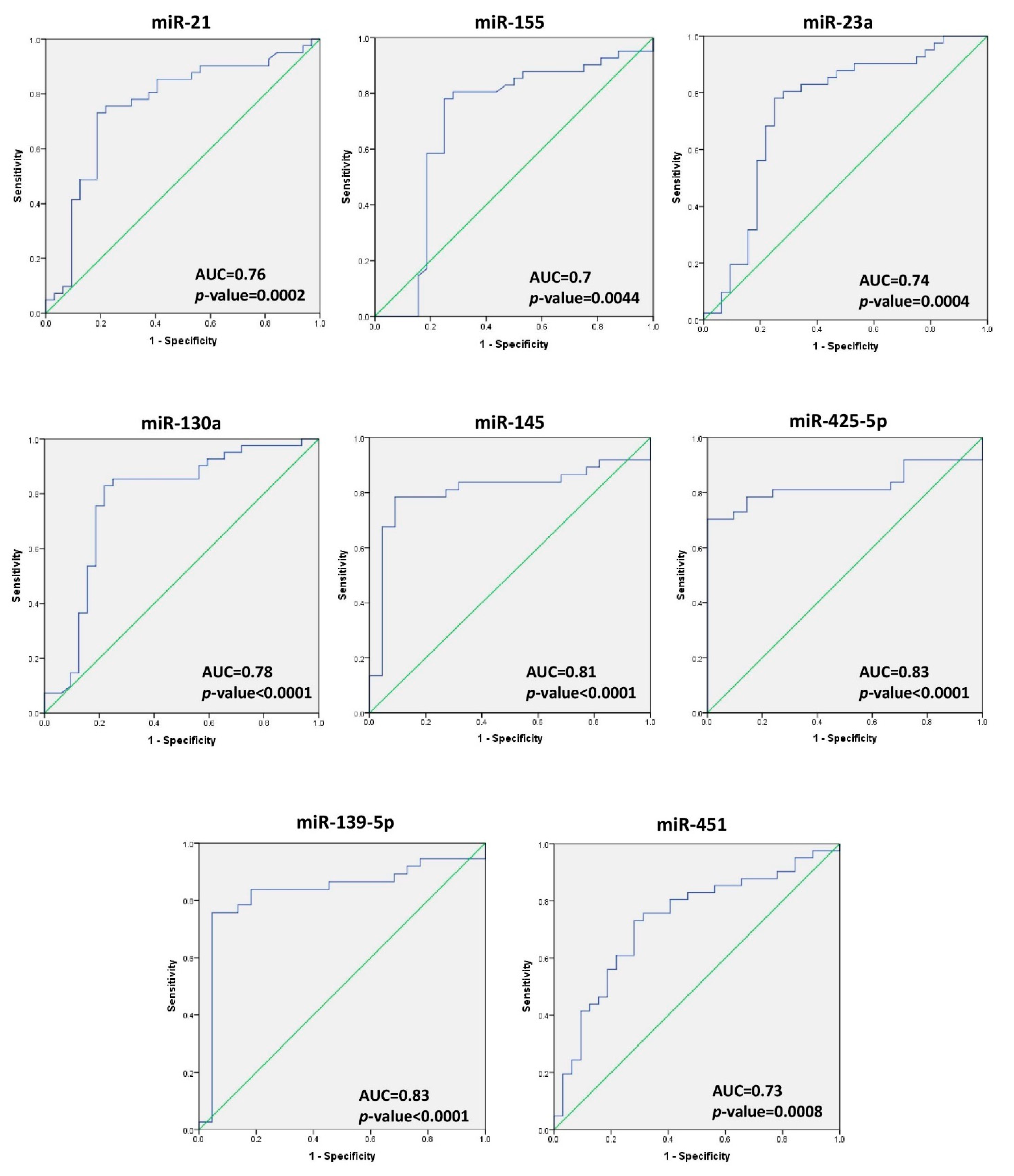
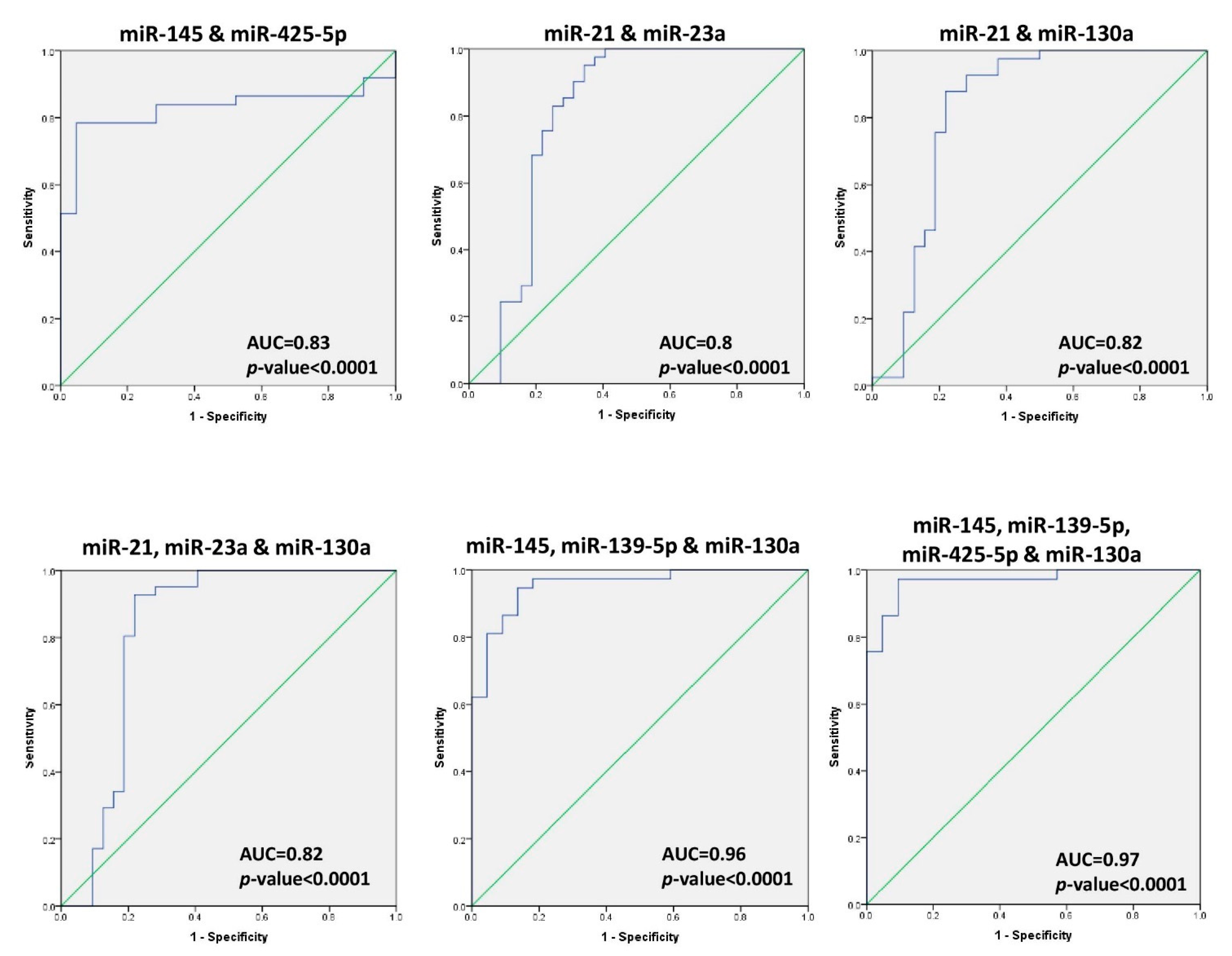
2.4. Diagnostic Accuracy of miRNA in BC
3. Discussion
4. Materials and Methods
4.1. Specimen Collection
4.2. Total RNA Extraction
4.3. cDNA Synthesis
4.4. Quantitative Real-Time Polymerase Chain Reaction (RT-qPCR) Analysis
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Mathers, C.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int. J. Cancer 2019, 144, 1941–1953. [Google Scholar] [CrossRef] [Green Version]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018. [Google Scholar] [CrossRef] [Green Version]
- Becker, S. A historic and scientific review of breast cancer: The next global healthcare challenge. Int. J. Gynaecol. Obstet. 2015, 131 (Suppl. 1), S36–S39. [Google Scholar] [CrossRef] [Green Version]
- Wadhwa, A.; Sullivan, J.R.; Gonyo, M.B. Missed Breast Cancer: What Can We Learn? Curr. Probl. Diagn. Radiol. 2016, 45, 402–419. [Google Scholar] [CrossRef]
- Bartel, D.P. MicroRNAs: Genomics, biogenesis, mechanism, and function. Cell 2004, 116, 281–297. [Google Scholar] [CrossRef] [Green Version]
- Herranz, H.; Cohen, S.M. MicroRNAs and gene regulatory networks: Managing the impact of noise in biological systems. Genes Dev. 2010, 24, 1339–1344. [Google Scholar] [CrossRef] [Green Version]
- Sohel, M.H. Extracellular/Circulating MicroRNAs: Release Mechanisms, Functions and Challenges. Achiev. Life Sci. 2016, 10, 175–186. [Google Scholar] [CrossRef] [Green Version]
- Nassar, F.J.; Nasr, R.; Talhouk, R. MicroRNAs as biomarkers for early breast cancer diagnosis, prognosis and therapy prediction. Pharmacol. Ther. 2017. [Google Scholar] [CrossRef]
- Nassar, F.J.; El Sabban, M.; Zgheib, N.K.; Tfayli, A.; Boulos, F.; Jabbour, M.; El Saghir, N.S.; Talhouk, R.; Bazarbachi, A.; Calin, G.A.; et al. miRNA as potential biomarkers of breast cancer in the Lebanese population and in young women: A pilot study. PLoS ONE 2014, 9, e107566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nassar, F.J.; Talhouk, R.; Zgheib, N.K.; Tfayli, A.; El Sabban, M.; El Saghir, N.S.; Boulos, F.; Jabbour, M.N.; Chalala, C.; Boustany, R.M.; et al. microRNA Expression in Ethnic Specific Early Stage Breast Cancer: An Integration and Comparative Analysis. Sci. Rep. 2017, 7, 16829. [Google Scholar] [CrossRef] [Green Version]
- Cui, C.; Cui, Q. The relationship of human tissue microRNAs with those from body fluids. Sci. Rep. 2020, 10, 5644. [Google Scholar] [CrossRef] [Green Version]
- Stückrath, I.; Rack, B.; Janni, W.; Jäger, B.; Pantel, K.; Schwarzenbach, H. Aberrant plasma levels of circulating miR-16, miR-107, miR-130a and miR-146a are associated with lymph node metastasis and receptor status of breast cancer patients. Oncotarget 2015, 6, 13387–13401. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Zou, W.; Wang, Y.; Liao, Z.; Li, L.; Zhai, Y.; Zhang, L.; Gu, S.; Zhao, X. Plasma-based microRNA signatures in early diagnosis of breast cancer. Mol. Genet. Genom. Med. 2020, 8, e1092. [Google Scholar] [CrossRef] [Green Version]
- Bertoli, G.; Cava, C.; Castiglioni, I. MicroRNAs: New Biomarkers for Diagnosis, Prognosis, Therapy Prediction and Therapeutic Tools for Breast Cancer. Theranostics 2015, 5, 1122–1143. [Google Scholar] [CrossRef] [PubMed]
- El Asmar, M.; Bechnak, A.; Fares, J.; Al Oweini, D.; Alrazim, A.; El Achkar, A.; Tamim, H. Knowledge, Attitudes and Practices Regarding Breast Cancer amongst Lebanese Females in Beirut. Asian Pac. J. Cancer Prev. 2018, 19, 625. [Google Scholar]
- Karimi, A.; Delpisheh, A.; Sayehmiri, K.; Saboori, H.; Rahimi, E. Predictive factors of survival time of breast cancer in kurdistan province of Iran between 2006-2014: A cox regression approach. Asian Pac. J. Cancer Prev. 2014, 15, 8483–8488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asiaf, A.; Ahmad, S.T.; Arjumand, W.; Zargar, M.A. MicroRNAs in breast cancer: Diagnostic and therapeutic potential. In MicroRNA and Cancer; Springer: Berlin/Heidelberg, Germany, 2018; pp. 23–43. [Google Scholar]
- Matamala, N.; Vargas, M.T.; González-Cámpora, R.; Miñambres, R.; Arias, J.I.; Menéndez, P.; Andrés-León, E.; Gómez-López, G.; Yanowsky, K.; Calvete-Candenas, J. Tumor microRNA expression profiling identifies circulating microRNAs for early breast cancer detection. Clin. Chem. 2015, 61, 1098–1106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ng, E.K.; Li, R.; Shin, V.Y.; Jin, H.C.; Leung, C.P.; Ma, E.S.; Pang, R.; Chua, D.; Chu, K.-M.; Law, W.; et al. Circulating microRNAs as specific biomarkers for breast cancer detection. PLoS ONE 2013, 8, e53141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, H.; Liu, H.; Zou, H.; Chen, R.; Dou, Y.; Sheng, S.; Dai, S.; Ai, J.; Melson, J.; Kittles, R.A.; et al. Evaluation of plasma miR-21 and miR-152 as diagnostic biomarkers for common types of human cancers. J. Cancer 2016, 7, 490. [Google Scholar] [CrossRef] [Green Version]
- Khalighfard, S.; Alizadeh, A.M.; Irani, S.; Omranipour, R. Plasma miR-21, miR-155, miR-10b, and Let-7a as the potential biomarkers for the monitoring of breast cancer patients. Sci. Rep. 2018, 8, 1–11. [Google Scholar] [CrossRef]
- Soleimanpour, E.; Babaei, E.; Hosseinpour-Feizi, M.-A.; Montazeri, V. Circulating miR-21 and miR-155 as potential noninvasive biomarkers in Iranian Azeri patients with breast carcinoma. J. Cancer Res. Ther. 2019, 15, 1092. [Google Scholar] [PubMed]
- Eissa, S.; Matboli, M.; Shehata, H.H. Breast tissue–based microRNA panel highlights microRNA-23a and selected target genes as putative biomarkers for breast cancer. Transl. Res. 2015, 165, 417–427. [Google Scholar] [CrossRef]
- Wang, F.; Zheng, Z.; Guo, J.; Ding, X. Correlation and quantitation of microRNA aberrant expression in tissues and sera from patients with breast tumor. Gynecol. Oncol. 2010, 119, 586–593. [Google Scholar] [CrossRef] [PubMed]
- Dai, X.; Fang, M.; Li, S.; Yan, Y.; Zhong, Y.; Du, B. miR-21 is involved in transforming growth factor β1-induced chemoresistance and invasion by targeting PTEN in breast cancer. Oncol. Lett. 2017, 14, 6929–6936. [Google Scholar] [CrossRef] [Green Version]
- Petrovic, N. miR-21 might be involved in breast cancer promotion and invasion rather than in initial events of breast cancer development. Mol. Diagn. Ther. 2016, 20, 97. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Chen, C.; Guo, G. MiR-155 promotes the proliferation and migration of breast cancer cells via targeting SOCS1 and MMP16. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 7323–7332. [Google Scholar]
- Ding, Y.; Zhang, C.; Zhang, J.; Zhang, N.; Li, T.; Fang, J.; Zhang, Y.; Zuo, F.; Tao, Z.; Tang, S.; et al. miR-145 inhibits proliferation and migration of breast cancer cells by directly or indirectly regulating TGF-β1 expression. Int. J. Oncol. 2017, 50, 1701–1710. [Google Scholar] [CrossRef] [Green Version]
- Mar-Aguilar, F.; Mendoza-Ramírez, J.A.; Malagón-Santiago, I.; Espino-Silva, P.K.; Santuario-Facio, S.K.; Ruiz-Flores, P.; Rodríguez-Padilla, C.; Reséndez-Pérez, D. Serum circulating microRNA profiling for identification of potential breast cancer biomarkers. Dis. Markers 2013, 34, 163–169. [Google Scholar]
- Pan, Y.; Wang, R.; Zhang, F.; Chen, Y.; Lv, Q.; Long, G.; Yang, K. MicroRNA-130a inhibits cell proliferation, invasion and migration in human breast cancer by targeting the RAB5A. Int. J. Clin. Exp. Pathol. 2015, 8, 384. [Google Scholar]
- Chen, X.; Zhao, M.; Huang, J.; Li, Y.; Wang, S.; Harrington, C.A.; Qian, D.Z.; Sun, X.X.; Dai, M.S. MicroRNA-130a suppresses breast cancer cell migration and invasion by targeting FOSL1 and upregulating ZO-1. J. Cell. Biochem. 2018, 119, 4945–4956. [Google Scholar] [CrossRef]
- Zhao, H.; Kang, X.; Xia, X.; Wo, L.; Gu, X.; Hu, Y.; Xie, X.; Chang, H.; Lou, L.; Shen, X. miR-145 suppresses breast cancer cell migration by targeting FSCN-1 and inhibiting epithelial-mesenchymal transition. Am. J. Transl. Res. 2016, 8, 3106. [Google Scholar]
- Luo, J.; Zhao, Q.; Zhang, W.; Zhang, Z.; Gao, J.; Zhang, C.; Li, Y.; Tian, Y. A novel panel of microRNAs provides a sensitive and specific tool for the diagnosis of breast cancer. Mol. Med. Rep. 2014, 10, 785–791. [Google Scholar] [CrossRef] [Green Version]
- Pan, X.; Wang, R.; Wang, Z.-X. The potential role of miR-451 in cancer diagnosis, prognosis, and therapy. Mol. Cancer Ther. 2013, 12, 1153–1162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gu, X.; Li, J.-Y.; Guo, J.; Li, P.-S.; Zhang, W.-H. Influence of MiR-451 on drug resistances of paclitaxel-resistant breast cancer cell line. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2015, 21, 3291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, W.; Zhang, L.; Wang, Y.; Ding, Y.; Chen, T.; Wang, Y.; Wang, H.; Li, Y.; Duan, K.; Chen, S.; et al. Involvement of miR-451 in resistance to paclitaxel by regulating YWHAZ in breast cancer. Cell Death Dis. 2017, 8, e3071. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kodahl, A.R.; Lyng, M.B.; Binder, H.; Cold, S.; Gravgaard, K.; Knoop, A.S.; Ditzel, H.J. Novel circulating microRNA signature as a potential non-invasive multi-marker test in ER-positive early-stage breast cancer: A case control study. Mol. Oncol. 2014, 8, 874–883. [Google Scholar] [CrossRef]
- Xiao, S.; Zhu, H.; Luo, J.; Wu, Z.; Xie, M. miR-425-5p is associated with poor prognosis in patients with breast cancer and promotes cancer cell progression by targeting PTEN. Oncol. Rep. 2019, 42, 2550–2560. [Google Scholar] [CrossRef]
- Krishnan, K.; Steptoe, A.L.; Martin, H.C.; Pattabiraman, D.R.; Nones, K.; Waddell, N.; Mariasegaram, M.; Simpson, P.T.; Lakhani, S.R.; Vlassov, A.; et al. miR-139-5p is a regulator of metastatic pathways in breast cancer. RNA 2013, 19, 1767–1780. [Google Scholar] [CrossRef] [Green Version]
- Zhao, H.; Shen, J.; Medico, L.; Wang, D.; Ambrosone, C.B.; Liu, S. A pilot study of circulating miRNAs as potential biomarkers of early stage breast cancer. PLoS ONE 2010, 5, e13735. [Google Scholar] [CrossRef] [PubMed]
- Nadeem, F.; Hanif, M.; Ahmed, A.; Jamal, Q.; Khan, A. Clinicopathological features associated to MiRNA-195 expression in patients with breast cancer: Evidence of a potential biomarker. Pak. J. Med. Sci. 2017, 33, 1242. [Google Scholar] [CrossRef]
- McAnena, P.; Tanriverdi, K.; Curran, C.; Gilligan, K.; Freedman, J.E.; Brown, J.A.; Kerin, M.J. Circulating microRNAs miR-331 and miR-195 differentiate local luminal a from metastatic breast cancer. BMC Cancer 2019, 19, 436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qattan, A.; Intabli, H.; Alkhayal, W.; Eltabache, C.; Tweigieri, T.; Amer, S.B. Robust expression of tumor suppressor miRNA’s let-7 and miR-195 detected in plasma of Saudi female breast cancer patients. BMC Cancer 2017, 17, 799. [Google Scholar] [CrossRef] [PubMed]
- Shams, R.; Dianatpour, A.; Omrani, M.D.; Ghafouri-Fard, S. Expression analysis of miR-100 and selected genes from mTOR pathway in breast cancer patients. Meta Gene 2019, 21, 100577. [Google Scholar] [CrossRef]
- Yan, L.-X.; Huang, X.-F.; Shao, Q.; Huang, M.-Y.; Deng, L.; Wu, Q.-L.; Zeng, Y.-X.; Shao, J.-Y. MicroRNA miR-21 overexpression in human breast cancer is associated with advanced clinical stage, lymph node metastasis and patient poor prognosis. RNA 2008, 14, 2348–2360. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinicopathological Characteristics | Number | Percentage (%) | |
|---|---|---|---|
| Total number of breast cancer (BC) cases | 41 | 100 | |
| Age (years) | Mean ± SD | 53 ± 11.88 | |
| Range | 30–84 | ||
| Menopausal status | Premenopausal | 17 | 41.5 |
| Postmenopausal | 22 | 53.7 | |
| Unknown | 2 | 4.9 | |
| Age at menarche (years) | ≤12 | 17 | 41.5 |
| 13 | 12 | 29.3 | |
| ≥14 | 10 | 24.4 | |
| Unknown | 2 | 4.9 | |
| BMI 1 | Normal weight | 20 | 48.8 |
| Overweight/obese | 18 | 44.0 | |
| Unknown | 3 | 7.3 | |
| Family history of BC | Yes | 17 | 41.5 |
| No | 22 | 53.6 | |
| Unknown | 2 | 4.9 | |
| Cigarette smoking | Yes | 12 | 29.3 |
| No | 26 | 63.4 | |
| Unknown | 3 | 7.3 | |
| Waterpipe smoking | Yes | 5 | 12.2 |
| No | 33 | 80.5 | |
| Unknown | 3 | 7.3 | |
| Alcohol intake | Yes | 10 | 24.4 |
| No | 28 | 68.3 | |
| Unknown | 3 | 7.3 | |
| History of OCP Use 2 | Yes | 23 | 56.1 |
| No | 16 | 39.0 | |
| Unknown | 2 | 4.9 | |
| History of HRT use 3 | Yes | 8 | 19.5 |
| No | 31 | 75.6 | |
| Unknown | 2 | 4.9 | |
| HER-2 status | Positive | 26 | 63.4 |
| Equivocal | 12 | 29.3 | |
| Negative | 3 | 7.3 | |
| Histological grade | 1 | 17 | 41.5 |
| 2 | 16 | 39.0 | |
| 3 | 7 | 17.1 | |
| Unknown | 1 | 2.4 | |
| Tumor size | Tumor size (T1) ≤2 cm | 27 | 65.9 |
| Tumor size (T2) >2 cm but ≤5 cm | 13 | 31.7 | |
| Tumor size (T3) >5 cm | 1 | 2.4 | |
| Lymph node involvement | No | 25 | 61.0 |
| Yes | 15 | 36.6 | |
| Unknown | 1 | 2.4 | |
| Distant metastasis | Yes | 0 | 0 |
| No | 41 | 100 | |
| miRNA | AUC a. | p-Value | SE b. | 95% CI c. | Youden’s Index | Cut-Off | Sensitivity (%) | Specificity (%) | PPV (%) d. | NPV (%) e. | DA (%) f. |
|---|---|---|---|---|---|---|---|---|---|---|---|
| miR-21 | 0.76 | 0.0002 | 0.06 | 0.640–0.876 | 0.54 | 4.46 | 73 | 81 | 76 | 78 | 77 |
| miR-155 | 0.70 | 0.0044 | 0.07 | 0.559–0.832 | 0.53 | 10.54 | 78 | 75 | 78 | 75 | 77 |
| miR-23a | 0.74 | 0.0004 | 0.063 | 0.619–0.866 | 0.53 | 11.69 | 78 | 75 | 88 | 44 | 68 |
| miR-130a | 0.78 | <0.0001 | 0.060 | 0.660–0.896 | 0.61 | 10.18 | 83 | 78 | 83 | 78 | 81 |
| miR-145 | 0.81 | <0.0001 | 0.062 | 0.686–0.928 | 0.69 | 9.09 | 78 | 91 | 78 | 91 | 83 |
| miR-425-5p | 0.83 | <0.0001 | 0.056 | 0.716–0.936 | 0.70 | 7.96 | 70 | 100 | 70 | 100 | 81 |
| miR-139-5p | 0.83 | <0.0001 | 0.060 | 0.710–0.946 | 0.71 | 8.54 | 76 | 96 | 76 | 95 | 83 |
| miR-451 | 0.73 | 0.0008 | 0.060 | 0.613–0.849 | 0.45 | 2.5 | 73 | 72 | 73 | 72 | 73 |
| miR-145 + miR-425-5p | 0.83 | <0.0001 | 0.057 | 0.716–0.940 | 0.74 | 0.62 | 78 | 95 | 78 | 95 | 84 |
| miR-21 + miR-23a | 0.80 | <0.0001 | 0.061 | 0.684–0.924 | 0.61 | 0.38 | 95 | 66 | 95 | 66 | 82 |
| miR-21 + miR-130a | 0.82 | <0.0001 | 0.058 | 0.710–0.937 | 0.659 | 0.42 | 88 | 78 | 88 | 78 | 84 |
| miR-21 + miR-23a + miR-130a | 0.82 | <0.0001 | 0.061 | 0.702–0.940 | 0.71 | 0.46 | 93 | 78 | 93 | 78 | 86 |
| miR-145 + miR-139-5p + miR-130a | 0.96 | <0.0001 | 0.026 | 0.905–1.000 | 0.81 | 0.39 | 95 | 86 | 95 | 86 | 92 |
| miR-145 + miR-139-5p + miR-130a + miR-425-5p | 0.97 | <0.0001 | 0.020 | 0.929–1.000 | 0.88 | 0.36 | 97 | 91 | 97 | 90 | 95 |
| miR-21 | miR-155 | miR-23a | miR-130a | miR-145 | miR-425-5p | miR-139-5p | miR-451 | |
|---|---|---|---|---|---|---|---|---|
| miR-21 | 1.00 | 0.752 * | 0.909 * | 0.803 * | 0.682 * | 0.596 * | 0.582 * | 0.12 |
| miR-155 | 1.00 | 0.695 * | 0.737 * | 0.672 * | 0.607 * | 0.483 * | −0.16 | |
| miR-23a | 1.00 | 0.781 * | 0.676 * | 0.626 * | 0.56 * | −0.13 | ||
| miR-130a | 1.00 | 0.654 * | 0.59 * | 0.506 * | −0.03 | |||
| miR-145 | 1.00 | 0.920 * | 0.713 * | −0.20 | ||||
| miR-425-5p | 1.00 | 0.726 * | −0.22 | |||||
| miR-139-5p | 1.00 | −0.19 | ||||||
| miR-451 | 1.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Itani, M.M.; Nassar, F.J.; Tfayli, A.H.; Talhouk, R.S.; Chamandi, G.K.; Itani, A.R.S.; Makoukji, J.; Boustany, R.-M.N.; Hou, L.; Zgheib, N.K.; et al. A Signature of Four Circulating microRNAs as Potential Biomarkers for Diagnosing Early-Stage Breast Cancer. Int. J. Mol. Sci. 2021, 22, 6121. https://doi.org/10.3390/ijms22116121
Itani MM, Nassar FJ, Tfayli AH, Talhouk RS, Chamandi GK, Itani ARS, Makoukji J, Boustany R-MN, Hou L, Zgheib NK, et al. A Signature of Four Circulating microRNAs as Potential Biomarkers for Diagnosing Early-Stage Breast Cancer. International Journal of Molecular Sciences. 2021; 22(11):6121. https://doi.org/10.3390/ijms22116121
Chicago/Turabian StyleItani, Maha M., Farah J. Nassar, Arafat H. Tfayli, Rabih S. Talhouk, Ghada K. Chamandi, Abdul Rahman S. Itani, Joelle Makoukji, Rose-Mary N. Boustany, Lifang Hou, Nathalie K. Zgheib, and et al. 2021. "A Signature of Four Circulating microRNAs as Potential Biomarkers for Diagnosing Early-Stage Breast Cancer" International Journal of Molecular Sciences 22, no. 11: 6121. https://doi.org/10.3390/ijms22116121
APA StyleItani, M. M., Nassar, F. J., Tfayli, A. H., Talhouk, R. S., Chamandi, G. K., Itani, A. R. S., Makoukji, J., Boustany, R. -M. N., Hou, L., Zgheib, N. K., & Nasr, R. R. (2021). A Signature of Four Circulating microRNAs as Potential Biomarkers for Diagnosing Early-Stage Breast Cancer. International Journal of Molecular Sciences, 22(11), 6121. https://doi.org/10.3390/ijms22116121