The Use of Wearable Sensors for the Movement Assessment on Muscle Contraction Sequences in Post-Stroke Patients during Sit-to-Stand

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
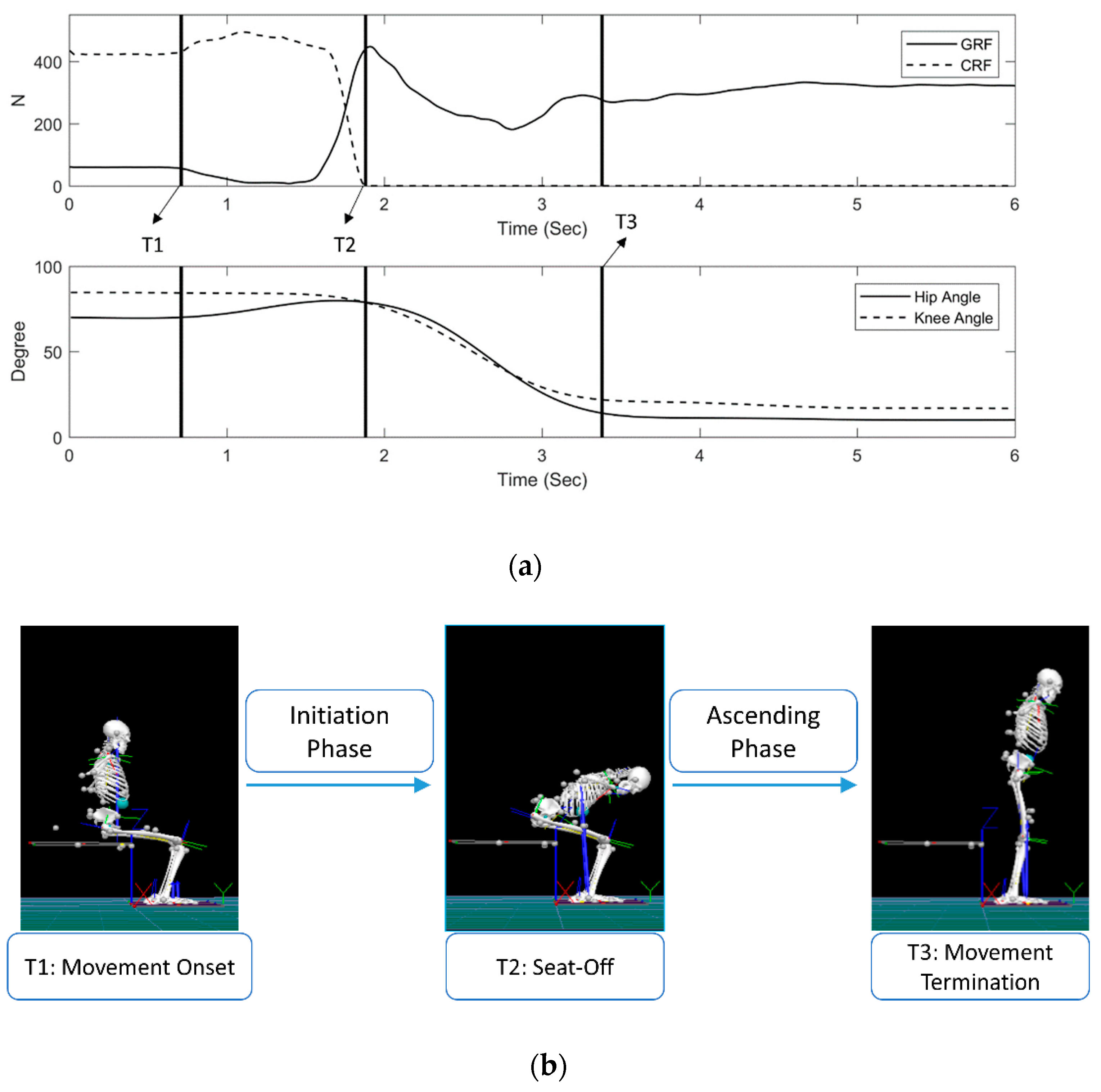
2.2. Instruments and STS Cycle
2.3. Experiments Procedure
2.4. Data Analysis
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; De Ferranti, S.; Després, J.P.; Fullerton, H.J.; Howard, V.J. Executive summary: Heart disease and stroke statistics-2015 update: A report from the american heart association. Circulation 2015, 131, 434–441. [Google Scholar] [CrossRef]
- Silva, P.F.d.S.; Quintino, L.F.; Franco, J.; Rodrigues-de-Paula, F.; Albuquerque de Araújo, P.; Faria, C.D.C.d.M. Trunk kinematics related to generation and transfer of the trunk flexor momentum are associated with sit-to-stand performance in chronic stroke survivors. NeuroRehabilitation 2017, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Roy, G.; Nadeau, S.; Gravel, D.; Malouin, F.; McFadyen, B.J.; Piotte, F. The effect of foot position and chair height on the asymmetry of vertical forces during sit-to-stand and stand-to-sit tasks in individuals with hemiparesis. Clin. Biomech. 2006, 21, 585–593. [Google Scholar] [CrossRef] [PubMed]
- Duclos, C.; Nadeau, S.; Lecours, J. Lateral trunk displacement and stability during sit-to-stand transfer in relation to foot placement in patients with hemiparesis. Neurorehabil. Neural Repair. 2008, 22, 715–722. [Google Scholar] [CrossRef] [PubMed]
- Boukadida, A.; Piotte, F.; Dehail, P.; Nadeau, S. Determinants of sit-to-stand tasks in individuals with hemiparesis post stroke: A review. Ann. Phys. Rehabil. Med. 2015, 58, 167–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pollock, A.; Gray, C.; Culham, E.; Durward, B.R.; Langhorne, P. Interventions for improving sit-to-stand ability following stroke. Cochrane Libr. 2014, CD007232. [Google Scholar] [CrossRef] [PubMed]
- Cheng, P.T.; Liaw, M.Y.; Wong, M.K.; Tang, F.T.; Lee, M.Y.; Lin, P.S. The sit-to-stand movement in stroke patients and its correlation with falling. Arch. Phys. Med. Rehabil. 1998, 79, 1043–1046. [Google Scholar] [CrossRef]
- Brière, A.; Lauzière, S.; Gravel, D.; Nadeau, S. Perception of weight-bearing distribution during sit-to-stand tasks in hemiparetic and healthy individuals. Stroke 2010, 41, 1704–1708. [Google Scholar] [CrossRef]
- Dehail, P.; Bestaven, E.; Muller, F.; Mallet, A.; Robert, B.; Bourdel-Marchasson, I.; Petit, J. Kinematic and electromyographic analysis of rising from a chair during a “sit-to-walk” task in elderly subjects: Role of strength. Clin. Biomech. 2007, 22, 1096–1103. [Google Scholar] [CrossRef]
- Blache, Y.; Pairot de Fontenay, B.; Monteil, K. The effects of seat height and foot placement on lumbar spine load during sit-to-stand tasks. Ergonomics 2014, 57, 1687–1695. [Google Scholar] [CrossRef]
- Khemlani, M.; Carr, J.; Crosbie, W. Muscle synergies and joint linkages in sit-to-stand under two initial foot positions. Clin. Biomech. 1999, 14, 236–246. [Google Scholar] [CrossRef]
- Brunt, D.; Greenberg, B.; Wankadia, S.; Trimble, M.A.; Shechtman, O. The effect of foot placement on sit to stand in healthy young subjects and patients with hemiplegia. Arch. Phys. Med. Rehabil. 2002, 83, 924–929. [Google Scholar] [CrossRef] [PubMed]
- Benjuya, N.; Melzer, I.; Kaplanski, J. Aging-induced shifts from a reliance on sensory input to muscle cocontraction during balanced standing. J. Gerontol. A-Biol. 2004, 59, M166–M171. [Google Scholar] [CrossRef]
- Ashford, S.; De Souza, L. A comparison of the timing of muscle activity during sitting down compared to standing up. Physiother. Res. Int. 2000, 5, 111–128. [Google Scholar] [CrossRef] [PubMed]
- Roebroeck, M.; Doorenbosch, C.; Harlaar, J.; Jacobs, R.; Lankhorst, G. Biomechanics and muscular activity during sit-to-stand transfer. Clin. Biomech. 1994, 9, 235–244. [Google Scholar] [CrossRef]
- Munton, J.; Ellis, M.; Wright, V. Use of electromyography to study leg muscle activity in patients with arthritis and in normal subjects during rising from a chair. Ann. Rheum. Dis. 1984, 43, 63. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.; Sousa, A.S.; Pinheiro, R.; Ferraz, J.; Tavares, J.M.R.; Santos, R.; Sousa, F. Activation timing of soleus and tibialis anterior muscles during sit-to-stand and stand-to-sit in post-stroke vs. Healthy subjects. Somatosens. Mot. Res. 2013, 30, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Cheng, P.T.; Chen, C.L.; Wang, C.M.; Hong, W.H. Leg muscle activation patterns of sit-to-stand movement in stroke patients. Am. J. Phys. Med. Rehabil. 2004, 83, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Camargos, A.C.R.; Rodrigues-de-Paula-Goulart, F.; Teixeira-Salmela, L.F. The effects of foot position on the performance of the sit-to-stand movement with chronic stroke subjects. Arch. Phys. Med. Rehabil. 2009, 90, 314–319. [Google Scholar] [CrossRef] [PubMed]
- Lu, R.-R.; Li, F.; Zhu, B. Electromyographical characteristics and muscle utilization in hemiplegic patients during sit-to-stand activity: An observational study. Eur. J. Phys. Rehabil. Med. 2016, 52, 186–194. [Google Scholar]
- Perotto, A.O. Anatomical Guide for the Electromyographer: The Limbs and Trunk; Charles C Thomas Publisher: Springfield, IL, USA, 2011. [Google Scholar]
- Wu, G.; Cavanagh, P.R. Isb recommendations for standardization in the reporting of kinematic data. J. Biomech. 1995, 28, 1257–1260. [Google Scholar] [CrossRef]
- Shao, Q.; Bassett, D.N.; Manal, K.; Buchanan, T.S. An emg-driven model to estimate muscle forces and joint moments in stroke patients. Comput. Biol. Med. 2009, 39, 1083–1088. [Google Scholar] [CrossRef] [PubMed]
- Jang, E.M.; Kim, M.H.; Yoo, W.G. Comparison of the tibialis anterior and soleus muscles activities during the sit-to-stand movement with hip adduction and hip abduction in elderly females. J. Phys. Ther. Sci. 2014, 26, 1045–1047. [Google Scholar] [CrossRef] [PubMed]
- Gross, M.M.; Stevenson, P.J.; Charette, S.L.; Pyka, G.; Marcus, R. Effect of muscle strength and movement speed on the biomechanics of rising from a chair in healthy elderly and young women. Gait Posture 1998, 8, 175–185. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Stroke | Healthy Controls | Mean Difference of 95% CI | p | |
|---|---|---|---|---|
| Initiation phase (s) | 0.987 ± 0.326 | 0.752 ± 0.161 | 0–0.286 | 0.100 |
| Ascending phase (s) | 1.329 ± 0.443 | 1.169 ± 0.343 | 0.096–0.704 | 0.400 |
| Total duration (s) | 2.315 ± 0.692 | 1.921 ± 0.457 | 0.016–0.584 | 0.300 |
| Seat-off (% STS Cycle) | 41.665 ± 7.557 | 38.985 ± 6.224 | 0.096–0.704 | 0.400 |
| Onset Timing of Muscular Activities 1 (% STS Cycle) Before Seat-Off (−)/After Seat-Off (+) | Stroke Group | Healthy Control Group | Mean Difference of 95% CI | p * | |
|---|---|---|---|---|---|
| TA | Unaffected/Dominant | −36.571 ± 18.147 | −46.959 ± 8.909 | 0–0.259 | 0.000 * |
| Affected/Non-Dominant | −36.855 ± 16.615 | −48.228 ± 12.007 | 0–0.286 | 0.100 | |
| ES | Unaffected/Dominant | −36.825 ± 10.245 | −45.091 ± 7.384 | 0–0.259 | 0.000 * |
| Affected/Non-Dominant | −39.344 ± 6.748 | −44.710 ± 7.665 | 0–0.286 | 0.100 | |
| RF | Unaffected/Dominant | −40.736 ± 7.973 | −39.837 ± 9.766 | 0.552–1 | 0.800 |
| Affected/Non-Dominant | −37.271 ± 10.834 | −41.581 ± 7.506 | 0.416–0.984 | 0.700 | |
| RA | Unaffected/Dominant | −35.642 ± 8.435 | −41.137 ± 11.190 | 0–0.286 | 0.100 |
| Affected/Non-Dominant | −34.486 ± 10.646 | −39.950 ± 10.531 | 0–0.286 | 0.100 | |
| BF | Unaffected/Dominant | −28.224 ± 12.302 | −39.766 ± 12.785 | 0–0.259 | 0.000 * |
| Affected/Non-Dominant | −33.951 ± 7.603 | −40.399 ± 11.814 | 0–0.286 | 0.100 | |
| GMax | Unaffected/Dominant | −17.489 ± 16.429 | −34.260 ± 8.927 | 0–0.259 | 0.000 * |
| Affected/Non-Dominant | −19.866 ± 14.707 | −37.987 ± 10.070 | 0–0.259 | 0.000 * | |
| GMed | Unaffected/Dominant | −25.665 ± 12.841 | −24.917 ± 18.036 | 0.552–1 | 0.800 |
| Affected/Non-Dominant | −18.894 ± 19.396 | −35.185 ± 12.176 | 0–0.259 | 0.000 * | |
| SOL | Unaffected/Dominant | −13.593 ± 17.658 | −27.577 ± 19.338 | 0–0.286 | 0.100 |
| Affected/Non-Dominant | −14.336 ± 16.630 | −9.497 ± 18.697 | 0.096–0.704 | 0.400 | |
| Peak Timing of Muscular Activities 1 (% STS Cycle) Before Seat-Off (−)/After Seat-Off (+) | Stroke Group | Healthy Control Group | Mean Difference of 95% CI | p * | |
|---|---|---|---|---|---|
| TA | Unaffected/Dominant | −18.703 ± 12.773 | −31.723 ± 8.477 | 0–0.259 | 0.000 * |
| Affected/Non-Dominant | −17.707 ± 11.124 | −30.025 ± 10.165 | 0–0.259 | 0.000 * | |
| ES | Unaffected/Dominant | −23.712 ± 10.698 | −30.430 ± 9.601 | 0–0.286 | 0.100 |
| Affected/Non-Dominant | −24.703 ± 6.502 | −25.734 ± 9.644 | 0.741–1 | 1.000 | |
| RF | Unaffected/Dominant | −24.055 ± 5.505 | −21.546 ± 13.073 | 0.741–1 | 1.000 |
| Affected/Non-Dominant | −18.447 ± 12.602 | −15.072 ± 18.552 | 0.741–1 | 1.000 | |
| RA | Unaffected/Dominant | −10.115 ± 13.512 | −21.668 ± 13.368 | 0–0.259 | 0.000 * |
| Affected/Non-Dominant | −7.560 ± 15.244 | −10.189 ± 24.503 | 0.296–0.904 | 0.600 | |
| BF | Unaffected/Dominant | 10.844 ± 17.547 | −14.749 ± 17.668 | 0–0.259 | 0.000 * |
| Affected/Non-Dominant | 6.582 ± 25.901 | −9.926 ± 24.706 | 0–0.286 | 0.100 | |
| GMax | Unaffected/Dominant | 6.005 ± 14.387 | −13.505 ± 20.714 | 0–0.259 | 0.000 * |
| Affected/Non-Dominant | 8.654 ± 15.792 | −11.925 ± 10.091 | 0–0.259 | 0.000 * | |
| GMed | Unaffected/Dominant | 9.535 ± 15.634 | −0.905 ± 20.152 | 0–0.286 | 0.100 |
| Affected/Non-Dominant | 12.330 ± 17.590 | −7.491 ± 16.485 | 0–0.259 | 0.000 * | |
| SOL | Unaffected/Dominant | 1.396 ± 13.690 | −16.481 ± 18.323 | 0–0.259 | 0.000 * |
| Affected/Non-Dominant | 7.390 ± 14.144 | 7.495 ± 16.692 | 0.714–1 | 0.900 | |
| Offset Timing of Muscular Activities 1 (% STS Cycle) Before Seat-Off (−)/After Seat-Off (+) | Stroke Group | Healthy Control Group | Mean Difference of 95% CI | p* | |
|---|---|---|---|---|---|
| TA | Unaffected/Dominant | 1.349 ± 13.577 | −5.163 ± 11.901 | 0.096–0.704 | 0.400 |
| Affected/Non-Dominant | 0.873 ± 19.117 | −10.364 ± 11.62 | 0–0.286 | 0.100 | |
| ES | Unaffected/Dominant | 21.354 ± 18.684 | 17.126 ± 12.246 | 0–0.286 | 0.100 |
| Affected/Non-Dominant | 29.609 ± 12.627 | 17.327 ± 24.381 | 0–0.286 | 0.100 | |
| RF | Unaffected/Dominant | 26.588 ± 12.493 | 23.056 ± 17.839 | 0.096–0.704 | 0.400 |
| Affected/Non-Dominant | 25.067 ± 13.036 | 28.773 ± 11.567 | 0.416–0.984 | 0.700 | |
| RA | Unaffected/Dominant | 33.775 ± 12.725 | 18.548 ± 22.487 | 0–0.259 | 0.000 * |
| Affected/Non-Dominant | 29.205 ± 18.689 | 16.927 ± 24.429 | 0–0.286 | 0.100 | |
| BF | Unaffected/Dominant | 34.419 ± 18.714 | 20.265 ± 13.054 | 0–0.259 | 0.000 * |
| Affected/Non-Dominant | 27.457 ± 16.333 | 21.007 ± 20.719 | 0.096–0.704 | 0.400 | |
| GMax | Unaffected/Dominant | 26.952 ± 18.733 | 8.986 ± 27.998 | 0–0.259 | 0.000 * |
| Affected/Non-Dominant | 33.920 ± 9.780 | 15.178 ± 16.764 | 0–0.259 | 0.000 * | |
| GMed | Unaffected/Dominant | 30.671 ± 17.243 | 27.750 ± 10.986 | 0.296–0.904 | 0.600 |
| Affected/Non-Dominant | 35.596 ± 14.294 | 13.07 ± 25.459 | 0–0.259 | 0.000 * | |
| SOL | Unaffected/Dominant | 16.286 ± 13.909 | 1.078 ± 21.193 | 0–0.259 | 0.000 * |
| Affected/Non-Dominant | 20.803 ± 17.615 | 18.199 ± 13.802 | 0.096–0.704 | 0.400 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, W.-C.; Chang, C.-C.; Lin, Y.-J.; Yang, F.-C.; Lin, L.-F.; Chou, K.-N. The Use of Wearable Sensors for the Movement Assessment on Muscle Contraction Sequences in Post-Stroke Patients during Sit-to-Stand. Sensors 2019, 19, 657. https://doi.org/10.3390/s19030657
Hsu W-C, Chang C-C, Lin Y-J, Yang F-C, Lin L-F, Chou K-N. The Use of Wearable Sensors for the Movement Assessment on Muscle Contraction Sequences in Post-Stroke Patients during Sit-to-Stand. Sensors. 2019; 19(3):657. https://doi.org/10.3390/s19030657
Chicago/Turabian StyleHsu, Wei-Chun, Chao-Chin Chang, Yi-Jia Lin, Fu-Chi Yang, Li-Fong Lin, and Kuan-Nien Chou. 2019. "The Use of Wearable Sensors for the Movement Assessment on Muscle Contraction Sequences in Post-Stroke Patients during Sit-to-Stand" Sensors 19, no. 3: 657. https://doi.org/10.3390/s19030657
APA StyleHsu, W. -C., Chang, C. -C., Lin, Y. -J., Yang, F. -C., Lin, L. -F., & Chou, K. -N. (2019). The Use of Wearable Sensors for the Movement Assessment on Muscle Contraction Sequences in Post-Stroke Patients during Sit-to-Stand. Sensors, 19(3), 657. https://doi.org/10.3390/s19030657