
Diversity and Traditional Use Knowledge of Medicinal Plants among Communities in the South and South-Eastern Zones of the Tigray Region, Ethiopia



Abstract
:1. Introduction
2. Materials and Methods
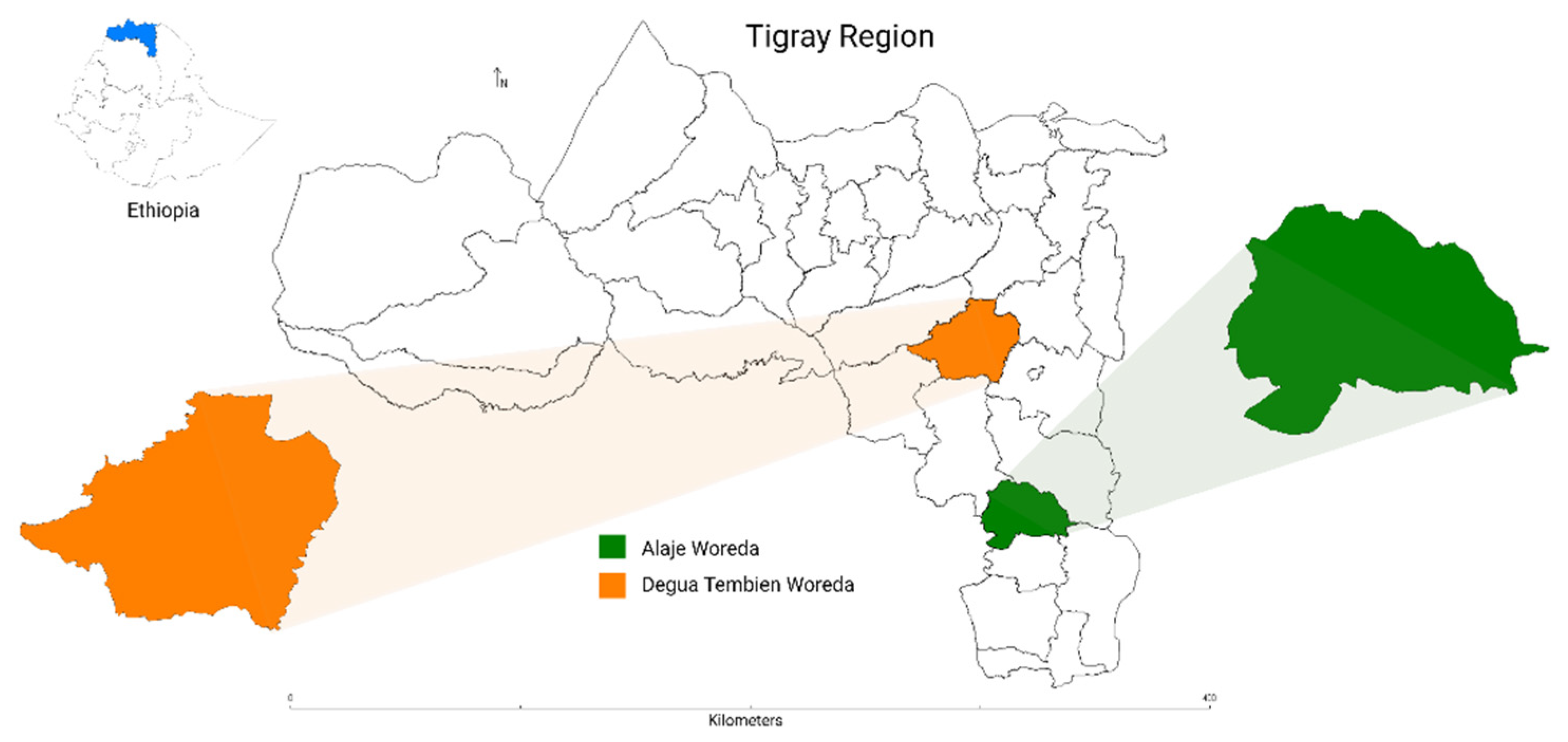
2.1. Geo-Physiological Features of the Study Areas
2.2. Land Use and Climate of the Study Areas
2.3. Study Participant Selection and Data Collection
2.4. Ethnobotanical Data Collection
2.5. Data Analysis
3. Results
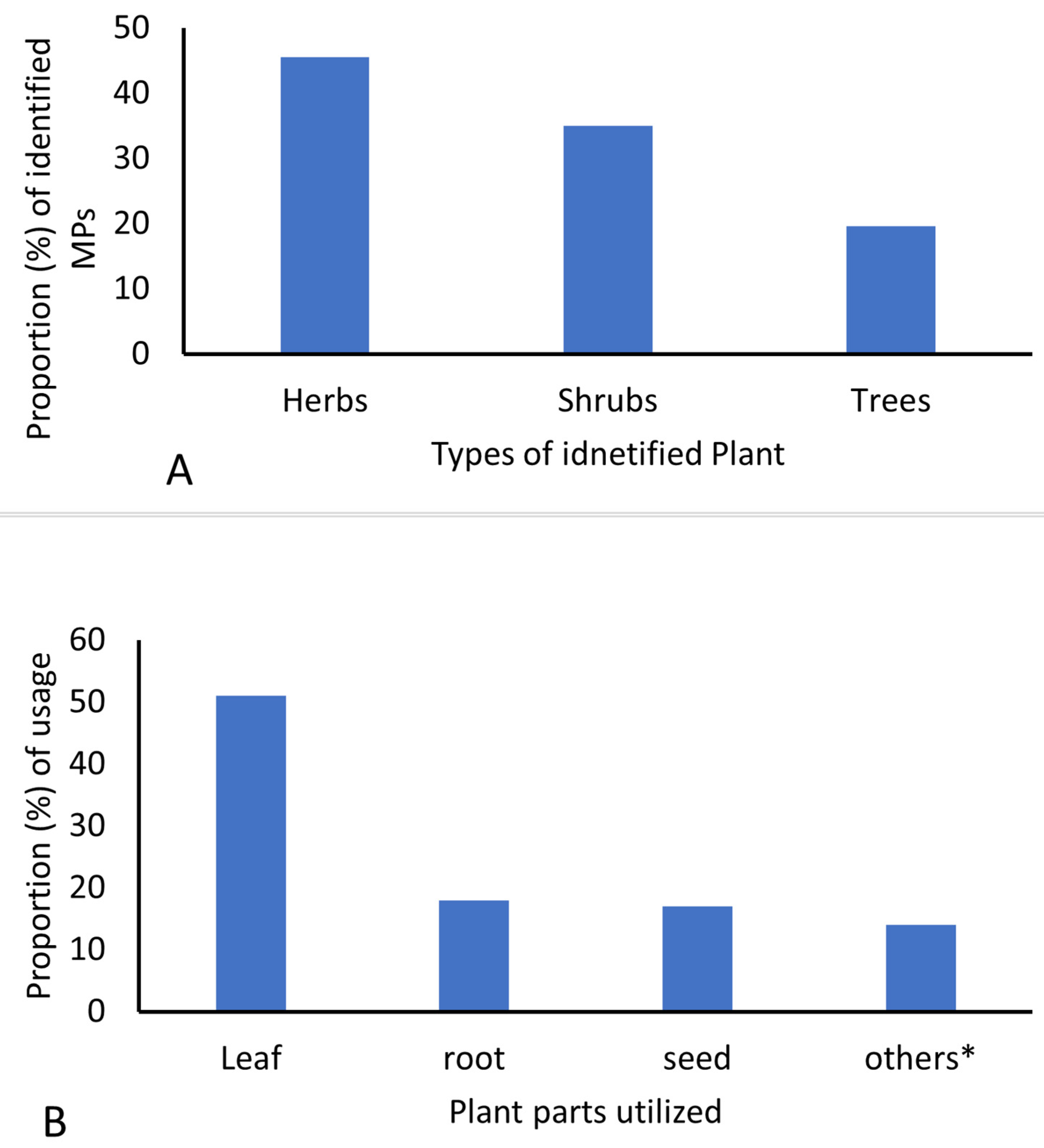
3.1. Diversity of MPs Identified in the Study Areas
3.2. Diseases Treated Using Herbal Medicine
3.3. Local Knowledge of Traditional Medicine
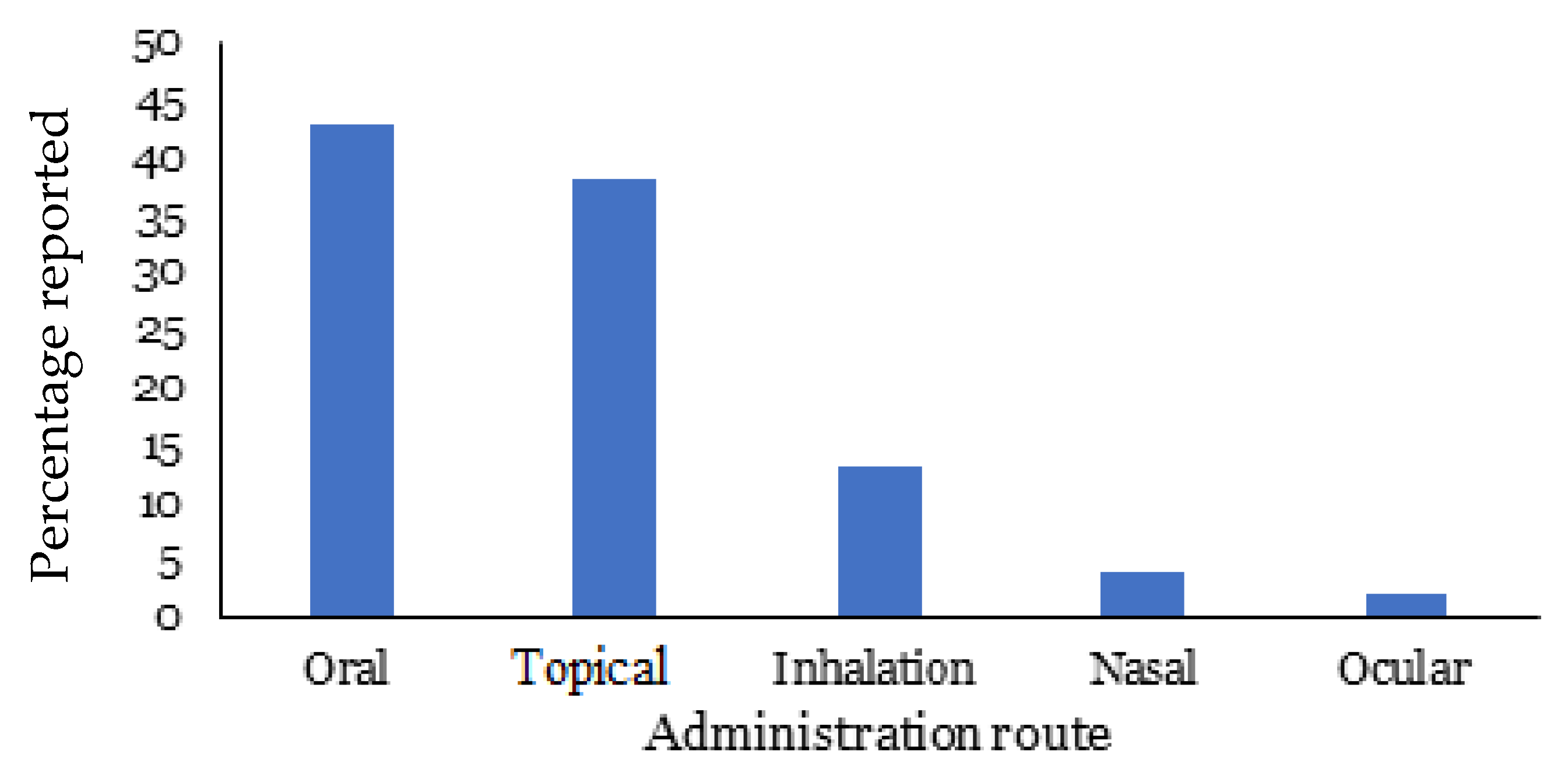
3.4. Herbal Medicine Preparation, Form, and Dosage
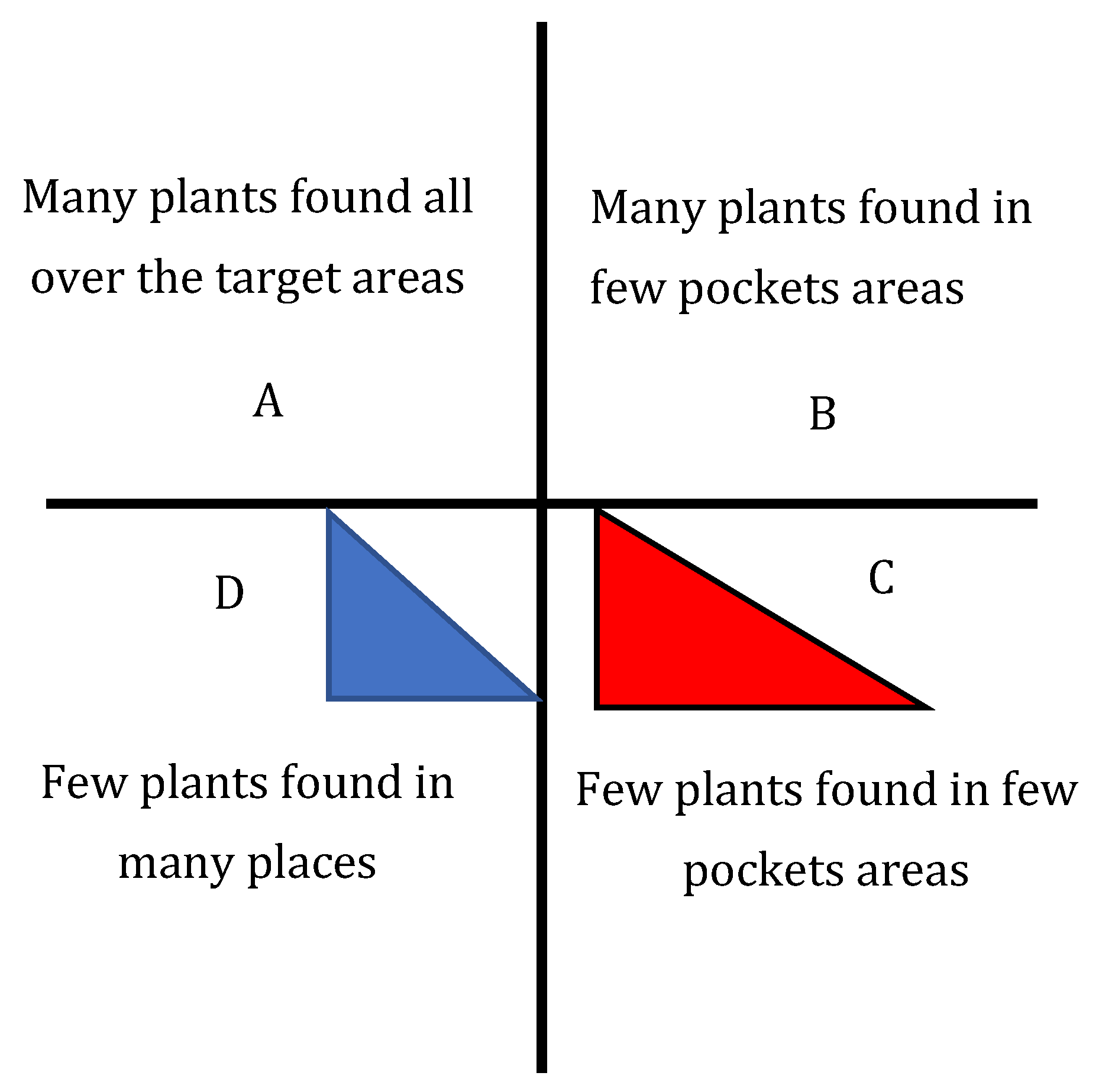
3.5. Abundance of the Identified Medicinal Plants
4. Discussion
- Increase the interest of the young generations in the use of herbal medicine for health maintenance and treatment.
- Promote herbal medicine as a livelihood strategy for many individuals.
- Continue to provide traditional healers with access to traditional MPs within their vicinity, so that they are not forced to travel long distances to gather them.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Birhanu, T.; Abera, D.; Ejeta, E. Ethnobotanical study of medicinal plants in selected Horro Gudurru Woredas, Western Ethiopia. J. Biol. Agric. Healthc. 2015, 5, 83–93. [Google Scholar]
- Bekele, G.; Reddy, P. Ethnobotanical study of medicinal plants used to treat human aliment by Guji Oromo tribes in Abaya district, Borena, Oromia, Ethiopia. Univers. J. Plant Sci. 2015, 3, 1–8. [Google Scholar] [CrossRef]
- Bekele, E. Study on Actual Situation of Medicinal Plants in Ethiopia. Japan Association for International Collaboration of Agriculture and Forestry (JAICAF). 2007. Available online: http://www.endashaw.com (accessed on 15 September 2021).
- Teklay, A.; Abera, B.; Giday, M. An ethnobotanical study of medicinal plants used in Kilte Awulaelo District, Tigray Region of Ethiopia. J. Ethnobiol. Ethnomed. 2013, 9, 65. [Google Scholar] [CrossRef] [Green Version]
- Desissa, D.; Binggeli, P. Uses and Conservation Status of Medicinal Plans Used by the Shinasha People. Available online: http://www.mikepalmer.co.uk/woodyplantecology/ethiopia/shinasha.html (accessed on 20 April 2016).
- Cunningham, A. African Medicinal Plants: Setting Priorities at the Interface between Conservation and Primary Health Care; People and Plants Working Paper I; Paris, UNESCO, 7 Place de Fontenoy: Paris, France, 1993. [Google Scholar]
- Fullas, F. Ethiopian Traditional medicines: Common medicinal plants in perspective. J. Black Stud. 2002, 32, 610–612. [Google Scholar]
- FAO. Health and Wealth from Medicinal Aromatic Plants; Diversification Booklet 17; Rural Infrastructure and Agro-Industries Division Food and Agriculture Organization of the United Nations: Rome, Italy, 2012. [Google Scholar]
- WHO. African Traditional Medicine; The AFRO Technical Report Series, 1; Report of the Regional Expert Committee; WHO: Brazzaville, Congo, 1976; pp. 3–4. [Google Scholar]
- Tolossa, T.; Megersa, M. Ethnobotanical Study of Medicinal Plants Used to Treat Human Diseases in Berbere District, Bale Zone of Oromia Regional State, South East Ethiopia. Evid.-Based Complement. Altern. Med. 2018, 2018, 8602945. [Google Scholar]
- Aragaw, T.; Afework, D.; Getahun, K. Assessment of Knowledge, Attitude, and Utilization of Traditional Medicine among the Communities of Debre Tabor Town, Amhara Regional State, North Central Ethiopia: A Cross-Sectional Study. Evid.-Based Complement. Altern. Med. 2020, 2020, 6565131. [Google Scholar] [CrossRef] [Green Version]
- Zerabruk, S.; Yirga, G. Traditional knowledge of medicinal plants in Gindeberet district, Western Ethiopia. S. Afr. J. Bot. 2012, 78, 165–169. [Google Scholar] [CrossRef]
- Mansouri, S.; Kazemi, I.; Baghestani, A.; Zayeri, F.; Ghorbanifar, Z. Evaluating the effect of Coriandrum sativum syrup on being migraine-free using mixture models. Med. J. Islamic Repub. Iran 2020, 34, 44. [Google Scholar] [CrossRef]
- Pal, S.; Shukla, Y. Herbal medicine: Current status and the future. Asian Pac. J. Cancer Prev. 2003, 4, 281–288. [Google Scholar]
- Birhane, E.; Aynekulu, E.; Mekuria, W.; Endale, D. Management, use and ecology of medicinal plants in the degraded dry lands of Tigray, Northern Ethiopia. J. Med. Plant Res. 2011, 5, 309–318. [Google Scholar]
- Tewodros, G.; Biadgilgn, D.; Tesfamariam, Z. Assessment of Natural Resources and Its Implication for Ecotourism Development in Hashenge Watershed. Master’s Thesis, Mekelle University, Mekelle, Ethiopia, 2014. [Google Scholar]
- Lepers, E.; Lambin, E.F.; Janetos, A.C.; Defries, R.; Achard, F.; Ramankutty, N.; Scholes, R.J. A synthesis of information on rapid land-cover change for the period 1981–2000. BioScience 2005, 55, 115–124. [Google Scholar] [CrossRef]
- Gebrewahid, L.; Dejene, K.M.; Yemane, T.; Addis, A.; Dereje, A.A. Variability among Ethiopian durum wheat genotypes grown under different climatic conditions of Tigray for some agronomic and grain-quality traits. J. Crop Improv. 2021, 35, 184–203. [Google Scholar] [CrossRef]
- Mengistu, D.; Afewerki, Y.K.; Jemal, N.M.; Yemane, T.; Carlo, F. Exploitation of diversity within farmers’ durum wheat varieties enhanced the chance of selecting productive, stable and adaptable new varieties to the local climatic conditions. Plant Genet. Resour. Charact. Util. 2019, 17, 401–411. [Google Scholar] [CrossRef]
- Teklehymanot, T.; Giday, M. Ethnobotanical study of medicinal plants used by people in Zegie Peninsula, Northern Ethiopia. J. Ethnobiol. Ethnomed. 2007, 3, 12. [Google Scholar] [CrossRef] [Green Version]
- Mengistu, M.; Kebede, D.; Atomsa, D.; Abebe, A.; Alemnie, D. Status and utilization of medicinal and aromatic plants in Eastern Hararghe, Ethiopia. Cogent Food Agric. 2019, 5, 1701349. [Google Scholar] [CrossRef]
- Alexiades, M.; Sheldon, J. Selected guidelines for ethnobotanical research: A field manual. Adv. Econ. Bot. 1996, 10, 167–169. [Google Scholar]
- Sthapit, B.R.; Shrestha, P.; Upadhyay, M. (Eds.) On-Farm Management of Agricultural Biodiversity in Nepal: Good Practices, 2nd ed.; NARC/LI-BIRD/Bioversity International: Pokhara, Nepal, 2012. [Google Scholar]
- Getnet, Z.; Chandrodyam, S.; Masresha, G. Studies on traditional medicinal plants in Ambagiorgis area of Wogera district, Amhara regional state, Ethiopia. Int. J. Pure Appl. Biosci. 2016, 4, 38–45. [Google Scholar]
- Wondimu, T.; Asfaw, Z.; Kelbessa, E. Ethnobotanical study of medicinal plants around ‘Dheeraa’ town, Arsi Zone, Ethiopia. J. Ethnopharmacol. 2007, 112, 152–161. [Google Scholar] [CrossRef]
- Tilahun, T. Ethnobotanical study of knowledge and medicinal plants use by the people in Dek Island in Ethiopia. J. Ethnopharmacol. 2009, 124, 69–78. [Google Scholar]
- Lauren, A. Faith as a Means of Healing: Traditional Medicine and the Ethiopian Orthodox Church in and around Lalibela. Independent Study Project (ISP) Collection. 128. Available online: https://digitalcollections.sit.edu/ispcollection/128 (accessed on 13 July 2021).
- Tizazu, G. Ethnobotanical Study of Medicinal Plants in the Konso Special Woreda (SNNPR), Ethiopia. Master’s Thesis, Addis Ababa University, Addis Ababa, Ethiopia, 2005. [Google Scholar]
- Tuasha, N.; Petros, B.; Asfaw, Z. Medicinal plants used by traditional healers to treat malignancies and other human ailments in Dalle District, Sidama Zone, Ethiopia. J. Ethnobiol. Ethnomed. 2018, 14, 15. [Google Scholar] [CrossRef] [Green Version]
- Schulz, V.; Hänsel, R.; Tyler, V. Rational Phytotherapy. A Physician’s Guide to Herbal Medicine, 4th ed.; Springer: Berlin, Germany, 2001. [Google Scholar]
- Asfaw, D.; Abebe, D.; Urga, K. Traditional medicine in Ethiopia: Perspectives and developmental efforts. J. Ethiop. Med. Pract. 1999, 1, 114–117. [Google Scholar]
- Addis, G.; Abebe, D.; Urga, K. A survey of traditional medicine in Shirka District, Arsi Zone, Ethiopia. Ethiop. Pharm. J. 2001, 19, 30–47. [Google Scholar]
- Moges, A.; Beyene, A.; Triest, L.; Ambelu, A.; Kelbessa, E. Imbalance of ecosystem services of wetlands and the perception of the local community towards their restoration and management in Jimma Highlands, Southwestern Ethiopia. Wetlands 2018, 38, 1081–1095. [Google Scholar] [CrossRef]
- Demissie, A. Biodiversity conservation of medicinal plants: Problems and prospects. In Conservation and Sustainable Use of Medicinal Plants in Ethiopia, Proceedings of the National Workshop on Biodiversity Conservation and Sustainable Use of Medicinal Plants in Ethiopia; Zewdu, M., Demissie, A., Eds.; Institute of Biodiversity Conservation and Research (IBCR): Addis Ababa, Ethiopia, 2001; pp. 56–64. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SN | Disease Treated | Number MPs Identified to Treat the Disease | Types of MPs | MP Parts Used to Treat the Disease | Administration | Administration Method and Frequency |
|---|---|---|---|---|---|---|
| 1 | Wound/swelling | 19 | Herbs/shrubs/trees | Seeds/stems/fruits/roots | Mostly topical | Ranges from a single dose to multiple applications until completely healed. |
| 2 | Abdominal pain | 15 | Herbs/trees/shrubs | Seeds/leaves/stems/fruits/roots/clades | Mostly oral | Dose and frequency vary, depending on patient age and plant parts used. |
| 3 | Eye infection | 5 | Herbs/trees/shrubs | Leaves/bark/fruits/roots | Ocular or through inhalation | Extracts of the parts applied to the infected eye in powder or liquid form. The dose varies, depending on patient age. |
| 4 | Toothache | 7 | Shrubs/herbs/trees | Leaves/seeds/roots | Oral | Chewing the recommended part and holding it on the affected tooth. Administration is continued until the pain ceases. |
| 5 | Hepatitis | 6 | Trees/herbs/shrubs | Leaves/seeds/roots/fruits | Orally or topically | The extract of the plant part is blended with butter, milk, coffee or human urine and taken orally or applied to the skin. Dosage varies, depending on the administration method applied. |
| 6 | Cough | 5 | Herbs/shrubs | Seeds/leaves/roots | Oral, inhalation or nasal | Boil the plant part and drink or inhale directly into the lungs until the patient is relieved of the cough. |
| 7 | Tonsilitis | 6 | Shrubs/herbs | Leaves/roots/stems/fruits/bark | Topical/oral | For children: crush the parts and apply dermally to the head. Adult: extract the part and take orally until the pain disappears. |
| 8 | Bone fracture/dislocation | 5 | Shrubs/tree | Roots/leaves | Topical | The plant parts are prepared into a paste and placed on broken or dislocated bones, and then bound with appropriate material. |
| 9 | Mental illness/epilepsy | 3 | Herbs | Leaves/roots | Inhalation/oral | Boil leaves and inhale the vapor. Extract of leaves and roots is eaten with injera. |
| 10 | Fever ** | 11 | Herbs/trees | Leaves/roots | Oral/inhalation | Boil the leaves and inhale the vapor, or add the leaves to coffee or tea and drink. |
| 11 | Malaria | 6 | Herbs/shrubs/trees | Leaves/seed/bulb/flower | Oral | Extracts of the selected parts are blended with food or drinks and consumed. |
| 12 | Heart disease | 1 | Shrubs | Fruits | Oral | Eat the fruit on an empty stomach. |
| 13 | Skin infections | 8 | Trees/herbs/shrubs | Leaves/seeds/roots | Topical | Parts are crushed and applied to the affected area. |
| 14 | Ear infections, such as otitis media | 4 | Shrubs/herbs | Seeds/fruits | Topical | Extracts of the selected parts are blended with binding agents (such as butter) and applied directly into the affected ear. |
| 15 | Hair follicle infection | 2 | Tree/herb | Leaves/seeds | Topical | Extracts are applied to the affected part. |
| 16 | Herpes simplex virus ** | 6 | Herbs/shrubs | Leaves/stems/roots/fruits | Topical | Extracts are applied to the affected area. |
| 17 | Arthritis | 3 | Shrubs | Stems/roots | Inhalation | The parts are boiled and vapor is inhaled. |
| 18 | Intestinal parasites ⸸ | 4 | Shrubs/trees | Leaves/roots/seeds | Oral | Eat or drink the extract of the selected parts alone or with other foodstuffs. |
| 19 | Hemorrhoid | 4 | Herbs/shrubs | Stems/leaves | Topical | Apply plant extracts to the affected parts. |
| 20 | Headache/migraine | 3 | Trees/herbs/shrubs | Leaves | Topical/inhalation | Crush leaves, blended with butter and applied to the head; dried parts are put on the fire and the smoke is inhaled. |
| 21 | Constipation | 2 | Herbs | Seeds | Oral | Grind the seeds, mix with water and drink. |
| 22 | Evil eye (buda) ⸶ | 1 | Shrub | Roots | Inhalation | Mix the root with Hangoro midri, boil and inhale the vapor. |
| 23 | Gonorrhea ⸶ | 1 | Shrubs | Fluid | Topical | Apply extracted fluid to the affected area. |
| 24 | Joint inflammation | 2 | Herbs/shrubs | Bulbs/seeds | Topical | Blend plant part with unguents/butter and apply to the inflamed area. |
| 25 | Tuberculosis | 1 | Shrub | Leaves | Apply prepared plant remedy to the affected areas. | |
| 26 | Herpes zoster | 2 | Herbs | Seeds/leaves | Topical | Boil in water and wash with it; or leaves burned to ash, blended with butter and applied to affected parts. |
| 27 | Sunstrike (Michi) | 5 | Herbs/shrubs | Leaves/stems/seeds | Inhalation | Boil plant parts, sometimes together, and inhale every evening until cured. |
| 28 | Stabbing chest pain | 5 | Trees/shrubs | Roots/leaves | Oral | Chew the parts, swallow the juice, but spit out the residue. |
| 29 | Insect bites δ | 2 | Shrubs/herbs | Leaves/roots | Fumigation | Burn the roots and leaves and fumigate the house to repel insects. |
| 30 | External bleeding | 1 | Tree | Leaves | Topical | Crush young leaves and tie on to the affected part. |
| SN | Animal Disease Treated | No. of MPs Identified to Treat the Disease | Types of Plants | Parts Used to Treat the Disease | Administration Method | Preparation and Administration |
|---|---|---|---|---|---|---|
| 1 | Abdominal pain | 3 | Trees | Leaves | Oral | Crush the leaves, squeeze and feed the juice to the animal. |
| 2 | Eye infection | 4 | Shrubs/herbs | Leaves/stems/roots | Ocular | Crush the leaves, squeeze them and apply the refined juice into the affected eye. |
| 3 | Blood-sucking insects ‡ | 9 | Shrubs/herbs/trees | Leaves | Topical, oral | Crush the identified part, mix with water and wash the animal’s body with it. |
| 4 | Rabies | 2 | Herbs/shrubs | Leaves | Topical | Dry the leaves, crush them, mix with butter and apply the paste to the bite wound by the rabid animal. |
| 5 | External wound | 5 | Herbs/shrubs/trees | Leaves/bark/fruits | Topical | Crush the plant part, mix with water and wash the affected body part. |
| SN | Therapeutical Use | Number of Medicinal Plants Used (Nt) | Use Citation (Nur) | FIC Value |
|---|---|---|---|---|
| 1 | Wound/swelling | 19 | 153 | 0.88 |
| 2 | Abdominal pain | 15 | 50 | 0.71 |
| 3 | Eye infection | 5 | 46 | 0.91 |
| 4 | Toothache | 7 | 34 | 0.82 |
| 5 | Hepatitis | 6 | 23 | 0.77 |
| 6 | Cough | 5 | 20 | 0.79 |
| 7 | Tonsilitis | 6 | 52 | 0.90 |
| 8 | Bone fractures/dislocation | 5 | 35 | 0.88 |
| 9 | Mental illness/epilepsy | 3 | 8 | 0.71 |
| 10 | Fever | 11 | 29 | 0.64 |
| 11 | Malaria | 6 | 31 | 0.83 |
| 12 | Heart disease | 1 | 4 | 1.00 |
| 13 | Skin infections | 8 | 26 | 0.72 |
| 14 | Ear infections, such A otitis media | 4 | 30 | 0.90 |
| 15 | Hair follicle infection | 2 | 4 | 0.67 |
| 16 | Herpes simplex virus | 6 | 8 | 0.29 |
| 17 | Arthritis | 3 | 25 | 0.92 |
| 18 | Intestinal parasites | 4 | 52 | 0.94 |
| 19 | Hemorrhoids | 4 | 12 | 0.73 |
| 20 | Headache/migraine | 3 | 42 | 0.95 |
| 21 | Constipation | 2 | 12 | 0.91 |
| 22 | Evil eye (buda) | 3 | 16 | 0.87 |
| 23 | Gonorrhea | 2 | 23 | 0.95 |
| 24 | Joint inflammation | 2 | 13 | 0.92 |
| 25 | Tuberculosis | 1 | 12 | 1.00 |
| 26 | Herpes zoster | 2 | 8 | 0.86 |
| 27 | Sunstrike (Michi) | 5 | 51 | 0.92 |
| 28 | Stabbing chest pain | 2 | 14 | 0.92 |
| 29 | Insect bite | 2 | 27 | 0.96 |
| 30 | External bleeding | 3 | 33 | 0.94 |
| SD | 4.01 | 27.64 | 0.14 |
| Sn | MPs | Therapeutical Use | Np | N | FL Value (%) |
|---|---|---|---|---|---|
| 1 | Allium sativum L. | Toothache, malaria, coughs | 51 | 53 | 96 |
| 2 | Aloe megalacantha Bark | Abdominal pain, ameba, gonorrhea, dislocated bone | 32 | 48 | 67 |
| 3 | Artemisia abyssinica Sch. | Mental illness/epilepsy, Agnin | 8 | 12 | 67 |
| 4 | Brassica nigra L. | Coughs, malaria | 53 | 53 | 100 |
| 5 | Calputina avena (Ait) | Hepatitis | 30 | 50 | 60 |
| 6 | Dodonia augustifolia L. f | Bone fractures, hair follicle infection, wounds | 24 | 40 | 60 |
| 7 | Eucalyptus globulus Labili | Migraine, fever, Michi (sunstrike) | 50 | 53 | 94 |
| 8 | Melia azandrachata L. | Abdominal pain | 45 | 50 | 90 |
| 9 | Merendra bengalensis | Epilepsy | 6 | 8 | 75 |
| 10 | Ricinus communis | Wounds | 48 | 53 | 91 |
| 11 | Rosa abyssinica | Arthritis | 10 | 14 | 71 |
| 12 | Rumex nervosus | Herpes simplex virus | 8 | 15 | 53 |
| 13 | Ruta chalepensis L. | Fever, coughs | 53 | 53 | 100 |
| 14 | Solanum bastifolium | Otitis media | 9 | 12 | 75 |
| 15 | Verbena officinalis | Tonsillitis, abdominal pain | 37 | 51 | 73 |
| SD (sample) | 18.73 | 18.98 | 15.74 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mengistu, D.K.; Mohammed, J.N.; Kidane, Y.G.; Fadda, C. Diversity and Traditional Use Knowledge of Medicinal Plants among Communities in the South and South-Eastern Zones of the Tigray Region, Ethiopia. Diversity 2022, 14, 306. https://doi.org/10.3390/d14040306
Mengistu DK, Mohammed JN, Kidane YG, Fadda C. Diversity and Traditional Use Knowledge of Medicinal Plants among Communities in the South and South-Eastern Zones of the Tigray Region, Ethiopia. Diversity. 2022; 14(4):306. https://doi.org/10.3390/d14040306
Chicago/Turabian StyleMengistu, Dejene K., Jemal N. Mohammed, Yosef Gebrehawaryat Kidane, and Carlo Fadda. 2022. "Diversity and Traditional Use Knowledge of Medicinal Plants among Communities in the South and South-Eastern Zones of the Tigray Region, Ethiopia" Diversity 14, no. 4: 306. https://doi.org/10.3390/d14040306
APA StyleMengistu, D. K., Mohammed, J. N., Kidane, Y. G., & Fadda, C. (2022). Diversity and Traditional Use Knowledge of Medicinal Plants among Communities in the South and South-Eastern Zones of the Tigray Region, Ethiopia. Diversity, 14(4), 306. https://doi.org/10.3390/d14040306