Vital Signs Prediction and Early Warning Score Calculation Based on Continuous Monitoring of Hospitalised Patients Using Wearable Technology

 , , , , ,
, , , , ,  and
and 
Abstract
:1. Introduction
2. Data Generation
2.1. Study Design
2.2. Study Population
2.3. Measuring Device
- Accelerometer (x, y and z-axis) (m/s) capable of detecting motion and the position of the body
- Pulse oximeter to measure the oxygen saturation (%)
- Photoplethysmograph (PPG) which is used in combination with the ECG to derive cuff-less, noninvasive blood pressure using pulse transit time (PTT) technique.
- 3-channel ECG from which the heart rate and respiration rate can be derived.
- Intercostal electromyography (EMG) electrodes to estimate the respiration based on muscle movement.
3. Methods
3.1. High-Rate EWS Computation
3.2. Vital Signs Time-Series Prediction
3.3. Local Learning of SVMs
3.3.1. Support Vector Machines
3.3.2. KNN-LS-SVM Regressor
- Given a test example , compute distances to all training examples and pick the nearest K neighbours;
- Train the LS-SVM model with the K nearest neighbours.
- Use the resulting regressor to estimate the output of .
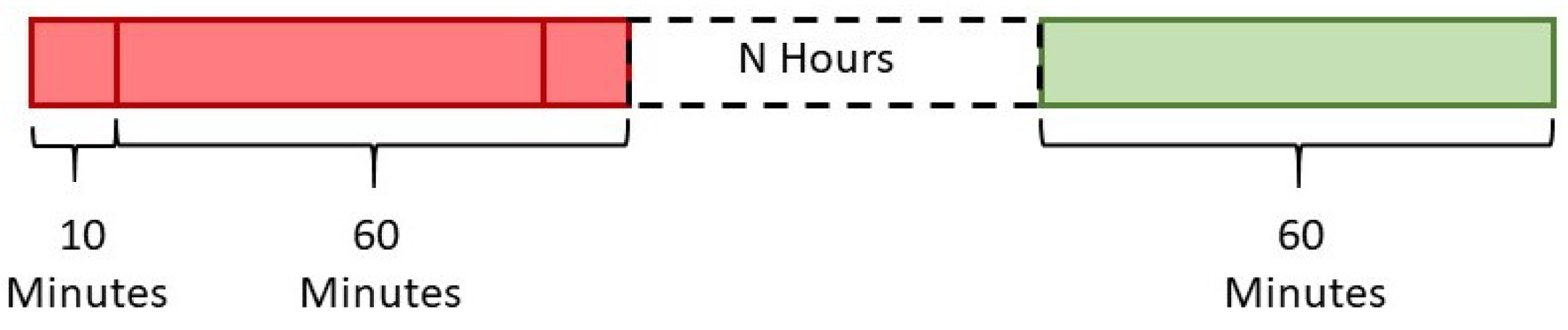
3.3.3. Prediction-Approach Design
4. Results
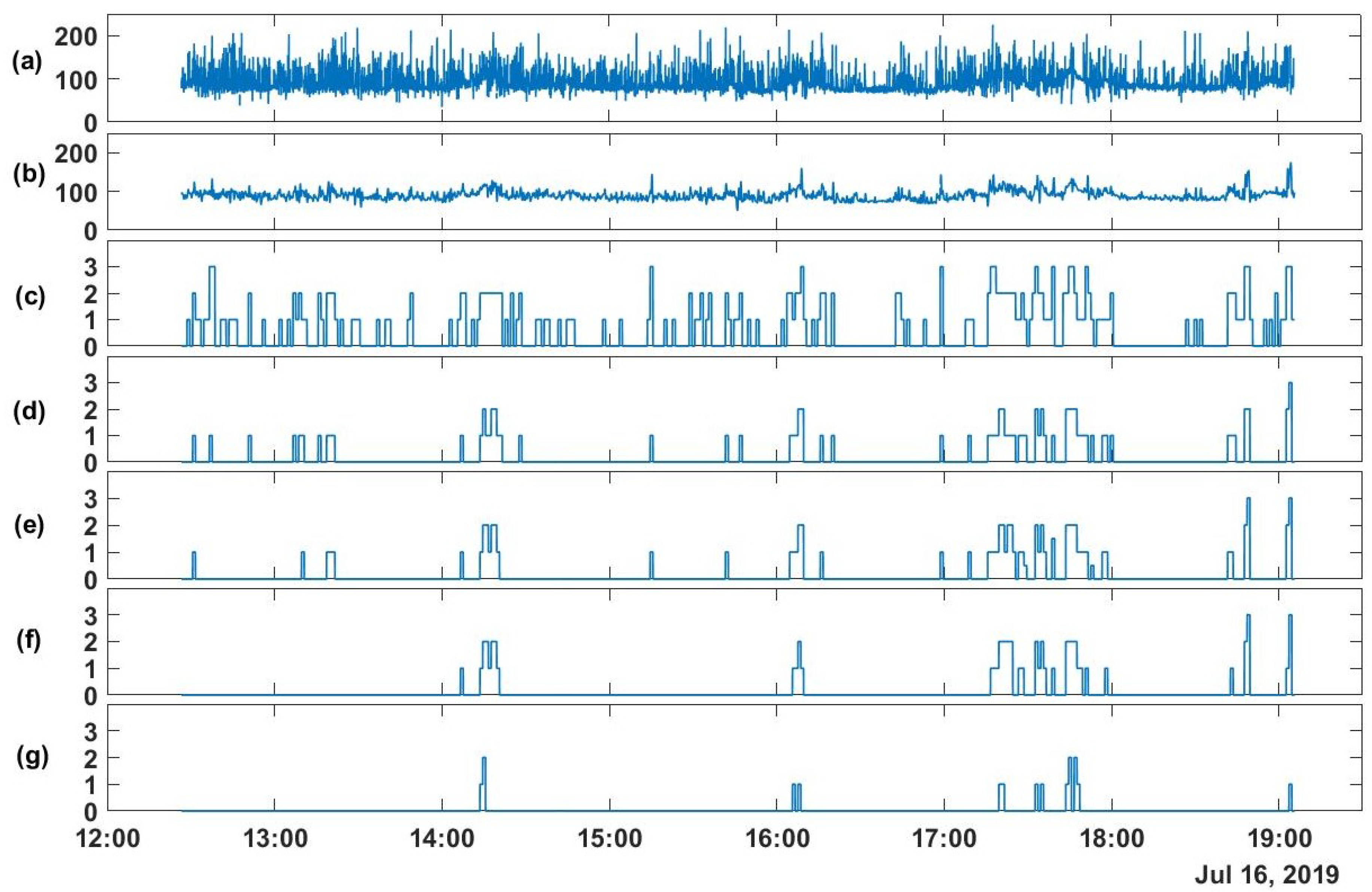
4.1. High-Rate EWS Computation
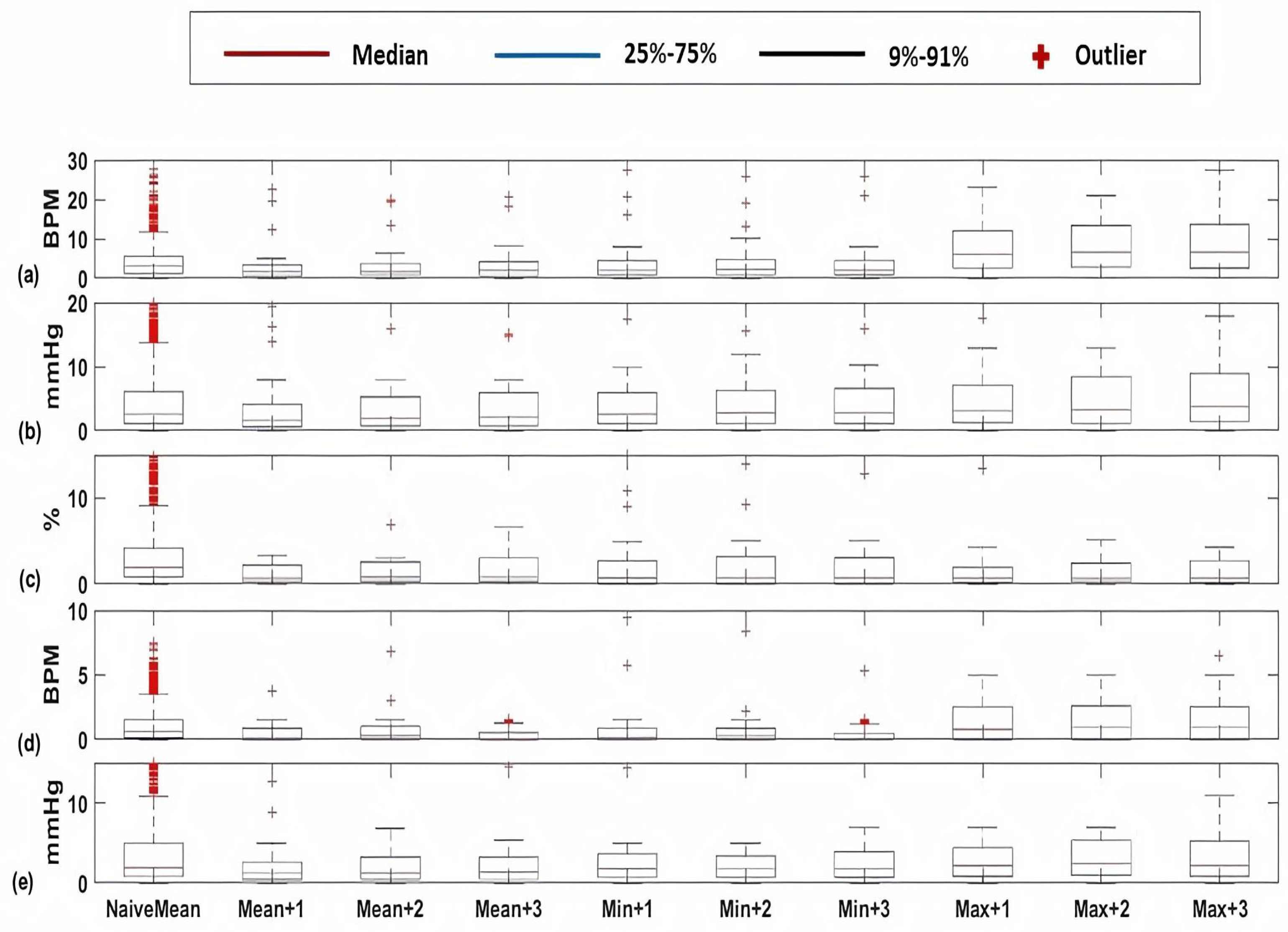
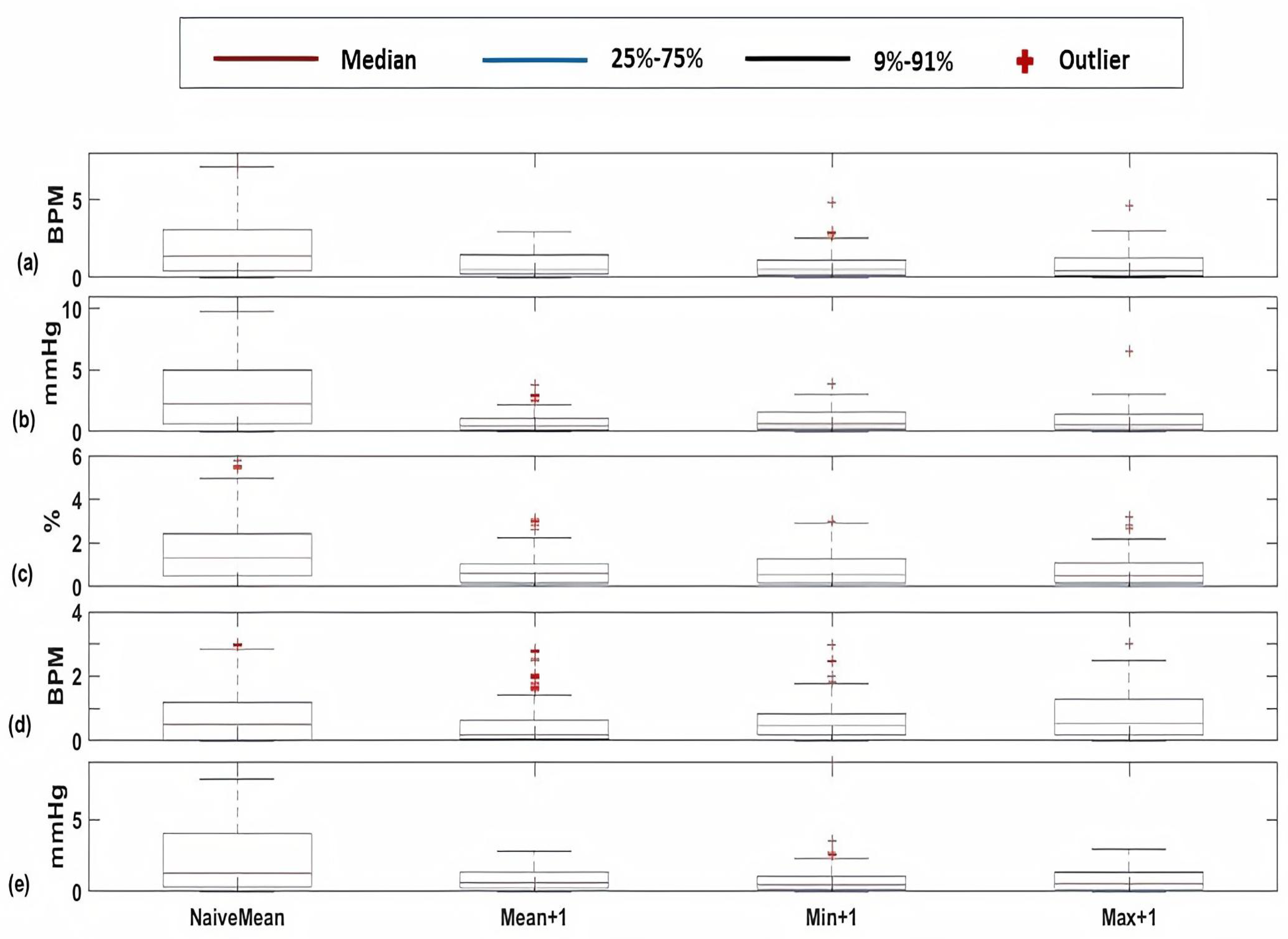
4.2. Vital Signs Time-Series Prediction
4.2.1. Cardiology and Postsurgical Patients
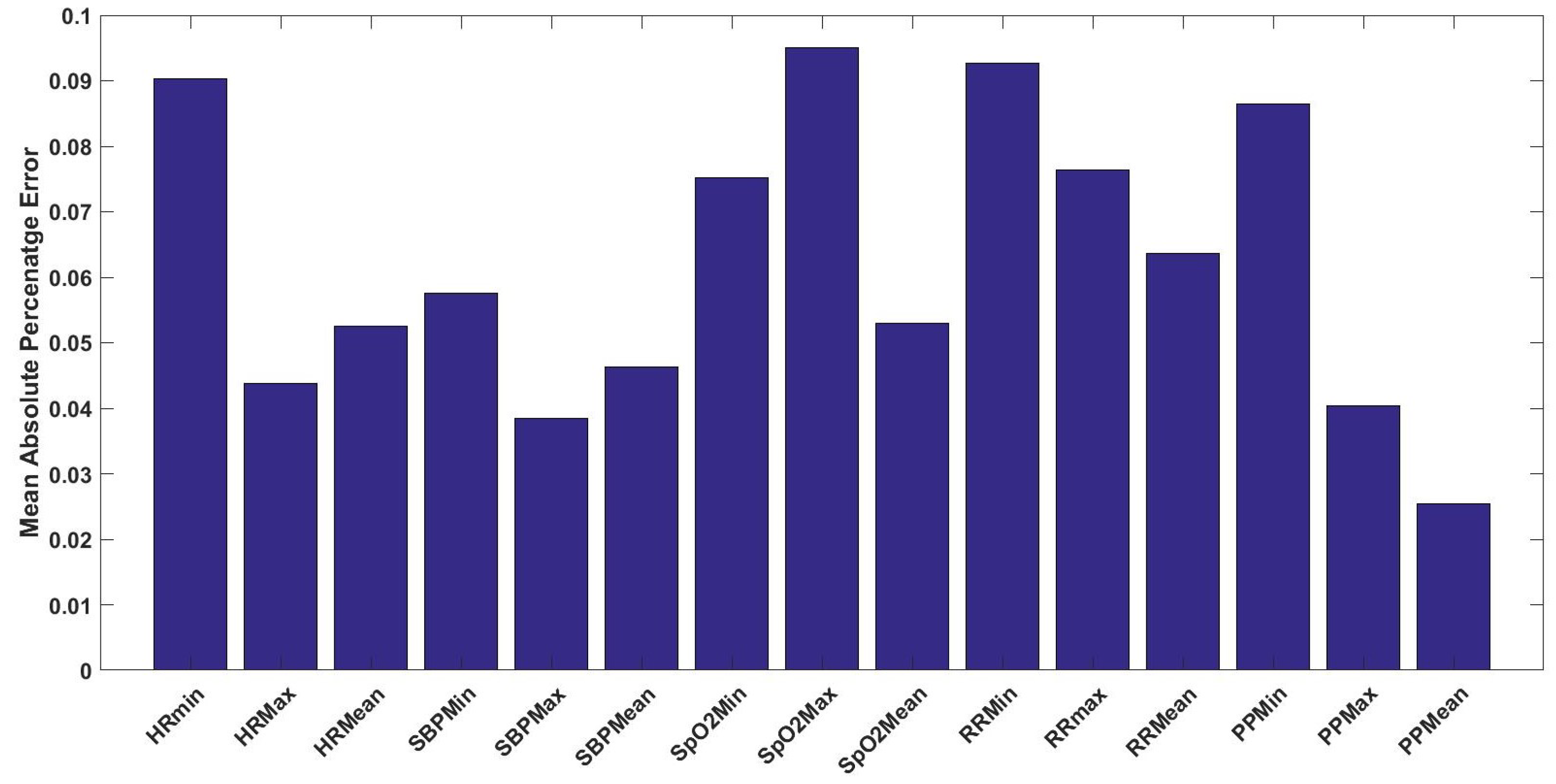
4.2.2. Dialysis Patients
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Brekke, I.J.; Puntervoll, L.H.; Pedersen, P.B.; Kellett, J.; Brabr, M. The value of vital sign trends in predicting and monitoring clinical deterioration: A systematic review. PLoS ONE 2019, 14. [Google Scholar] [CrossRef]
- Kause, J.; Smith, G.; Prytherch, D.; Parr, M.; Flabouris, A.; Hillman, K. A comparison of Antecedents to Cardiac Arrests, Deaths and EMergency Intensive care Admissions in Australia and New Zealand, and the United Kingdom—The ACADEMIA study. Resuscitation 2004, 62, 275–282. [Google Scholar] [CrossRef]
- Buist, M.; Bernard, S.; Nguyen, T.V.; Moore, G.; Anderson, J. Association between clinically abnormal observations and subsequent in-hospital mortality: A prospective study. Resuscitation 2004, 62, 137–141. [Google Scholar] [CrossRef]
- Hillman, K.M.; Bristow, P.J.; Chey, T.; Daffurn, K.; Jacques, T.; Norman, S.L.; Bishop, G.F.; Simmons, G. Antecedents to hospital deaths. Intern. Med. J. 2001, 31, 343–348. [Google Scholar] [CrossRef]
- Henriksen, D.P.; Brabr, M.; Lassen, A.T. Prognosis and risk factors for deterioration in patients admitted to a medical emergency department. PLoS ONE 2014, 9, e94649. [Google Scholar] [CrossRef]
- Barfod, C.; Lauritzen, M.M.P.; Danker, J.K.; Sölétormos, G.; Forberg, J.L.; Berlac, P.A.; Lippert, F.; Lundstrøm, L.H.; Antonsen, K.; Lange, K.H.W. Abnormal vital signs are strong predictors for intensive care unit admission and in-hospital mortality in adults triaged in the emergency department—A prospective cohort study. Scand. Trauma Resusc. Emerg. Med. 2012, 10, 20–28. [Google Scholar] [CrossRef] [Green Version]
- Javanbakht, M.; Mashayekhi, A.; Trevor, M.; Hemami, M.R.; Downey, C.L.; Branagan-Harris, M.; Atkinson, J. Cost utility analysis of continuous and intermittent versus intermittent vital signs monitoring in patients admitted to surgical wards. J. Med. Econ. 2020, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Fang, A.; Lim, W.; Balakrishnan, T. Early warning score validation methodologies and performance metrics: A systematic review. BMC Med. Inform. Decis. Mak. 2020, 20. [Google Scholar] [CrossRef] [PubMed]
- Petersen, O.A.; Kristian, A.; Larsn, S.R. Frequency of early warning score assessment and clinical deterioration in hospitalized patients: A randomized trial. Resuscitation 2016, 101, 43191–43196. [Google Scholar] [CrossRef] [PubMed]
- Downey, C.L.; Chapman, S.; Randell, R.; Brown, J.M.; Jayne, D.G. The impact of continuous versus intermittent vital signs monitoring in hospitals: A systematic review and narrative synthesis. Int. J. Nurs. Stud. 2018, 84, 19–27. [Google Scholar] [CrossRef] [Green Version]
- Reyna, M.A.; Josef, C.S.; Jeter, R.; Shashikumar, S.P.; Westover, M.B.; Nemati, S.; Clifford, G.D.; Sharma, A. Early prediction of sepsis from clinical data: The PhysioNet/Computing in Cardiology Challenge 2019. Crit. Care Med. 2019, 48, 210–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amer, A.Y.A.; Vranken, J.; Wouters, F.; Mesotten, D.; Vandervoort, P.; Storms, V.; Luca, S.; Vanrumste, B.; Aerts, J.-M. Feature Engineering for ICU Mortality Prediction Based on Hourly to Bi-Hourly Measurements. Appl. Sci. 2019, 9, 3525. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.; Yao, J.; Motani, M. Early Prediction of Vital Signs Using Generative Boosting via LSTM Networks. In Proceedings of the IEEE International Conference on Bioinformatics and Biomedicine (BIBM), San Diego, CA, USA, 18–21 November 2019; pp. 437–444. [Google Scholar]
- Amer, A.Y.A.; Aerts, J.M.; Vanrumste, B.; Luca, S. A Localised Learning Approach Applied to Human Activity Recognition. IEEE Intell. Syst. 2020, 99, 1. [Google Scholar]
- Amer, A.Y.A. Localised Least Squares Support Vector Machines with Appli-Cation to Weather Forecasting. Master’s Thesis, KU Leuven, Leuven, Belgium, 2016. [Google Scholar]
- Zifang, H.; Shyu, M.-L. k-NN based LS-SVM framework for long-term time series prediction. In Proceedings of the IEEE International Conference on Information Reuse and Integration, Las Vegas, NV, USA, 4–6 August 2010. [Google Scholar]
- Zifang, H.; Shyu, M.-L. Long-term time series prediction using k-NN based LS-SVM framework with multi-value integration. In Recent Trends in Information Reuse and Integration; Springer: Vienna, Austria, 2012; pp. 191–209. [Google Scholar]
- Bottou, L.; Vapnik, V. Local Learning Algorithms. Neural Comput. 1992, 4, 888–900. [Google Scholar] [CrossRef]
- Moon, A.; Cosgrove, J.F.; Lea, D.; Fairs, A.; Cressey, D.M. An eight year audit before and after the introduction of modified early warning score (MEWS) charts, of patients admitted to a tertiary referral intensive care unit after CPR. Resuscitation 2011, 82, 150–154. [Google Scholar] [CrossRef]
- Jarvis, S.; Kovacs, C.; Briggs, J.S.; Meredith, P.; Schmidt, P.E.; Featherstone, P.I.; Prytherch, D.R.; Smith, G.B. Aggregate National Early Warning Score (NEWS) values are more important than high scores for a single vital signs parameter for discriminating the risk of adverse outcomes. Resuscitation 2015, 87, 75–80. [Google Scholar] [CrossRef] [Green Version]
- Gao, H.; McDonnell, A.; Harrison, D.A.; Moore, T.; Adam, S.; Daly, K.; Esmonde, L.; Goldhill, D.R.; Parry, G.J.; Rashidian, A.; et al. Systematic review and evaluation of physiological track and trigger warning systems for identifying at-risk patients on the ward. Intensive Care Med. 2007, 33, 667–679. [Google Scholar] [CrossRef]
- Subbe, C.P.; Duller, B.; Bellomo, R. Effect of an automated notification system for deteriorating ward patients on clinical outcomes. Crit. Care 2017, 21, 52. [Google Scholar] [CrossRef] [Green Version]
- Smith, M.B.; Chiovaro, J.C.; O’Neil, M.; Kansagara, D.; Quiñones, A.R.; Freeman, M.; Motu’Apuaka, M.L.; Slatore, C.G. Early warning system scores for clinical deterioration in hospitalized patients: A systematic review. Ann. Am. Thorac. Soc. 2014, 11, 1454–1465. [Google Scholar] [CrossRef]
- Smith, M.E.B.; Chiovaro, J.C.; O’Neil, M.; Kansagara, D.; Quinones, A.; Freeman, M.; Motu’Apuaka, M.; Slatore, C.G. Early Warning System Scores: A Systematic Review. In VA Evidence-Based Synthesis Program Reports; Department of Veterans Affairs (US): Washington, DC, USA, 2014. [Google Scholar]
- Youssef, A.; Amer, A.Y.A.; Caballero, N.; Aerts, J.M. Towards Online Personalized-Monitoring of Human Thermal Sensation Using Machine Learning Approach. Appl. Sci. 2019, 9, 3303. [Google Scholar] [CrossRef] [Green Version]
- Cheng, H.; Tan, P.-N.; Jin, R. Localized support vector machine and its efficient algorithm. In Proceedings of the SIAM International Conference on Data Mining, Minneapolis, MN, USA, 26–28 April 2007. [Google Scholar]
- Bischl, B.; Schiffner, J.; Weihs, C. Benchmarking local classiffication methods. Comput. Stat. 2013, 28, 2599–2619. [Google Scholar] [CrossRef]
- Cheng, H.; Tan, P.; Jin, R. Efficient algorithm for localized support vector machine. IEEE Trans. Knowl. Data Eng. 2010, 22, 537–549. [Google Scholar] [CrossRef]
- Yang, H.; Huang, K.; King, I.; Lyu, M.R. Localized support vector regression for time series prediction. Neurocomputing 2009, 72, 10–12. [Google Scholar] [CrossRef]
- Karevan, Z.; Feng, Y.; Suykens, J. Moving least squares support vector machines for weather temperature prediction. In Proceedings of the European Symposium on Artificial Neural Networks, Bruges, Belgium, 26–28 April 2017. [Google Scholar]
- Berg, A.; Maire, M.; Malik, J. SVM-KNN: Discriminative Nearest Neighbor Classiffcation for Visual Category Recognition. In Proceedings of the IEEE Computer Society Conference on Computer Vision and Pattern Recognition (CVPR’06), New York, NY, USA, 7–22 June 2006; pp. 2126–2136. [Google Scholar]
- Suykens, J.A.K.; Vandewalle, J. Least Squares Support Vector Machine Classifiers. Neural Process. Lett. 1999, 9, 293–300. [Google Scholar] [CrossRef]
- Suykens, J.A.K.; De Brabanter, J.; Lukas, L.; Vandewalle, J. Weighted least squares support vector machines: Robustness and sparse approximation. Neurocomputing 2002, 48, 85–105. [Google Scholar] [CrossRef]
- Cayton, L. Fast nearest neighbor retrieval for bregman divergences. In Proceedings of the 25th International Conference on Machine Learning, Helsinki, Finland, 5–9 July 2008; pp. 112–119, ISBN 9781605582054. [Google Scholar] [CrossRef] [Green Version]
- Saeed, M.; Villarroel, M.; Reisner, A.T.; Clifford, G.; Lehman, L.W.; Moody, G.; Heldt, T.; Kyaw, T.H.; Moody, B.; Mark, R.G. Multiparameter Intelligent Monitoring in Intensive Care II (MIMIC-II): A public-access intensive care unit database. Crit. Care Med. 2011, 39, 952–960. [Google Scholar] [CrossRef] [Green Version]
- Johnson, A.E.W.; Pollard, T.J.; Shen, L.; Li-Wei, H.L.; Feng, M.; Ghassemi, M.; Moody, B.; Szolovits, P.; Celi, L.A.; Mark, R.G. MIMIC-III, a freely accessible critical care database. Sci. Data 2016, 3, 160035. [Google Scholar] [CrossRef] [Green Version]
- Lehman, L.-W.H.; Adams, R.P.; Mayaud, L.; Moody, G.B.; Malhotra, A.; Mark, R.G.; Nemati, S. A physiological time series dynamics-based approach to patient monitoring and outcome prediction. IEEE J. Biomed. Health Inform. 2015, 19, 1068–1076. [Google Scholar] [CrossRef]
- Reyes-García, J.; Galeana-Zapién, H.; Galaviz-Mosqueda, A.; Torres-Huitzil, A. Evaluation of the Impact of Data Uncertainty on the Prediction of Physiological Patient Deterioration. IEEE Access 2018, 6, 38595–38606. [Google Scholar] [CrossRef]
- Pimentel, M.A.F.; Clifton, D.A.; Clifton, L.; Watkinson, P.J.; Tarassenko, L. Modelling physiological deterioration in post-surgical patient vital-sign data. Med. Biol. Eng. Comput. 2013, 51, 869–877. [Google Scholar] [CrossRef] [Green Version]
- Clifton, L.; Clifton, D.A.; Watkinson, P.J.; Tarassenko, L. Identification of patient deterioration in vital-sign data using one-class support vector machines. In Proceedings of the Federated Conference on Computer Science and Information Systems (FedCSIS), Szczecin, Poland, 18–21 September 2011; pp. 125–131. [Google Scholar]
- Clifton, L.; Clifton, D.A.; Zhang, Y.; Watkinson, P.; Tarassenko, L.; Yin, H. Probabilistic novelty detection with support vector machines. IEEE Trans. Rel. 2014, 63, 455–467. [Google Scholar] [CrossRef]
- Luca, S.E.; Pimentel, M.A.F.; Watkinson, P.J.; Clifton, D.A. Point process models for novelty detection on spatial point patterns and their extremes. Comput. Stat. Data Anal. 2018, 125, 86–103. [Google Scholar] [CrossRef]
- Da Silva, D.B.; Schimidt, D.; DaCosta, C.A.; DaRosa, R.R.; Eskofier, B. DeepSigns: A predictive model based on Deep Learning for the early detection of patient health deterioration. Expert Syst. Appl. 2020, 165, 113905. [Google Scholar] [CrossRef]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SCORE | 3 | 2 | 1 | 0 | 1 | 2 | 3 |
|---|---|---|---|---|---|---|---|
| Temperature (C) | <35.1 | 35.1–36.5 | 36.6–37.5 | >37.5 | |||
| Heart Rate (BPM) | <40 | 40–50 | 51–100 | 101–110 | 111–130 | >130 | |
| Respiration Rate (BPM) | <9 | 9–14 | 15–20 | 21–30 | >30 | ||
| Oxygen Saturation (%) | <91 | 91–93 | 94–95 | >95 | |||
| Systolic Blood Pressure (mmHg) | <70 | 70–80 | 81–100 | 101–180 | 180–200 | >200 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Youssef Ali Amer, A.; Wouters, F.; Vranken, J.; de Korte-de Boer, D.; Smit-Fun, V.; Duflot, P.; Beaupain, M.-H.; Vandervoort, P.; Luca, S.; Aerts, J.-M.; et al. Vital Signs Prediction and Early Warning Score Calculation Based on Continuous Monitoring of Hospitalised Patients Using Wearable Technology. Sensors 2020, 20, 6593. https://doi.org/10.3390/s20226593
Youssef Ali Amer A, Wouters F, Vranken J, de Korte-de Boer D, Smit-Fun V, Duflot P, Beaupain M-H, Vandervoort P, Luca S, Aerts J-M, et al. Vital Signs Prediction and Early Warning Score Calculation Based on Continuous Monitoring of Hospitalised Patients Using Wearable Technology. Sensors. 2020; 20(22):6593. https://doi.org/10.3390/s20226593
Chicago/Turabian StyleYoussef Ali Amer, Ahmed, Femke Wouters, Julie Vranken, Dianne de Korte-de Boer, Valérie Smit-Fun, Patrick Duflot, Marie-Hélène Beaupain, Pieter Vandervoort, Stijn Luca, Jean-Marie Aerts, and et al. 2020. "Vital Signs Prediction and Early Warning Score Calculation Based on Continuous Monitoring of Hospitalised Patients Using Wearable Technology" Sensors 20, no. 22: 6593. https://doi.org/10.3390/s20226593
APA StyleYoussef Ali Amer, A., Wouters, F., Vranken, J., de Korte-de Boer, D., Smit-Fun, V., Duflot, P., Beaupain, M. -H., Vandervoort, P., Luca, S., Aerts, J. -M., & Vanrumste, B. (2020). Vital Signs Prediction and Early Warning Score Calculation Based on Continuous Monitoring of Hospitalised Patients Using Wearable Technology. Sensors, 20(22), 6593. https://doi.org/10.3390/s20226593