Breast Cancer Detection Using Infrared Thermal Imaging and a Deep Learning Model




Abstract
:1. Introduction
- To give a clear picture of breast cancer detection using infrared images.
- To propose a model powerful enough to help in the early detection of breast cancer.
2. Previous Techniques and Comments
2.1. Related Studies
2.2. Economic Aspects of Breast Cancer
3. Discussion of Related Work
4. Proposed Model
- Total number of subjects (N) = 67.
- Total number of healthy/normal subjects (NH) = 43.
- Total number of sick/abnormal subjects (NS) = 24.
4.1. Why a New Model?
- A second well known classifier (SVM) is coupled to that, and is involved only in the case of an uncertainty in the output of the DNN.
4.2. Pre-Processing of Breast Thermal Images:
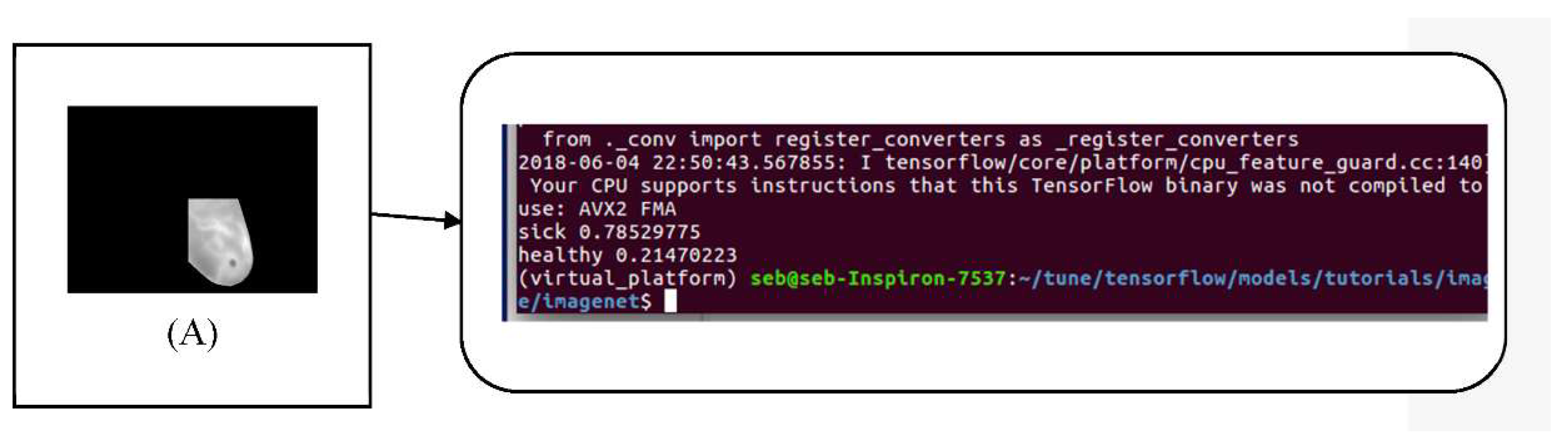
- Pre-treatment of the breast thermal images: We chose to use a well-known dataset [7]. The thermal images of this dataset were obtained by following a dynamic protocol, which consists of taking picture after the cooling of breasts by air stream. During the process of returning the patient’s body to thermal equilibrium with the environment, the author of the dataset obtained 20 sequential images with intervals of 15 s between them. The images in their original input format (640 × 480) are very large for our DNN, so it is important to crop them to remove unwanted areas.
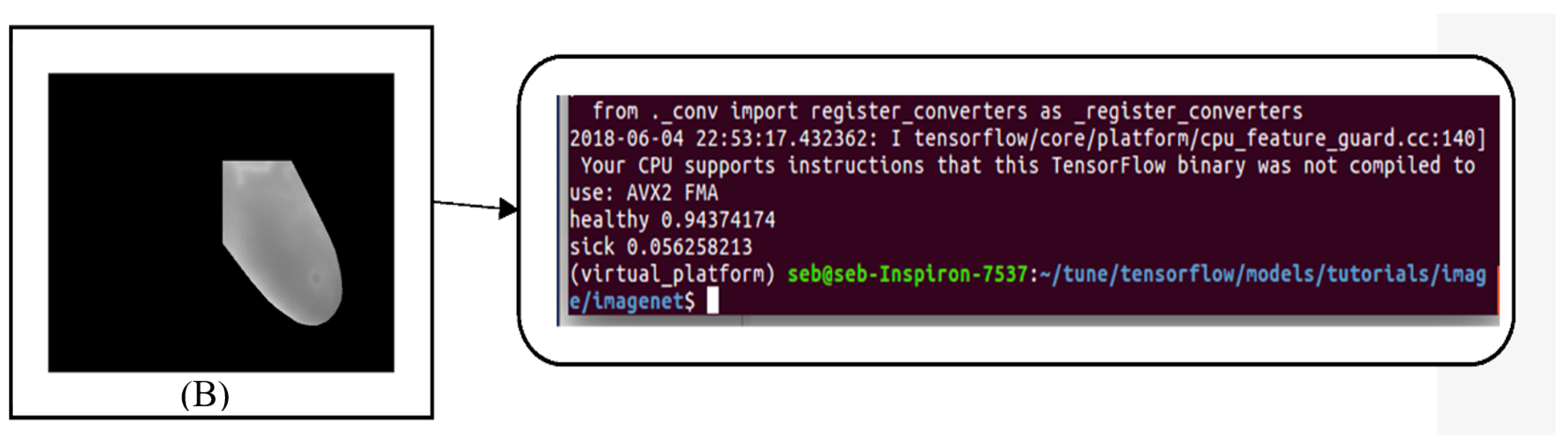
- Obtaining the Region of Interest: From each grey scale image, the Region of Interest (ROI) was extracted. Each ROI image is converted into a matrix of characteristics that will be processed, and the areas most likely to have cancer will be transferred to the input of the next component.
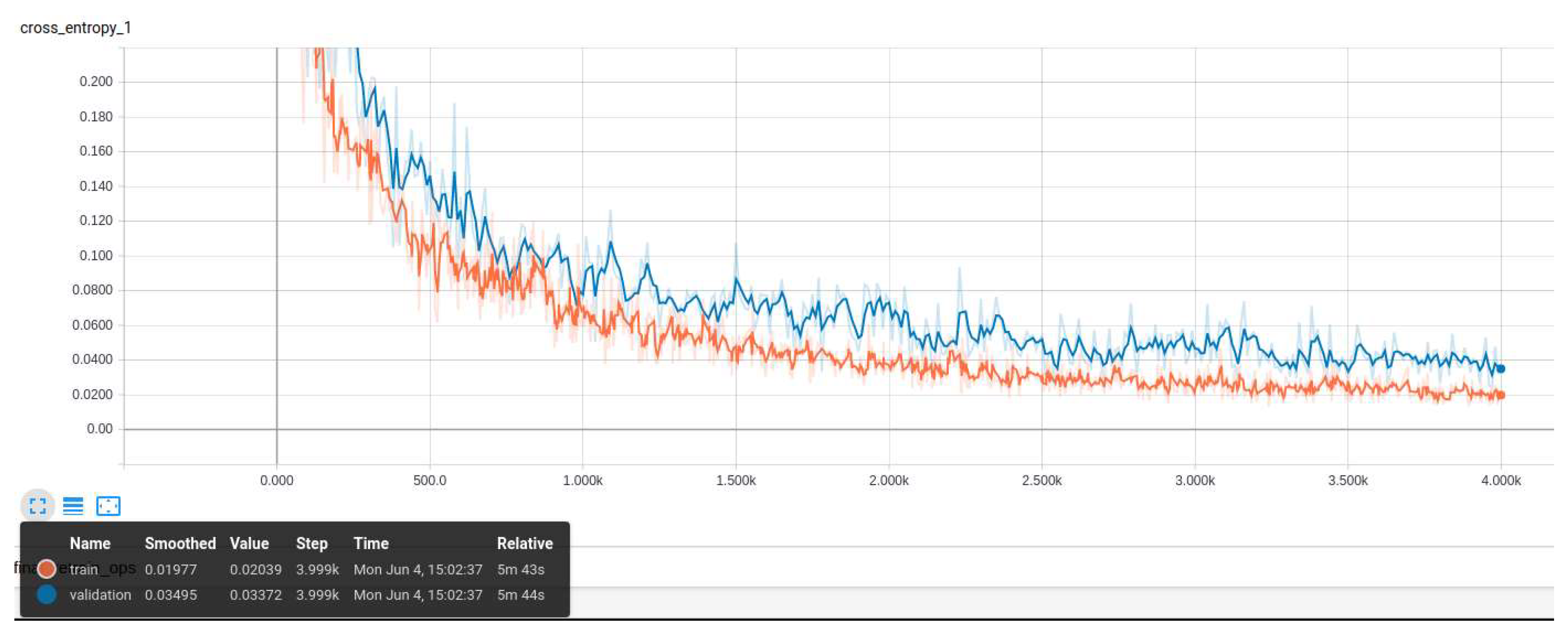
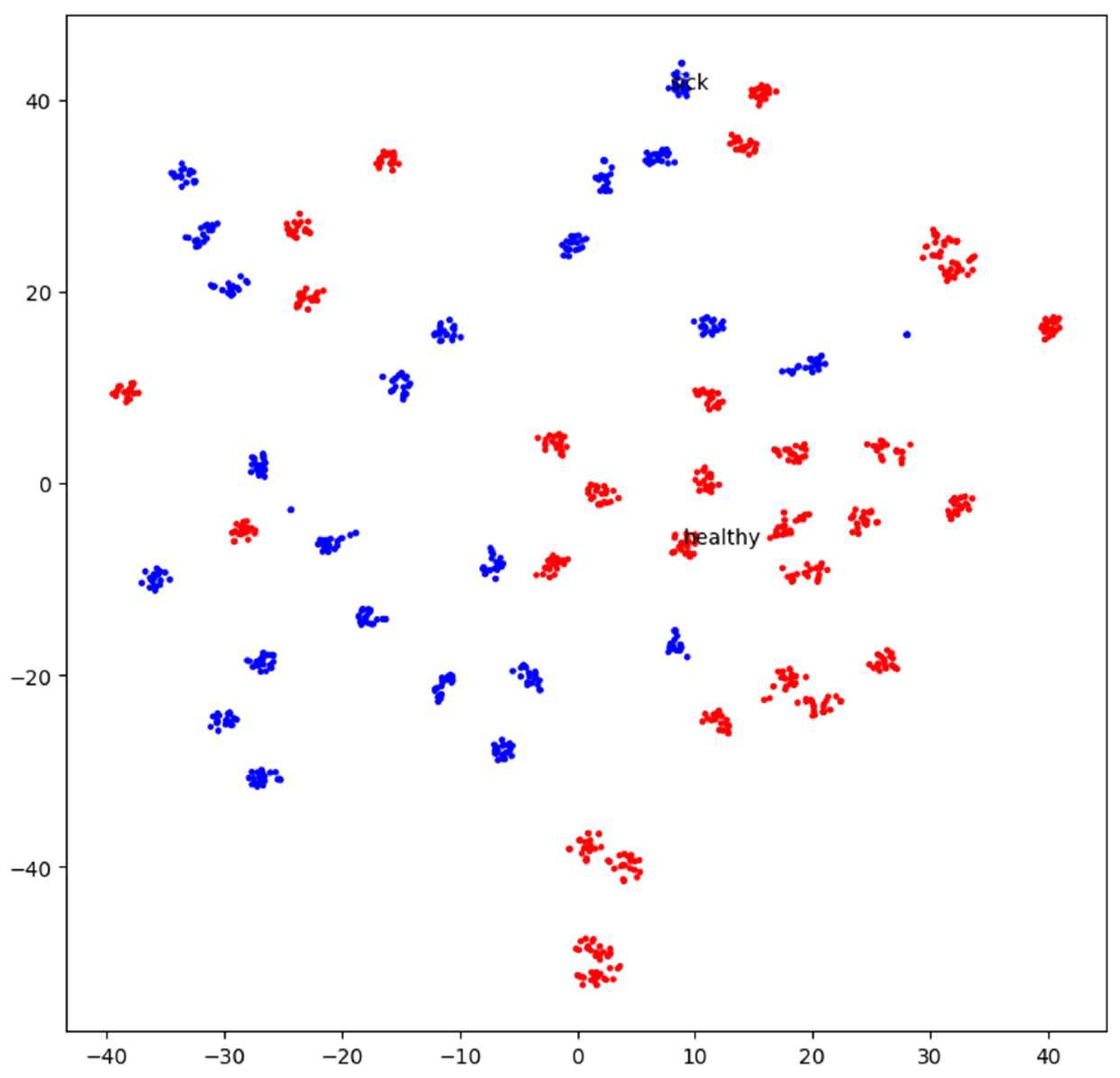
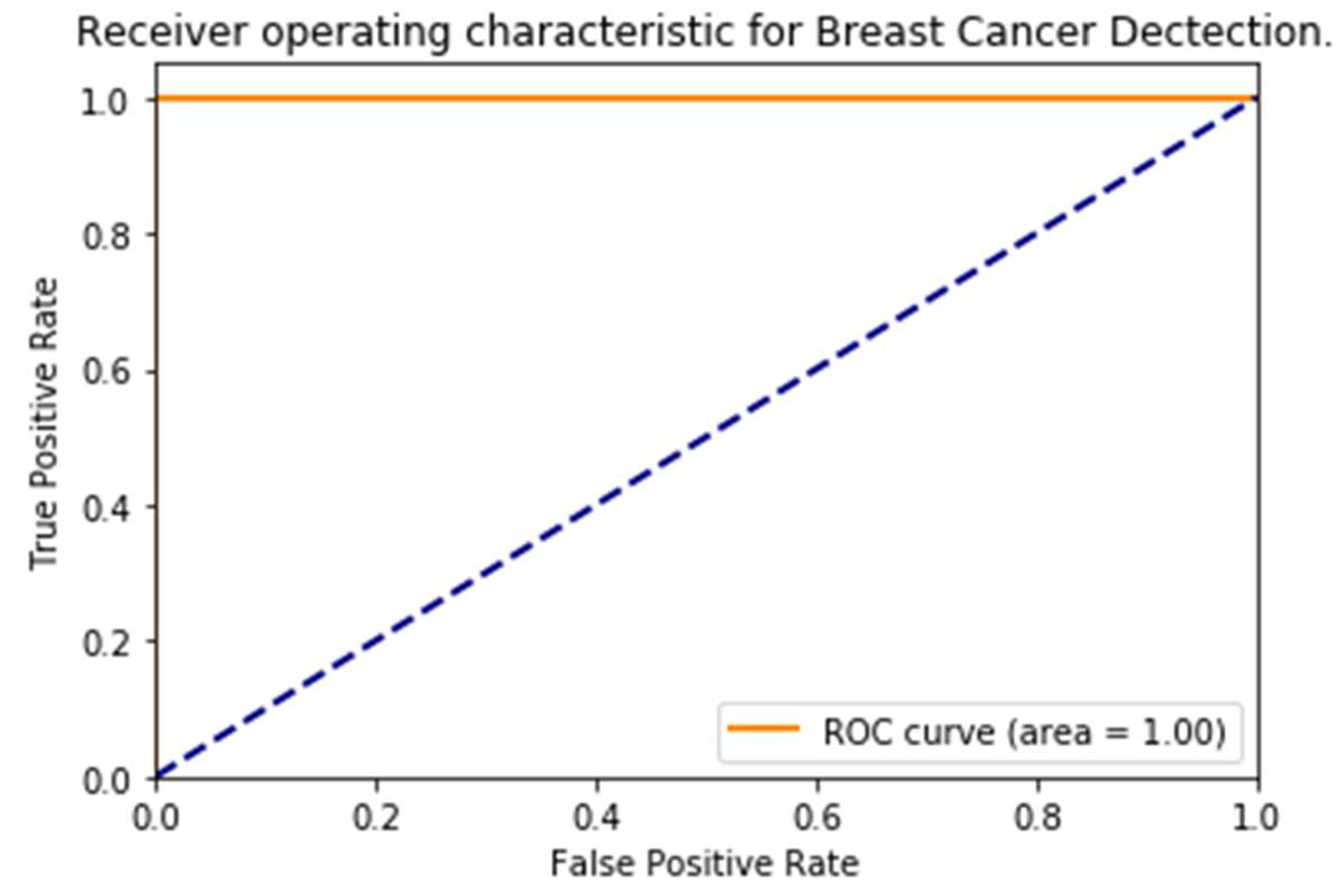
4.3. Image Classification Framework
4.4. Results
5. Conclusions
Funding
Conflicts of Interest
References
- National Breast Cancer Foundation. Breast Cancer Facts; National Breast Cancer Foundation: Sydney, Australia, 2016. [Google Scholar]
- Dongola, N. Mammography in Breast Cancer. Available online: https://emedicine.medscape.com/article/346529-overview (accessed on 24 August 2018).
- Hamidinekoo, A.; Denton, E.; Rampun, A.; Honnor, K.; Zwiggelaar, R. Deep learning in mammography and breast histology, an overview and future trends. Med. Image Anal. 2018, 47, 45–67. [Google Scholar] [CrossRef] [PubMed]
- Kosus, N.; Kosus, A.; Duran, M.; Simavlı, S.; Turhan, N. Comparison of standard mammography with Digital mammography and Digital infrared thermal imaging for breast cancer screening. J. Turk. Ger. Gynecol. Assoc. 2010, 11, 152–157. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Weng, J.; Shi, Y.; Gu, W.; Mao, Y.; Wang, Y.; Liu, W.; Zhang, J. An improved deep learning approach for detection of thyroid papillary cancer in ultrasound images. Sci. Rep. 2018, 8. [Google Scholar] [CrossRef]
- Dezs, R.; Anna, H.; Zsuzsa, U.; Peter, P.; Istvan, C. Detecting and classifying lesions in mammograms with Deep Learning. Sci. Rep. 2018, 8, 4165. [Google Scholar] [CrossRef]
- Visual Lab. A Methodology for Breast Disease Computer-Aided Diagnosis using dynamic thermography. Available online: http://visual.ic.uff.br/en/proeng/thiagoelias/ (accessed on 24 August 2018).
- Alireza, O.; Bita, S. Machine Learning Techniques to Diagnose BreastCancer. In Proceedings of the 2010 5th International Symposium on Health Informatics and Bioinformatics, Antalya, Turkey, 20–22 April 2010. [Google Scholar] [CrossRef]
- Saira, C.; Muhammad, K.; Khurram, K. Breast Cancer Detection in Mammograms using Convolutional Neural Network. In Proceedings of the 2018 International Conference on Computing, Mathematics and Engineering Technologies (iCoMET), Sukkur, Pakistan, 3–4 March 2018; pp. 1–5. [Google Scholar]
- Adriel, A.; Aura, C.; Roger, R.; Anselmo, M.; Claudineia, A. Computer Aided Diagnosis for Breast Diseases Based on Infrared Images. In Proceedings of the 2017 IEEE/ACS 14th International Conference on Computer Systems and Applications (AICCSA), Hammamet, Tunisia, 30 October–3 November 2017; pp. 172–177. [Google Scholar]
- Vijaya, M.; Christy, B. Thermal imaging based breast cancer analysis using BEMD and uniform RLBP. In Proceedings of the 2017 Third International Conference on Biosignals, Images and Instrumentation (ICBSII), Chennai, India, 16–18 March 2017; pp. 1–6. [Google Scholar]
- Dina, A.; Sheida, N.; Reda, A.; Clifford, Y. Survey on deep convolutional neural networks in mammography. In Proceedings of the 2017 IEEE 7th International Conference on Computational Advances in Bio and Medical Sciences (ICCABS), Orlando, FL, USA, 19–21 October 2017. [Google Scholar]
- Litjens, G.; Kooi, T.; Bejnordi, B.E.; Setio, A.A.A.; Ciompi, F.; Ghafoorian, M.; van der Laak, J.A.W.M.; van Ginneken, B.; Sánchez, C.I. A Survey on Deep Learning in Medical Image Analysis. Med. Image Anal. 2017, 42, 60–88. [Google Scholar] [CrossRef] [PubMed]
- Rampun, A.; Scotney, B.W.; Morrow, P.J.; Wang, H. Breast Density Classification Using Local Quinary Patterns with Various Neighbourhood Topologies. J. Imaging 2018, 4, 14. [Google Scholar] [CrossRef]
- Li, S.; Johnson, J.; Peck, A.; Xie, Q. Near infrared fluorescent imaging of brain tumor with IR780 dye incorporated phospholipid nanoparticles. J. Transl. Med. 2017, 15. [Google Scholar] [CrossRef] [PubMed]
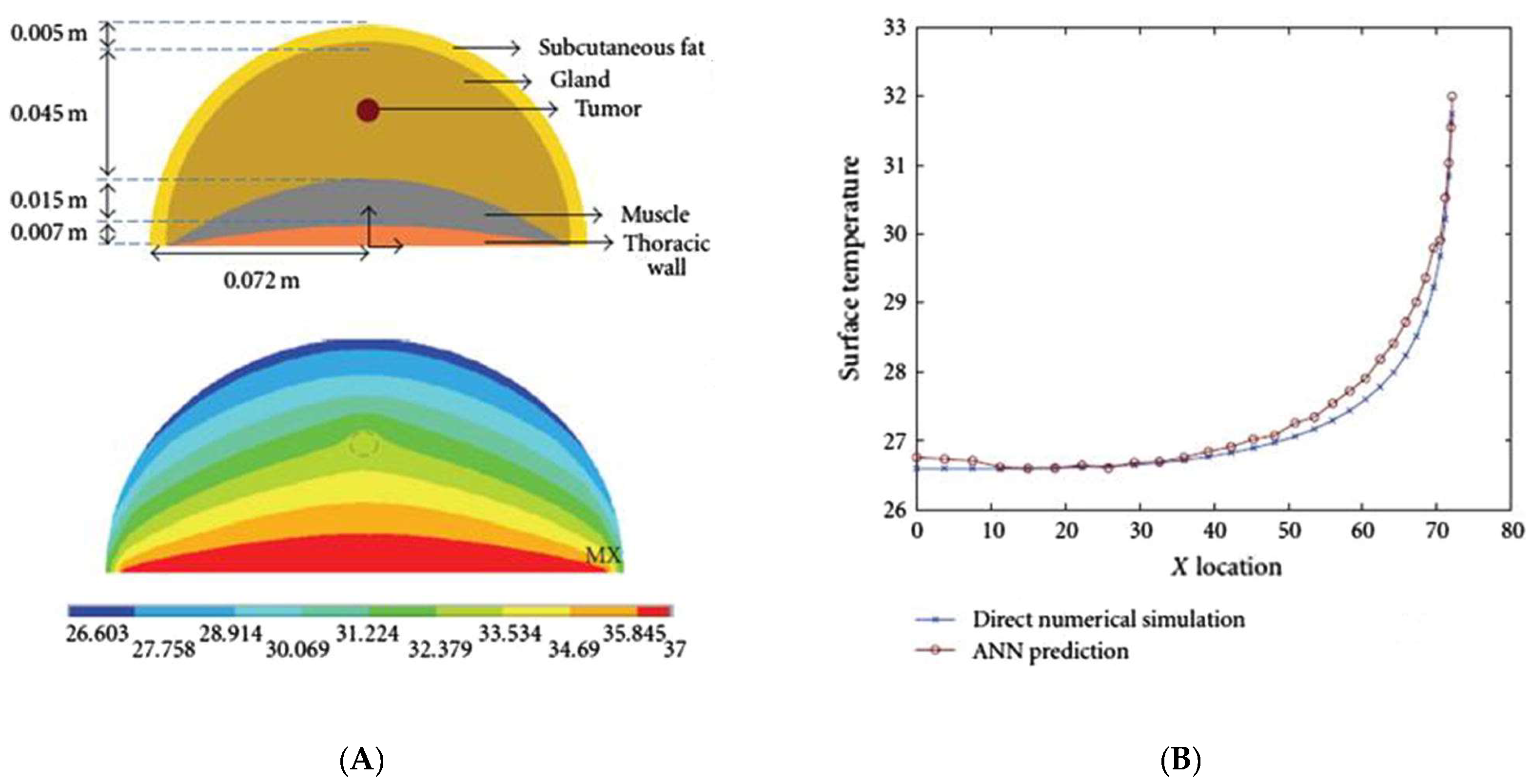
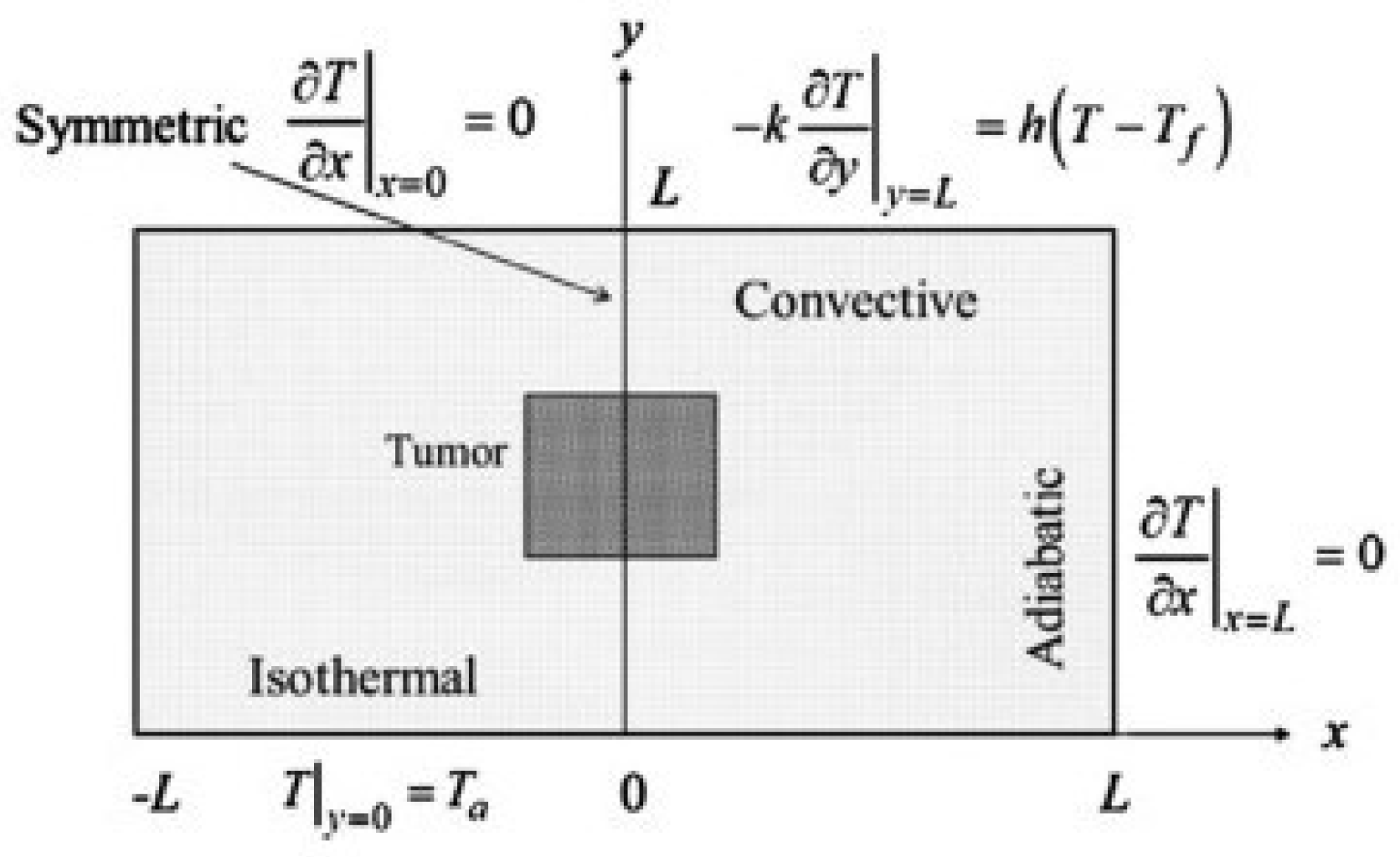
- Amria, A.; Pulko, S.H.; Wilk, A.J. Potentialities of steady-state and transient thermography in breast tumour depth detection: A numerical study. Comput. Methods Progr. Biomed. 2016, 123, 68–80. [Google Scholar] [CrossRef] [PubMed]
- Boogerd, L.S.; Handgraaf, H.J.; Lam, H.D.; Huurman, V.A.; FarinaSarasqueta, A.; Frangioni, J.V.; van de Velde, C.J.; Braat, A.E.; Vahrmeijer, A.L. Laparoscopic detection and resection of occult liver tumors of multiple cancer types using real-time near-infrared fluorescence guidance. Surg. Endosc. 2017, 31, 952–961. [Google Scholar] [CrossRef] [PubMed]
- Kandlikar, S.G.; Perez-Raya, I.; Raghupathi, P.A.; Gonzalez-Hernandez, J.L.; Dabydeen, D.; Medeiros, L.; Phatak, P. Infrared imaging technology for breast cancer detection—Current status, protocols and new directions. Int. J. Heat Mass Transf. 2017, 108, 2303–2320. [Google Scholar] [CrossRef]
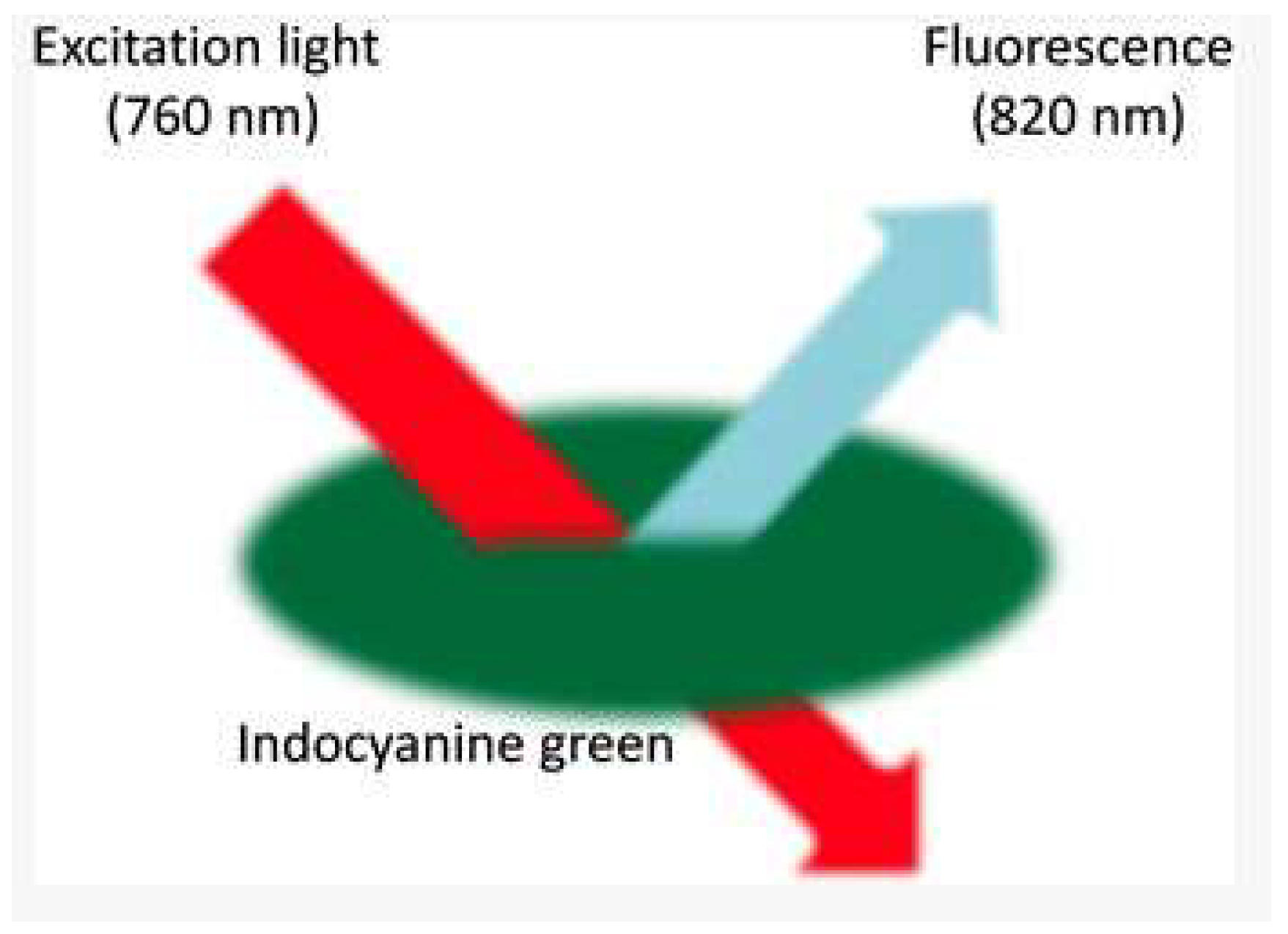
- Namikawa, T.; Sato, T.; Hanazaki, K. Recent advances in near-infrared fluorescence-guided imaging surgery using indocyanine green. Surg. Today 2015, 45, 1467–1474. [Google Scholar] [CrossRef] [PubMed]
- Kontos, M.; Wilson, R.; Fentiman, I. Digital infrared thermal imaging (DITI) of breast lesions: Sensitivity and specificity of detection of primary breast cancers. Clin. Radiol. 2011, 66, 536–539. [Google Scholar] [CrossRef] [PubMed]
- Mambou, S.; Maresova, P.; Krejcar, O.; Selamat, A.; Kuca, K. Breast Cancer Detection Using Modern Visual IT Techniques. In Modern Approaches for Intelligent Information and Database Systems; Andrzej, S., Adrianna, K., Manuel, N., Quang Thuy, H., Eds.; Springer: Berlin, Germany, 2018; Volume 769, pp. 397–407. [Google Scholar]
- Kandlikar, S.G.; Perez-Raya, I.; Raghupathi, P.A.; Gonzalez-Hernandez, J.L.; Dabydeen, D.; Medeiros, L.; Phatak, P. Infrared imaging technology for breast cancer detection—Current status, protocols and new directions. Int. J. Heat Mass Transf. 2017, 108, 2303–2320. [Google Scholar] [CrossRef]
- Czech Society for Oncology. National Oncology Program. Available online: https://www.linkos.cz/narodni-onkologicky-program/ (accessed on 24 August 2018).
- Unar-Mungu´ıa, M.; Meza, R.; Colchero, M.A.; Torres-Mejía, G.; de Cosío, T.G. Economic and disease burden of breast cancer associated with suboptimal breastfeeding practices in Mexico. Cancer Causes Control 2017, 28, 1381–1391. [Google Scholar] [CrossRef] [PubMed]
- Boquete, L.; Ortega, S.; Miguel-Jimenez, J.M.; Rodrıguez-Ascariz, J.M.; Blanco, R. Automated Detection of Breast Cancer in Thermal Infrared Images, Based on Independent Component Analysis. J. Med. Syst. 2012, 36, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Kubicek, J.; Bryjova, I.; Faltynova, K.; Penhaker, M.; Augustynek, M.; Maresova, P. Evaluation of Gama Analysis Results Significance within Verification of Radiation IMRT Plans in Radiotherapy. In Proceedings of the Conference on Computational Collective Intelligence Technologies and Applications, Nicosia, Cyprus, 27 September 2017; pp. 541–548. [Google Scholar] [CrossRef]
- Augustynek, M.; Korpas, D.; Penhaker, M.; Cvek, J.; Binarova, A. Monitoring of CRT-D devices during radiation therapy in vitro. Biomed. Eng. Online 2016, 15. [Google Scholar] [CrossRef] [PubMed]
- Yszczarz, B.L.; Nojszewska, E. Productivity losses and public finance burden attributable to breast cancer in Poland, 2010–2014. BMC Cancer 2017, 17. [Google Scholar] [CrossRef] [Green Version]
- Nitori, N.; Deguchi, T.; Kubota, K.; Yoshida, M.; Kato, A.; Kojima, M.; Kadomura, T.; Okada, A.; Okamura, J.; Kobayashi, M.; et al. Successful treatment of non-occlusive mesenteric ischemia (NOMI) using the HyperEye Medical System for intraoperative visualization of the mesenteric and bowel circulation: Report of a case. Surg Today. 2014, 44, 359–362. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, F.; Harbeck, N.; Barrios, C.H.; Bergh, J.; Cortés, J.; El Saghir, N.; Francis, P.A.; Hudis, C.A.; Ohno, S.; Partridge, A.H.; et al. Research needs in breast cancer. Ann. Oncol. 2016, 28, 208–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Šmídová, I. Alcohol and Breast Cancer-Economic Costs. Hygiena 2012, 51, 17–21. [Google Scholar]
- Gustavsen, G.; Schroeder, B.; Kennedy, P.; Pothier, K.C.; Erlander, M.G.; Schnabel, C.A.; Ali, H. Health economic analysis of Breast Cancer Index in patients with ER+, LN-breast cancer. Am. J. Manag. Care 2014, 20, e302-10. [Google Scholar] [PubMed]
- IMS Institute for Healthcare Informatics. Global Oncology Trend Report: A Review of 2015 and Outlook to 2020. Available online: https://morningconsult.com/wp-content/uploads/2016/06/IMS-Institute-Global-Oncology-Report-05.31.16.pdf (accessed on 24 August 2018).
- Kim, Y.A.; Oh, I.H.; Yoon, S.J.; Kim, H.J.; Seo, H.Y.; Kim, E.J.; Lee, Y.H.; Jung, J.H. The Economic Burden of Breast Cancer in Korea from 2007–2010. Cancer Res. Treat. 2015, 47, 583–590. [Google Scholar] [CrossRef] [PubMed]
- Angel, C.; Hannah, G.; Ajay, B.; Michael, F.; Shridar, G.; Natalie, N.C.; John, L.; Anant, M. Accurate and reproducible invasive breast cancer detection in wholeslide images: A Deep Learning approach for quantifying tumor extent. Sci. Rep. 2017, 7. [Google Scholar] [CrossRef]
- Guo, Y.; Liu, S.; Li, Z.; Shang, X. BCDForest: A boosting cascade deep forest model towards the classification of cancer subtypes based on gene expression data. BMC Bioinform. 2018, 19, 118. [Google Scholar] [CrossRef] [PubMed]
- Szegedy, C.; Liu, W.; Jia, Y.; Sermanet, P.; Reed, S.; Anguelov, D.; Erhan, D.; Vanhoucke, V.; Rabinovich, A. Going deeper with convolutions. In Proceedings of the 2015 IEEE Conference on Computer Vision and Pattern Recognition, Boston, MA, USA, 7–12 June 2015; pp. 1–9. [Google Scholar]
- Bryjova, I.; Kubicek, J.; Molnarova, K.; Peter, L.; Penhaker, M.; Kuca, K. Multiregional Segmentation Modeling in Medical Ultrasonography: Extraction, Modeling and Quantification of Skin Layers and Hypertrophic Scars. In Proceedings of the International Conference on Computational Collective Intelligence, Nicosia, Cyprus, 27 September 2017; pp. 182–670775. [Google Scholar] [CrossRef]
- Scikit-Learn, A. Sklearn.Svm.LinearSVC. Available online: http://scikit-learn.org/stable/modules/generated/sklearn.svm.LinearSVC.html (accessed on 24 August 2018).
- Wikipedia. Kernel method Mathematics: the kernel trick. Available online: https://en.wikipedia.org/wiki/Kernel_method_Mathematics:_the_kernel_trick (accessed on 24 August 2018).




















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Feature | Non-Contact Breast Scan | Sentinel Breast Scan |
|---|---|---|
| IR Camera resolution given in pixels | 640 × 512 | 320 × 240 |
| Temperature sensitivity in °C | 0.05 | 0.08 |
| Number of IR cameras | 2 | 1 |
| Transient IR | Yes | Yes |
| Wavelength range | 3.5–10.5 | 7–12 |
| Cooling time in min | 5–6 | 3–6 |
| Analysis time in min | Immediate | 4–5 |
| Cooling method | Cold Air | Cold Air |
| Deep Neural network (DNN) | Yes | Yes |
| Age < 50 sensitivity with DNN [32] | 78% | 67% |
| Age < 50 sensitivity without DNN [32] | 89% | 78% |
| Age Range | Total Number of Sick | Total Number of Healthy |
|---|---|---|
| 29–50 | 11 | 07 |
| 51–70 | 12 | 31 |
| 71–85 | 01 | 05 |
| Training | Testing | Total | |
|---|---|---|---|
| Healthy | 481 | 121 | 602 |
| Sick | 368 | 92 | 460 |
| Total | 849 | 213 | 1062 |
| Testing | |
|---|---|
| Healthy | 300 |
| Sick | 180 |
| Total | 480 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mambou, S.J.; Maresova, P.; Krejcar, O.; Selamat, A.; Kuca, K. Breast Cancer Detection Using Infrared Thermal Imaging and a Deep Learning Model. Sensors 2018, 18, 2799. https://doi.org/10.3390/s18092799
Mambou SJ, Maresova P, Krejcar O, Selamat A, Kuca K. Breast Cancer Detection Using Infrared Thermal Imaging and a Deep Learning Model. Sensors. 2018; 18(9):2799. https://doi.org/10.3390/s18092799
Chicago/Turabian StyleMambou, Sebastien Jean, Petra Maresova, Ondrej Krejcar, Ali Selamat, and Kamil Kuca. 2018. "Breast Cancer Detection Using Infrared Thermal Imaging and a Deep Learning Model" Sensors 18, no. 9: 2799. https://doi.org/10.3390/s18092799
APA StyleMambou, S. J., Maresova, P., Krejcar, O., Selamat, A., & Kuca, K. (2018). Breast Cancer Detection Using Infrared Thermal Imaging and a Deep Learning Model. Sensors, 18(9), 2799. https://doi.org/10.3390/s18092799