
Real-Time Electrical Bioimpedance Characterization of Neointimal Tissue for Stent Applications

 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
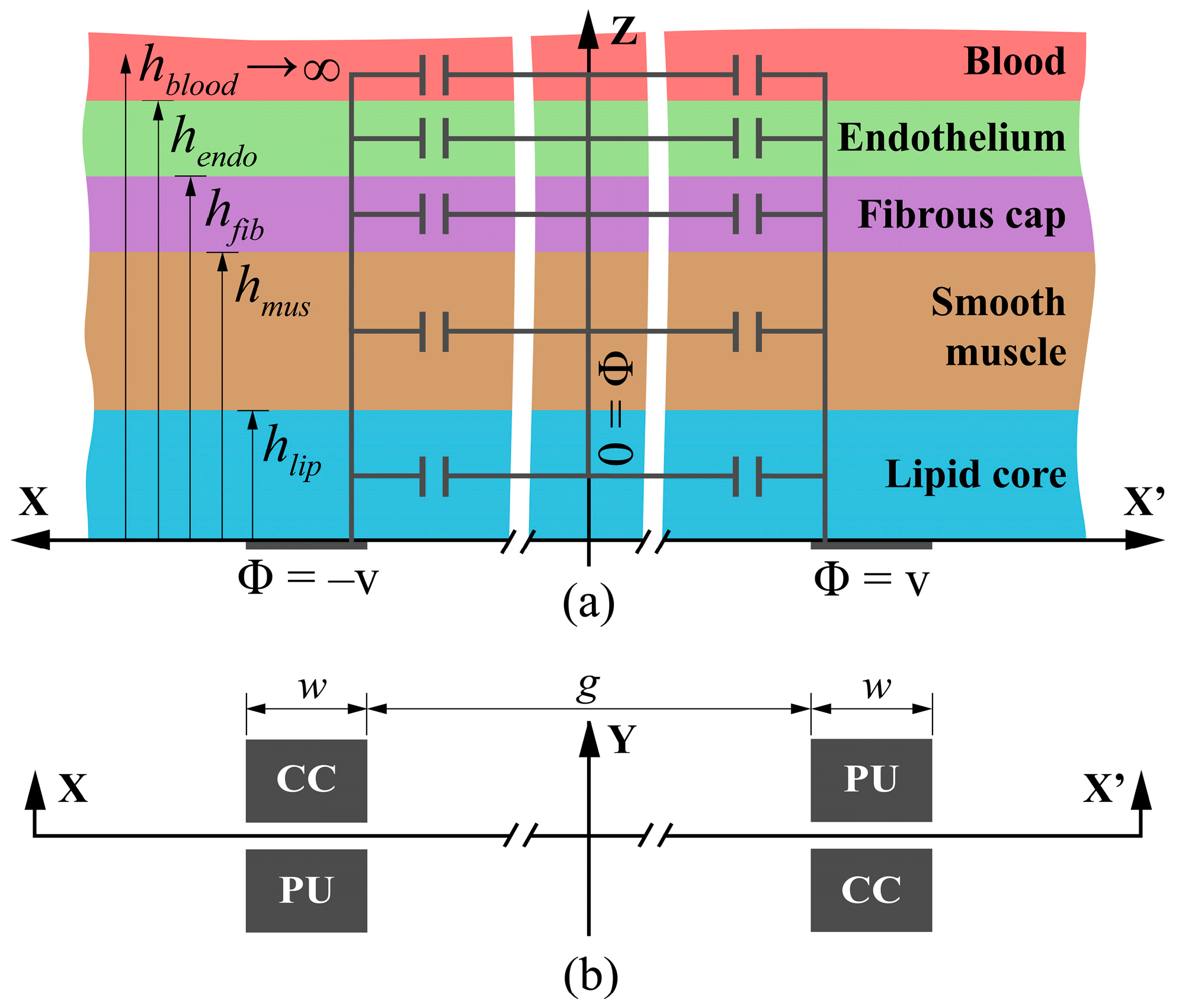
2.1. Analytical Model
2.1.1. Neointima–Blood Interface (“Double Layer”)
2.1.2. Dielectric Interface
- Dirichlet Boundary Condition (DBC), for ε2 ≫ ε1—constant electric potential at the interface (Φ = 0).
- Neumann Boundary Condition (NBC), for ε2 ≪ ε1—no potential gradient normal to the interface (∂Φ⁄∂n = 0).
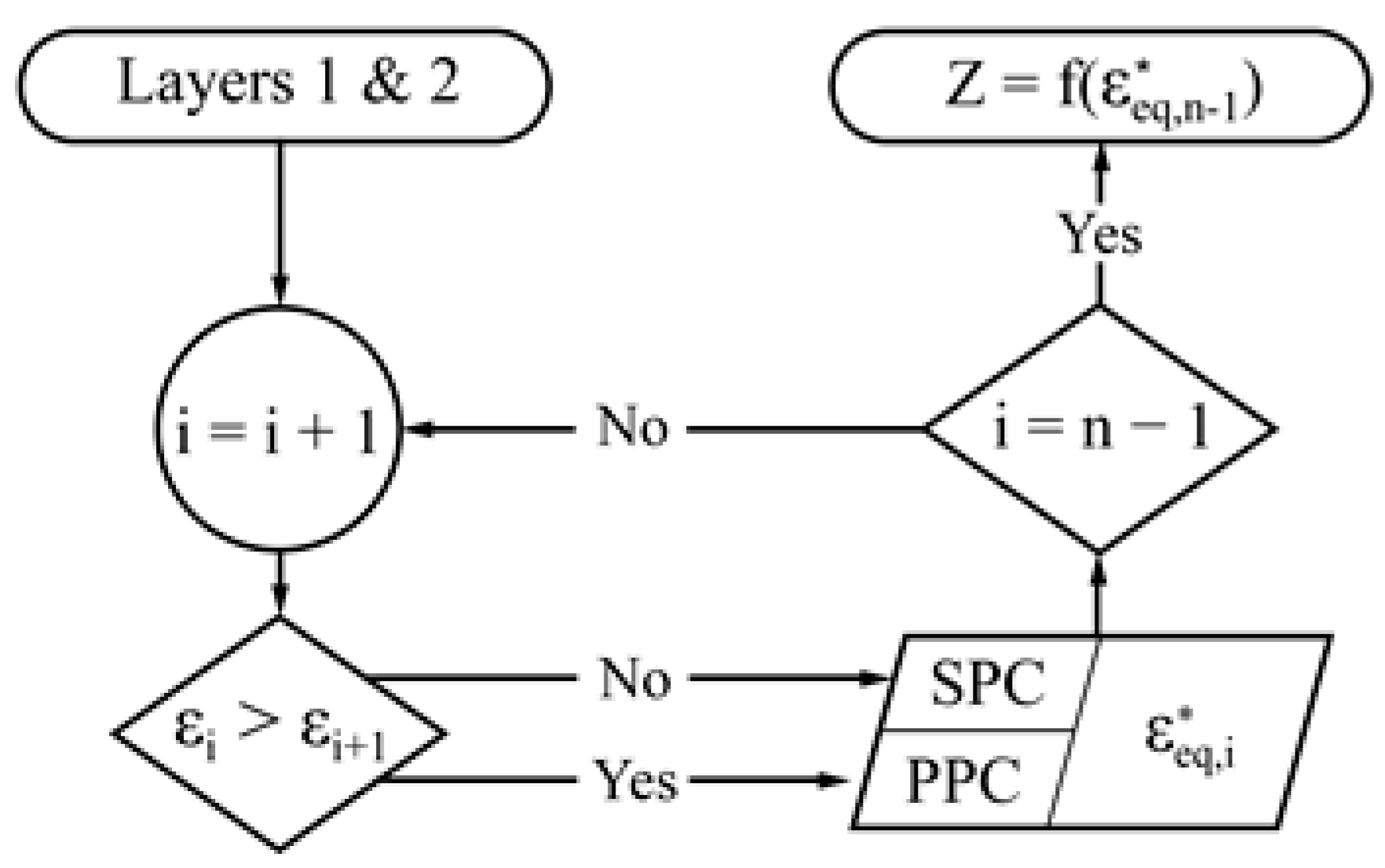
2.1.3. Partial Capacitance Method
2.1.4. Iterative Complex Method
2.2. Finite Element Analysis Simulations
3. Results
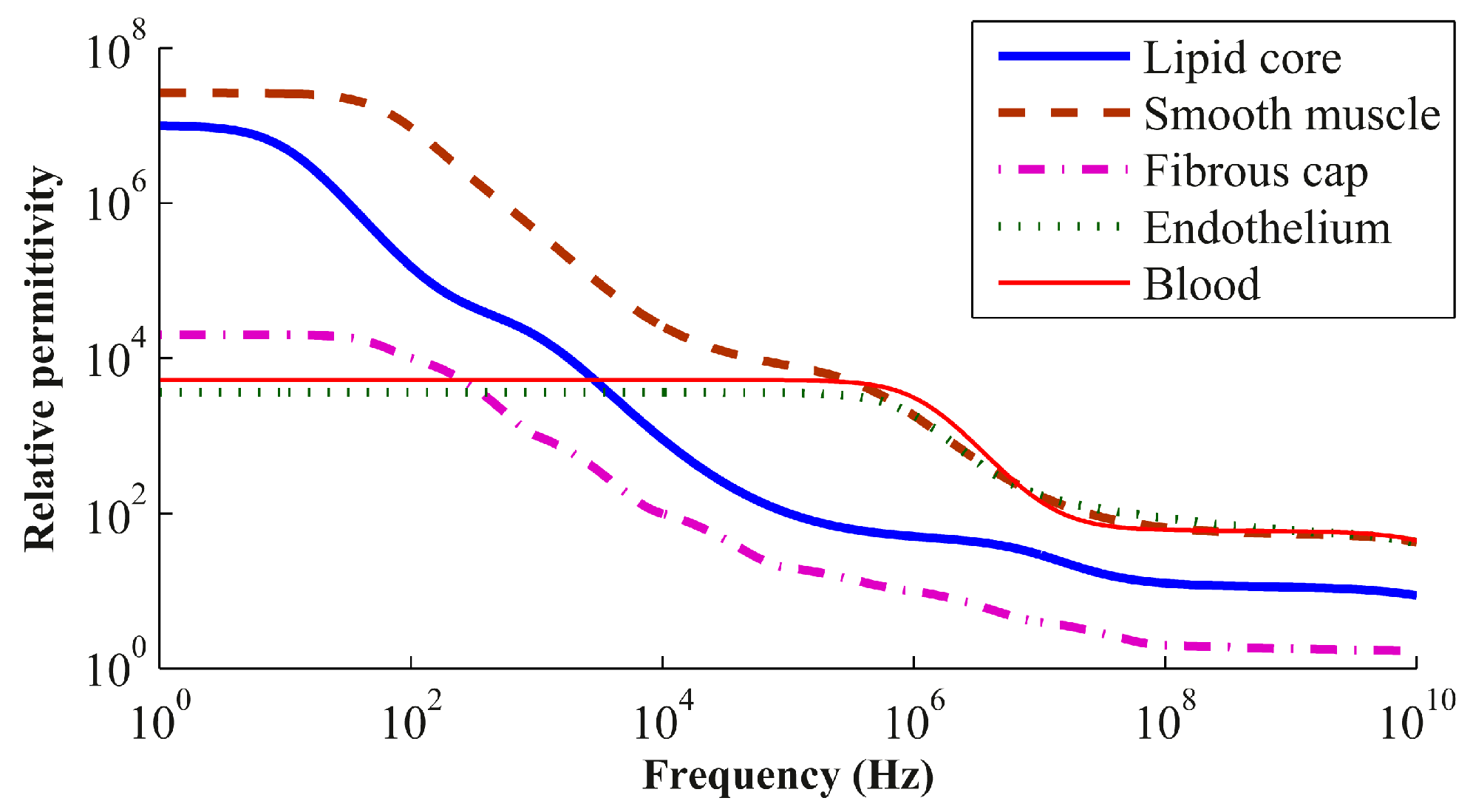
3.1. Analytical Model and 2D Finite Element Analysis Simulation Results
3.2. Generalization of the Bioimpedance Model
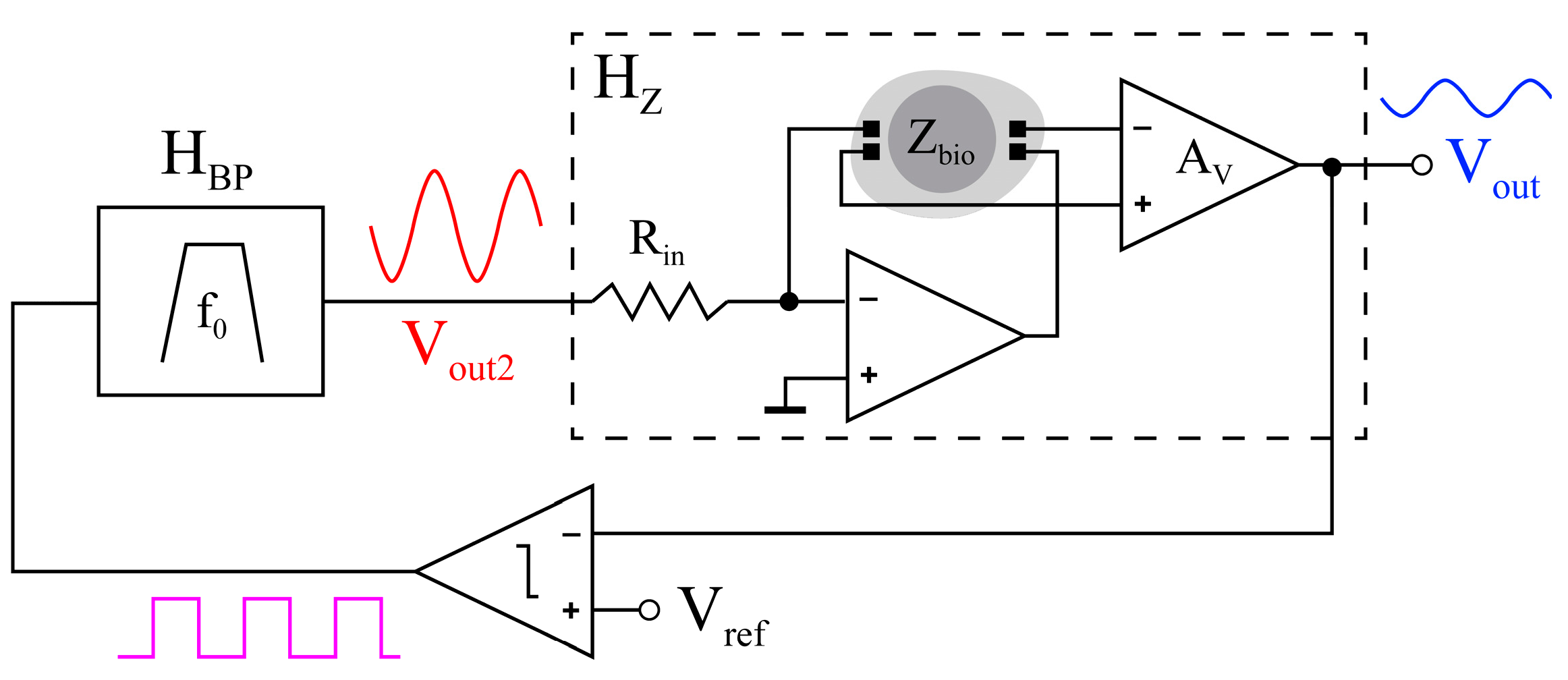
3.3. Oscillation-Based Test Auto-Calibration Circuit
4. Discussion
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Organisation for Economic Co-operation and Development (OECD)/European Union (EU). Health at a Glance: Europe 2016: State of Health in the EU Cycle; OECD Publishing: Paris, France, 2016. [Google Scholar]
- Townsend, N.; Wilson, L.; Bhatnagar, P.; Wickramasinghe, K.; Rayner, M.; Nichols, M. Cardiovascular disease in Europe: Epidemiological update. Eur. Heart J. 2016, 37, 3232–3245. [Google Scholar] [CrossRef] [PubMed]
- Chow, E.Y.; Chlebowski, A.L.; Chakraborty, S.; Chappell, W.J.; Irazoqui, P.P. Fully wireless implantable cardiovascular pressure monitor integrated with a medical stent. IEEE Trans. Biomed. Eng. 2010, 57, 1487–1496. [Google Scholar] [CrossRef] [PubMed]
- Gundert, T.J.; Marsden, A.L.; Yang, W.; Marks, D.S.; LaDisa, J.F., Jr. Identification of hemodynamically optimal coronary stent designs based on vessel caliber. IEEE Trans. Biomed. Eng. 2012, 59, 1992–2002. [Google Scholar] [CrossRef] [PubMed]
- Beier, S.; Ormiston, J.; Weister, M.; Carter, J.; Norris, S.; Medrano-Garcia, P.; Young, A.; Cowan, B. Hemodynamics in idealized stented coronary arteries: Important stent design considerations. Ann. Biomed. Eng. 2016, 44, 315–329. [Google Scholar] [CrossRef] [PubMed]
- Kokkalis, E.; Aristokleus, N.; Houston, J.G. Hemodynamics and flow modification stents for peripheral arterial disease: A review. Ann. Biomed. Eng. 2016, 44, 466–476. [Google Scholar] [CrossRef] [PubMed]
- Stone, G.W.; Ellis, S.G.; Cannon, L.; Mann, J.T.; Greenberg, J.D.; Spriggs, D.; O’Shaughnessy, C.D.; DeMaio, S.; Hall, P.; Popma, J.J.; et al. Comparison of a polymer-based paclitaxel-eluting stent with a bare metal stent in patients with complex coronary artery disease: A randomized controlled trial. J. Am. Med. Assoc. 2005, 294, 1215–1223. [Google Scholar] [CrossRef] [PubMed]
- Park, S.J.; Kang, S.J.; Virmani, R.; Nakano, M.; Ueda, Y. In-stent neoatherosclerosis: A final common pathway of late stent failure. J. Am. Coll. Cardiol. 2012, 59, 2052–2057. [Google Scholar] [CrossRef] [PubMed]
- Miguel, J.A.; Rivas-Marchena, D.; Lechuga, Y.; Allende, M.A.; Martínez, M. A novel computer-assisted design tool for implantable MEMS pressure sensors. Microprocess. Microsyst. 2016, 46, 75–83. [Google Scholar] [CrossRef]
- Rivas-Marchena, D.; Miguel, J.A.; Lechuga, Y.; Allende, M.A.; Martinez, M. Energy-efficient implantable transmitter for restenosis monitoring with intelligent-stents. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; pp. 3323–3326. [Google Scholar]
- Rivas-Marchena, D. Caracterización de Bioimpedancia para la Calibración de Sensores de Presión Capacitivos MEMS en Aplicaciones Cardiovasculares. Master’s Thesis, University of Seville, Seville, Spain, 2016. [Google Scholar]
- Süselbeck, T.; Thielecke, H.; Weinschenk, I.; Reiniger-Mack, A.; Stieglitz, T.; Metz, J.; Borggrefe, M.; Robitzki, A.; Haase, K.K. In vivo intravascular electric impedance spectroscopy using a new catheter with integrated microelectrodes. Basic Res. Cardiol. 2005, 100, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.; Patterson, R.P. A novel impedance-based tomography approach for stenotic plaque detection: A simulation study. Int. J. Cardiol. 2010, 144, 279–283. [Google Scholar] [CrossRef] [PubMed]
- Opie, N.L.; John, S.E.; Rind, G.S.; Ronayne, S.M.; Grayden, D.B.; Burkitt, A.N.; May, C.N.; O’Brien, T.J.; Oxley, T.J. Chronic impedance spectroscopy of an endovascular stent-electrode array. J. Neural Eng. 2016, 13, 046020. [Google Scholar] [CrossRef] [PubMed]
- Shedden, L.; Kennedy, S.; Wadsworth, R.; Connolly, P. Towards a self-reporting coronary artery stent—Measuring neointimal growth associated with in-stent restenosis using electrical impedance techniques. Biosens. Bioelectron. 2010, 26, 661–666. [Google Scholar] [CrossRef] [PubMed]
- Huertas, G.; Maldonado, A.; Yúfera, A.; Rueda, A.; Huertas, J.L. The bio-oscillator: A circuit for cell-culture assays. IEEE Trans. Circuits Syst. II 2015, 62, 164–168. [Google Scholar] [CrossRef]
- Schwan, H.P.; Ferris, C.D. Four-electrode null techniques for impedance measurement with high resolution. Rev. Sci. Instrum. 1968, 39, 481–485. [Google Scholar] [CrossRef]
- Grimnes, S.; Martinsen, Ø.G. Bioimpedance and Bioelectricity Basics, 3rd ed.; Elsevier: Oslo, Norway, 2014. [Google Scholar]
- Sverjensky, D.A. Interpretation and prediction of triple-layer model capacitances and the structure of the oxide-electrolyte-water interface. Geochim. Cosmochim. Acta 2001, 65, 3643–3655. [Google Scholar] [CrossRef]
- Theodor, M.; Dominic, R.; Ocker, M.; Spether, D.; Förster, K.; Heilmann, C.; Beyersdorf, F.; Manoli, Y.; Zappe, H.; Seifert, A. Implantable Impedance Plethysmography. Sensors 2014, 14, 14858–14872. [Google Scholar] [CrossRef] [PubMed]
- Ghione, G.; Goano, M. Revisiting the partial-capacitance approach to the analysis of coplanar transmission lines on multilayered substrates. IEEE Trans. Microw. Theory Tech. 2003, 51, 2007–2014. [Google Scholar] [CrossRef]
- Igreja, R.; Dias, C.J. Extension to the analytical model of the interdigital electrodes capacitance for a multi-layared structure. Sens. Actuators A Phys. 2011, 172, 392–399. [Google Scholar] [CrossRef]
- Blume, S.O.P.; Ben-Mrad, R.; Sullivan, P.E. Modelling the capacitance of multi-layer conductor-facing interdigitated electrode structures. Sens. Actuators B Chem. 2015, 213, 423–433. [Google Scholar] [CrossRef]
- MATLAB Software®, version 6.0; Mathworks Inc.: Apple Hill Drive, Natick, USA, 2000.
- Gabriel, C.; Gabriel, S. Compilation of the Dielectric Properties of Body Tissues at RF and Microwave Frequencies, 1996. Available online: http://niremf.ifac.cnr.it/docs/DIELECTRIC/Report.html (accessed on 12 July 2016).
- COMSOL Multiphysics®, version 5.2; COMSOL Inc.: Burlington, MA, USA, 2011.
- Olmo, A.; Yúfera, A. Computer simulation of microelectrode based bio-impedance measurements with COMSOL. In Proceedings of the Third International Conference on Biomedical Electronics and Devices, Valencia, Spain, 20–23 January 2010; pp. 178–182. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Series Partial Capacitance (SPC) | Parallel Partial Capacitance (PPC) |
|---|---|
| Config. | Lipid Core | Muscle | Fibrous Cap | Endothelium |
|---|---|---|---|---|
| 1 | 0 µm | 25 µm | 0 µm | 10 µm |
| 2 | 0 µm | 50 µm | 0 µm | 10 µm |
| 3 | 25 µm | 50 µm | 5 µm | 10 µm |
| 4 | 50 µm | 100 µm | 10 µm | 10 µm |
| 5 | 100 µm | 100 µm | 20 µm | 10 µm |
| 6 | 200 µm | 100 µm | 40 µm | 10 µm |
| Param. | Lipid Core (α1) | Muscle (α2) | Fibrous Cap (α3) | Independent (α4) |
|---|---|---|---|---|
| A | — | 4.60 × 10−1 | — | 1.72 × 102 |
| p1 | — | −1.17 × 10 | — | 4.52 × 102 |
| p2 | — | 2.45 × 103 | — | 1.82 × 106 |
| p3 | — | 2.56 × 106 | — | 8.59 × 108 |
| z1 | — | 2.30 × 10–1 | — | 6.28 × 102 |
| z2 | — | −9.72 × 103 | — | 4.24 × 106 |
| Param. | Lipid Core (α1) | Muscle (α2) | Fibrous Cap (α3) | Independent (α4) |
|---|---|---|---|---|
| A | 1.17 | 4.41 | 2.30 × 10−1 | 4.14 × 102 |
| p1 | −1.70 × 10−1 | −9.50 × 10−1 | −3.00 × 10−2 | 2.24 × 102 |
| p2 | 3.02 × 104 | 1.80 × 105 | 6.03 × 103 | 1.36 × 107 |
| p3 | 4.40 × 104 | 2.99 × 105 | 8.80 × 103 | 5.46 × 108 |
| z1 | −2.10 × 10−1 | −1.23 | −4.00 × 10−2 | 2.80 × 102 |
| z2 | −4.79 × 104 | 2.86 × 105 | 9.57 × 103 | 1.97 × 107 |
| Config. | Lipid Core | Muscle | Fibrous Cap | Endothelium |
|---|---|---|---|---|
| 1 | 0 µm | 25 µm | 0 µm | 10 µm |
| 2 | 0 µm | 50 µm | 0 µm | 10 µm |
| 3 | 0 µm | 100 µm | 0 µm | 10 µm |
| 4 | 0 µm | 200 µm | 0 µm | 10 µm |
| 5 | 25 µm | 50 µm | 5 µm | 10 µm |
| 6 | 100 µm | 50 µm | 20 µm | 10 µm |
| 7 | 300 µm | 50 µm | 50 µm | 10 µm |
| 8 | 50 µm | 100 µm | 10 µm | 10 µm |
| 9 | 100 µm | 100 µm | 20 µm | 10 µm |
| 10 | 200 µm | 100 µm | 40 µm | 10 µm |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rivas-Marchena, D.; Olmo, A.; Miguel, J.A.; Martínez, M.; Huertas, G.; Yúfera, A. Real-Time Electrical Bioimpedance Characterization of Neointimal Tissue for Stent Applications. Sensors 2017, 17, 1737. https://doi.org/10.3390/s17081737
Rivas-Marchena D, Olmo A, Miguel JA, Martínez M, Huertas G, Yúfera A. Real-Time Electrical Bioimpedance Characterization of Neointimal Tissue for Stent Applications. Sensors. 2017; 17(8):1737. https://doi.org/10.3390/s17081737
Chicago/Turabian StyleRivas-Marchena, David, Alberto Olmo, José A. Miguel, Mar Martínez, Gloria Huertas, and Alberto Yúfera. 2017. "Real-Time Electrical Bioimpedance Characterization of Neointimal Tissue for Stent Applications" Sensors 17, no. 8: 1737. https://doi.org/10.3390/s17081737
APA StyleRivas-Marchena, D., Olmo, A., Miguel, J. A., Martínez, M., Huertas, G., & Yúfera, A. (2017). Real-Time Electrical Bioimpedance Characterization of Neointimal Tissue for Stent Applications. Sensors, 17(8), 1737. https://doi.org/10.3390/s17081737