
Selected Essential and Toxic Chemical Elements in Hypothyroidism—A Literature Review (2001–2021)




Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Eligibility Criteria
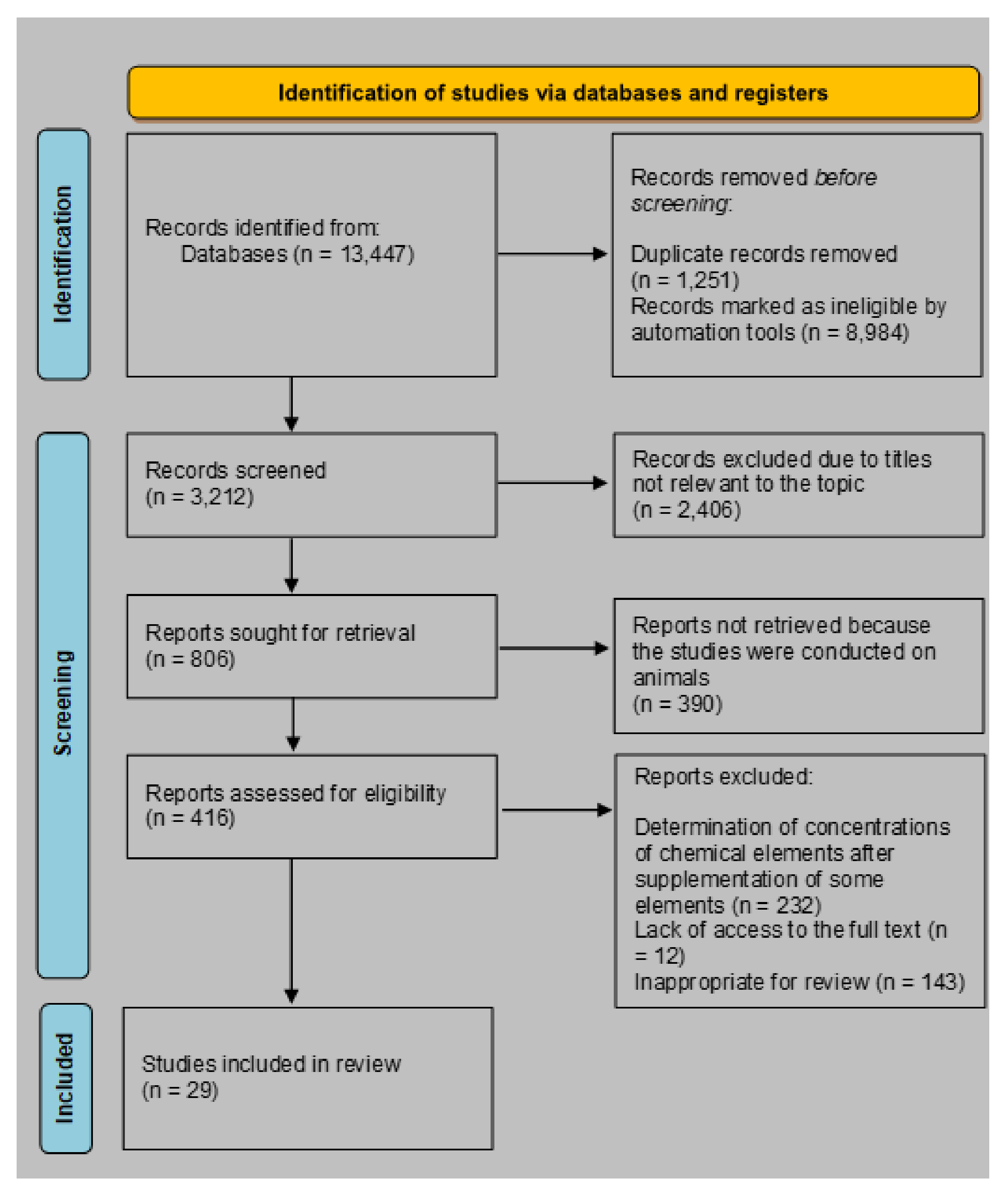
2.3. Study Selection
3. Results and Discussion
3.1. Selenium
3.2. Zinc
3.3. Copper
3.4. Iron
3.5. Manganese
3.6. Chromium
3.7. Fluoride
3.8. Lead (Pb)
3.9. Cadmium
3.10. Summary of the Findings
3.11. Strengths and Limitations
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Zoeller, R.T.; Tan, S.W.; Tyl, R.W. General Background on the Hypothalamic-Pituitary-Thyroid (HPT) Axis. Crit. Rev. Toxicol. 2007, 37, 11–53. [Google Scholar] [CrossRef] [PubMed]
- Kostoglou-Athanassiou, I.; Ntalles, K. Hypothyroidism-new aspects of an old disease. Hippokratia 2010, 14, 82–87. [Google Scholar] [PubMed]
- Mullur, R.; Liu, Y.Y.; Brent, G.A. Thyroid Hormone Regulation of Metabolism. Physiol. Rev. 2014, 94, 355–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wassner, A.J. Pediatric Hypothyroidism: Diagnosis and Treatment. Pediatr. Drugs 2017, 19, 291–301. [Google Scholar] [CrossRef] [PubMed]
- Rasic-Milutinovic, Z.; Jovanovic, D.; Bogdanovic, G.; Trifunovic, J.; Mutic, J. Potential Influence of Selenium, Copper, Zinc and Cadmium on L-Thyroxine Substitution in Patients with Hashimoto Thyroiditis and Hypothyroidism. Exp. Clin. Endocrinol. Diabetes 2017, 125, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Chaker, L.; Bianco, A.C.; Jonklaas, J.; Peeters, R.P. Hypothyroidism. Lancet 2017, 390, 1550–1562. [Google Scholar] [CrossRef]
- Antonelli, A.; Ferrari, S.M.; Corrado, A.; Di Domenicantonio, A.; Fallahi, P. Autoimmune Thyroid Disorders. Autoimmun. Rev. 2015, 14, 174–180. [Google Scholar] [CrossRef] [PubMed]
- Mendes, D.; Alves, C.; Silverio, N.; Batel Marques, F. Prevalence of Undiagnosed Hypothyroidism in Europe: A Systematic Review and Meta-Analysis. Eur. Thyroid J. 2019, 8, 130–143. [Google Scholar] [CrossRef]
- Khandelwal, D.; Tandon, N. Overt and Subclinical Hypothyroidism: Who to Treat and How. Drugs 2012, 72, 17–33. [Google Scholar] [CrossRef]
- Almandoz, J.P.; Gharib, H. Hypothyroidism: Etiology, Diagnosis, and Management. Med. Clin. N. Am. 2012, 96, 203–221. [Google Scholar] [CrossRef]
- Duntas, L. The Role of Iodine and Selenium in Autoimmune Thyroiditis. Horm. Metab. Res. 2015, 47, 721–726. [Google Scholar] [CrossRef] [Green Version]
- Ragusa, F.; Fallahi, P.; Elia, G.; Gonnella, D.; Paparo, S.R.; Giusti, C.; Churilov, L.P.; Ferrari, S.M.; Antonelli, A. Hashimotos’ Thyroiditis: Epidemiology, Pathogenesis, Clinic and Therapy. Best Pract. Res. Clin. Endocrinol. Metab. 2019, 33, 101367. [Google Scholar] [CrossRef] [PubMed]
- McAninch, E.A.; Bianco, A.C. The History and Future of Treatment of Hypothyroidism. Ann. Intern. Med. 2016, 164, 50–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maenhaut, C.; Christophe, D.; Vassart, G.; Dumont, J.; Roger, P.P.; Opitz, R. Ontogeny, Anatomy, Metabolism and Physiology of the Thyroid. In Endotext [Internet]; Feingold, K.R., Anawalt, B., Boyce, A., et al., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 2000; Available online: https://www.ncbi.nlm.nih.gov/books/NBK285554/ (accessed on 16 September 2021).
- Ventura, M.; Melo, M.; Carrilho, F. Selenium and Thyroid Disease: From Pathophysiology to Treatment. Int. J. Endocrinol. 2017, 2017, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baltaci, A.K.; Mogulkoc, R.; Baltaci, S.B. Review: The role of zinc in the endocrine system. Pak. J. Pharm. Sci. 2019, 32, 231–239. [Google Scholar]
- Kandhro, G.A.; Kazi, T.G.; Afridi, H.I.; Kazi, N.; Arain, M.B.; Sarfraz, R.A.; Sirajuddin; Syed, N.; Baig, J.A.; Shah, A.Q. Evaluation of Iron in Serum and Urine and Their Relation with Thyroid Function in Female Goitrous Patients. Biol. Trace Elem. Res. 2008, 125, 203–212. [Google Scholar] [CrossRef] [PubMed]
- Soldin, O.P.; Aschner, M. Effects of Manganese on Thyroid Hormone Homeostasis: Potential Links. NeuroToxicology 2007, 28, 951–956. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- KheradPisheh, Z.; Mirzaei, M.; Mahvi, A.H.; Mokhtari, M.; Azizi, R.; Fallahzadeh, H.; Ehrampoush, M.H. Impact of Drinking Water Fluoride on Human Thyroid Hormones: A Case-Control Study. Sci. Rep. 2018, 8, 2674. [Google Scholar] [CrossRef] [Green Version]
- ARUP Laboratories. Available online: https://www.aruplab.com/ (accessed on 10 June 2021).
- Mayo Clinic Laboratories. Available online: https://www.mayocliniclabs.com/ (accessed on 10 June 2021).
- Błażewicz, A.; Dolliver, W.; Sivsammye, S.; Deol, A.; Randhawa, R.; Orlicz-Szczesna, G.; Błażewicz, R. Determination of Cadmium, Cobalt, Copper, Iron, Manganese, and Zinc in Thyroid Glands of Patients with Diagnosed Nodular Goitre Using Ion Chromatography. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2009, 878, 34–38. [Google Scholar] [CrossRef]
- Ambroziak, U.; Hybsier, S.; Shahnazaryan, U.; Krasnodębska-Kiljańska, M.; Rijntjes, E.; Bartoszewicz, Z.; Bednarczuk, T.; Schomburg, L. Severe Selenium Deficits in Pregnant Women Irrespective of Autoimmune Thyroid Disease in an Area with Marginal Selenium Intake. J. Trace Elem. Med. Biol. 2017, 44, 186–191. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. J. Clin. Endocrinol. 2021, 134, 178–189. [Google Scholar] [CrossRef]
- Benamer, S.; Aberkane, L.; Benamar, M.A. Study of Blood Selenium Level in Thyroid Pathologies by Instrumental Neutron Activation Analysis. Instrum. Sci. Technol. 2006, 34, 417–423. [Google Scholar] [CrossRef]
- Blasig, S.; Kühnen, P.; Schuette, A.; Blankenstein, O.; Mittag, J.; Schomburg, L. Positive Correlation of Thyroid Hormones and Serum Copper in Children with Congenital Hypothyroidism. J. Trace Elem. Med. Biol. 2016, 37, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Cayir, A.; Doneray, H.; Kurt, N.; Orbak, Z.; Kaya, A.; Turan, M.I.; Yildirim, A. Thyroid Functions and Trace Elements in Pediatric Patients with Exogenous Obesity. Biol. Trace Elem. Res. 2014, 157, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Erdal, M.; Sahin, M.; Hasimi, A.; Uckaya, G.; Kutlu, M.; Saglam, K. Trace Element Levels in Hashimoto Thyroiditis Patients with Subclinical Hypothyroidism. Biol. Trace Elem. Res. 2008, 123, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Federige, M.A.F.; Romaldini, J.H.; Miklos, A.B.P.P.; Koike, M.K.; Takei, K.; Portes, E.D.S. Serum Selenium and Selenoprotein-p Levels in Autoimmune Thyroid Diseases Patients in a Select Center: A Transversal Study. Arch. Endocrinol. Metab. 2017, 61, 600–607. [Google Scholar] [CrossRef] [Green Version]
- Guo, X.; Zhou, L.; Xu, J.; Liu, Z.; Liu, J.; Yan, C. Prenatal Maternal Low Selenium, High Thyrotropin, and Low Birth Weights. Biol. Trace Elem. Res. 2021, 199, 18–25. [Google Scholar] [CrossRef]
- Hanif, S.; Ilyas, A.; Shah, M.H. Statistical Evaluation of Trace Metals, TSH and T4 in Blood Serum of Thyroid Disease Patients in Comparison with Controls. Biol. Trace Elem. Res. 2018, 183, 58–70. [Google Scholar] [CrossRef]
- Khatiwada, S.; Gelal, B.; Baral, N.; Lamsal, M. Association between Iron Status and Thyroid Function in Nepalese Children. Thyroid Res. 2016, 9, 2. [Google Scholar] [CrossRef] [Green Version]
- Khatun, S.; Santhini, G.; Malligai, E.; Kumar, H.V. Evaluation of Serum Zinc, Copper Level and Their Correlation with Cu/Zn Ratio and FT3/FT4 Ratio in Hypothyroidism. J. Clin. Diagn. Res. 2019, 13, BC08–BC010. [Google Scholar] [CrossRef]
- Mehl, S.; Sun, Q.; Görlich, C.L.; Hackler, J.; Kopp, J.F.; Renko, K.; Mittag, J.; Schwerdtle, T.; Schomburg, L. Cross-Sectional Analysis of Trace Element Status in Thyroid Disease. J. Trace Elem. Med. Biol. 2020, 58, 126430. [Google Scholar] [CrossRef] [PubMed]
- Memon, N.S.; Kazi, T.G.; Afridi, H.I.; Baig, J.A.; Sahito, O.M.; Baloch, S.; Waris, M. Correlation of Manganese with Thyroid Function in Females Having Hypo- and Hyperthyroid Disorders. Biol. Trace Elem. Res. 2015, 167, 165–171. [Google Scholar] [CrossRef]
- Nisa, F.U.; Mumtaz, A.; Ullah, M.I.; Atif, M.; Sami, W. Determination of Serum Zinc and Magnesium Levels in Patients with Hypothyroidism. Trace Elem. Electrolytes 2014, 31, 43–47. [Google Scholar] [CrossRef]
- Nourbakhsh, M.; Ahmadpour, F.; Chahardoli, B.; Malekpour-Dehkordi, Z.; Nourbakhsh, M.; Hosseini-Fard, S.R.; Doustimotlagh, A.; Golestani, A.; Razzaghy-Azar, M. Selenium and Its Relationship with Selenoprotein P and Glutathione Peroxidase in Children and Adolescents with Hashimoto’s Thyroiditis and Hypothyroidism. J. Trace Elem. Med. Biol. 2016, 34, 10–14. [Google Scholar] [CrossRef]
- Przybylik-Mazurek, E.; Zagrodzki, P.; Kuźniarz-Rymarz, S.; Hubalewska-Dydejczyk, A. Thyroid Disorders-Assessments of Trace Elements, Clinical, and Laboratory Parameters. Biol. Trace Elem. Res. 2011, 141, 65–75. [Google Scholar] [CrossRef] [PubMed]
- Rezaei, M.; Javadmoosavi, S.Y.; Mansouri, B.; Azadi, N.A.; Mehrpour, O.; Nakhaee, S. Thyroid Dysfunction: How Concentration of Toxic and Essential Elements Contribute to Risk of Hypothyroidism, Hyperthyroidism, and Thyroid Cancer. Environ. Sci. Pollut. Res. 2019, 26, 35787–35796. [Google Scholar] [CrossRef] [PubMed]
- Rostami, R.; Nourooz-Zadeh, S.; Mohammadi, A.; Khalkhali, H.R.; Ferns, G.; Nourooz-Zadeh, J. Serum Selenium Status and Its Interrelationship with Serum Biomarkers of Thyroid Function and Antioxidant Defense in Hashimoto’s Thyroiditis. Antioxidants 2020, 9, 1–14. [Google Scholar] [CrossRef]
- Shaik, N.; Shanbhog, R.; Nandlal, B.; Tippeswamy, H. Fluoride and Thyroid Function in Children Resident of Naturally Fluoridated Areas Consuming Different Levels of Fluoride in Drinking Water: An Observational Study. Contemp. Clin. Dent. 2019, 10, 24–30. [Google Scholar] [CrossRef]
- Singh, N.; Verma, K.G.; Verma, P.; Sidhu, G.K.; Sachdeva, S. A Comparative Study of Fluoride Ingestion Levels, Serum Thyroid Hormone & TSH Level Derangements, Dental Fluorosis Status among School Children from Endemic and Non-Endemic Fluorosis Areas. Springerplus 2014, 3, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Stojsavljević, A.; Trifković, J.; Rasić-Milutinović, Z.; Jovanović, D.; Bogdanović, G.; Mutić, J.; Manojlović, D. Determination of Toxic and Essential Trace Elements in Serum of Healthy and Hypothyroid Respondents by ICP-MS: A Chemometric Approach for Discrimination of Hypothyroidism. J. Trace Elem. Med. Biol. 2018, 48, 134–140. [Google Scholar] [CrossRef] [Green Version]
- Verni, E.R.; Nahan, K.; Lapiere, A.V.; Martinez, L.D.; Gil, R.A.; Landero-Figueroa, J.A. Metalloprotein and Multielemental Content Profiling in Serum Samples from Diabetic and Hypothyroid Persons Based on PCA Analysis. Microchem. J. 2018, 137, 258–265. [Google Scholar] [CrossRef]
- Zagrodzki, P.; Przybylik-Mazurek, E. Selenium and Hormone Interactions in Female Patients with Hashimoto Disease and Healthy Subjects. Endocr. Res. 2010, 35, 24–34. [Google Scholar] [CrossRef] [PubMed]
- Osterode, W.; Zettinig, G.; Pötzi, C.; Männer, G. Increased Lead Excretion in Hypothyroid Patients after Levothyroxine Medication. J. Toxicol. Environ. Health-Part A 2002, 65, 649–654. [Google Scholar] [CrossRef] [PubMed]
- Stojsavljević, A.; Rovčanin, B.; Jagodić, J.; Radojković, D.D.; Paunović, I.; Gavrović-Jankulović, M.; Manojlović, D. Significance of Arsenic and Lead in Hashimoto’s Thyroiditis Demonstrated on Thyroid Tissue, Blood, and Urine Samples. Environ. Res. 2020, 186, 109538. [Google Scholar] [CrossRef] [PubMed]
- Khorasani, E.; Mirhafez, S.R.; Niroumand, S. Assessment of the Selenium Status in Hypothyroid Children from North East of Iran. J. Biol. Today’s World 2017, 6, 21–26. [Google Scholar] [CrossRef]
- Krassas, G.E.; Pontikides, N.; Tziomalos, K.; Tzotzas, T.; Zosin, I.; Vlad, M.; Luger, A.; Gessl, A.; Marculescu, R.; Toscano, V.; et al. Selenium Status in Patients with Autoimmune and Non-Autoimmune Thyroid Diseases from Four European Countries. Expert Rev. Endocrinol. Metab. 2014, 9, 685–692. [Google Scholar] [CrossRef] [PubMed]
- Maouche, N.; Meskine, D.; Alamir, B.; Koceir, E.A. Trace Elements Profile Is Associated with Insulin Resistance Syndrome and Oxidative Damage in Thyroid Disorders: Manganese and Selenium Interest in Algerian Participants with Dysthyroidism. J. Trace Elem. Med. Biol. 2015, 32, 112–121. [Google Scholar] [CrossRef]
- Malin, A.J.; Riddell, J.; McCague, H.; Till, C. Fluoride Exposure and Thyroid Function among Adults Living in Canada: Effect Modification by Iodine Status. Environ. Int. 2018, 121, 667–674. [Google Scholar] [CrossRef]
- Liu, N.; Liu, P.; Xu, Q.; Zhu, L.; Zhao, Z.; Wang, Z.; Li, Y.; Feng, W.; Zhu, L. Elements in Erythrocytes of Population with Different Thyroid Hormone Status. Biol. Trace Elem. Res. 2001, 84, 37–43. [Google Scholar] [CrossRef]
- Chung, H.R. Iodine and thyroid function. Ann. Pediatr. Endocrinol. Metab. 2014, 19, 8–12. [Google Scholar] [CrossRef] [Green Version]
- Carayanniotis, G. Molecular Parameters Linking Thyroglobulin Iodination with Autoimmune Thyroiditis. Hormones 2011, 10, 27–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kieliszek, M.; Błażejak, S. Selenium: Significance, and outlook for supplementation. Nutrition 2013, 29, 713–718. [Google Scholar] [CrossRef] [PubMed]
- Köhrle, J. Selenium and the control of thyroid hormone metabolism. Thyroid 2005, 15, 841–853. [Google Scholar] [CrossRef]
- Drutel, A.; Archambeaud, F.; Caron, P. Selenium and the Thyroid Gland: More Good News for Clinicians. Clin. Endocrinol. 2013, 78, 155–164. [Google Scholar] [CrossRef]
- Luongo, C.; Dentice, M.; Salvatore, D. Deiodinases and Their Intricate Role in Thyroid Hormone Homeostasis. Nat. Rev. Endocrinol. 2019, 15, 479–488. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, G.; Isidori, A.M.; Moretti, C.; Di Dato, C.; Greco, E.; Ciolli, P.; Bonomi, M.; Petrone, L.; Fumarola, A.; Campagna, G.; et al. Selenium Supplementation in the Management of Thyroid Autoimmunity during Pregnancy: Results of the “SERENA Study”, a Randomized, Double-Blind, Placebo-Controlled Trial. Endocrine 2019, 66, 542–550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Severo, J.S.; Morais, J.B.S.; de Freitas, T.E.C.; Andrade, A.L.P.; Feitosa, M.M.; Fontenelle, L.C.; de Oliveira, A.R.S.; Cruz, K.J.C.; do Nascimento Marreiro, D. The Role of Zinc in Thyroid Hormones Metabolism. Int. J. Vitam. Nutr. Res. 2019, 89, 80–88. [Google Scholar] [CrossRef]
- Institute of Medicine (US) Panel on Micronutrients. Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc; National Academies Press: Washington, DC, USA, 2001. [Google Scholar] [CrossRef] [Green Version]
- Paulazo, M.A.; Klecha, A.J.; Sterle, H.A.; Valli, E.; Torti, H.; Cayrol, F.; Barreiro Arcos, M.L.; Cremaschi, G.A. Hypothyroidism-Related Zinc Deficiency Leads to Suppression of T Lymphocyte Activity. Endocrine 2019, 66, 266–277. [Google Scholar] [CrossRef]
- Katz, N.; Rader, D.J. Manganese Homeostasis: From Rare Single-Gene Disorders to Complex Phenotypes and Diseases. J. Clin. Invest. 2019, 129, 5082–5085. [Google Scholar] [CrossRef] [PubMed]
- Talebi, S.; Ghaedi, E.; Sadeghi, E.; Mohammadi, H.; Hadi, A.; Clark, C.C.T.; Askari, G. Trace Element Status and Hypothyroidism: A Systematic Review and Meta-Analysis. Biol. Trace Elem. Res. 2020, 197, 1–14. [Google Scholar] [CrossRef]
- Crinnion, W.J.; Pizzorno, J.E. Clinical Environmental Medicine: Identification and Natural Treatment of Diseases Caused by Common Pollutants; Elsevier Inc.: Amsterdam, The Netherlands, 2019; ISBN 13. [Google Scholar]
- Wilbur, S.; Abadin, H.; Fay, M.; Yu, D.; Tencza, B.; Ingerman, L.; Klotzbach, J.; James, S.; Toxicological Profile for Chromium. Toxicological Profile for Chromium; U.S. Department of Health and Human Services, Public Health Service. Agency for Toxic Substances and Disease Registry (ATSDR): Atlanta, GA, USA. Available online: https://www.ncbi.nlm.nih.gov/books/NBK158855/ (accessed on 10 June 2021).
- Sijko, M.; Janasik, B.; Wąsowicz, W.; Kozłowska, L. Can the effects of chromium compounds exposure be modulated by vitamins and microelements? Int. J. Occup. Med. Environ. Health 2021, 34, 461–490. [Google Scholar] [CrossRef]
- Kuo, H.W.; Wu, M.L. Effects of chromic acid exposure on immunological parameters among electroplating workers. Int. Arch. Occup. Environ. Health 2002, 75, 186–190. [Google Scholar] [CrossRef]
- Mahmood, T.; Qureshi, I.Z.; Javed Iqba, M. Histopathological and biochemical changes in rat thyroid following acute exposure to hexavalent chromium. Histol. Histopathol. 2010, 25, 1355–1370. [Google Scholar] [PubMed]
- Dayan, A.D.; Paine, A.J. Mechanisms of chromium toxicity, carcinogenicity and allergenicity: Review of the literature from 1985 to 2000. Hum. Exp. Toxicol. 2001, 20, 439–451. [Google Scholar] [CrossRef] [PubMed]
- Hasan, H.G.; Mahmood, T.J.; Ismael, P.A. Studies on the Relationship Between Chromium(III) ion and Thyroid Peroxidase Activity in Sera of Patients with Thyroid Dysfunction, Ibn. Al-Haitham J. Pure Appl. Sci. 2011, 24, 120–127. [Google Scholar]
- Peckham, S.; Lowery, D.; Spencer, S. Are Fluoride Levels in Drinking Water Associated with Hypothyroidism Prevalence in England? A Large Observational Study of GP Practice Data and Fluoride Levels in Drinking Water. J. Epidemiol. Comm. Health 2015, 69, 619–624. [Google Scholar] [CrossRef] [Green Version]
- Xiang, Q.; Chen, L.; Liang, Y.; Wu, M.; Chen, B. Fluoride and Thyroid Function in Children in Two Villages in China. J. Toxicol. Environ. Health Sci. 2009, 1, 054–059. [Google Scholar]
- Hosur, M.B.; Puranik, R.S.; Vanaki, S.; Puranik, S.R. Study of Thyroid Hormones Free Triiodothyronine (FT3), Free Thyroxine (FT4) and Thyroid Stimulating Hormone (TSH) in Subjects with Dental Fluorosis. Eur. J. Dent. 2012, 6, 184–190. [Google Scholar] [CrossRef] [Green Version]
- Pekcici, R.; Kavlakoğlu, B.; Yilmaz, S.; Şahin, M.; Delibaşi, T. Effects of lead on thyroid functions in lead-exposed workers. Open Med. 2010, 5, 215–218. [Google Scholar] [CrossRef]
- Hormozi, M.; Mirzaei, R.; Nakhaee, A.; Izadi, S.; Dehghan, H.J. The biochemical effects of occupational exposure to lead and cadmium on markers of oxidative stress and antioxidant enzymes activity in the blood of glazers in tile industry. Toxicol. Ind. Health 2018, 34, 459–467. [Google Scholar] [CrossRef]
- Fahim, Y.; Sharaf, N.; Hasani, I.; Ragab, E.; Abdelhakim, H. Assessment of Thyroid Function and Oxidative Stress State in Foundry Workers Exposed to Lead. J. Health Pollut. 2020, 10, 200903. [Google Scholar] [CrossRef]
- Krieg, E.F. A Meta-Analysis of Studies Investigating the Effects of Occupational Lead Exposure on Thyroid Hormones. Am. J. Ind. Med. 2016, 59, 583–590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, B.; Chandran, V.; Bandhu, H.K.; Mittal, B.R.; Bhattacharya, A.; Jindal, S.K.; Varma, S. Impact of lead exposure on pituitary-thyroid axis in humans. Biometals 2000, 13, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Sherif, M.M.; Mohammed, Y.S.; Zedan, H.A.E. Toxic Effect of Some Heavy Metals (Cadmium and Lead) on Thyroid Function. Egypt. J. Hosp. Med. 2017, 69, 2512–2515. [Google Scholar] [CrossRef]
- Buha, A.; Matovic, V.; Antonijevic, B.; Bulat, Z.; Curcic, M.; Renieri, E.A.; Tsatsakis, A.M.; Schweitzer, A.; Wallace, D. Overview of Cadmium Thyroid Disrupting Effects and Mechanisms. Int. J. Mol. Sci. 2018, 19, 1501. [Google Scholar] [CrossRef] [Green Version]
- Uetani, M.; Kobayashi, E.; Suwazono, Y.; Honda, R.; Nishijo, M.; Nakagawa, H.; Kido, T.; Nogawa, K. Tissue cadmium (Cd) concentrations of people living in a Cd polluted area, Japan. BioMetals 2006, 19, 521–525. [Google Scholar] [CrossRef]
- Monteiro, C.; Ferreira de Oliveira, J.M.P.; Pinho, F.; Bastos, V.; Oliveira, H.; Peixoto, F.; Santos, C. Biochemical and transcriptional analyses of cadmium-induced mitochondrial dysfunction and oxidative stress in human osteoblasts. J. Toxicol. Environ. Health Part A 2018, 81, 705–717. [Google Scholar] [CrossRef]
- Jain, R.B.; Choi, Y.S. Interacting effects of selected trace and toxic metals on thyroid function. Int. J. Environ. Health Res. 2016, 26, 75–91. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.B.; Boelaert, K. Iodine Deficiency and Thyroid Disorders. Lancet Diabetes Endocrinol. 2015, 3, 286–295. [Google Scholar] [CrossRef]
- Zhao, H.; Tian, Y.; Liu, Z.; Li, X.; Feng, M.; Huang, T. Correlation Between Iodine Intake and Thyroid Disorders: A Cross-Sectional Study from the South of China. Biol. Trace Elem. Res. 2014, 162, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Yeliosof, O.; Silverman, L.A. Veganism as a Cause of Iodine Deficient Hypothyroidism. J. Pediatr. Endocrinol. Metab. 2018, 31, 91–94. [Google Scholar] [CrossRef] [PubMed]
- Ikomi, C.; Cole, C.R.; Vale, E.; Golekoh, M.; Khoury, J.C.; Jones, N.H.Y. Hypothyroidism and Iodine Deficiency in Children on Chronic Parenteral Nutrition. Pediatrics 2018, 141, e20173046. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Articles written in English | Articles written in a language other than English |
| Articles containing original data or meta-analyses | Articles that do not contain original data: reviews, mini-reviews, comments, and letters |
| Peer-reviewed publications | Publications which have not been independently peer-reviewed |
| Studies on humans | Studies on animals |
| Element | Thyroid Disorder (Type of Sample) | Outcome in Patients | Outcome Controls | Significantly Increased (↑) or Decreased (↓) Level in Hypothyroidism Compared with Controls | References |
|---|---|---|---|---|---|
| Fe | Reference values: serum—50–170 μg/dLM; 30–160 μg/dLW | Arup Laboratories | [20] | ||
| Reference values: serum—50–150 μg/dLM; 35–145 μg/dLW | Mayo Clinic Laboratories | [21] | |||
| Hypothyroid (serum) | a. 39.80 ± 3.069 μg/g | a. 14.32 ± 1.970 μg/g | ↑ | [31] | |
| Autoimmune thyroiditis patients with SH (serum) | a. Pretreatment: 55.7 ± 38 μg/dL Posttreatment: 73.2 ± 54.7 μg/dL | a. 75.7 ± 24 μg/dL | ↓ | [28] | |
| Hypothyroid (serum) | b. 2.659 ± 1.145 μg/ml | b. 8.782 ± 6.792 μg/mL | - | [44] | |
| Hypothyroid (serum) | a. 475.4 ± 236 μg/g | a. 438.4 ± 186 μg/g | - | [39] | |
| Hypothyroid (erythrocytes) | a. 2466 ± 314 μg/g Dry Weight | a. 2570 ± 456 μg/g Dry Weight | - | [52] | |
| Hypothyroid (serum) | a. 57.0 ± 26.6 μg/dL | a. 74.0 ± 36.7 μg/dL | ↓ | [32] | |
| Zn | Reference values: serum—60.0–120.0 µg/dL; urine—15.0–120.0 μg/dL | Arup Laboratories | [20] | ||
| Reference values: serum—0.66–1.10 µg/dL | Mayo Clinic Laboratories | [21] | |||
| Hypothyroid (serum) | a. 9.448 ± 2.124 μg/g | a. 7.944 ± 1.787 μg/g | - | [31] | |
| Autoimmune thyroiditis patients with subclinical hypothyroidism (serum) | a. Pretreatment: 109.3 ± 34.3 μg/dL Posttreatment: 103.6 ± 35.3 μg/dL | a. 101.5 ± 10.7 μg/dL | - | [28] | |
| Hypothyroid (serum) | b. 696.7 ± 299.9 μg/L | b. 1865.1 ± 1040.89 μg/L | ↓ | [44] | |
| Hypothyroid (serum) | a. 11.7 ± 5.3 μg/g | a. 66.7 ± 49.9 μg/g | ↓ | [39] | |
| Hashimoto disease (serum) | a. 12.2 ± 1.4 μM/L | a. 12.5 ± 2.8 μM/L | - | [38] | |
| Hypothyroid (erythrocytes) | a. 42 ± 13 μg/g Dry Weight | a. 34 ± 10 μg/g Dry Weight | - | [52] | |
| Hypothyroid (serum) | a. 12.19 ± 3.33 | a. 12.99 ± 2.70 | - | [36] | |
| Thyroid patients (serum) | a. 1025.0 ± 232.6 μg/L | a. 1068.0 ± 230.0 μg/L | ↓ | [34] | |
| Hypothyroid (serum) | a. 1053.56 ± 113.2 μg/L | a. 548.42 ± 59.48 μg/L | ↑ | [43] | |
| Hypothyroid (serum) | a. 85.206 ± 36.112 μg/dL | a. 100.825 ± 23.865 μg/dL | ↓ | [33] | |
| Hashimoto thyroiditis (thyroid tissue) | a. 6035 ± 3628 ng/g | a. 6098 ± 2480 ng/g | ↓ | [47] | |
| Hashimoto thyroiditis(blood) | a. 1707 ± 243 ng/g | a. 4801 ± 1124 ng/g | |||
| Hashimoto thyroiditis(urine) | a. 94.3 ± 62.3 ng/g | a. 217 ± 177 ng/g | |||
| Overweight (serum) | a. Pretreatment: 263.2 ± 91 6th month: 353.3 ± 141 | a. 342.3 ± 102 | ↓ | [27] | |
| Obese(serum) | a. Pretreatment: 292.6 ± 140 6th month: 257.5 ± 132 | ||||
| Morbidly obese (serum) | a. Pretreatment: 254.6 ± 125 6th month: 251.5 ± 114 | ||||
| Cu | Reference values:serum—70.0–140.0 μg/dLM; 80.0–155.0 μg/dLW; urine—0.3–3.2 μg/dL | Arup Laboratories | [20] | ||
| Reference values: serum—0.75–1.45 µg/mL; urine—(>18 years) 9–71 mcg/24 h | Mayo Clinic Laboratories | [21] | |||
| Hypothyroid (serum) | a. 2.397 ± 0.148 μg/g | a. 1.718 ± 0.123 μg/g | ↑ | [31] | |
| Autoimmune thyroiditis patients with SH (serum) | a. Pretreatment: 108.1 ± 53.08 mmol/ Posttreatment: 118.6 ± 46.5 mmol/L | a. 106.9 ± 14.9 mmol/L | - | [28] | |
| Hypothyroid (serum) | b. 919.6 ± 365.4 μg/L | b. 454.5 ± 871.67 μg/L | ↑ | [44] | |
| Hypothyroid (serum) | a. 29.0 ± 10.4 μg/g | a. 39.2 ± 14.5 μg/g | ↓ | [39] | |
| Hashimoto disease (serum) | a. 17.5 ± 2.3 μM/L | a. 17.3 ±3.0 μM/L | - | [38] | |
| Thyroid patients (serum) | a. 1365.0 ± 372.9 μg/L | a. 1394.0 ± 398.3 μg/L | - | [34] | |
| Hypothyroid (serum) | a. 151.113 ± 51.015 μg/dL | a. 140.500 ± 21.223 μg/dL | - | [33] | |
| Hypothyroid (serum) | a. 987.15 ± 246.03 μg/dL | a. 718.26 ± 146.60 μg/dL | ↑ | [43] | |
| Hypothyroid (erythrocytes) | a. 9.6 ± 3.8 μg/g Dry Weight | a. 9.6 ± 2.1 μg/g Dry Weight | - | [52] | |
| Hashimoto thyroiditis (thyroid tissue) | a. 515 ± 398 ng/g | a. 335 ± 153 ng/g | ↓ | [47] | |
| Hashimoto thyroiditis(blood) | a. 545 ± 131 ng/g | a. 965 ± 258 ng/g | |||
| Hashimoto thyroiditis(urine) | a. 132 ± 96.0 ng/g | a. 17.8 ± 3.40 ng/g | |||
| Congenital hypothyroidism (serum) | a. 1384.2 ± 388.8μg/L | - | [26] | ||
| Overweight (serum) | a. Pretreatment: 229.7 ± 193.7 6th month: 145.3 ± 30.7 | a. 172.7 ± 22.9 | ↑ | [27] | |
| Obese (serum) | a. Pretreatment: 195.2 ± 35.6 6th month: 132.5 ± 37.2 | ||||
| Morbidly obese (serum) | a. Pretreatment: 187 ± 50.9 6th month: 147.5 ± 38.7 | ||||
| Mn | Reference values: serum—0.0–0.2 μg/L; blood—4.2–16.5 μg/L | Arup Laboratories | [20] | ||
| Reference values: serum—<2.4 ng/mL; blood—4.7–18.3 ng/ml | Mayo Clinic Laboratories | [21] | |||
| Hypothyroid (serum) | a. 0.987 ± 0.103 μg/g | a. 0.899 ± 0.101 μg/g | - | [31] | |
| Hypothyroid (serum) | b. 50.3 ± 116.5 μg/L | b. 109.0 ± 87.43 μg/L | ↓ | [44] | |
| Hypothyroidism (serum) | a. 8.98 ± 3.9 μg/L | a. 0.92 ± 0.25 μg/L | ↑ | [43] | |
| Hashimoto thyroiditis (thyroid tissue) | a. 209 ± 125 ng/g | a. 129 ± 64.7 ng/g | ↑ | [47] | |
| Hashimoto thyroiditis(blood) | a. 16.5 ± 9.36 ng/g | a. 14.4 ± 7.82 ng/g | |||
| Hashimoto thyroiditis(urine) | a. 4.21 ± 3.66 ng/g | a. 3.69 ± 1.02 ng/g | |||
| Hypothyroid (serum) | a. 1.29 ± 0.27 | a. 2.37 ± 0.34 | ↓ | [35] | |
| Overweight (serum) | a. Pretreatment: 2.5 ± 0.4 6th month: 3.5 1.5 | a. 2.1 ± 0.3 | ↑ | [27] | |
| Obese (serum) | a. Pretreatment: 2.5 ± 0.3 6th month: 3.0 ± 1.4 | ||||
| Morbidly obese (serum) | a. Pretreatment: 2.7 ± 0.8 6th month: 3.1 ± 1.1 | ||||
| Cr | Reference values: serum—<5.0 µg/L | Arup Laboratories | [20] | ||
| Reference values: blood—18 years: <1.0 ng/mL | Mayo Clinic Laboratories | [21] | |||
| Hypothyroid (serum) | a. 12.31 ± 1.229 μg/g | a. 8.422 ± 0.886 μg/g | ↑ | [31] | |
| Hypothyroid (serum) | b. 14.0 ±10.0 μg/L | b. 170.1 ±173.01 μg/L | ↓ | [44] | |
| Hypothyroid (serum) | a. 31.6 ± 11.3 μg/g | a. 18.9 ± 7.6 μg/g | ↑ | [39] | |
| Hypothyroid (serum) | a. 16.41 ± 3.65 μg/L | a. 0.42 ± 0.00 μg/L | ↑ | [43] | |
| Cd | Reference values: - | Arup Laboratories | [20] | ||
| Reference values: blood—<5.0 ng/mL | Mayo Clinic Laboratories | [21] | |||
| Hypothyroid (serum) | a. 1.182 ± 0.114 μg/g | a. 0.423 ± 0.035 μg/g | ↑ | [31] | |
| Hypothyroid (serum) | b. 2.4 ± 3.1 μg/L | b. 45.3 ± 44.07 μg/L | - | [44] | |
| Hypothyroid (serum) | a. 1.1 ± 0.5 μg/g | a. 0.42 ± 0.31 μg/g | ↑ | [39] | |
| Hypothyroid (serum) | a. 0.50 ± 0.29 μg/L | a. 0.02 ± 0.00 μg/L | ↑ | [43] | |
| Hashimoto thyroiditis (thyroid tissue) | a. 50.7 ± 37.3 ng/g | a. 39.5 ± 29.7 ng/g | - | [47] | |
| Hashimoto thyroiditis(blood) | a. 0.25 ± 0.23 ng/g | a. 0.77 ± 0.56 ng/g | ↓ | ||
| Hashimoto thyroiditis(urine) | a. 0.78 ± 0.52 ng/g | a. 1.14 ± 1.12 ng/g | - | ||
| Pb | Reference values: blood (venous)—≤4.9 μg/dL | Arup Laboratories | [20] | ||
| Reference values: blood (venous)—<5.0 mcg/dL; urine—<2 mcg/24 h | Mayo Clinic Laboratories | [21] | |||
| Hypothyroid (serum) | a. 12.84 ± 1.287 μg/g | a. 5.365 ± 0.761 μg/g | ↑ | [31] | |
| Hypothyroid (serum) | a. 5.58 ± 2.8 μg/g | a. 4.0 ± 2.5μg/g | ↑ | [39] | |
| Hypothyroid (whole blood) | a. Pretreatment: 3.44 ± 1.7 μg/dL Posttreatment: 2.74 ± 1.3 μg/dL | a. 4.18 ± 1.7 μg/dL | ↑ | [46] | |
| Hypothyroid (urine) | a. Pretreatment: 3.42 ± 2.1 μg/gCr Posttreatment: 6.25 ± 3.6 μg/gCr | a. 4.03 ± 2.2 μg/gCr | |||
| Hashimoto thyroiditis(thyroid tissue) | a. 88.2 ± 51.9 ng/g | a. 29.8 ± 23.0 ng/g | ↑ | [47] | |
| Hashimoto thyroiditis(blood) | a. 24.2 ± 12.0 ng/g | a. 12.3 ±7.65 ng/g | |||
| Hashimoto thyroiditis(urine) | a. 0.18 ± 0.13 ng/g | a. 0.53 ± 0.17 ng/g | |||
| Se | Reference values: serum/plasma—23.0–190.0 μg/L; urine—12.0–40.0 µg/l | Arup Laboratories | [20] | ||
| Reference values: serum—70–150 ng/mL; blood—≥150–241 ng/ml | Mayo Clinic Laboratories | [21] | |||
| Autoimmune thyroiditis patients with subclinical hypothyroidism (serum) | a. Pretreatment: 67.7 ± 10.4 μg/dL Posttreatment: 66.2 ± 15.7 μg/dL | a. 83.7 ± 17.3 μg/dL | ↓ | [28] | |
| Hypothyroid (serum) | b. 49.3 ± 14.6 μg/L | b. 54.1 ± 11.13 μg/L | - | [44] | |
| Hashimoto disease(serum) | a. 0.75 ± 0.11 μM/L | a. 0.76 ± 0.12 μM/L | - | [38] | |
| Thyroid patients (serum) | a. 76.9 ± 18.8 μg/L | a. 85.1 ± 17.4 μg/L | ↓ | [34] | |
| Hashimoto thyroiditis(serum) | a. 0.72 ± 0.09 μM/L | 5th and 95th centiles 0.7–1.2 μM/L | - | [45] | |
| Hypothyroidism (serum) | a. 98.6 ± 31.1 μg/L | a. 75.9 ± 11.07 μg/L | ↑ | [43] | |
| Hashimoto thyroiditis (serum) | median and interquartile ranges 51.9 (44.6–58.5) μg/L | median and interquartile ranges 56.0 (52.4–61.5) μg/; | - | [29] | |
| Hashimoto thyroiditis+LT4 (serum) | median and interquartile ranges 54.4 (44–63.4) μg/L | median and interquartile ranges 56.0 (52.4–61.5) μg/L | - | ||
| Hashimoto thyroiditis (serum) | a. 91.6 ± 17.7 μg/L | a. 97.2 ± 29.4 μg/L | - | [37] | |
| Hypothyroid (serum) | a. 85.9 ± 14.8 μg/L | a. 97.2 ± 29.4 μg/L | - | ||
| Hypothyroid(erythrocytes) | a. 0.50 ± 0.09 μg/g Dry Weight | a.0.47 ± 0.11 μg/g Dry Weight | - | [52] | |
| Hashimoto thyroiditis (thyroid tissue) | a. 102 ± 50.2 ng/g | a. 158 ± 102 ng/g | ↓ | [47] | |
| Hashimoto thyroiditis(blood) | a. 84.2 ± 28.9 ng/g | a. 95.4 ± 28.3 ng/g | |||
| Hashimoto thyroiditis(urine) | a. 65.1 ± 35.0 ng/g | a. 37.2 ± 15.5 ng/g | |||
| Hashimoto thyroiditis (serum) | a. 0.87 ± 0.29 μmol/L | a. 1.11 ± 0.37 μmol/L | ↓ | [40] | |
| Hashimoto thyroiditis (plasma) | a. 86.7 ± 37.1 μg/L | a. 89.3 ± 28.7 μg/L | - | [49] | |
| Autoimmune thyroid disease(serum) | a. 1st trimester: 66.6 ± 12.6 μg/L 2nd trimester: 59.0 ± 9.9 μg/L 3rd trimester: 52.2 ± 11.6 μg/L | a. 1st trimester: 64.6 ± 14.6 μg/L 2nd trimester: 57.8 ± 14.0 μg/L 3rd trimester: 48.4 ± 11.3 μg/L | - | [24] | |
| Hypothyroid(venous blood) | a. 160.47 ± 25.76 µg/L | a. 206.72 ± 17.98 µg/L | - | [25] | |
| Hypothyroid (plasma) | a. 98.79 ± 13.63 μg/L | - | [48] | ||
| Congenital hypothyroidism (serum) | a. 69.2 ± 17.4 μg/L | - | [26] | ||
| Overweight (serum) | a. Pretreatment: 76.4 ± 21 6th month: 74.6 ± 30.2 | a. 53.1 ± 27.9 | ↑ | [27] | |
| Obese (serum) | a. Pretreatment: 78.7 ± 24.5 6th month: 60.5 ± 23.6 | ||||
| Morbidly obese (serum) | a. Pretreatment: 77.5 ± 25.7 6th month: 67.2 ± 19.9 | ||||
| Pregnant women (serum) | a. 136.9 ± 47.9 μg/L | - | [30] | ||
| F | Reference values: plasma—<4.1 mcmol/L | Mayo Clinic Laboratories | [21] | ||
| Iodine deficient adults (urine) | UFSG 1.06 ± 1.11 mg/L | - | [51] | ||
| Non-iodine deficient adults (urine) | UFSG 0.91 ± 0.65 mg/L | - | |||
| Healthy children (serum) | mean I: 0.03 ppm II: 0.035 ppm III: 0.05 ppm | - | [41] | ||
| Children with dental fluorosis (urine) | range 0.24–8.9 ppm | range (urine) 0.19–1.01 ppm range (serum) 0.02–0.09 ppm | ↑ | [42] | |
| Children with dental fluorosis (serum) | range 0.02–0. 77 ppm | ||||
| Children without dental fluorosis (urine) | range 0.4–7.79 ppm | ||||
| Children without dental fluorosis (serum) | range 0.03–0.75 ppm | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Błażewicz, A.; Wiśniewska, P.; Skórzyńska-Dziduszko, K. Selected Essential and Toxic Chemical Elements in Hypothyroidism—A Literature Review (2001–2021). Int. J. Mol. Sci. 2021, 22, 10147. https://doi.org/10.3390/ijms221810147
Błażewicz A, Wiśniewska P, Skórzyńska-Dziduszko K. Selected Essential and Toxic Chemical Elements in Hypothyroidism—A Literature Review (2001–2021). International Journal of Molecular Sciences. 2021; 22(18):10147. https://doi.org/10.3390/ijms221810147
Chicago/Turabian StyleBłażewicz, Anna, Patrycja Wiśniewska, and Katarzyna Skórzyńska-Dziduszko. 2021. "Selected Essential and Toxic Chemical Elements in Hypothyroidism—A Literature Review (2001–2021)" International Journal of Molecular Sciences 22, no. 18: 10147. https://doi.org/10.3390/ijms221810147
APA StyleBłażewicz, A., Wiśniewska, P., & Skórzyńska-Dziduszko, K. (2021). Selected Essential and Toxic Chemical Elements in Hypothyroidism—A Literature Review (2001–2021). International Journal of Molecular Sciences, 22(18), 10147. https://doi.org/10.3390/ijms221810147