

The Effect of Renal Denervation on T Cells in Patients with Resistant Hypertension
 , , and
, , and
Abstract
:1. Introduction
2. Results
2.1. Baseline Characteristics
2.2. Patients with Resistant Hypertension Display High Levels of Inflammatory Markers
2.3. Differences in T-Cell Subsets between Patients with Hypertension and Healthy Controls
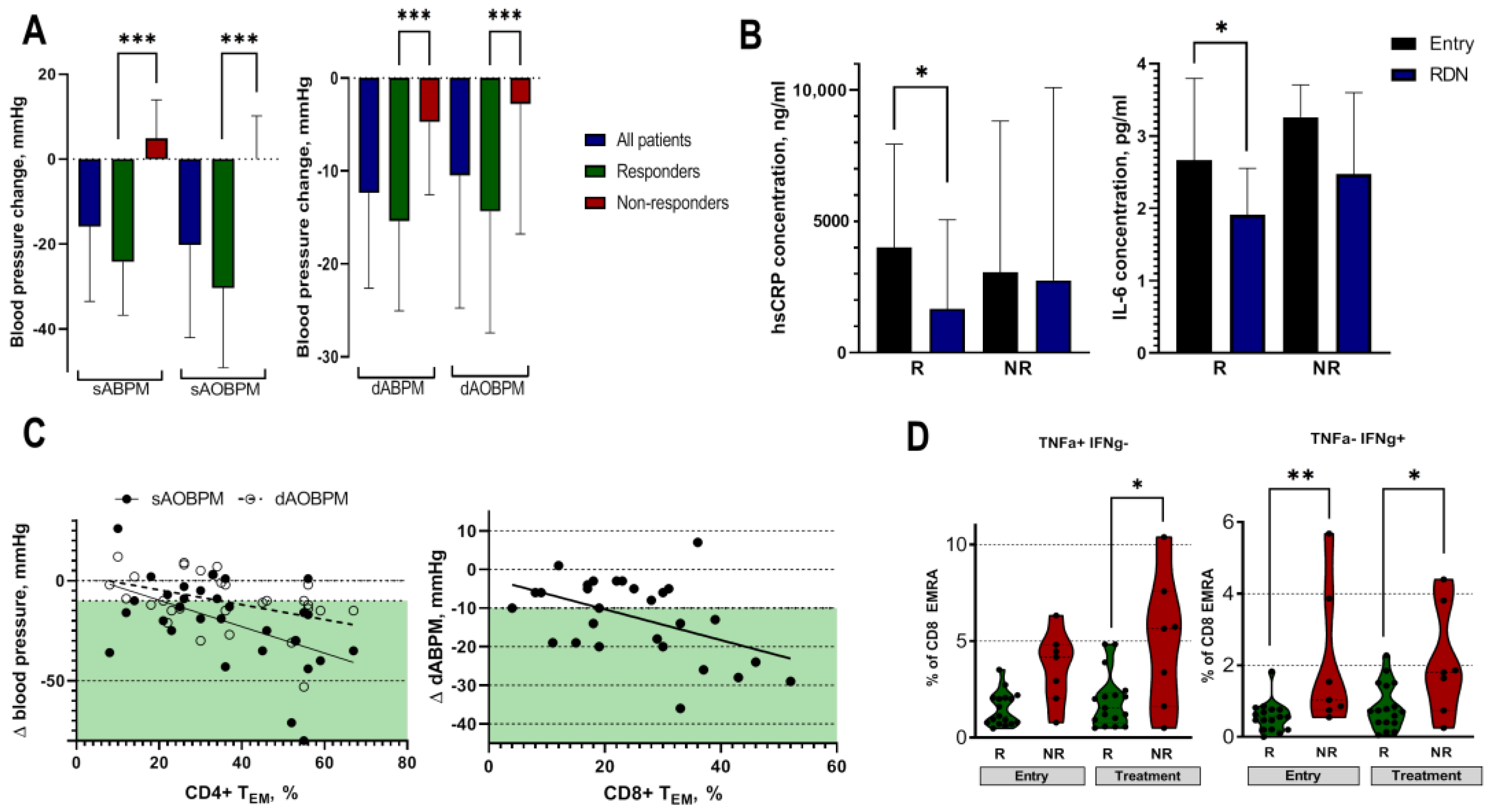
2.4. Effect of RDN on Blood Pressure and Low-Grade Inflammation
2.5. Effect of RDN on T-Cell Signatures
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. Renal Denervation Procedure
4.3. Follow-Up of Patients with RH after Renal Denervation Procedure
4.4. Measurement of Inflammation Markers
4.5. Measurement of T-Cell Signature
4.6. Data Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhou, B.; Carrillo-Larco, R.M.; Danaei, G.; Riley, L.M.; Paciorek, C.J.; Stevens, G.A.; Gregg, E.W.; Bennett, J.E.; Solomon, B.; Singleton, R.K.; et al. Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: A pooled analysis of 1201 population-representative studies with 104 million participants. Lancet 2021, 398, 957–980. [Google Scholar] [CrossRef] [PubMed]
- Kearney, P.M.; Whelton, M.; Reynolds, K.; Muntner, P.; Whelton, P.K.; He, J. Global burden of hypertension: Analysis of worldwide data. Lancet 2005, 365, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Zhou, D.; Xi, B.; Zhao, M.; Wang, L.; Veeranki, S.P. Uncontrolled hypertension increases risk of all-cause and cardiovascular disease mortality in US adults: The NHANES III Linked Mortality Study. Sci. Rep. 2018, 8, 9418. [Google Scholar] [CrossRef] [Green Version]
- Dai, H.; Bragazzi, N.L.; Younis, A.; Zhong, W.; Liu, X.; Wu, J.; Grossman, E. Worldwide Trends in Prevalence, Mortality, and Disability-Adjusted Life Years for Hypertensive Heart Disease from 1990 to 2017. Hypertension 2021, 77, 1223–1233. [Google Scholar] [CrossRef]
- Wei, J.; Galaviz, K.I.; Kowalski, A.J.; Magee, M.J.; Haw, J.S.; Narayan, K.M.V.; Ali, M.K. Comparison of Cardiovascular Events among Users of Different Classes of Antihypertension Medications: A Systematic Review and Network Meta-analysis. JAMA Netw. Open 2020, 3, e1921618. [Google Scholar] [CrossRef] [Green Version]
- Hopstock, L.A.; Eggen, A.E.; Lochen, M.L.; Mathiesen, E.B.; Nilsen, A.; Njolstad, I.; Wilsgaard, T. Blood pressure target achievement and antihypertensive medication use in women and men after first-ever myocardial infarction: The Tromsø Study 1994–2016. Open Hear. 2018, 5, e000746. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banegas, J.R.; López-García, E.; Dallongeville, J.; Guallar, E.; Halcox, J.P.; Borghi, C.; Massó-González, E.L.; Jiménez, F.J.; Perk, J.; Steg, P.G.; et al. Achievement of treatment goals for primary prevention of cardiovascular disease in clinical practice across Europe: The EURIKA study. Eur. Heart J. 2011, 32, 2143–2152. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Rosei, E.A.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [Green Version]
- Cardoso, C.R.L.; Salles, G.F. Refractory hypertension and risks of adverse cardiovascular events and mortality in patients with resistant hypertension: A prospective cohort study. J. Am. Heart Assoc. 2020, 9, e017634. [Google Scholar] [CrossRef]
- Kaczmarski, K.R.; Sozio, S.M.; Chen, J.; Sang, Y.; Shafi, T. Resistant hypertension and cardiovascular disease mortality in the US: Results from the National Health and Nutrition Examination Survey (NHANES). BMC Nephrol. 2019, 20, 138. [Google Scholar] [CrossRef] [Green Version]
- Grassi, G. The Sympathetic Nervous System in Hypertension: Roadmap Update of a Long Journey. Am. J. Hypertens. 2021, 34, 1247–1254. [Google Scholar] [CrossRef] [PubMed]
- Tsioufis, C.; Kordalis, A.; Flessas, D.; Anastasopoulos, I.; Tsiachris, D.; Papademetriou, V.; Stefanadis, C. Pathophysiology of resistant hypertension: The role of sympathetic nervous system. Int. J. Hypertens. 2011, 2011, 642416. [Google Scholar] [CrossRef] [Green Version]
- Hering, L.; Rahman, M.; Potthoff, S.A.; Rump, L.C.; Stegbauer, J. Role of α2-Adrenoceptors in Hypertension: Focus on Renal Sympathetic Neurotransmitter Release, Inflammation, and Sodium Homeostasis. Front. Physiol. 2020, 11, 566871. [Google Scholar] [CrossRef] [PubMed]
- Hering, L.; Rahman, M.; Hoch, H.; Markó, L.; Yang, G.; Reil, A.; Yakoub, M.; Gupta, V.; Potthoff, S.A.; Vonend, O.; et al. α2A-Adrenoceptors modulate renal sympathetic neurotransmission and protect against hypertensive kidney disease. J. Am. Soc. Nephrol. 2020, 31, 783–798. [Google Scholar] [CrossRef]
- Saxena, M.; Schmieder, R.E.; Kirtane, A.J.; Mahfoud, F.; Daemen, J.; Basile, J.; Lurz, P.; Gosse, P.; Sanghvi, K.; Fisher, N.D.L.; et al. Predictors of blood pressure response to ultrasound renal denervation in the RADIANCE-HTN SOLO study. J. Hum. Hypertens. 2022, 36, 629–639. [Google Scholar] [CrossRef]
- Fengler, K.; Reimann, P.; Rommel, K.P.; Kresoja, K.P.; Blazek, S.; Unterhuber, M.; Besler, C.; von Roeder, M.; Böhm, M.; Desch, S.; et al. Comparison of long-term outcomes for responders versus non-responders following renal denervation in resistant hypertension. J. Am. Heart Assoc. 2021, 10, e022429. [Google Scholar] [CrossRef]
- Azizi, M.; Sanghvi, K.; Saxena, M.; Gosse, P.; Reilly, J.P.; Levy, T.; Rump, L.C.; Persu, A.; Basile, J.; Bloch, M.J.; et al. Ultrasound renal denervation for hypertension resistant to a triple medication pill (RADIANCE-HTN TRIO): A randomised, multicentre, single-blind, sham-controlled trial. Lancet 2021, 397, 2476–2486. [Google Scholar] [CrossRef] [PubMed]
- Burlacu, A.; Brinza, C.; Floria, M.; Stefan, A.E.; Covic, A.; Covic, A. Predicting Renal Denervation Response in Resistant High Blood Pressure by Arterial Stiffness Assessment: A Systematic Review. J. Clin. Med. 2022, 11, 4837. [Google Scholar] [CrossRef]
- Carnagarin, R.; Matthews, V.; Zaldivia, M.T.K.; Peter, K.; Schlaich, M.P. The bidirectional interaction between the sympathetic nervous system and immune mechanisms in the pathogenesis of hypertension. Br. J. Pharmacol. 2019, 176, 1839–1852. [Google Scholar] [CrossRef]
- Ziegler, K.A.; Ahles, A.; Wille, T.; Kerler, J.; Ramanujam, D.; Engelhardt, S. Local sympathetic denervation attenuates myocardial inflammation and improves cardiac function after myocardial infarction in mice. Cardiovasc. Res. 2018, 114, 291–299. [Google Scholar] [CrossRef] [Green Version]
- Xiao, L.; Kirabo, A.; Wu, J.; Saleh, M.A.; Zhu, L.; Wang, F.; Takahashi, T.; Loperena, R.; Foss, J.D.; Mernaugh, R.L.; et al. Renal denervation prevents immune cell activation and renal inflammation in Angiotensin II-induced hypertension. Circ. Res. 2015, 117, 547–557. [Google Scholar] [CrossRef] [PubMed]
- Marvar, P.J.; Thabet, S.R.; Guzik, T.J.; Lob, H.E.; McCann, L.A.; Weyand, C.; Gordon, F.J.; Harrison, D.G. Central and peripheral mechanisms of T-lymphocyte activation and vascular inflammation produced by angiotensin II-induced hypertension. Circ. Res. 2010, 107, 263–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Werdan, K. The activated immune system in congestive heart failure-from dropsy to the cytokine paradigm. J. Intern. Med. 1998, 243, 87–92. [Google Scholar]
- Slota, C.; Shi, A.; Chen, G.; Bevans, M.; Weng N ping. Norepinephrine preferentially modulates memory CD8 T cell function inducing inflammatory cytokine production and reducing proliferation in response to activation. Brain Behav. Immun. 2015, 46, 168–179. [Google Scholar] [CrossRef] [Green Version]
- Xiao, L.; do Carmo, L.S.; Foss, J.D.; Chen, W.; Harrison, D.G. Sympathetic enhancement of memory T-cell homing and hypertension sensitization. Circ. Res. 2020, 126, 708–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trott, D.W.; Thabet, S.R.; Kirabo, A.; Saleh, M.A.; Itani, H.; Norlander, A.E.; Wu, J.; Goldstein, A.; Arendshorst, W.J.; Madhur, M.S.; et al. Oligoclonal CD8+ T cells play a critical role in the development of hypertension. Hypertension 2014, 64, 1108–1115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.; Bundy, J.D.; Hamm, L.L.; Hsu, C.Y.; Lash, J.; Miller, E.R.; Thomas, G.; Cohen, D.L.; Weir, M.R.; Raj, D.S.; et al. Inflammation and apparent treatment-resistant hypertension in patients with chronic kidney disease: The results from the CRIC study. Hypertension 2019, 73, 785–793. [Google Scholar] [CrossRef]
- Chamarthi, B.; Williams, G.H.; Ricchiuti, V.; Srikumar, N.; Hopkins, P.N.; Luther, J.M.; Jeunemaitre, X.; Thomas, A. Inflammation and hypertension: The interplay of interleukin-6, dietary sodium, and the renin-angiotensin system in humans. Am. J. Hypertens. 2011, 24, 1143–1148. [Google Scholar] [CrossRef]
- Delgado-Silva, J.; Rodrigues-Santos, P.; Almeida, J.S.; Santos-Rosa, M.; Gonçalves, L. Dynamics of Soluble Factors and Double-Negative T Cells Associated with Response to Renal Denervation in Resistant Hypertension Patients. J. Pers. Med. 2022, 12, 343. [Google Scholar] [CrossRef]
- Rodriguez, I.J.; Lalinde Ruiz, N.; Llano León, M.; Martínez Enríquez, L.; Montilla Velásquez, M.D.P.; Ortiz Aguirre, J.P.; Rodríguez Bohórquez, O.M.; Velandia Vargas, E.A.; Hernández, E.D.; Parra López, C.A. Immunosenescence Study of T Cells: A Systematic Review. Front. Immunol. 2021, 11, 3460. [Google Scholar] [CrossRef]
- Olson, N.C.; Doyle, M.F.; Jenny, N.S.; Huber, S.A.; Psaty, B.M.; Kronmal, R.A.; Tracy, R.P. Decreased Naive and Increased Memory CD4+ T Cells Are Associated with Subclinical Atherosclerosis: The Multi-Ethnic Study of Atherosclerosis. PLoS ONE 2013, 8, e71498. [Google Scholar] [CrossRef]
- De Ciuceis, C.; Rossini, C.; Airò, P.; Scarsi, M.; Tincani, A.; Tiberio, G.A.M.; Piantoni, S.; Porteri, E.; Solaini, L.; Duse, S.; et al. Relationship between different subpopulations of circulating CD4+ T-lymphocytes and microvascular structural alterations in humans. Am. J. Hypertens. 2017, 30, 51–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rattik, S.; Engelbertsen, D.; Wigren, M.; Ljungcrantz, I.; Östling, G.; Persson, M.; Fredrikson, G.N.; Bengtsson, E.; Nilsson, J.; Björkbacka, H. Elevated circulating effector memory T cells but similar levels of regulatory T cells in patients with type 2 diabetes mellitus and cardiovascular disease. Diabetes Vasc. Dis. Res. 2019, 16, 270–280. [Google Scholar] [CrossRef] [Green Version]
- Kundu, S.; Freiberg, M.S.; Tracy, R.P.; So-Armah, K.A.; Koethe, J.R.; Duncan, M.S.; Tindle, H.A.; Beckman, J.A.; Feinstein, M.J.; McDonnell, W.J.; et al. Circulating T Cells and Cardiovascular Risk in People with and Without HIV Infection. J. Am. Coll. Cardiol. 2022, 80, 1633–1644. [Google Scholar] [CrossRef] [PubMed]
- Padgett, L.E.; Dinh, H.Q.; Wu, R.; Gaddis, D.E.; Araujo, D.J.; Winkels, H.; Nguyen, A.; McNamara, C.A.; Hedrick, C.C. Naive CD8+T Cells Expressing CD95 Increase Human Cardiovascular Disease Severity. Arterioscler. Thromb. Vasc. Biol. 2020, 40, 2845–2859. [Google Scholar] [CrossRef] [PubMed]
- Lang, D.; Nahler, A.; Lambert, T.; Grund, M.; Kammler, J.; Kellermair, J.; Blessberger, H.; Kypta, A.; Steinwender, C.; Auer, J. Anti-Inflammatory Effects and Prediction of Blood Pressure Response by Baseline Inflammatory State in Catheter-Based Renal Denervation. J. Clin. Hypertens. 2016, 18, 1173–1179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fengler, K.; Rommel, K.P.; Blazek, S.; Von Roeder, M.; Besler, C.; Hartung, P.; Desch, S.; Thiele, H.; Lurz, P. Predictors for profound blood pressure response in patients undergoing renal sympathetic denervation. J. Hypertens. 2018, 36, 1578–1584. [Google Scholar] [CrossRef]
- Balasubramanian, P.; Hall, D.; Subramanian, M. Sympathetic nervous system as a target for aging and obesity-related cardiovascular diseases. GeroScience 2019, 41, 13–24. [Google Scholar] [CrossRef]
- Zaldivia, M.T.K.; Rivera, J.; Hering, D.; Marusic, P.; Sata, Y.; Lim, B.; Eikelis, N.; Lee, R.; Lambert, G.W.; Esler, M.D.; et al. Renal Denervation Reduces Monocyte Activation and Monocyte-Platelet Aggregate Formation: An Anti-Inflammatory Effect Relevant for Cardiovascular Risk. Hypertension 2017, 69, 323–331. [Google Scholar] [CrossRef] [Green Version]
- Dörr, O.; Liebetrau, C.; Möllmann, H.; Mahfoud, F.; Ewen, S.; Gaede, L.; Troidl, C.; Hoffmann, J.; Busch, N.; Laux, G.; et al. Beneficial effects of renal sympathetic denervation on cardiovascular inflammation and remodeling in essential hypertension. Clin. Res. Cardiol. 2015, 104, 175–184. [Google Scholar] [CrossRef]
- Fliser, D.; Buchholz, K.; Haller, H. Antiinflammatory effects of angiotensin II subtype 1 receptor blockade in hypertensive patients with microinflammation. Circulation 2004, 110, 1103–1107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Awad, K.; Zaki, M.M.; Mohammed, M.; Banach, M. Effect of the renin angiotensin system inhibitors on inflammatory markers: A systematic review and meta-analysis of 32 randomized controlled trials. Eur. Heart J. 2021, 42 (Suppl. S1), ehab724.2383. [Google Scholar] [CrossRef]
- Caccamo, N.; Joosten, S.A.; Ottenhoff, T.H.M.; Dieli, F. Atypical Human Effector/Memory CD4+ T Cells with a Naive-Like Phenotype. Front. Immunol. 2018, 9, 2832. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Rafferty, T.M.; Rhee, S.W.; Webber, J.S.; Song, L.; Ko, B.; Hoover, R.S.; He, B.; Mu, S. CD8+ T cells stimulate Na-Cl co-transporter NCC in distal convoluted tubules leading to salt-sensitive hypertension. Nat. Commun. 2017, 8, 14037. [Google Scholar] [CrossRef] [Green Version]
- Carnevale, D.; Carnevale, L.; Perrotta, S.; Pallante, F.; Migliaccio, A.; Iodice, D.; Perrotta, M.; Lembo, G. Chronic 3D Vascular-Immune Interface Established by Coculturing Pressurized Resistance Arteries and Immune Cells. Hypertension 2021, 78, 1648–1661. [Google Scholar] [CrossRef]
- Kirabo, A.; Fontana, V.; De Faria, A.P.C.; Loperena, R.; Galindo, C.L.; Wu, J.; Bikineyeva, A.T.; Dikalov, S.; Xiao, L.; Chen, W.; et al. DC isoketal-modified proteins activate T cells and promote hypertension. J. Clin. Investig. 2014, 124, 4642–4656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henegar, J.R.; Zhang, Y.; Hata, C.; Narciso, I.; Hall, M.E.; Hall, J.E. Catheter-based radiofrequency renal denervation: Location effects on renal norepinephrine. Am. J. Hypertens. 2015, 28, 909–914. [Google Scholar] [CrossRef] [Green Version]
- Tzafriri, A.R.; Mahfoud, F.; Keating, J.H.; Spognardi, A.M.; Markham, P.M.; Wong, G.; Highsmith, D.; O’Fallon, P.; Fuimaono, K.; Edelman, E.R. Procedural and anatomical determinants of multielectrode renal denervation efficacy: Insights from preclinical models. Hypertension 2019, 74, 546–554. [Google Scholar] [CrossRef]
- Cohen-Mazor, M.; Mathur, P.; Stanley, J.R.L.; Mendelsohn, F.O.; Lee, H.; Baird, R.; Zani, B.G.; Markham, P.M.; Rocha-Singh, K. Evaluation of renal nerve morphological changes and norepinephrine levels following treatment with novel bipolar radiofrequency delivery systems in a porcine model. J. Hypertens. 2014, 32, 1678–1692. [Google Scholar] [CrossRef] [Green Version]
- Madhur, M.S.; Harrison, D.G. Senescent T cells and hypertension: New ideas about old cells. Hypertension 2013, 62, 13–15. [Google Scholar] [CrossRef] [Green Version]
- Mahfoud, F.; Schmieder, R.; Davies, J.; Kandzari, D.E.; Weil, J.; Whitbourn, R. Catheter-based renal sympathetic denervation—Long-term symplicityTM renal denervation clinical evidence, new data and future perspectives. Interv. Cardiol. Rev. Res. Resour. 2013, 8, 118–123. [Google Scholar]
- Puleo, A.; Carroll, C.; Maecker, H.; Gupta, R. Isolation of PBMCs Using Vacutainer® Cellular Preparation Tubes (CPTTM). Bio-Protocol 2017, 7, e2103. [Google Scholar] [CrossRef]
- Barcelo, H.; Faul, J.; Crimmins, E.; Thyagarajan, B. A Practical Cryopreservation and Staining Protocol for Immunophenotyping in Population Studies. Curr. Protoc. Cytom. 2018, 84, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, S.; Maecker, H. Intracellular Cytokine Staining (ICS) on Human Lymphocytes or Peripheral Blood Mononuclear Cells (PBMCs). Bio-Protocol 2015, 5, e1442. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Parameter | RH | RH Treatment | ||
|---|---|---|---|---|
| Responder | Non-Responder | Responder | Non-Responder | |
| Age, y | 66.0 ± 5.8 | 51.2 ± 12.2 *** | 66.5 ± 5.8 | 51.7 ± 12.2 *** |
| Sex (M:F) | 12:8 | 5:5 | 12:8 | 5:5 |
| AOBPM, mmHg | 169 ± 15/92±18 | 167 ± 18/92 ± 19 | 139 ± 14/78 ± 10 ### | 167 ± 16/89 ± 10 ** |
| ABPM, mmHg | 159 ± 17/90 ±12 | 150 ± 6/90 ± 8 | 139 ± 14/78 ± 10 ### | 155 ± 8/85 ± 10 ** |
| Antihypertensive, N | 5.0 ± 1.0 | 6.0 ± 1.0 | 5.0 ± 2.0 | 6.0 ± 1.0 |
| Antihypertensive class | ||||
| ― ACEi/ARB | 17 (85%) | 10 (100%) | 18 (90%) | 10 (100%) |
| ― MRA | 4 (20%) | 2 (20%) | 7 (35%) | 3 (30%) |
| ― CCB | 17 (85%) | 8 (80%) | 16 (80%) | 8 (80%) |
| ― Diuretic | 19 (95%) | 10 (100%) | 15 (75%) | 10 (100%) |
| ― β-Blocker | 12 (60%) | 8 (80%) | 14 (70%) | 8 (80%) |
| ― α-Blocker | 7 (35%) | 4 (40%) | 6 (30%) | 2 (20%) |
| ― Other | 17 (85%) | 8 (80%) | 16 (80%) | 7 (70%) |
| BMI | 30.2 ± 5.8 | 30.8 ± 5.8 | 30.2 ± 5.8 | 30.8 ± 5.8 |
| OSAS, N (%) | 14 (70%) | 4 (40%) * | 14 (70%) | 4 (40%) * |
| Diabetes, N (%) | 5 (25%) | 3 (30%) | 5 (25%) | 3 (30%) |
| Hb1AC, % | 6.0 ± 0.9 | 5.9 ± 0.7 | 6.0 ± 0.9 | 5.8 ± 0.7 |
| eGFR, mL/min | 72 ± 27 | 75 ± 28 | 72 ± 27 | 75 ± 28 |
| hsCRP, ng/mL | 4041 (1261–8023) | 3063 (1043–8823) | 1909 (499–5110) # | 2745 (1331–10,099) |
| TNFα, pg/mL | 2.1 (1.5–2.9) | 2.6 (1.4–3.7) | 2.3 (1.8–2.8) | 2.7 (1.7–5.4) |
| IL-6, pg/mL | 2.8 (1.5–3.8) | 2.5 (1.7–3.6) | 1.9 (1.5–2.5) # | 3.2 (2.0–3.7) * |
| CD4, % | 65 ± 17 | 61 ± 14 | 65 ±15 | 63 ± 14 |
| CD4 TCM, % | 39 ± 17 | 38 ± 15 | 36 ± 15 | 39 ± 16 |
| CD4 TEM, % | 39 ± 18 | 29 ± 12 * | 38 ± 19 | 25 ± 8 * |
| CD4 TEMRA, % | 4 (2–8) | 7 (2–12) | 5 (3–9) | 4 (2–10) |
| CD4 naïve, % | 19 ± 13 | 27 ± 7 ** | 20 ± 15 | 26 ± 7 |
| CD8, % | 35 ± 17 | 39 ± 14 | 35 ± 15 | 37 ± 14 |
| CD8 TCM, % | 17 ± 8 | 15 ± 9 | 14 ± 7 # | 17 ± 8 |
| CD8 TEM, % | 26 ± 13 | 24 ± 9 | 25 ± 12 | 21 ± 8 |
| CD8 TEMRA, % | 11 (7–20) | 24 (10–39) * | 11 (7–17) | 25 (9–44) ** |
| CD8 naïve, % | 38 ± 13 | 37 ± 17 | 38 ± 15 | 33 ± 14 |
| CD4/CD8 | 2.3 (1.1–4.4) | 1.4 (0.9–2.9) | 2.2 (1.0–3.5) | 1.5 (1.0–3.3) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kantauskaite, M.; Vonend, O.; Yakoub, M.; Heilmann, P.; Maifeld, A.; Minko, P.; Schimmöller, L.; Antoch, G.; Müller, D.N.; Schmidt, C.; et al. The Effect of Renal Denervation on T Cells in Patients with Resistant Hypertension. Int. J. Mol. Sci. 2023, 24, 2493. https://doi.org/10.3390/ijms24032493
Kantauskaite M, Vonend O, Yakoub M, Heilmann P, Maifeld A, Minko P, Schimmöller L, Antoch G, Müller DN, Schmidt C, et al. The Effect of Renal Denervation on T Cells in Patients with Resistant Hypertension. International Journal of Molecular Sciences. 2023; 24(3):2493. https://doi.org/10.3390/ijms24032493
Chicago/Turabian StyleKantauskaite, Marta, Oliver Vonend, Mina Yakoub, Philipp Heilmann, Andras Maifeld, Peter Minko, Lars Schimmöller, Gerald Antoch, Dominik N. Müller, Claudia Schmidt, and et al. 2023. "The Effect of Renal Denervation on T Cells in Patients with Resistant Hypertension" International Journal of Molecular Sciences 24, no. 3: 2493. https://doi.org/10.3390/ijms24032493
APA StyleKantauskaite, M., Vonend, O., Yakoub, M., Heilmann, P., Maifeld, A., Minko, P., Schimmöller, L., Antoch, G., Müller, D. N., Schmidt, C., Duvnjak, B., Zierhut, U., Potthoff, S. A., Rump, L. C., Fischer, J. C., & Stegbauer, J. (2023). The Effect of Renal Denervation on T Cells in Patients with Resistant Hypertension. International Journal of Molecular Sciences, 24(3), 2493. https://doi.org/10.3390/ijms24032493