Reliability and Agreement of 3D Trunk and Lower Extremity Movement Analysis by Means of Inertial Sensor Technology for Unipodal and Bipodal Tasks

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Data Collection
2.2.1. Instrumentation
2.2.2. Movement Protocol
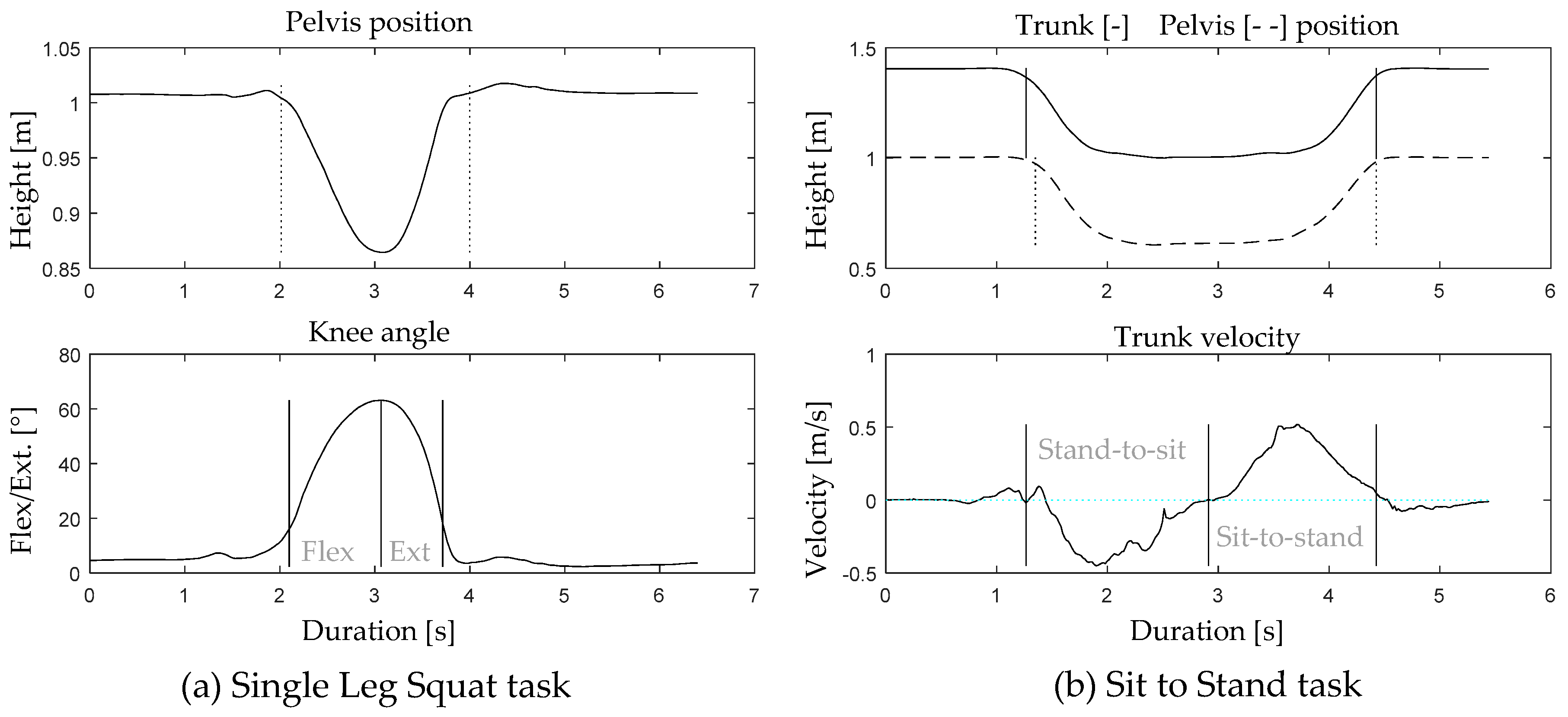
2.3. Data Analysis
2.4. Statistical Analysis and Data Interpretation
Statistical Analysis
3. Results
3.1. Participants
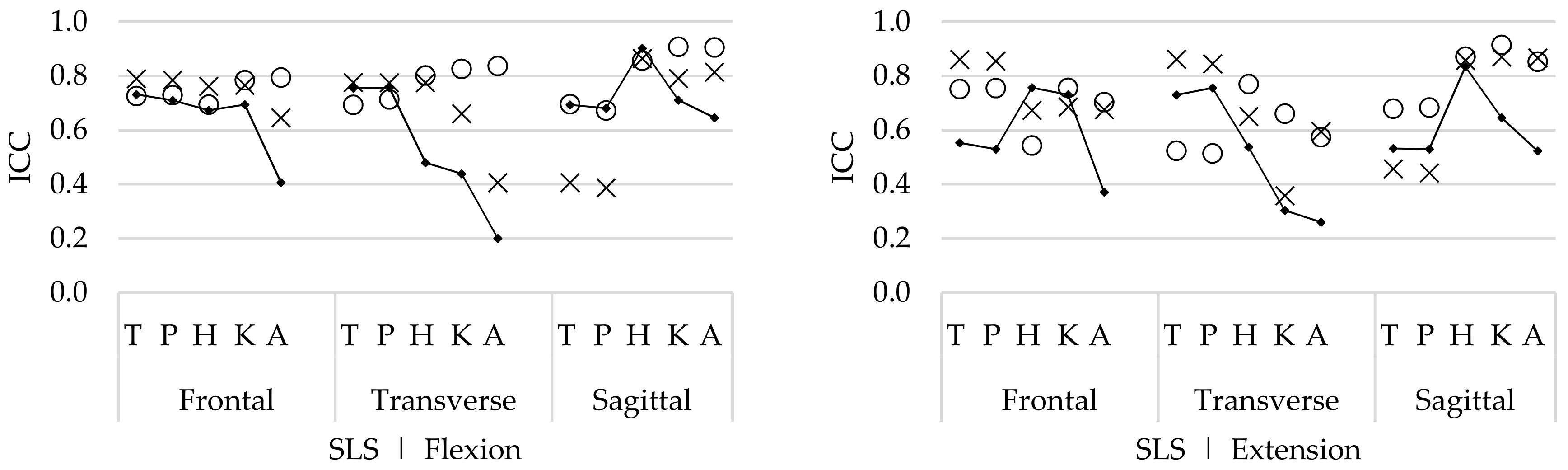
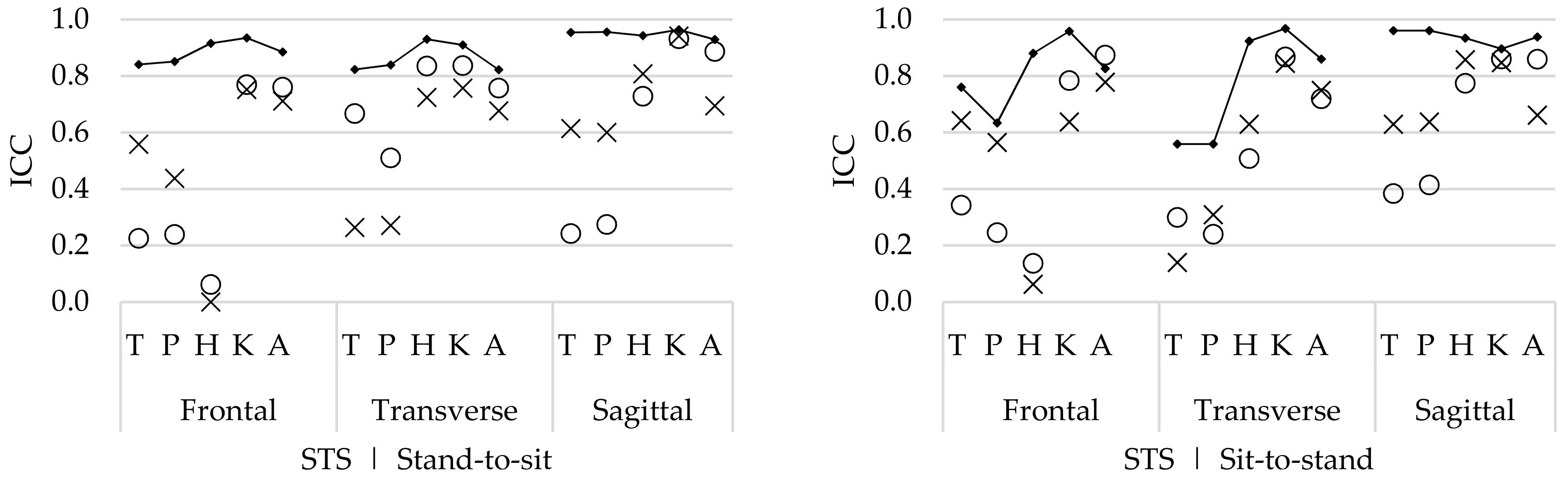
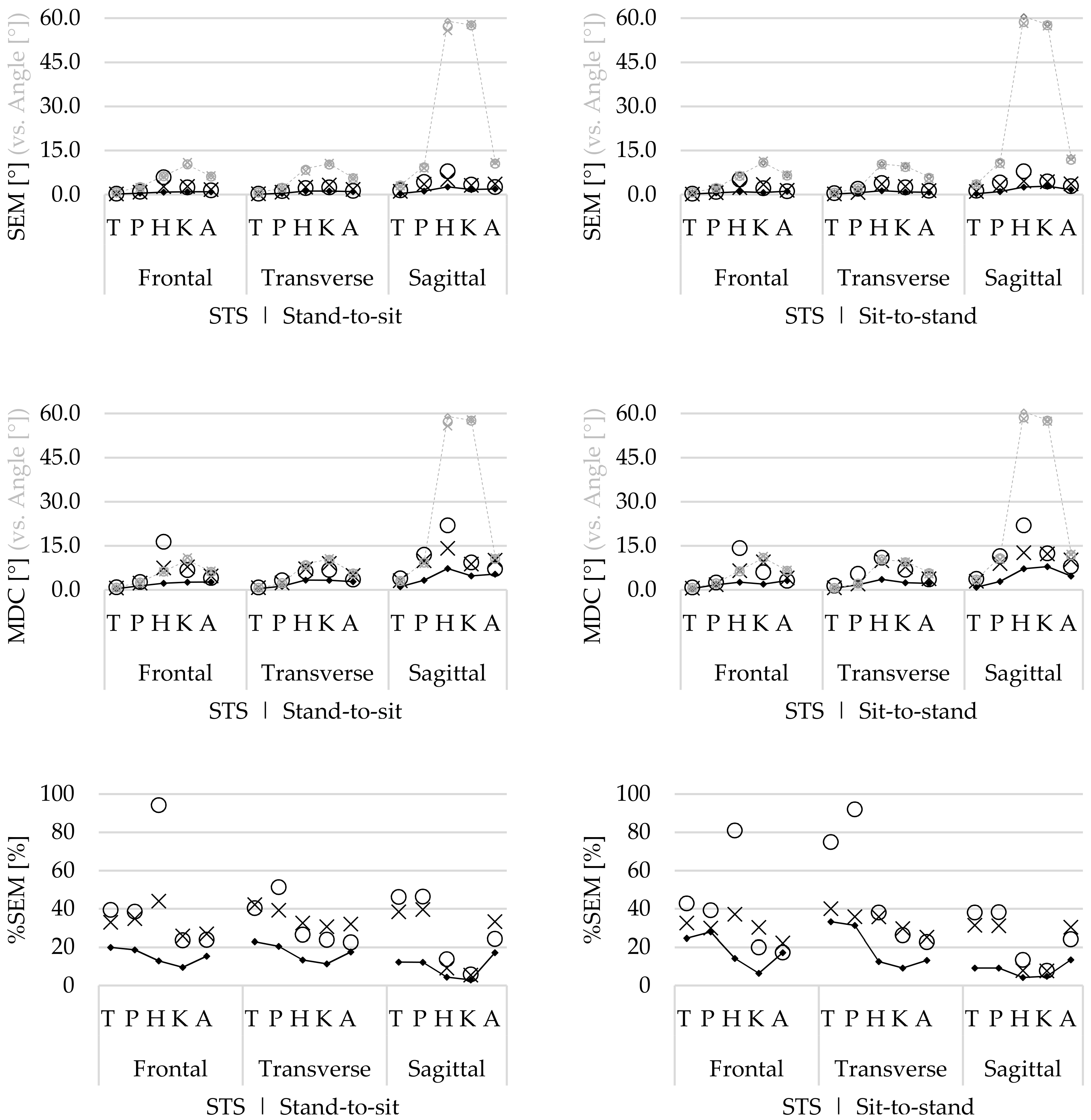
3.2. Reliability and Agreement
3.2.1. Main Movement
3.2.2. Conjunct Movement
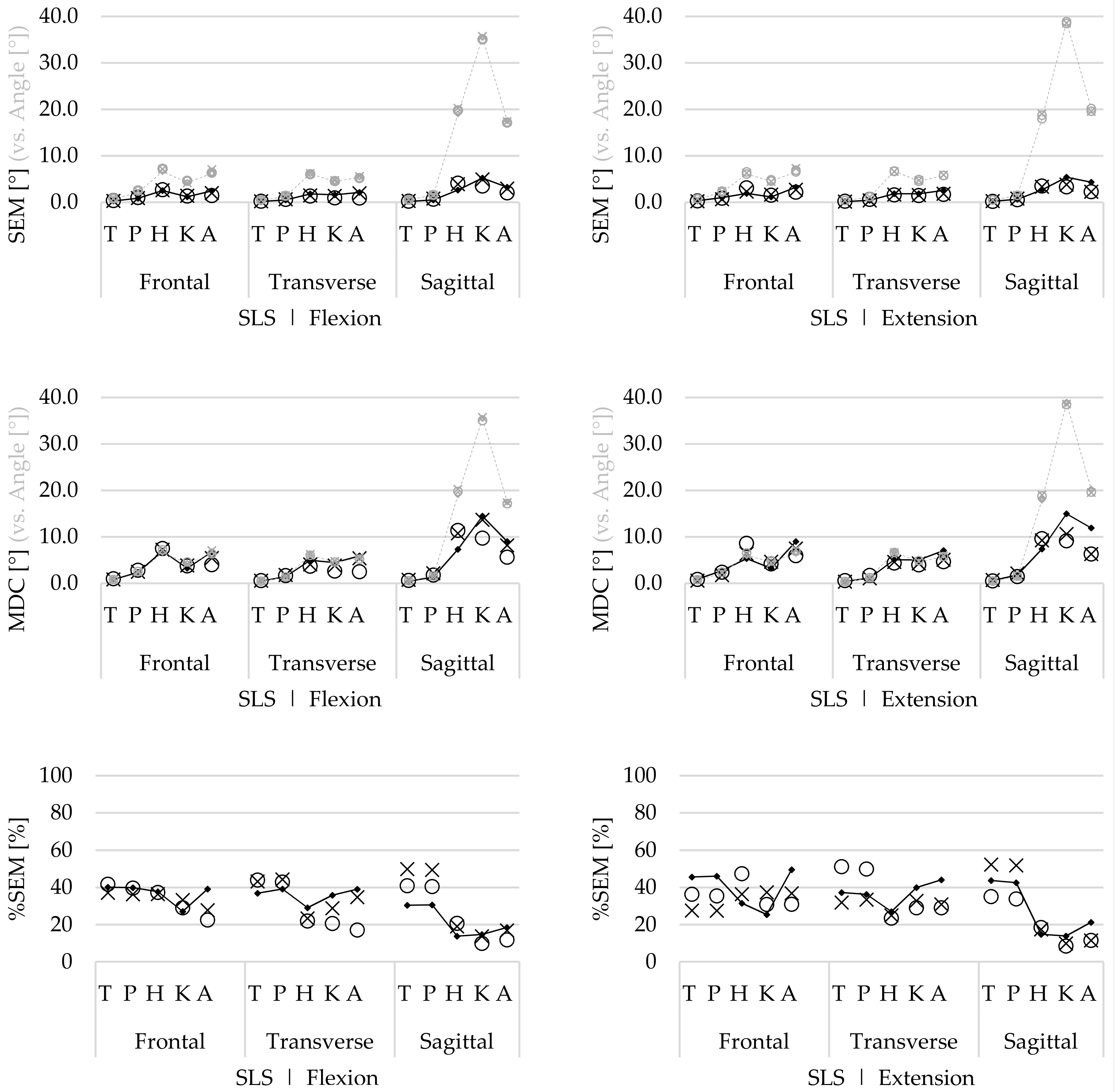
3.2.3. Agreement
4. Discussion
4.1. Interpretation of Study Results
4.1.1. Main Movement
4.1.2. Conjunct Movement
4.1.3. Differences in Movement Phases
4.1.4. Recommendations
4.2. Limitations and Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Luinge, H.J.; Veltink, P.H.; Baten, C.T. Estimating orientation with gyroscopes and accelerometers. Technol. Health Care Off. J. Eur. Soc. Eng. Med. 1999, 7, 455–459. [Google Scholar]
- Roetenberg, D.; Slycke, P.J.; Veltink, P.H. Ambulatory position and orientation tracking fusing magnetic and inertial sensing. IEEE Trans. Biol. Med Eng. 2007, 54, 883–890. [Google Scholar] [CrossRef] [PubMed]
- Roetenberg, D.; Luinge, H.; Slycke, P. Xsens MVN: Full 6DOF Human Motion Tracking Using Miniature Inertial Sensors. Available online: http://citeseerx.ist.psu.edu/viewdoc/summary?doi=10.1.1.569.9604 (accessed on 26 December 2018).
- van der Straaten, R.; De Baets, L.; Jonkers, I.; Timmermans, A. Mobile assessment of the lower limb kinematics in healthy persons and in persons with degenerative knee disorders: A systematic review. Gait Posture 2017, 59, 229–241. [Google Scholar] [CrossRef] [PubMed]
- Al-Amri, M.; Nicholas, K.; Button, K.; Sparkes, V.; Sheeran, L.; Davies, J. Inertial Measurement Units for Clinical Movement Analysis: Reliability and Concurrent Validity. Sensors 2018, 18, 719. [Google Scholar] [CrossRef] [PubMed]
- Cloete, T.; Scheffer, C. Repeatability of an off-the-shelf, full body inertial motion capture system during clinical gait analysis. In Proceedings of the 2010 Annual International Conference of the IEEE Engineering in Medicine and Biology, Buenos Aires, Argentina, 31 August–4 September 2010; Voulme 2010, pp. 5125–5128. [Google Scholar]
- Nuesch, C.; Roos, E.; Pagenstert, G.; Mundermann, A. Measuring joint kinematics of treadmill walking and running: Comparison between an inertial sensor based system and a camera-based system. J. Biomech. 2017, 57, 32–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simic, M.; Hinman, R.S.; Wrigley, T.V.; Bennell, K.L.; Hunt, M.A. Gait modification strategies for altering medial knee joint load: A systematic review. Arthritis Care Res. 2011, 63, 405–426. [Google Scholar] [CrossRef] [PubMed]
- van der Straaten, R.; Timmermans, A.; Bruijnes, A.; Vanwanseele, B.; Jonkers, I.; De Baets, L. Reliability of 3D Lower Extremity Movement Analysis by Means of Inertial Sensor Technology during Transitional Tasks. Sensors 2018, 18, 2638. [Google Scholar] [CrossRef]
- Khuu, A.; Foch, E.; Lewis, C.L. Not all single leg squats are equal: A biomechanical comparison of three variations. Int. J. Sports Phys. Ther. 2016, 11, 201–211. [Google Scholar]
- Turcot, K.; Armand, S.; Fritschy, D.; Hoffmeyer, P.; Suva, D. Sit-to-stand alterations in advanced knee osteoarthritis. Gait Posture 2012, 36, 68–72. [Google Scholar] [CrossRef]
- Boonstra, M.C.; De Waal Malefijt, M.C.; Verdonschot, N. How to quantify knee function after total knee arthroplasty? Knee 2008, 15, 390–395. [Google Scholar] [CrossRef]
- Xsens Technologies B.V.—MVN User Manual: User Guide MVN, MVN BIOMECH, MVN Link, MVN Awinda. Available online: https://fccid.io/QILMTW2-3A7G6/User-Manual/Users-Manual-2695756 (accessed on 26 December 2018).
- Robert-Lachaine, X.; Mecheri, H.; Larue, C.; Plamondon, A. Validation of inertial measurement units with an optoelectronic system for whole-body motion analysis. Med Biol. Eng. Comput. 2017, 55, 609–619. [Google Scholar] [CrossRef] [PubMed]
- Wu, G.; Siegler, S.; Allard, P.; Kirtley, C.; Leardini, A.; Rosenbaum, D.; Whittle, M.; D’Lima, D.D.; Cristofolini, L.; Witte, H.; et al. ISB recommendation on definitions of joint coordinate system of various joints for the reporting of human joint motion—Part I: Ankle, hip, and spine. International Society of Biomechanics. J. Biomech. 2002, 35, 543–548. [Google Scholar] [CrossRef]
- Weir, J.P. Quantifying test-retest reliability using the intraclass correlation coefficient and the SEM. J. Strength Cond. Res. Natl. Strength Cond. Assoc. 2005, 19, 231–240. [Google Scholar]
- Shrout, P.; Fleiss, J. Intraclass Correlations: Uses in Assessing Rater Reliability. Psychol. Bull. 1979, 86, 420–428. [Google Scholar] [CrossRef] [PubMed]
- Matheve, T.; De Baets, L.; Rast, F.; Bauer, C.; Timmermans, A. Within/between-session reliability and agreement of lumbopelvic kinematics in the sagittal plane during functional movement control tasks in healthy persons. Musculoskelet. Sci. Pract. 2018, 33, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, T.H.; Moriya, E.T.; Maciel, C.D.; Serrao, F.V. Test-retest reliability of three-dimensional kinematics using an electromagnetic tracking system during single-leg squat and stepping maneuver. Gait Posture 2014, 39, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Forner-Cordero, A.; Mateu-Arce, M.; Forner-Cordero, I.; Alcantara, E.; Moreno, J.C.; Pons, J.L. Study of the motion artefacts of skin-mounted inertial sensors under different attachment conditions. Physiol. Meas. 2008, 29, N21–N31. [Google Scholar] [CrossRef]
- Donoghue, O.A.; Harrison, A.J.; Coffey, N.; Hayes, K. Functional data analysis of running kinematics in chronic Achilles tendon injury. Med. Sci. Sports Exerc. 2008, 40, 1323–1335. [Google Scholar] [CrossRef]
- Laidig, D.; Schauer, T.; Seel, T. Exploiting kinematic constraints to compensate magnetic disturbances when calculating joint angles of approximate hinge joints from orientation estimates of inertial sensors. In Proceedings of the 2017 International Conference on Rehabilitation Robotics (ICORR), London, UK, 17–20 July 2017; Volume 2017, pp. 971–976. [Google Scholar]
- Kok, M.; Hol, J.D.; Schön, T.B. An optimization-based approach to human body motion capture using inertial sensors. Ifac. Proc. Vol. 2014, 47, 79–85. [Google Scholar] [CrossRef] [Green Version]
- Robert-Lachaine, X.; Mecheri, H.; Larue, C.; Plamondon, A. Accuracy and repeatability of single-pose calibration of inertial measurement units for whole-body motion analysis. Gait Posture 2017, 54, 80–86. [Google Scholar] [CrossRef]
- Graurock, D.; Schauer, T.; Seel, T. User-Adaptive Inertial Sensor Network for Feedback-Controlled Gait Support Systems. In Proceedings of the 20th Annual International FES Society Conference, La Grande Motte, France, 8–10 June 2016; pp. 1–4. [Google Scholar]
- Müller, P.; Bégin, M.; Schauer, T.; Seel, T. Alignment-Free, Self-Calibrating Elbow Angles Measurement Using Inertial Sensors. IEEE J. Biomed. Health Inform. 2017, 21, 312–319. [Google Scholar] [CrossRef] [PubMed]
- Taetz, B.; Bleser, G.; Miezal, M. Towards Self-Calibrating Inertial Body Motion Capture. In Proceedings of the 2016 19th International Conference on Information Fusion (FUSION), Heidelberg, Germany, 5–8 July 2016. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Task | Instruction | |
|---|---|---|
| Single Leg Squat (SLS) |  | Stand still with feet shoulder width apart and put your hands on the pelvis. Shift the weight to the right and lift the left foot from the ground by performing a flexion of the left knee. When standing on one leg with full knee extension, squat on the right leg as deep as possible but remain balanced and make sure the left leg is not contacting the ground. When maximal flexion is reached, extend the right knee and when the right leg is fully extended, place your left foot again down on the floor. |
| Sit to stand (STS) |  | Stand with your back towards the stool with the feet shoulder width apart and with the arms hanging alongside of the body. Sit down without looking over your shoulder, remain seated (like on a chair), and stand up again (without swinging your arms). |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Van der Straaten, R.; Bruijnes, A.K.B.D.; Vanwanseele, B.; Jonkers, I.; De Baets, L.; Timmermans, A. Reliability and Agreement of 3D Trunk and Lower Extremity Movement Analysis by Means of Inertial Sensor Technology for Unipodal and Bipodal Tasks. Sensors 2019, 19, 141. https://doi.org/10.3390/s19010141
Van der Straaten R, Bruijnes AKBD, Vanwanseele B, Jonkers I, De Baets L, Timmermans A. Reliability and Agreement of 3D Trunk and Lower Extremity Movement Analysis by Means of Inertial Sensor Technology for Unipodal and Bipodal Tasks. Sensors. 2019; 19(1):141. https://doi.org/10.3390/s19010141
Chicago/Turabian StyleVan der Straaten, Rob, Amber K. B. D. Bruijnes, Benedicte Vanwanseele, Ilse Jonkers, Liesbet De Baets, and Annick Timmermans. 2019. "Reliability and Agreement of 3D Trunk and Lower Extremity Movement Analysis by Means of Inertial Sensor Technology for Unipodal and Bipodal Tasks" Sensors 19, no. 1: 141. https://doi.org/10.3390/s19010141
APA StyleVan der Straaten, R., Bruijnes, A. K. B. D., Vanwanseele, B., Jonkers, I., De Baets, L., & Timmermans, A. (2019). Reliability and Agreement of 3D Trunk and Lower Extremity Movement Analysis by Means of Inertial Sensor Technology for Unipodal and Bipodal Tasks. Sensors, 19(1), 141. https://doi.org/10.3390/s19010141