Proof of Concept for an Intracochlear Acoustic Receiver for Use in Acute Large Animal Experiments

 , ,
, ,  and
and 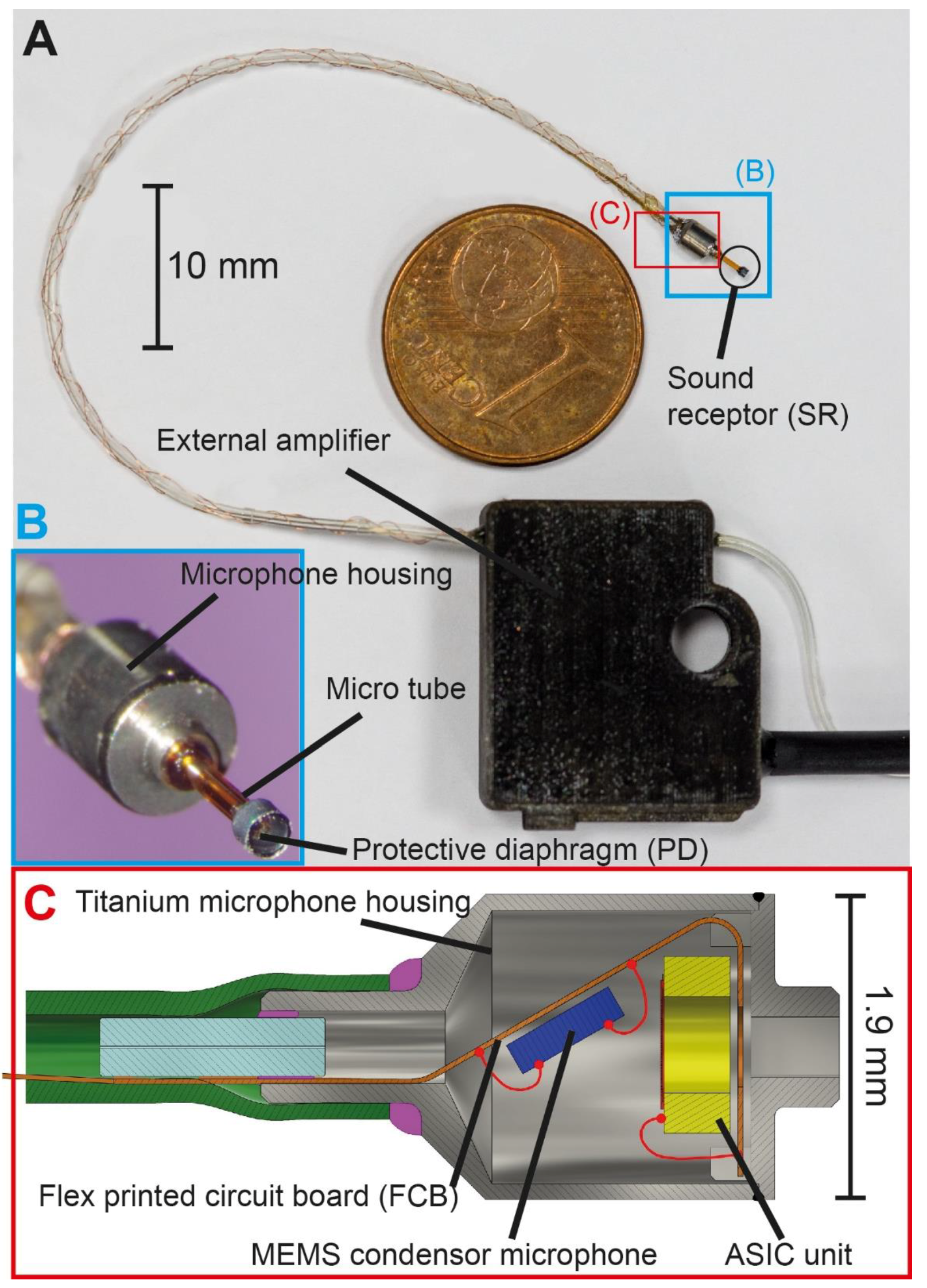{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. ICAR Requirements
2.2. Sensor Design
2.3. Sensor Parts
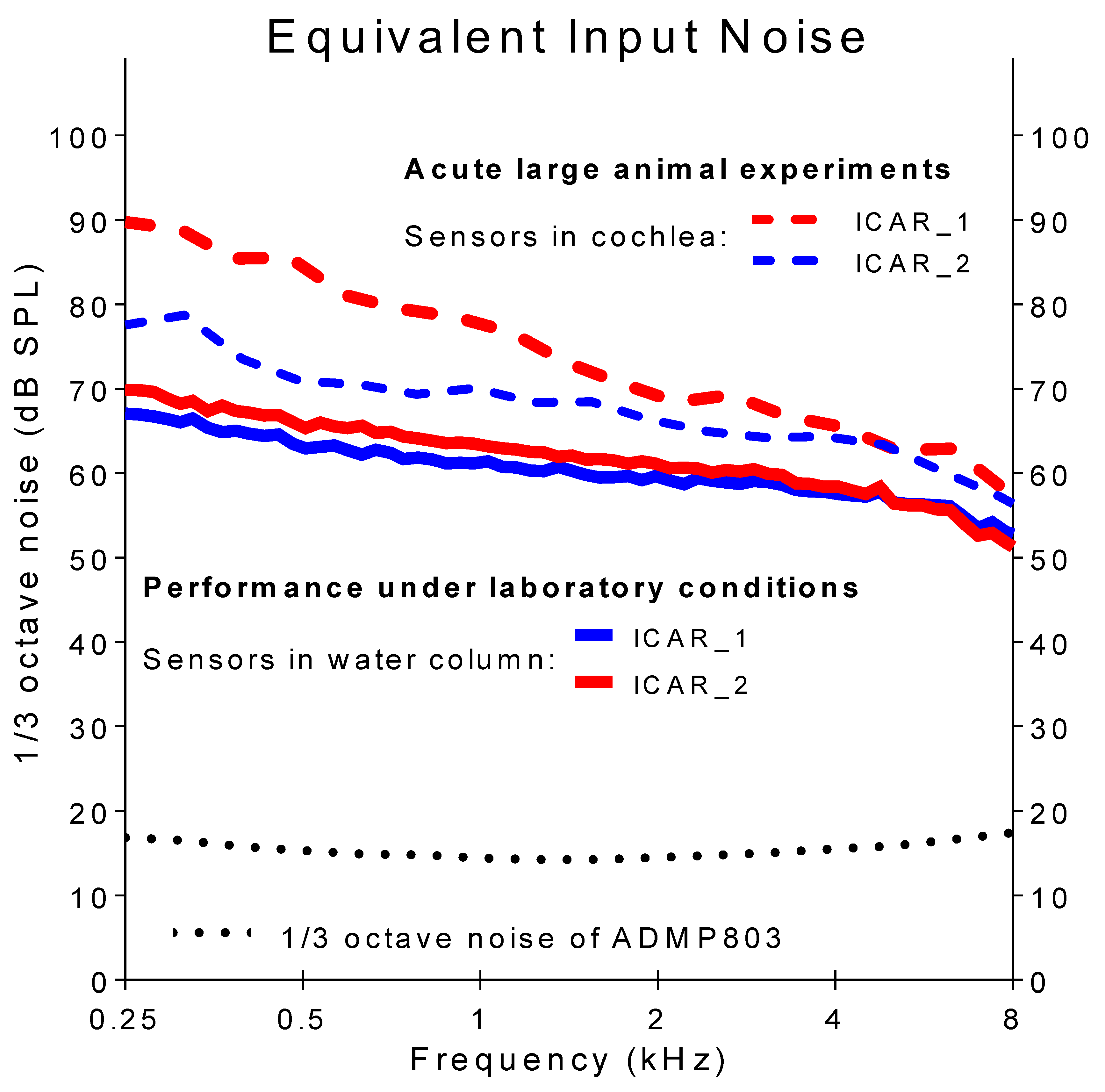
2.4. Functional Tests and Performance under Laboratory Conditions
2.5. Sensor Validation: ICAR Use in Acute Animal Experiments
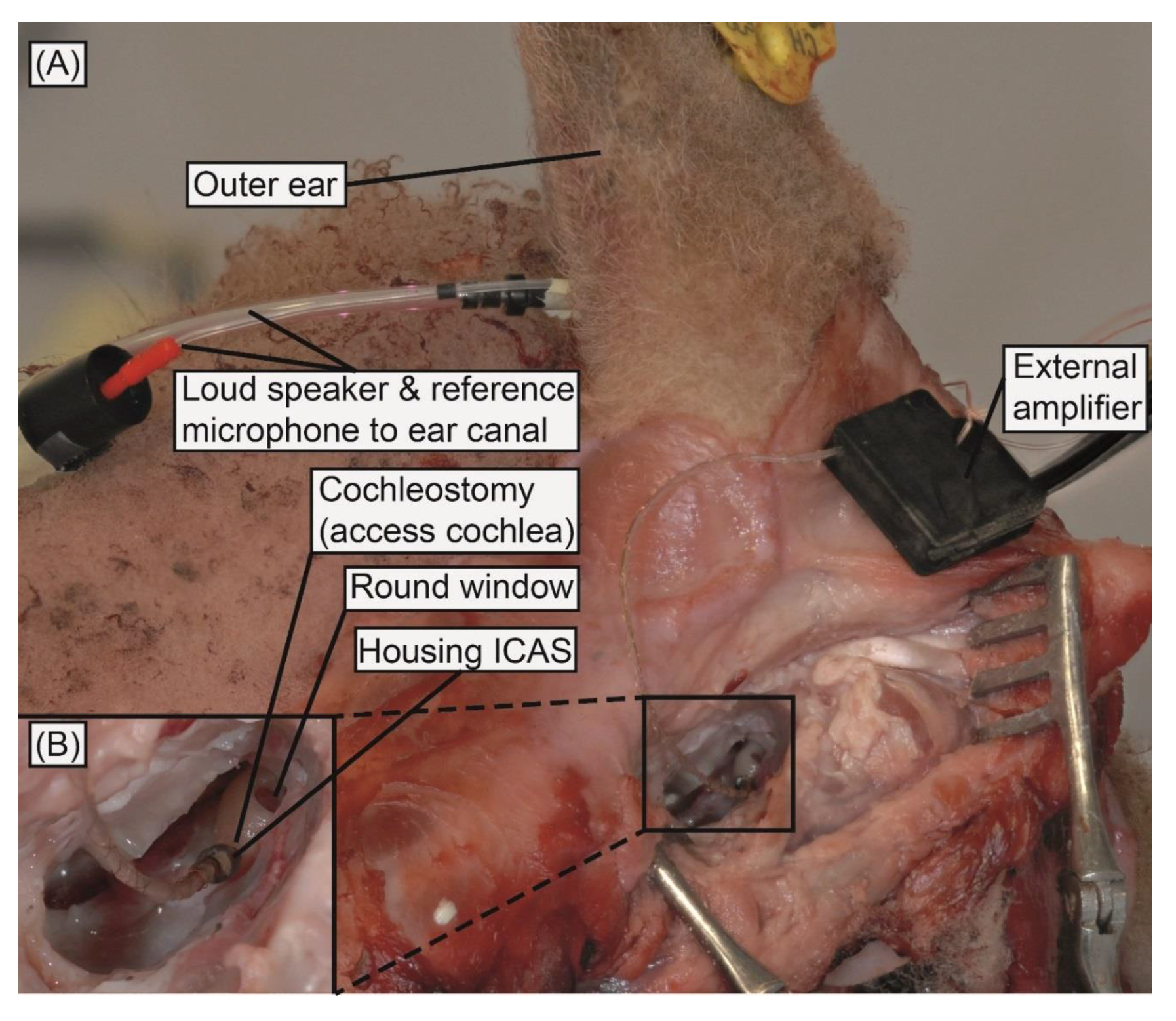
2.5.1. Surgical Approach
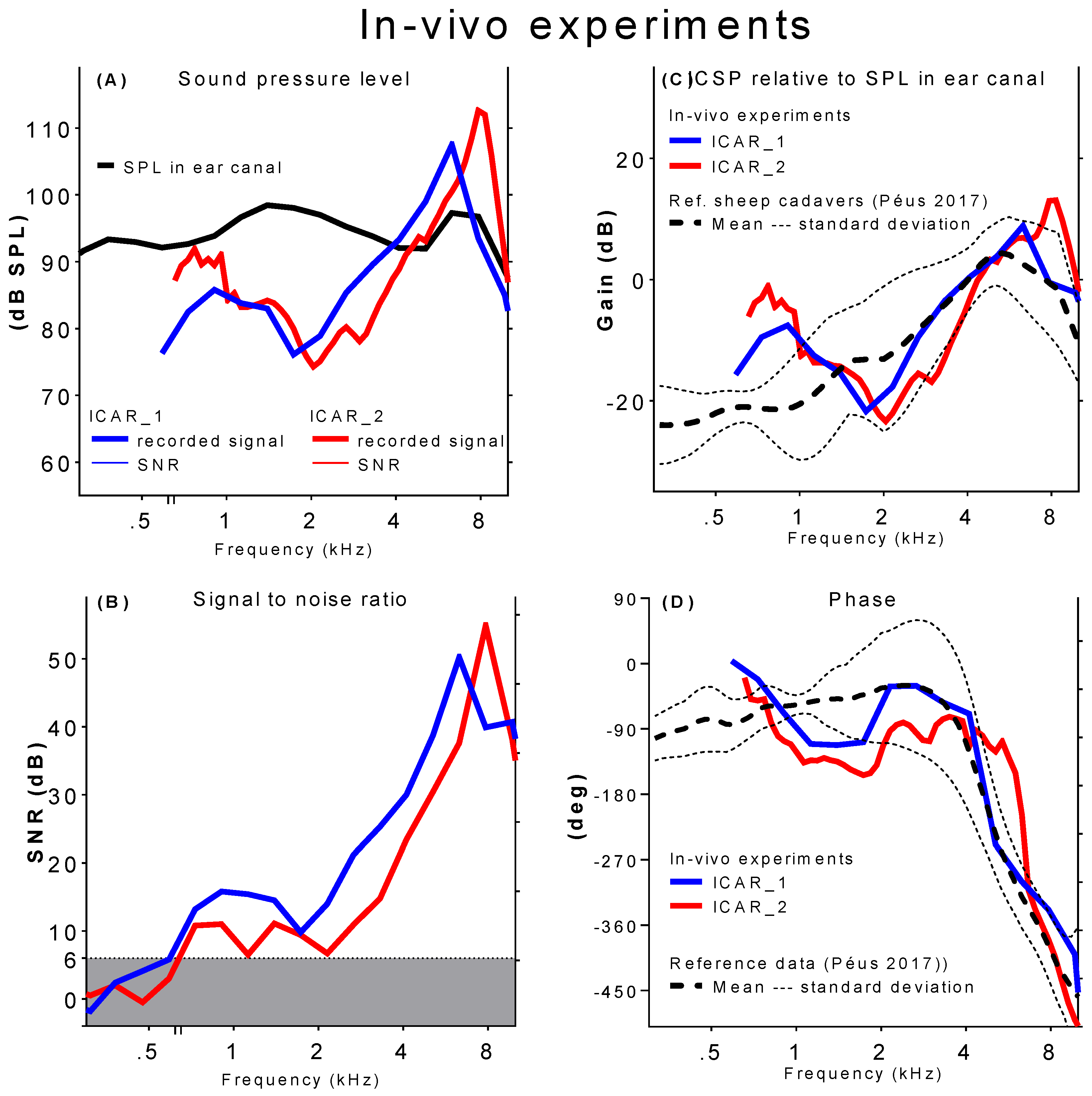
2.5.2. ICSP Measurements in Acute Animal Experiments
3. Results
3.1. Functional Tests and Performance under Laboratory Conditions
3.2. Animal Experiments
3.2.1. Surgical Approach
3.2.2. ICSP Measurements in Acute Animal Experiments
4. Discussion and Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Olson, E.S. Direct measurement of intra-cochlear pressure waves. Nature 1999, 402, 526–529. [Google Scholar] [CrossRef] [PubMed]
- Nakajima, H.H.; Dong, W.; Olson, E.S.; Merchant, S.N.; Ravicz, M.E.; Rosowski, J.J. Differential intracochlear sound pressure measurements in normal human temporal bones. J. Assoc. Res. Otolaryngol. 2009, 10, 23–36. [Google Scholar] [CrossRef] [PubMed]
- Grossohmichen, M.; Salcher, R.; Puschel, K.; Lenarz, T.; Maier, H. Differential intracochlear sound pressure measurements in human temporal bones with an off-the-shelf sensor. BioMed Res. Int. 2016, 2016, 6059479. [Google Scholar] [CrossRef] [PubMed]
- Nedzelnitsky, V. Measurements of sound pressure in the cochleae of anesthetized cats. In Facts and Models in Hearing, Proceedings of the Symposium on Psychophysical Models and Physiological Facts in Hearing, Tutzing, Germany, 22–26 April 1974; Zwicker, E., Terhardt, E., Eds.; Springer: Berlin/Heidelberg, Germany, 1974; pp. 45–53. [Google Scholar]
- Dancer, A.; Franke, R. Intracochlear sound pressure measurements in guinea pigs. Hear. Res. 1980, 2, 191–205. [Google Scholar] [CrossRef]
- Pfiffner, F.; Prochazka, L.; Peus, D.; Dobrev, I.; Dalbert, A.; Sim, J.H.; Kesterke, R.; Walraevens, J.; Harris, F.; Roosli, C.; et al. A mems condenser microphone-based intracochlear acoustic receiver. IEEE Trans. Bio-Med. Eng. 2017, 64, 2431–2438. [Google Scholar] [CrossRef] [PubMed]
- Puria, S.; Peake, W.T.; Rosowski, J.J. Sound-pressure measurements in the cochlear vestibule of human-cadaver ears. J. Acoust. Soc. Am. 1997, 101, 2754–2770. [Google Scholar] [CrossRef] [PubMed]
- Nagahara, K.; Fisch, U.; Dillier, N. Experimental study on the perilymphatic pressure. Am. J. Otol. 1981, 3, 1–8. [Google Scholar] [PubMed]
- Zwislocki, J.; Feldman, A.S. Post-mortem acoustic impedance of human ears. J. Acoust. Soc. Am. 1963, 35, 104–107. [Google Scholar] [CrossRef]
- Brenkman, C.J.; Grote, J.J.; Rutten, W.L.C. Acoustic transfer characteristics in human middle ears studied by a squid magnetometer method. J. Acoust. Soc. Am. 1987, 82, 1646–1654. [Google Scholar] [CrossRef] [PubMed]
- Ravicz, M.E.; Merchant, S.N.; Rosowski, J.J. Effect of freezing and thawing on stapes-cochlear input impedance in human temporal bones. Hear. Res. 2000, 150, 215–224. [Google Scholar] [CrossRef]
- Nedzelnitsky, V. Sound pressures in the basal turn of the cat cochlea. J. Acoust. Soc. Am. 1980, 68, 1676–1689. [Google Scholar] [CrossRef] [PubMed]
- Magnan, P.; Avan, P.; Dancer, A.; Smurzynski, J.; Probst, R. Reverse middle-ear transfer function in the guinea pig measured with cubic difference tones. Hear. Res. 1997, 107, 41–45. [Google Scholar] [CrossRef]
- Chhan, D.; Roosli, C.; McKinnon, M.L.; Rosowski, J.J. Evidence of inner ear contribution in bone conduction in chinchilla. Hear. Res. 2013, 301, 66–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mantokoudis, G.; Huth, M.E.; Weisstanner, C.; Friedrich, H.M.; Nauer, C.; Candreia, C.; Caversaccio, M.D.; Senn, P. Lamb temporal bone as a surgical training model of round window cochlear implant electrode insertion. Otol. Neurotol. 2016, 37, 52–56. [Google Scholar] [CrossRef] [PubMed]
- Schnabl, J.; Glueckert, R.; Feuchtner, G.; Recheis, W.; Potrusil, T.; Kuhn, V.; Wolf-Magele, A.; Riechelmann, H.; Sprinzl, G.M. Sheep as a large animal model for middle and inner ear implantable hearing devices: A feasibility study in cadavers. Otol. Neurotol. 2012, 33, 481–489. [Google Scholar] [CrossRef] [PubMed]
- Djinovic, Z.; Pavelka, R.; Tomic, M.; Sprinzl, G.; Plenk, H.; Losert, U.; Bergmeister, H.; Plasenzotti, R. In-vitro and in-vivo measurement of the animal’s middle ear acoustical response by partially implantable fiber-optic sensing system. Biosens. Bioelectron. 2018, 103, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Peus, D.; Dobrev, I.; Prochazka, L.; Thoele, K.; Dalbert, A.; Boss, A.; Newcomb, N.; Probst, R.; Roosli, C.; Sim, J.H.; et al. Sheep as a large animal ear model: Middle-ear ossicular velocities and intracochlear sound pressure. Hear. Res. 2017, 351, 88–97. [Google Scholar] [CrossRef] [PubMed]
- Walraevens, J.; Wiskerke, P.; Paris, F.; Huber, A.; Prochazka, L.; Obrist, D. Cochlear Implant Electrode Array Including Receptor and Sensor. WO2015068136 A1, 15 May 2015. [Google Scholar]
- Seibel, V.A.; Lavinsky, L.; De Oliveira, J.A. Morphometric study of the external and middle ear anatomy in sheep: A possible model for ear experiments. Clin. Anat. 2006, 19, 503–509. [Google Scholar] [CrossRef] [PubMed]
- Seibel, V.A.; Lavinsky, L.; Irion, K. Ct-scan sheep and human inner ear morphometric comparison. Braz. J. Otorhinolaryngol. 2006, 72, 370–376. [Google Scholar] [CrossRef]
- Schloss, F.; Strasberg, M. Hydrophone calibration in a vibrating column of liquid. J. Acoust. Soc. Am. 1962, 34, 958–959. [Google Scholar] [CrossRef]




© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pfiffner, F.; Prochazka, L.; Dobrev, I.; Klein, K.; Sulser, P.; Péus, D.; Sim, J.H.; Dalbert, A.; Röösli, C.; Obrist, D.; et al. Proof of Concept for an Intracochlear Acoustic Receiver for Use in Acute Large Animal Experiments. Sensors 2018, 18, 3565. https://doi.org/10.3390/s18103565
Pfiffner F, Prochazka L, Dobrev I, Klein K, Sulser P, Péus D, Sim JH, Dalbert A, Röösli C, Obrist D, et al. Proof of Concept for an Intracochlear Acoustic Receiver for Use in Acute Large Animal Experiments. Sensors. 2018; 18(10):3565. https://doi.org/10.3390/s18103565
Chicago/Turabian StylePfiffner, Flurin, Lukas Prochazka, Ivo Dobrev, Karina Klein, Patrizia Sulser, Dominik Péus, Jae Hoon Sim, Adrian Dalbert, Christof Röösli, Dominik Obrist, and et al. 2018. "Proof of Concept for an Intracochlear Acoustic Receiver for Use in Acute Large Animal Experiments" Sensors 18, no. 10: 3565. https://doi.org/10.3390/s18103565
APA StylePfiffner, F., Prochazka, L., Dobrev, I., Klein, K., Sulser, P., Péus, D., Sim, J. H., Dalbert, A., Röösli, C., Obrist, D., & Huber, A. (2018). Proof of Concept for an Intracochlear Acoustic Receiver for Use in Acute Large Animal Experiments. Sensors, 18(10), 3565. https://doi.org/10.3390/s18103565