A Dynamic Time Warping Based Algorithm to Evaluate Kinect-Enabled Home-Based Physical Rehabilitation Exercises for Older People



Abstract
:1. Introduction
2. Methods
2.1. Development of a DTW-Based Algorithm for Performance Evaluation
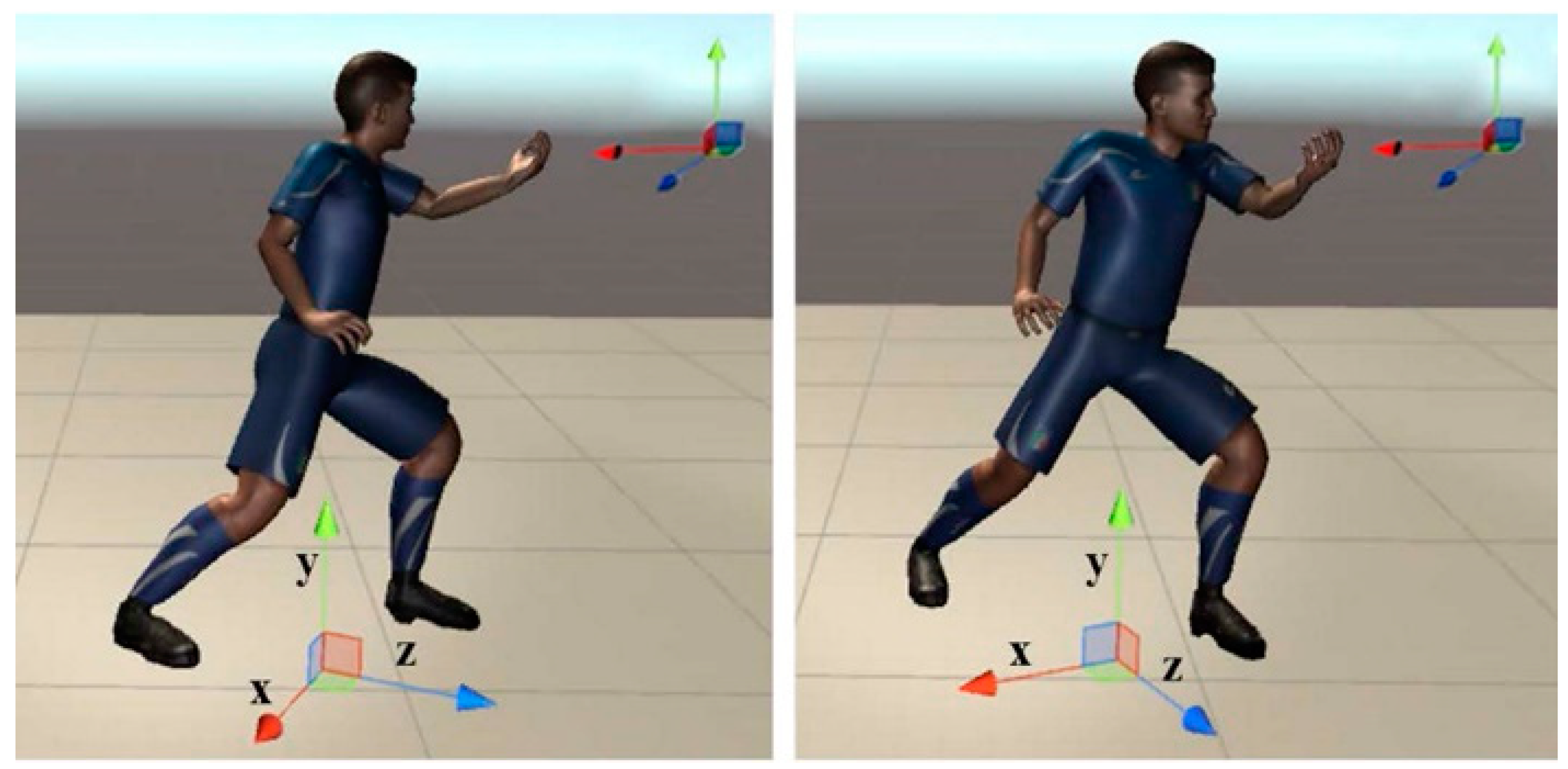
2.1.1. 3D Pose Comparison
2.1.2. Motion Comparison
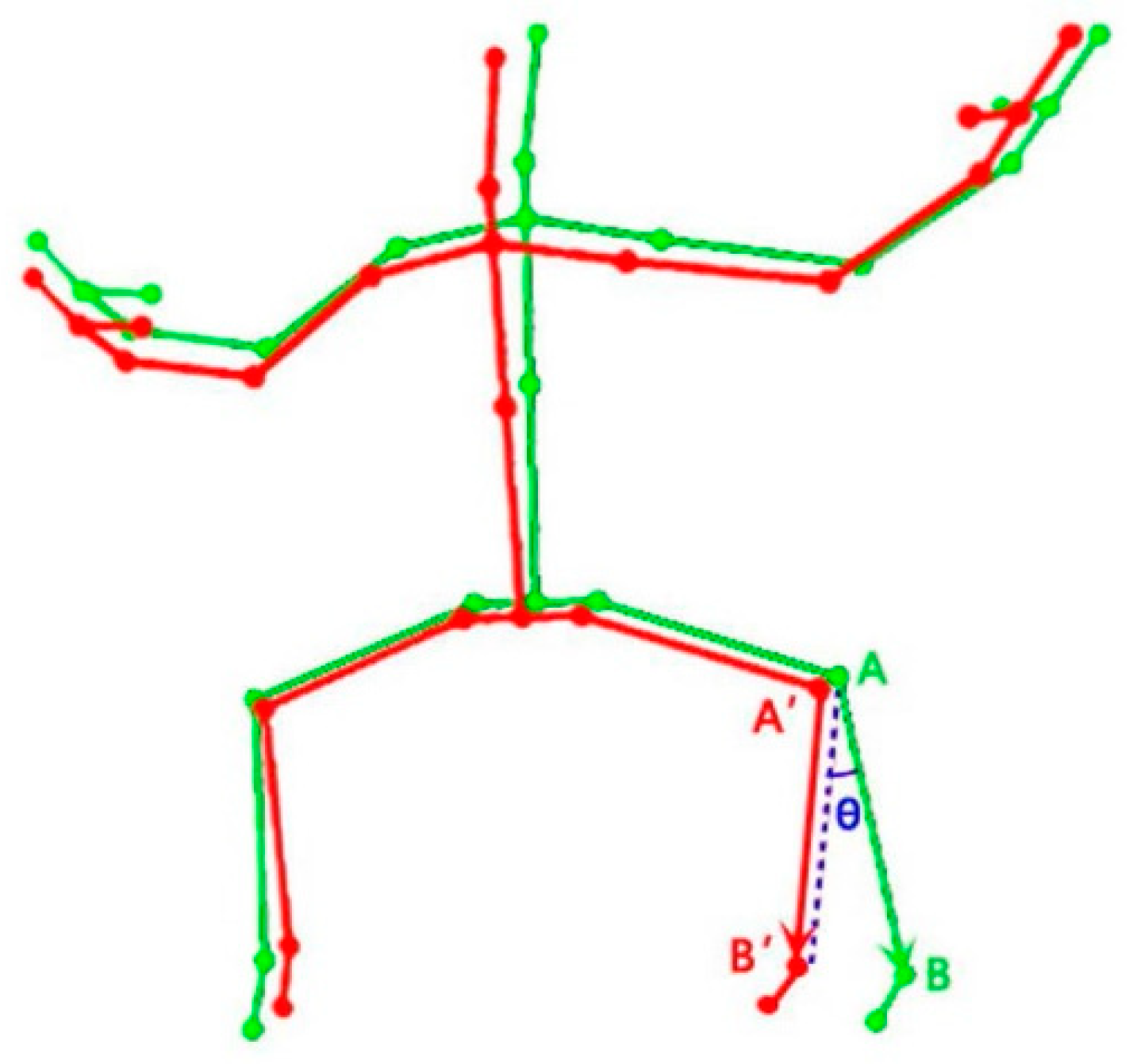
2.1.3. Body Orientation Offset
2.2. Validation of the Developed DTW-Based Algorithm
2.2.1. Experimental Participants
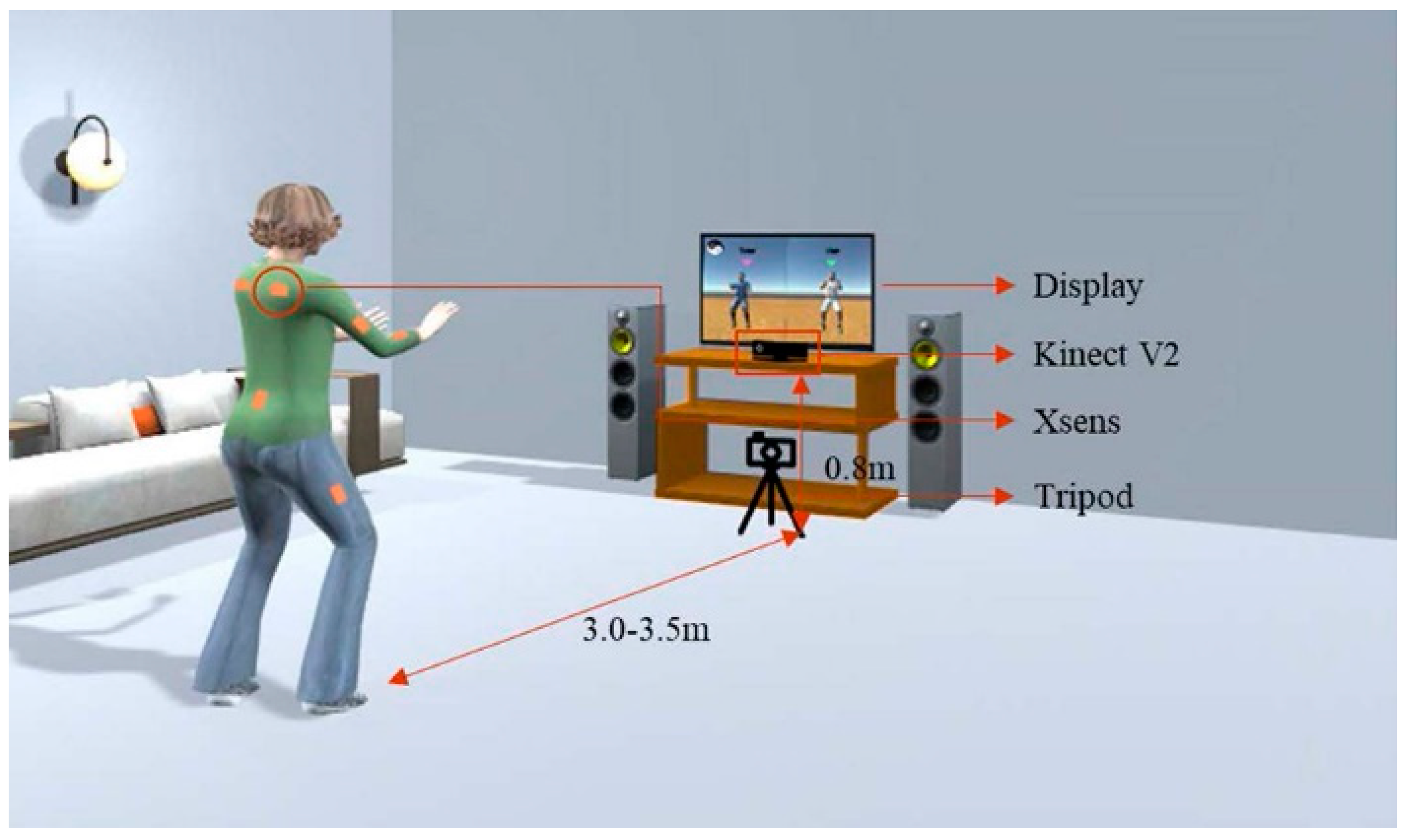
2.2.2. Experimental Setup and Procedure
2.2.3. Statistical Analysis
3. Results
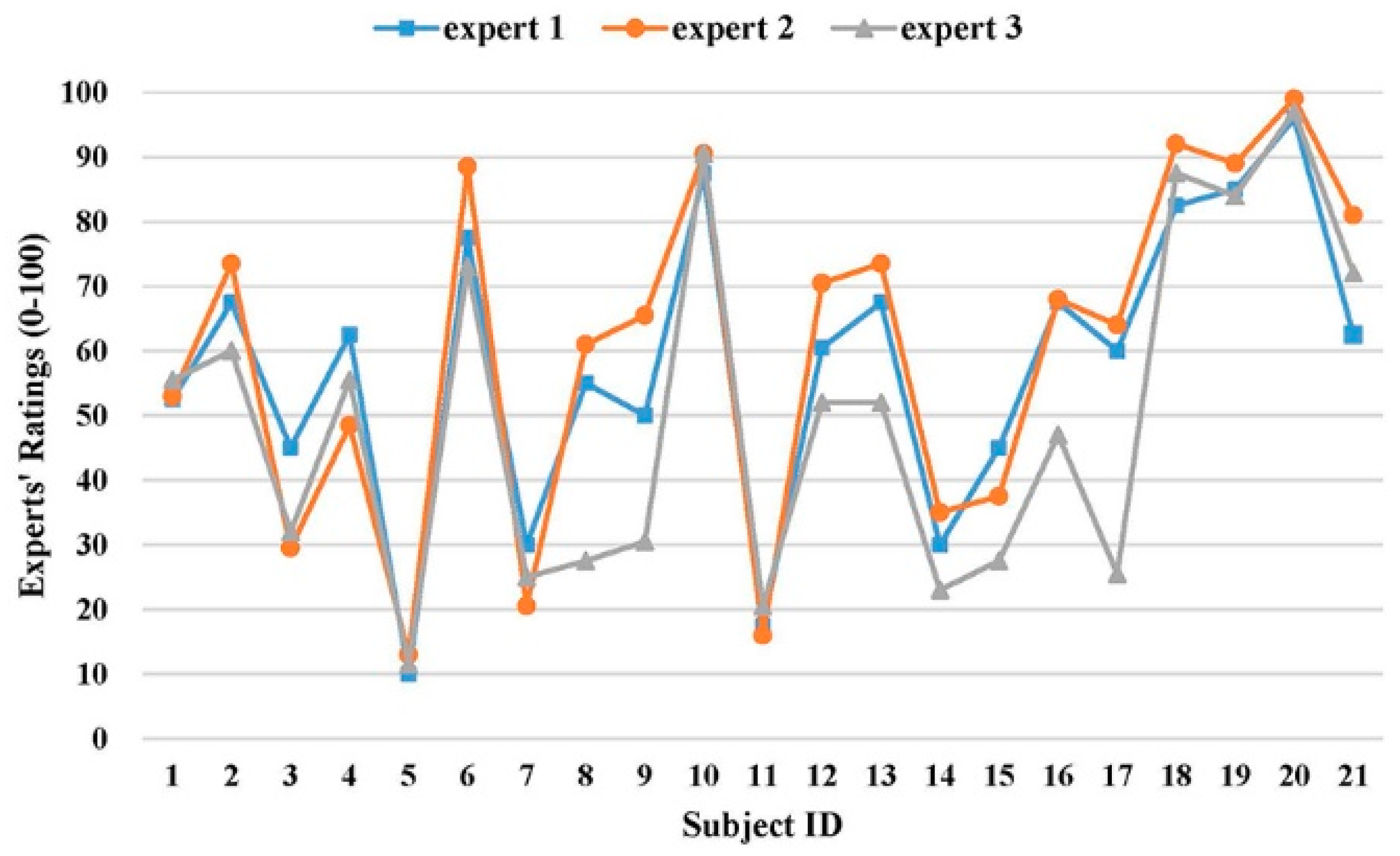
3.1. Inter-Rater Reliability of Experts’ Ratings
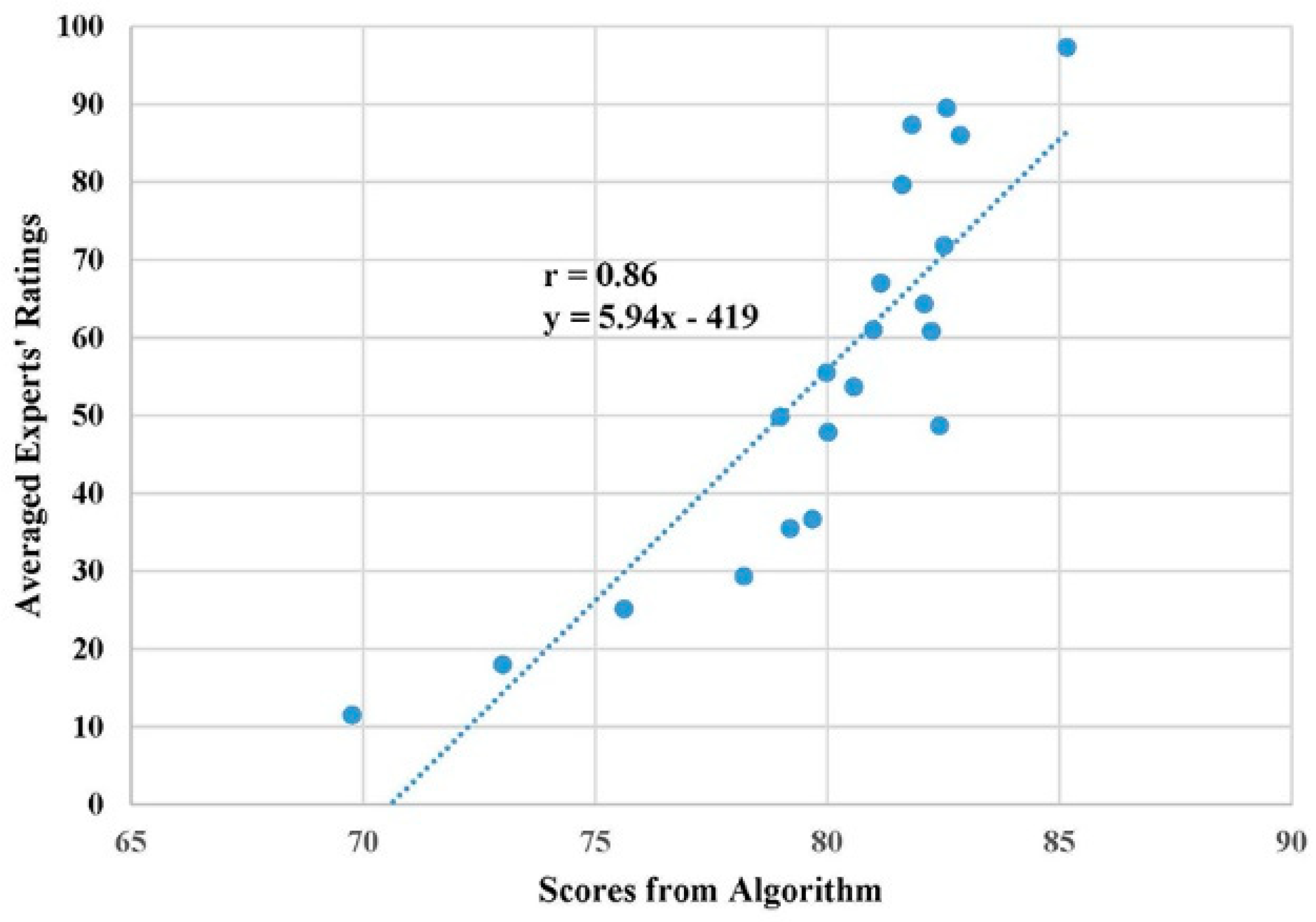
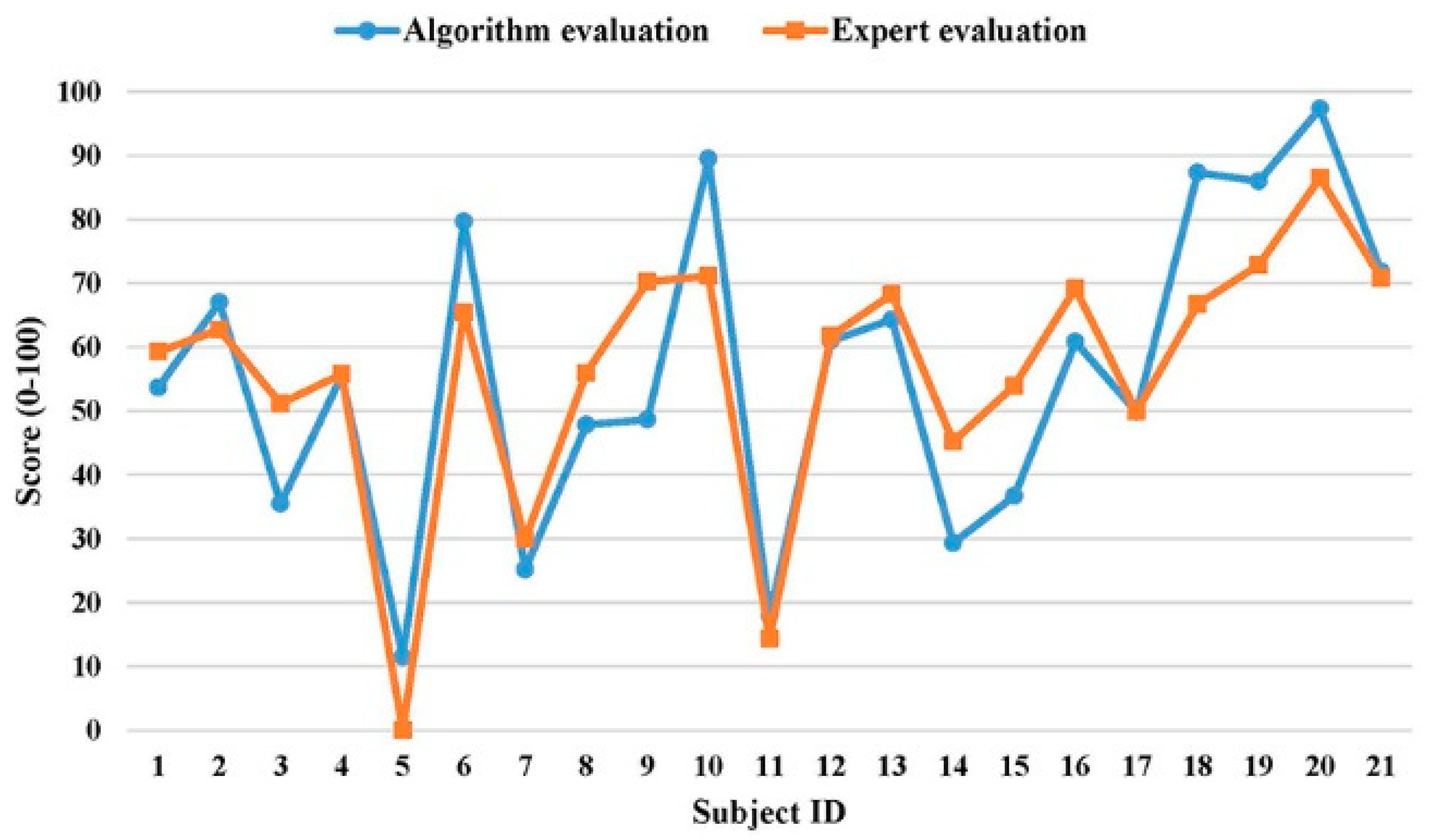
3.2. Evaluation Comparison between Experts and the Developed Algorithm
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Construct ID | Questions | Strongly Disagree | Disagree | Undecided | Agree | Strongly Agree |
|---|---|---|---|---|---|---|
| 1 | Perceived Usefulness (PU) | |||||
| PU1: Using this system will help improve my health quality. | 1 | 2 | 3 | 4 | 5 | |
| PU2: Using this system will make me more effective in my life. | 1 | 2 | 3 | 4 | 5 | |
| PU3: Overall, I find this system to be useful in my life. | 1 | 2 | 3 | 4 | 5 | |
| 2 | Hedonic Motivation (HM) | |||||
| HM1: Using this system is fun. | 1 | 2 | 3 | 4 | 5 | |
| HM2: Using this system is enjoyable. | 1 | 2 | 3 | 4 | 5 | |
| HM3: Using this system is entertaining. | 1 | 2 | 3 | 4 | 5 | |
| 3 | Effort Expectancy (EE) | |||||
| EE1: Learning how to use this system is easy for me. | 1 | 2 | 3 | 4 | 5 | |
| EE2: I find this system easy to use. | 1 | 2 | 3 | 4 | 5 | |
| EE3: It is easy for me to become skillful at using this system. | 1 | 2 | 3 | 4 | 5 | |
| 4 | Social Influence (SI) | |||||
| SI1: People who are important to me would think that I should use this system. | 1 | 2 | 3 | 4 | 5 | |
| SI2: People who influence me would think that I should use this system. | 1 | 2 | 3 | 4 | 5 | |
| SI3: People whose opinion are valued to me would prefer that I use this system. | 1 | 2 | 3 | 4 | 5 | |
| 5 | Self-Efficacy (SE) | |||||
| SE1: It is easy for me to improve my health conditions by using this system. | 1 | 2 | 3 | 4 | 5 | |
| SE2: I have the capability to use this system to improve my health condition. | 1 | 2 | 3 | 4 | 5 | |
| SE3: I am able to use this system to improve my health condition without much effort. | 1 | 2 | 3 | 4 | 5 | |
| 6 | Perceived Vulnerability (PV): having little knowledge about self-care and improving personal healthcare; suffering falls. | |||||
| PV1: I am at the risk of suffering from the stated problems. | 1 | 2 | 3 | 4 | 5 | |
| PV2: It is likely that I will suffer the stated problems. | 1 | 2 | 3 | 4 | 5 | |
| PV3: It is possible for me to suffer the stated problems. | 1 | 2 | 3 | 4 | 5 | |
| 7 | Perceived Severity (PS): having little knowledge about self-care and improving personal healthcare; suffering falls. | |||||
| PS1: If I suffered the stated problems, it would be severe. | 1 | 2 | 3 | 4 | 5 | |
| PS2: If I suffered the stated problems, it would be serious. | 1 | 2 | 3 | 4 | 5 | |
| PS3: If I suffered the stated problems, it would be significant. | 1 | 2 | 3 | 4 | 5 | |
| 8 | Perceived Privacy Risk (PPR) | |||||
| PPR1: It would be at risk to disclose my personal health information to the doctor. | 1 | 2 | 3 | 4 | 5 | |
| PPR2: There would be high potential for loss associated with disclosing my personal health information to the doctor. | 1 | 2 | 3 | 4 | 5 | |
| PPR3: There would be too much uncertainty associated with giving my personal health information to the doctor. | 1 | 2 | 3 | 4 | 5 | |
| 9 | Behavioral Intention (BI) | |||||
| BI1: I intend to use this system in the future. | 1 | 2 | 3 | 4 | 5 | |
| BI2: I intend to use this system at every opportunity in the future. | 1 | 2 | 3 | 4 | 5 | |
| BI3: I plan to increase my use of this system in the future. | 1 | 2 | 3 | 4 | 5 | |
| 10 | Attitude (AT) | |||||
| AT1: Using this system is a good idea. | 1 | 2 | 3 | 4 | 5 | |
| AT2: Using this system is a wise idea. | 1 | 2 | 3 | 4 | 5 | |
| AT3: I like the idea of using this system. | 1 | 2 | 3 | 4 | 5 | |
| 11 | Response Cost (RC) | |||||
| RC1: This system is expensive to purchase (the price of Kinect is $150). | 1 | 2 | 3 | 4 | 5 | |
| RC2: I have to spend effort on learning how to use this system. | 1 | 2 | 3 | 4 | 5 | |
| RC3: Using this system will change my life style. | 1 | 2 | 3 | 4 | 5 | |
References
- World Health Organization Ageing and Health. Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (accessed on 9 March 2019).
- Weening-Dijksterhuis, E.; de Greef, M.H.; Scherder, E.J.; Slaets, J.P.; van der Schans, C.P. Frail institutionalized older persons: A comprehensive review on physical exercise, physical fitness, activities of daily living, and quality-of-life. Am. J. Phys. Med. Rehabil. 2011, 90, 156–168. [Google Scholar] [CrossRef]
- Windle, G.; Hughes, D.; Linck, P.; Russell, I.; Woods, B. Is exercise effective in promoting mental well-being in older age? A systematic review. Aging Ment. Health 2010, 14, 652–669. [Google Scholar] [CrossRef]
- Frändin, K.; Grönstedt, H.; Helbostad, J.L.; Bergland, A.; Andresen, M.; Puggaard, L.; Harms-Ringdahl, K.; Granbo, R.; Hellström, K. Long-term effects of individually tailored physical training and activity on physical function, well-being and cognition in Scandinavian nursing home residents: A randomized controlled trial. Gerontology 2016, 62, 571–580. [Google Scholar] [CrossRef]
- Brach, J.S.; FitzGerald, S.; Newman, A.B.; Kelsey, S.; Kuller, L.; VanSwearingen, J.M.; Kriska, A.M. Physical activity and functional status in community-dwelling older women: A 14-year prospective study. Arch. Intern. Med. 2003, 163, 2565–2571. [Google Scholar] [CrossRef]
- Rydwik, E.; Frändin, K.; Akner, G. Effects of a physical training and nutritional intervention program in frail elderly people regarding habitual physical activity level and activities of daily living—A randomized controlled pilot study. Arch. Gerontol. Geriatr. 2010, 51, 283–289. [Google Scholar] [CrossRef]
- Organization, W.H. A guide for population-based approaches to increasing levels of physical activity. In Implementation of the WHO Global Strategy on Diet, Physical Activity and Health; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Lin, S.F.; Lee, J.W.; Modeste, N.; Johnson, E.G. Attitudes and beliefs predicting Taiwanese older adults’ intentions to attend strength and balance training programs. J. Appl. Gerontol. 2012, 31, 260–281. [Google Scholar] [CrossRef]
- Choi, S.D.; Guo, L.; Kang, D.; Xiong, S. Exergame technology and interactive interventions for elderly fall prevention: A systematic literature review. Appl. Ergon. 2017, 65, 570–581. [Google Scholar] [CrossRef]
- Yardley, L.; Bishop, F.L.; Beyer, N.; Hauer, K.; Kempen, G.I.; Piot-Ziegler, C.; Todd, C.J.; Cuttelod, T.; Horne, M.; Lanta, K. Older people’s views of falls-prevention interventions in six European countries. Gerontologist 2006, 46, 650–660. [Google Scholar] [CrossRef]
- Kobayashi, R.; Nakadaira, H.; Ishigami, K.; Muto, K.; Anesaki, S.; Yamamoto, M. Effects of physical exercise on fall risk factors in elderly at home in intervention trial. Environ. Health Prev. Med. 2006, 11, 250–255. [Google Scholar] [CrossRef]
- Liu-Ambrose, T.; Donaldson, M.G.; Ahamed, Y.; Graf, P.; Cook, W.L.; Close, J.; Lord, S.R.; Khan, K.M. Otago home-based strength and balance retraining improves executive functioning in older fallers: A randomized controlled trial. J. Am. Geriatr. Soc. 2008, 56, 1821–1830. [Google Scholar] [CrossRef]
- Uzor, S.; Baillie, L. Investigating the long-term use of exergames in the home with elderly fallers. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, Toronto, ON, Canada, 26 April–1 May 2014; pp. 2813–2822. [Google Scholar]
- Arlati, S.; Colombo, V.; Spoladore, D.; Greci, L.; Pedroli, E.; Serino, S.; Cipresso, P.; Goulene, K.; Stramba-Badiale, M.; Riva, G.; et al. A Social Virtual Reality-Based Application for the Physical and Cognitive Training of the Elderly at Home. Sensors 2019, 19, 261. [Google Scholar] [CrossRef]
- Fortino, G.; Gravina, R. A cloud-assisted wearable system for physical rehabilitation. In ICTs for Improving Patients Rehabilitation Research Techniques; Springer: Berlin, Germany, 2014; pp. 168–182. [Google Scholar]
- Ofli, F.; Kurillo, G.; Obdržálek, Š.; Bajcsy, R.; Jimison, H.B.; Pavel, M. Design and evaluation of an interactive exercise coaching system for older adults: Lessons learned. IEEE J. Biomed. Health Inform. 2016, 20, 201–212. [Google Scholar] [CrossRef]
- Lin, T.Y.; Hsieh, C.H.; Lee, J.D. A kinect-based system for physical rehabilitation: Utilizing Tai Chi exercises to improve movement disorders in patients with balance ability. In Proceedings of the Asia Modelling Symposium 2013: 7th Asia International Conference on Mathematical Modelling and Computer Simulation, Hong Kong, China, 23–25 July 2013; pp. 149–153. [Google Scholar]
- Muangmoon, O.-O.; Sureephong, P.; Tabia, K. Dance Training Tool Using Kinect-Based Skeleton Tracking and Evaluating Dancer’s Performance. In International Conference on Industrial, Engineering and other Applications of Applied Intelligent Systems; Springer: Berlin, Germany, 2017; pp. 27–32. [Google Scholar]
- Alexiadis, D.S.; Kelly, P.; Daras, P.; O’Connor, N.E.; Boubekeur, T.; Moussa, M.B. Evaluating a dancer’s performance using kinect-based skeleton tracking. In Proceedings of the 19th ACM International Conference on Multimedia, Scottsdale, AZ, USA, 28 November—1 December 2011; pp. 659–662. [Google Scholar]
- Ren, W.; Pu, F.; Fan, X.; Li, S.; Sun, L.; Li, D.; Wang, Y.; Fan, Y. Kinect-Based Skeleton-Matching Feedback for Motor Rehabilitation: Transient Performance Effect of Shoulder training. J. Mech. Med. Biol. 2016, 16. [Google Scholar] [CrossRef]
- Capecci, M.; Ceravolo, M.G.; Ferracuti, F.; Iarlori, S.; Kyrki, V.; Longhi, S.; Romeo, L.; Verdini, F. Physical rehabilitation exercises assessment based on hidden semi-markov model by kinect v2. In Proceedings of the 2016 IEEE-EMBS International Conference on Biomedical and Health Informatics (BHI), Las Vegas, NV, USA, 24–27 February 2016; pp. 256–259. [Google Scholar]
- Rybarczyk, Y.; Deters, J.K.; Gonzalo, A.A.; Esparza, D.; Gonzalez, M.; Villarreal, S.; Nunes, I.L. Recognition of physiotherapeutic exercises through DTW and low-cost vision-based motion capture. In International Conference on Applied Human Factors and Ergonomics; Springer: Berlin, Germany, 2017; pp. 348–360. [Google Scholar]
- Müller, M.; Röder, T. Motion templates for automatic classification and retrieval of motion capture data. In Proceedings of the 2006 ACM SIGGRAPH/Eurographics Symposium on Computer Animation, Vienna, Austria, 2–4 September 2006; Eurographics Association: Aire-la-Ville, Switzerland, 2006; pp. 137–146. [Google Scholar]
- Saraee, E.; Singh, S.; Hendron, K.; Zheng, M.; Joshi, A.; Ellis, T.; Betke, M. ExerciseCheck: Remote monitoring and evaluation platform for home based physical therapy. In Proceedings of the 10th International Conference on PErvasive Technologies Related to Assistive Environments, Rhodes, Greece, 21–23 June 2017; pp. 87–90. [Google Scholar]
- Semblantes, P.A.; Andaluz, V.H.; Lagla, J.; Chicaiza, F.A.; Acurio, A. Visual feedback framework for rehabilitation of stroke patients. Inform. Med. Unlocked 2018, 13, 41–50. [Google Scholar] [CrossRef]
- Saenz-de-Urturi, Z.; Garcia-Zapirain Soto, B. Kinect-based virtual game for the elderly that detects incorrect body postures in real time. Sensors 2016, 16, 704. [Google Scholar] [CrossRef]
- Su, C.-J.; Chiang, C.-Y.; Huang, J.-Y. Kinect-enabled home-based rehabilitation system using Dynamic Time Warping and fuzzy logic. Appl. Soft Comput. 2014, 22, 652–666. [Google Scholar] [CrossRef]
- Wei, Y.; Yan, H.; Bie, R.; Wang, S.; Sun, L. Performance monitoring and evaluation in dance teaching with mobile sensing technology. Pers. Ubiquitous Comput. 2014, 18, 1929–1939. [Google Scholar] [CrossRef]
- Chatzitofis, A.; Monaghan, D.; Mitchell, E.; Honohan, F.; Zarpalas, D.; O’Connor, N.E.; Daras, P. HeartHealth: A cardiovascular disease home-based rehabilitation system. Procedia Comput. Sci. 2015, 63, 340–347. [Google Scholar] [CrossRef]
- Mocanu, I.; Marian, C.; Rusu, L.; Arba, R. A Kinect based adaptive exergame. In Proceedings of the 2016 IEEE 12th International Conference on Intelligent Computer Communication and Processing, Cluj-Napoca, Romania, 8–10 September 2016; pp. 117–124. [Google Scholar]
- Osgouei, R.H.; Soulsbv, D.; Bello, F. An Objective Evaluation Method for Rehabilitation Exergames. In Proceedings of the 2018 IEEE Games, Entertainment, Media Conference (GEM), Galway, Ireland, 15–17 August 2018; pp. 28–34. [Google Scholar]
- Salvador, S.; Chan, P. Toward accurate dynamic time warping in linear time and space. Intell. Data Anal. 2007, 11, 561–580. [Google Scholar] [CrossRef] [Green Version]
- Müller, M. Information Retrieval for Music and Motion; Springer: Berlin, Germany, 2007; Volume 2. [Google Scholar]
- Shokoohi-Yekta, M.; Wang, J.; Keogh, E. On the non-trivial generalization of dynamic time warping to the multi-dimensional case. In Proceedings of the 2015 SIAM International Conference on Data Mining, Vancouver, BC, Canada, 30 April–2 May 2015; pp. 289–297. [Google Scholar]
- Lanciault, R. Mecanim Humanoids. Available online: https://blogs.unity3d.com/2014/05/26/mecanim-humanoids/ (accessed on 15 March 2019).
- Filkov, R. K2-Asset On-line Documentation. Available online: https://ratemt.com/k2docs/ (accessed on 9 May 2018).
- Moon, S.; Park, Y.; Ko, D.W.; Suh, I.H. Multiple kinect sensor fusion for human skeleton tracking using Kalman filtering. Int. J. Adv. Robot. Syst. 2016, 13. [Google Scholar] [CrossRef]
- Karatsidis, A.; Bellusci, G.; Schepers, H.M.; de Zee, M.; Andersen, M.S.; Veltink, P.H. Estimation of ground reaction forces and moments during gait using only inertial motion capture. Sensors 2016, 17, 75. [Google Scholar] [CrossRef]
- Guo, L.; Xiong, S. Accuracy of base of support using an inertial sensor based motion capture system. Sensors 2017, 17, 2091. [Google Scholar] [CrossRef]
- Reips, U.-D.; Funke, F. Interval-level measurement with visual analogue scales in Internet-based research: VAS Generator. Behav. Res. Methods 2008, 40, 699–704. [Google Scholar] [CrossRef]
- Shrout, P.E.; Fleiss, J.L. Intraclass correlations: Uses in assessing rater reliability. Psychol. Bull. 1979, 86, 420–428. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef]
- Ćwiękała-Lewis, K.J.; Gallek, M.; Taylor-Piliae, R.E. The effects of Tai Chi on physical function and well-being among persons with Parkinson’s Disease: A systematic review. J. Bodyw. Mov. Ther. 2017, 21, 414–421. [Google Scholar] [CrossRef]
- Sun, J.; Kanagawa, K.; Sasaki, J.; Ooki, S.; Xu, H.; Wang, L. Tai chi improves cognitive and physical function in the elderly: A randomized controlled trial. J. Phys. Ther. Sci. 2015, 27, 1467–1471. [Google Scholar] [CrossRef]
- Kottner, J.; Audigé, L.; Brorson, S.; Donner, A.; Gajewski, B.J.; Hróbjartsson, A.; Roberts, C.; Shoukri, M.; Streiner, D.L. Guidelines for reporting reliability and agreement studies (GRRAS) were proposed. Int. J. Nurs. Stud. 2011, 48, 661–671. [Google Scholar] [CrossRef]
- Kim, T.; Xiong, S. Comparison of seven fall risk assessment tools in community-dwelling Korean older women. Ergonomics 2017, 60, 421–429. [Google Scholar] [CrossRef]
- Chua, P.T.; Crivella, R.; Daly, B.; Hu, N.; Schaaf, R.; Ventura, D.; Camill, T.; Hodgins, J.; Pausch, R. Training for physical tasks in virtual environments: Tai Chi. In Proceedings of the IEEE Virtual Reality 2003, Los Angeles, CA, USA, 22–26 March 2003; pp. 87–94. [Google Scholar]
- Gao, Y.; Li, H.; Luo, Y. An empirical study of wearable technology acceptance in healthcare. Ind. Manag. Data Syst. 2015, 115, 1704–1723. [Google Scholar] [CrossRef]
- Kim, S.S. The integrative framework of technology use: An extension and test. MIS Q. 2009, 33, 513–537. [Google Scholar] [CrossRef]
- Bhattacherjee, A.; Hikmet, N. Physicians’ resistance toward healthcare information technologies: A dual-factor model. Proceedings of 2007 40th the Annual Hawaii International Conference on System Sciences, Waikoloa, HI, USA, 3–6 January 2007. [Google Scholar]
- Lee, Y.; Larsen, K.R. Threat or coping appraisal: Determinants of SMB executives’ decision to adopt anti-malware software. Eur. J. Inf. Syst. 2009, 18, 177–187. [Google Scholar] [CrossRef]








© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, X.; Xiong, S. A Dynamic Time Warping Based Algorithm to Evaluate Kinect-Enabled Home-Based Physical Rehabilitation Exercises for Older People. Sensors 2019, 19, 2882. https://doi.org/10.3390/s19132882
Yu X, Xiong S. A Dynamic Time Warping Based Algorithm to Evaluate Kinect-Enabled Home-Based Physical Rehabilitation Exercises for Older People. Sensors. 2019; 19(13):2882. https://doi.org/10.3390/s19132882
Chicago/Turabian StyleYu, Xiaoqun, and Shuping Xiong. 2019. "A Dynamic Time Warping Based Algorithm to Evaluate Kinect-Enabled Home-Based Physical Rehabilitation Exercises for Older People" Sensors 19, no. 13: 2882. https://doi.org/10.3390/s19132882
APA StyleYu, X., & Xiong, S. (2019). A Dynamic Time Warping Based Algorithm to Evaluate Kinect-Enabled Home-Based Physical Rehabilitation Exercises for Older People. Sensors, 19(13), 2882. https://doi.org/10.3390/s19132882