Bioimpedance Sensor and Methodology for Acute Pain Monitoring

 ,
, 
 ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
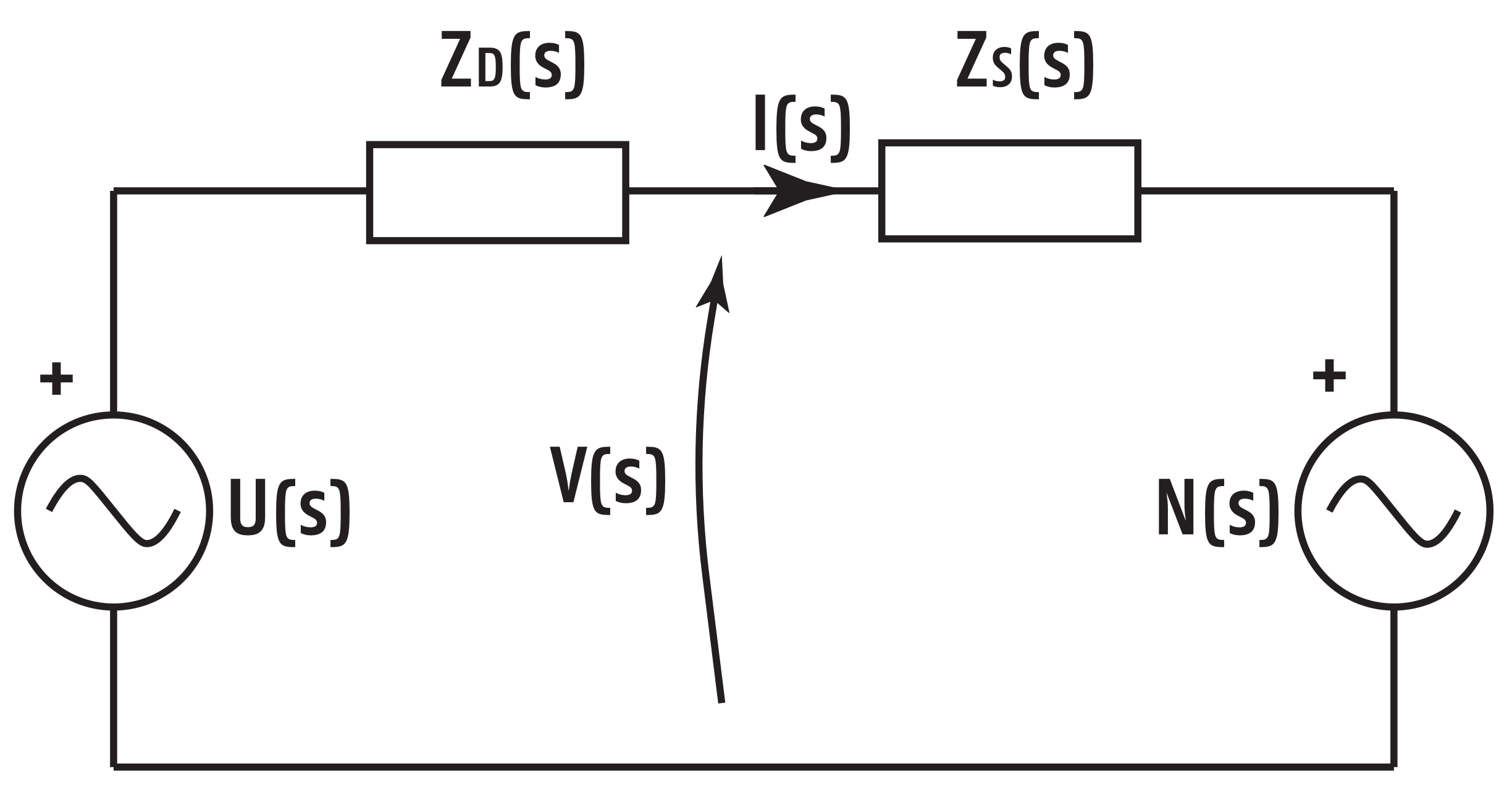
2.1. Background
2.2. Multisine Data-Analysis
2.3. Multisine Design
3. Results of Experimental Validation
3.1. Known Impedance Values
3.2. First Hand Results
- Minutes 1–5: The subject is in the nominal state, without applying any pain stimulation (NP1).
- Minute 6: Mechanical pain stimulation is applied by gripping the subject’s finger. The pain test is known as pressure test (P1).
- Minutes 7–9: The pain stimulation is ceased (NP2).
- Minutes 10–11: Mechanical pain stimulation is continuously applied as earlier (P2).
- Minutes 12–15: The pain stimulation is ceased (NP3).
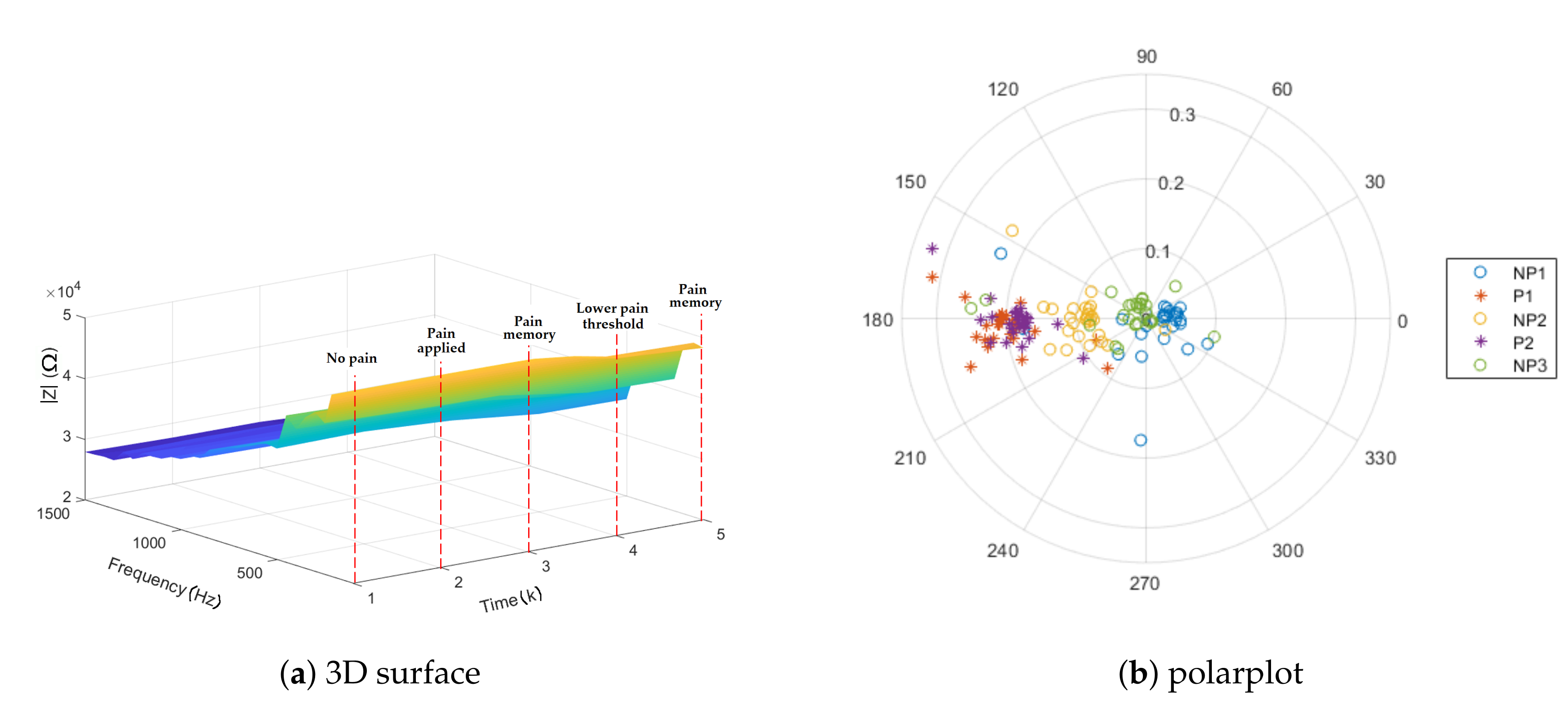
3.3. 3D Representation of Impedance
3.4. Repeatability and Impedance Dependence
- Minutes 1–2: The subject is in the nominal state, without applying any pain stimulation (NP1).
- Minutes 3–5: Thermal pain stimulation is produced by hand immersion in cold water (P1, P2, and P3).
- Minutes 6–8: The pain stimulation is ceased (NP2).
- Minutes 9–11: Thermal pain stimulation is continuously produced as earlier (P4, P5, and P6).
- Minutes 12–14: The pain stimulation is ceased (NP3).
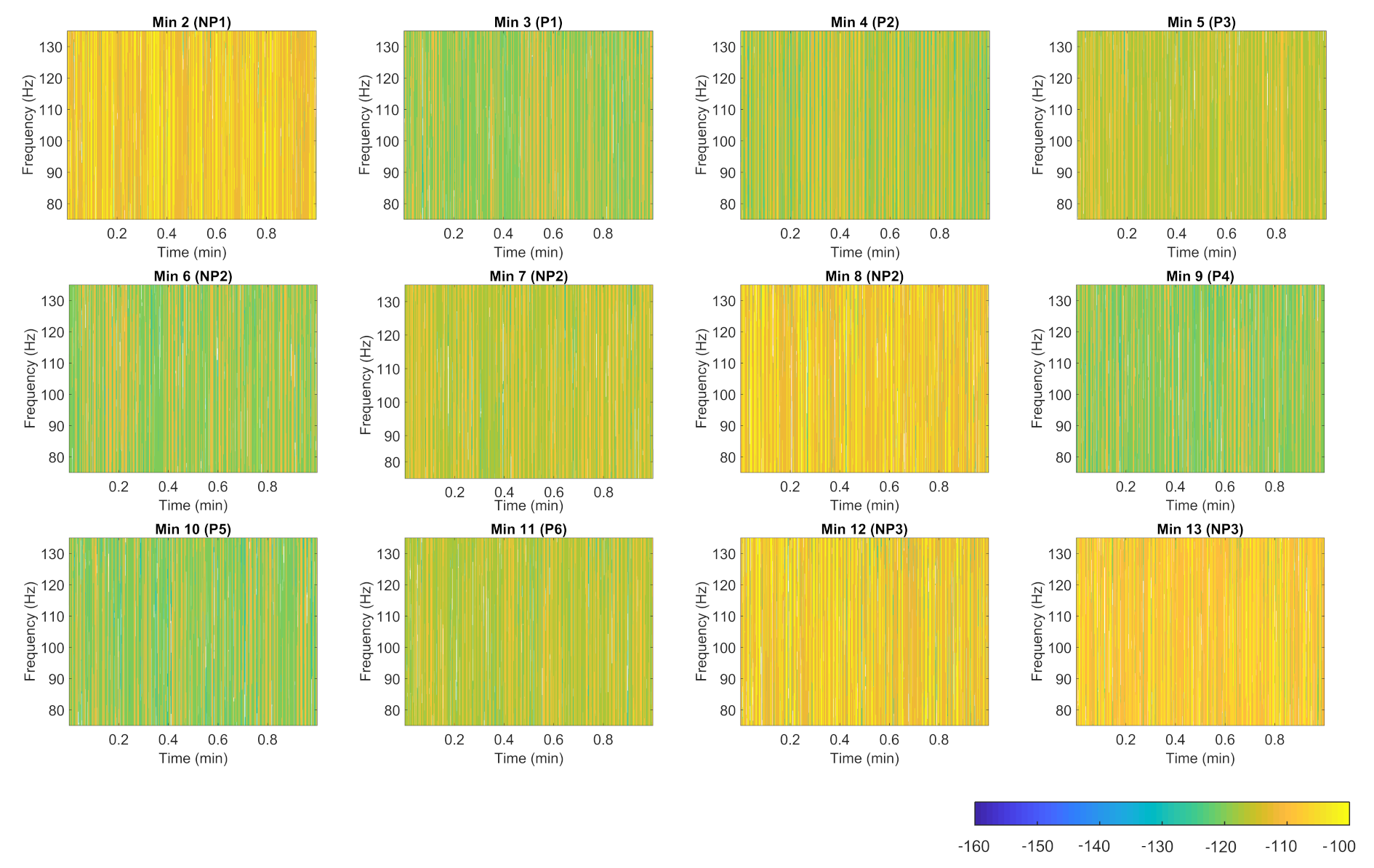
3.5. Spectrogram Representation
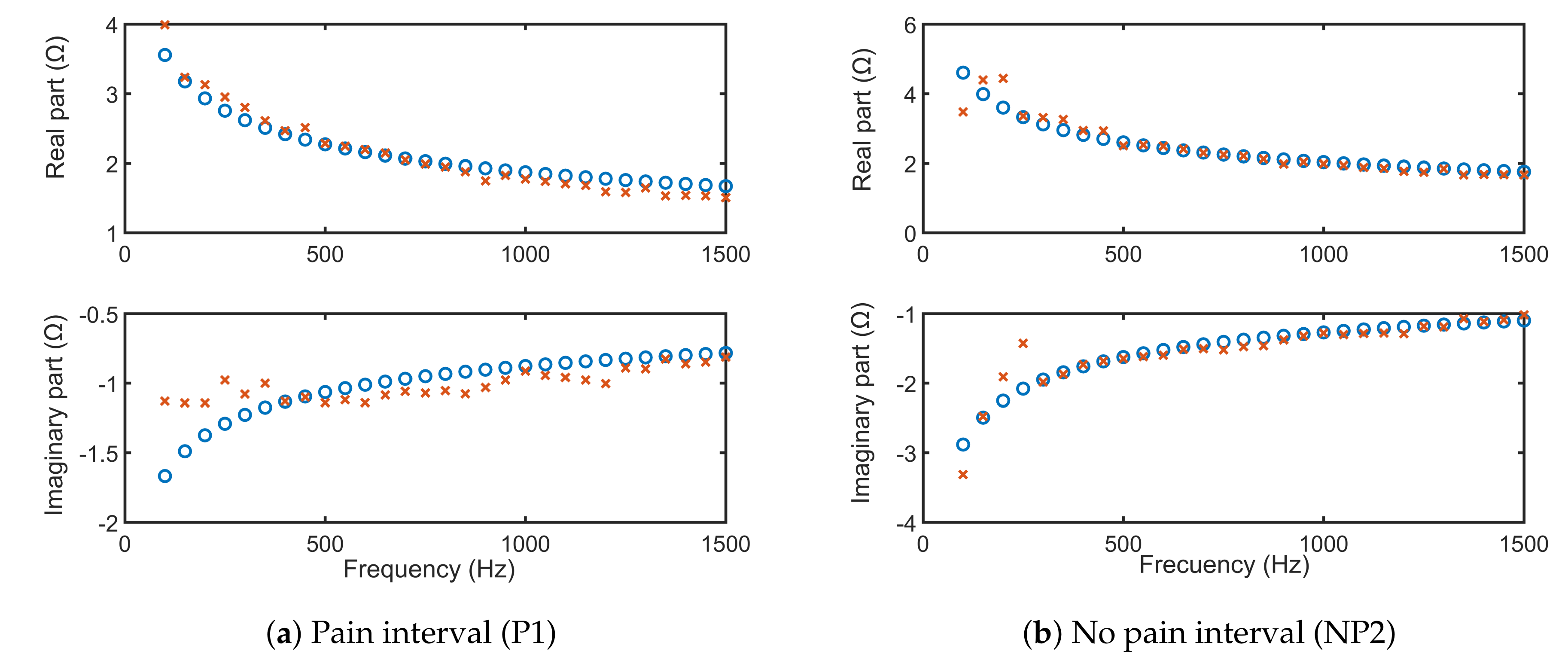
3.6. Bioimpedance Modeling
3.7. Other Features
- To investigate temperature tolerance of volunteers, the following hypotheses were tested on first Anspec-PRO: (i) the bioimpedance is increasing in time when the volunteer has one of his/her hands immersed in ice-cold water due to the new environment change and impact with ice-cold water; and (ii) the impedance of extracellular fluid is dependent on each individual after the threshold of pain is reached. The outcome of these measurements indicates that the device can successfully detect thermal pain. More details about this analysis can be found in [19].
- The authors also investigated detection of nociceptor stimulation followed by related tissue memory effects, using first Anspec-PRO. The method and model indicate that nociceptor stimulation perceived as pain in awake healthy volunteers is non-invasively detected. The existence of a memory effect is proven from measured data [18].
- Spectrographic analysis of the skin impedance measured with second Anspec-PRO device was approached to obtain a wider view towards the signal [20].
- Model identification was performed based on parametric methods. For identification purposes the multi-frequency voltage and corresponding current signals (multisine input–output) are used. More details about it can be found in [48].
4. Discussion
5. Conclusions and Perspectives
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AI | Analog Input |
| ADC | Analog-to-Digital Converter |
| AO | Analog Output |
| BIS | BioImpedance Spectroscopy |
| CE | Counter Electrode |
| cRIO | compactRIO |
| DAC | Digital-to-Analog Converter |
| EDA | Electrodermal Activity |
| FFT | Fast Fourier Transform |
| FRF | Frequency Response Function |
| FPGA | Field-Programmable Gate Array |
| GUI | Graphical User Interface |
| MSRE | Mean Square Root Error |
| Op Amp | Operational Amplifier |
| PSD | Power Spectra Density |
| RC | Circuit with both a resistor (R) and a capacitor (C) |
| RE | Reference Electrode |
| RMS | Root Mean Square |
| SC | Stratum Corneum |
| TIA | TransImpedance Amplifier |
| VB | Voltage Buffer |
| VS | Viable Skin |
| WE | Working Electrode |
Appendix A. Frequency Ranges

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Level | Frequency Range | Reference |
|---|---|---|
| Cells | 100 Hz to 1 MHz | [32] |
| 10–1 to 105 Hz | [33] | |
| Skin | 30 Hz–10 MHz | [57] |
| 20, 60, 100, 140, 180, 220 Hz | [58] | |
| 5 kHz to 1 MHz | [59] | |
| 10 Hz to 100 kHz | [60] | |
| Muscle | 0.02, 25.02, 50.02, 1000.02, 3000.02, and 5000.02 kHz | [57] |
| Entire body | 10 Hz, 1 kHz, 100 kHz, 10 MHz, 1 GHz, and 100 GHz | [35] |
| Bioelectrical impedance analysis | 5 to 1000 kHz | [36] |
| 100 Hz to 100 kHz | [37] | |
| 4–1000 Hz | [61] | |
| 32 to 992 kHz | [62] | |
| 30 Hz–10 MHz | [57] |
Appendix B. Hardware Components
- the data-acquisition unit (1) National Instruments’™ compactRIO connected to its power supply (3); and
- the signal conditioning circuit (2), also connected to its power supply (4).

- Data-acquisition is done with the embedded controller CompactRIO-9074 (cRIO) from National Instruments (Austin, Texas), which has a Field-Programmable Gate Array (FPGA) chip (Xilinx’ FPGA Spartan-3 1M), particularly useful for setups where a minimal robustness must be ensured for sending and acquiring signals in real-time. The FPGA is programmed within LabVIEW software. The National Instruments PS-15 Power Supply is used to power two C-series I/O modules:
- -
- Analog-to-Digital (ADC) converter as Analog Input (NI-9201): voltage input signals are scanned, buffered, conditioned, and then sampled by a single ADC.
- -
- Digital-to-Analog (DAC) converter as Analog Output (NI-9263): each channel of the Analog Output module has a DAC that produces a voltage signal.
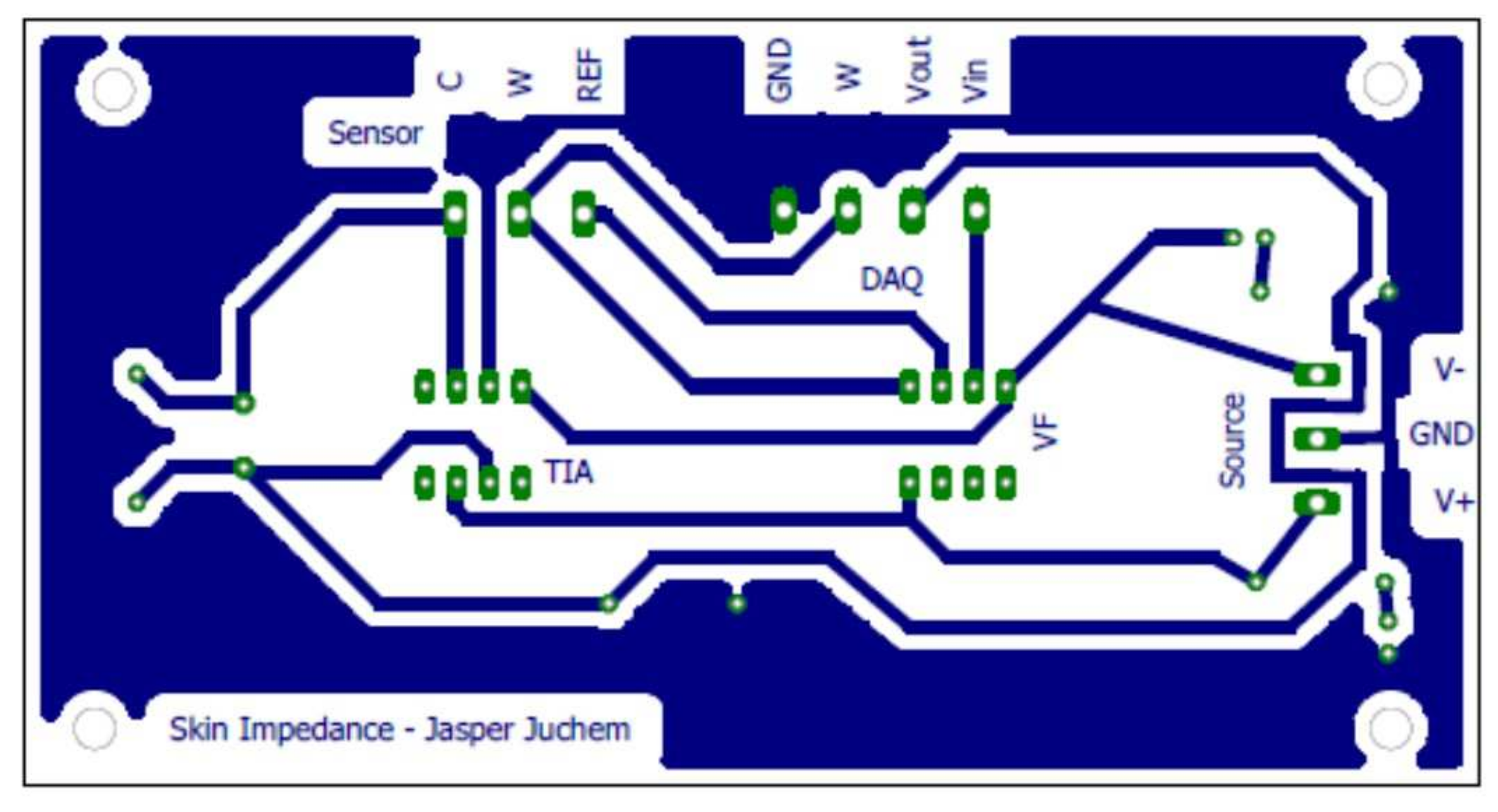
These are stand-alone data acquisition units and are used for converting the physical signal (analog) into a sequence of bits (digital signal) or vice versa. - Signal conditioning circuit is an interface between the computer and the electrodes, mitigating unwanted effects, such as noise or AC coupling. The signals coming from and going to National Instruments’ cRIO need to be conditioned before reaching the skin. This is done with a circuit containing operational amplifiers, which are connected to a DC power source with the voltage limited to V. The circuit encompasses:
- -
- Operational Amplifiers’ voltage source, in-house created for acquiring at least a +10 VDC and −10 VDC output compared to a common ground, as required by the I/O module manuals. An artificial Ground (GND) is created by the means of a galvanic separator, a transformer. However, to achieve the wanted supply voltages, a low drop-out voltage regulator is used to stabilize the output voltages. A rail with a positive voltage (MC7812) and with a negative voltage (MC7912), compared to this GND, are supplied to the voltage regulators, with the output voltage ±12 V.
- -
- Voltage Buffer (VB), which assures a correct voltage at the output of the circuit, being used just for transferring the voltage from the circuit to the skin. The active component is an Operational Amplifier (Op Amp) (Texas Instruments™ MC1458P). In a classic voltage buffer design, the output of the Op Amp is connected to the inverting supply, to achieve negative feedback. However, in this case, the voltage signal is first sent through a filter, namely the skin. The output signal is limited to ±15 V and ±25 mA.
- -
- TransImpedance Amplifier (TIA) circuit consists of an Op Amp (Analog Devices™ ADA4077), which, together with a resistor-capacitor circuit, allow transforming the current into a voltage. This process is motivated by the fact that ADC AI connected to cRIO can acquire only voltages, but current is also required for impedance calculations. However, by placing a resistance in the network, the current can be calculated from the measured voltage, based on Ohm’s law ().
| Module | Component | Manufacturer | Nr |
|---|---|---|---|
| cRIO | cRIO-9074 | National Instruments | 1 |
| cRIO | NI-9201 | National Instruments | 1 |
| cRIO | NI-9263 | National Instruments | 1 |
| cRIO | PS-125 | National Instruments | 1 |
| cRIO | Ethernet cable (5E - patched) | / | 2 |
| S | PCB | EELAB | 1 |
| S | 2way PCB Terminal Block | Phoenix | 1 |
| S | Transformer 15 V | Block | 1 |
| S | Diodes −400 V | ON Semiconductor | 6 |
| S | Electrolytic Capacitor (3300 nF–35 V) | United Chemi-Con | 2 |
| S | Voltage Regulator (+12 V/1 A) (MC7812) | ON Semiconductor | 1 |
| S | Voltage Regulator (−12 V/1 A) (MC7912) | ON Semiconductor | 1 |
| S | Electrolytic Capacitor (100 F–25 V) | Nichicon | 2 |
| S | Film Capacitor (0.1 F–63 V PET) | Kemet | 2 |
| S | Heat Sink TO-220 | AAVID-Thermalloy | 2 |
| S/VB | 3way PCB Terminal Block | Phoenix | 3 |
| VB | Op Amp MC1458P | Texas Instruments | 1 |
| VB | 4way PCB Terminal Block | Phoenix | 1 |
| VB | Audio Connector (3 contacts, Jack 3.5) | Pro Signal | 1 |
| VB | Sensor Cable (3 electrodes, Jack 3.5) | / | 1 |
| VB/TIA | PCB | Own Design | 1 |
| TIA | Op Amp ADA4077-2 | Analog Devices | 1 |
| TIA | Resistance (1000 –) | Velleman | 1 |
| TIA | Ceramic Capacitor (10 pF–50 V) | Kemet | 1 |
| Component | Electronic Specifications |
|---|---|
| ADC cRIO NI-9201 | Input range: V; 500 kS/s; ADC resolution: 12-Bit; Measurement voltage: V; Overvoltage protection V. |
| DAC cRIO NI-9263 | Output range: V; 100 kS/s/ch Simultaneous; DAC resolution: 16-Bit; Current drive: mA per channel maximum; Overvoltage protection: V. |
| NI LabVIEW FPGA Module | Loop rate of executable control algorithms up to 300 MHz. |
| Power Supply NI PS-15 | AC 100–120/200–240 V Auto-select input; The output terminals provide 24–28 VDC with 5 A of current. |
| TransImpedance Amplifier ADA4077-2 | Input Voltage Range: V; Output voltage range: 14 V; Output Current: mA; Gain Bandwidth: 3.6 MHz. |
| Voltage Buffer MC1458 | Input Voltage: V; Supply voltage: 15 V; Maximum-output-swing bandwidth (closed loop): 14 kHz; Unity Gain Bandwidth: 1 MHz; Short-circuit output current: mA; Supply current (both amplifiers): 3.4 mA. |


Appendix C. Software Architecture

- Before starting a new acquisition, all parameters are initialized and the graphs are cleared in the host program.
- The user manually introduces the analysis specific parameters and the path that indicates the location of the file containing the input/excitatory multisine signal.
- If the parameters are correctly assigned, the file is read and converted into an array with double precision numbers.
- All buffers are initialized and sufficient memory is allocated in order to avoid data overflow.
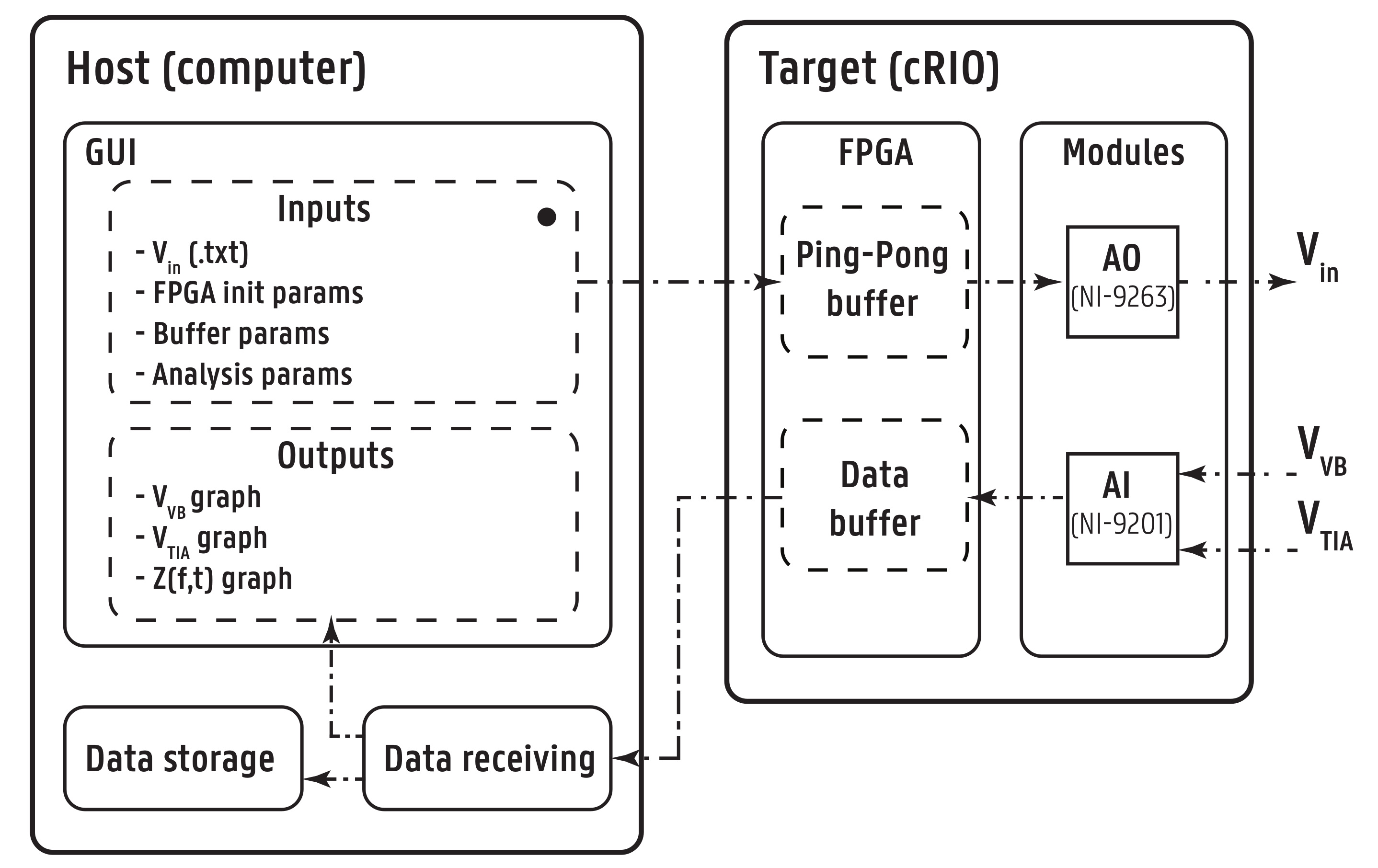
- The host sends the parameters and the signal array to FPGA target with the help of a First-In-First-Out (FIFO) Host to Target—Direct Memory Access (DMA) buffer, called Analog Output (AO). DMA makes it possible to transfer data from one hardware subsystem to another in real-time. The data are saved into another buffer AOH1 which is a Target-Scoped Block Memory FIFO buffer, with the same specifications of AO. Another buffer AOH2 is identical to buffer AOH1, hence both allow the ping-pong procedure explained below for the AO loop.
- If the host buffer is emptied and all data are copied on the target, the target software is ready for starting the data acquisition. The user receives a green-light in the graphical user interface (GUI) to start the data acquisition from the patient.
- Once the user starts the data acquisition, on the FPGA software, there are two parallel while loops: the Analog Output (AO) loop and the Analog Input (AI) loop:
- 7.1.
- In the AO loop, the input array enters the Ping-Pong Buffer. The array elements ping-pong between two buffers, one active and one passive.
- 7.2.
- With every sampling period , the active buffer is emptied element-wise and each value is sent to the output port (DAC module), while also saved in the passive buffer. When one buffer is filled, they interchange between being active and passive, thus creating a continuous periodic signal by repeatedly sending to the electrodes the same array of numerical values . This particular implementation architecture enables to continuously iterate through an array on the FPGA chip in delay-free real-time.
- 7.3.
- In parallel, the I/O hardware module measures the voltages from electrodes. With reference to Figure A3, AI modules acquire the voltage () from WE and the voltage of the output of TIA (), after being transformed from the bio-current by the active circuit implemented in the device.
- 7.4.
- The DAC from AI module transforms the analog signals into digital data.
- 7.5.
- For every sample from ADC, the two voltages, and , are stored in the Data Buffer, which is represented by two FIFO buffers: AIVoltage (for ) and AICurrent (for ). Pipeline method is used to guarantee that acquiring the voltage and writing it to the buffer is done simultaneously.
- 7.6.
- The Data Buffer is emptied in batches through a UTP cable into the Data Receiver, which is a container for all data on the host software.
- In parallel, a while loop on the host side starts reading all elements waiting in the Data Buffer (AIVoltage and AICurrent) into the Data Receiver. The measured voltage that describes the current is processed in the host software and the correct equivalent voltage is obtained. The data undergo a 180 phase shift, because the inverting properties of the op–amp, and the numerical values are divided by the resistance, which is 1000 .
- The while loop is stopped whenever an error is encountered or when the user presses the Stop button.
- The user can save the data in a file every on a specific location on the computer. The parameters and are plotted in real time in the GUI. The impedance is calculated and given in parallel with the data-acquisition and printed in the graphical user interface (GUI).
Appendix D. User Interface
- the input signal ;
- FPGA timer parameters;
- buffer allocation parameters; and
- parameters influencing the data analysis.

References
- Khalil, S.F.; Mohktar, M.S.; Ibrahim, F. The theory and fundamentals of bioimpedance analysis in clinical status monitoring and diagnosis of diseases. Sensors 2014, 14, 10895–10928. [Google Scholar] [CrossRef] [PubMed]
- Mayrovitz, H.N.; Gildenberg, S.R.; Spagna, P.; Killpack, L.; Altman, D.A. Characterizing the tissue dielectric constant of skin basal cell cancer lesions. Skin Res. Technol. 2018, 24, 686–691. [Google Scholar] [CrossRef] [PubMed]
- Hwang, H.J.; Ryu, M.Y.; Park, C.Y.; Ahn, J.; Park, H.G.; Choi, C.; Ha, S.D.; Park, T.J.; Park, J.P. High sensitive and selective electrochemical biosensor: Label-free detection of human norovirus using affinity peptide as molecular binder. Biosens. Bioelectron. 2017, 87, 16–170. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.K.; Kang, H.B. An analysis of fear of crime using multimodal measurement. Biomed. Signal Process. Control 2018, 41, 186–197. [Google Scholar] [CrossRef]
- Cannon, T.; Choi, J. Development of a segmental bioelectrical impedance spectroscopy device for body composition measurement. Sensors 2019, 19, 4825. [Google Scholar] [CrossRef] [Green Version]
- Naranjo-Hernández, D.; Reina-Tosina, J.; Roa, L.M.; Barbarov-Rostán, G.; Aresté-Fosalba, N.; Lara-Ruiz, A.; Cejudo-Ramos, P.; Ortega-Ruiz, F. Smart bioimpedance spectroscopy device for body composition estimation. Sensors 2020, 20, 70. [Google Scholar] [CrossRef] [Green Version]
- Rivas-Marchena, D.; Olmo, A.; Miguel, J.A.; Martínez, M.; Huertas, G.; Yùfera, A. Real-time electrical bioimpedance characterization of neointimal tissue for stent applications. Sensors 2017, 17, 1737. [Google Scholar] [CrossRef] [Green Version]
- Bari, D.S.; Yacoob-Aldosky, H.Y.; Tronstad, C.; Kalvøy, H.; Martinsen, Ø.G. Electrodermal activity responses for quantitative assessment of felt pain. J. Electr. Bioimpedance 2018, 9, 52–58. [Google Scholar] [CrossRef] [Green Version]
- Posada-Quintero, H.F.; Chon, K.H. Innovations in electrodermal activity data collection and signal processing: A systematic review. Sensors 2020, 20, 479. [Google Scholar] [CrossRef] [Green Version]
- Small, C.; Laycock, H. Acute postoperative pain management. Br. J. Surg. 2020, 107, e70–e80. [Google Scholar] [CrossRef]
- Glare, P.; Aubrey, K.R.; Myles, P.S. Transition from acute to chronic pain after surgery. Lancet 2019, 393, 1537–1546. [Google Scholar] [CrossRef]
- Bombardieri, A.M.; Mathur, S.; Soares, A.; Sharma, A.; Ben-Abdallah, A.; Wildes, T.; Avidan, M. Intraoperative awareness with recall: A descriptive, survey-based, cohort study. Anesth. Analg. 2019, 129, 1291–1297. [Google Scholar] [CrossRef] [PubMed]
- Storm, H.; Günther, A.; Sackey, P.V.; Bernhardsson, J.; Bäjrtå, A. Measuring pain—Physiological and self-rated measurements in relation to pain stimulation and anxiety. Acta Anesthesiol. Scand. 2019, 63, 668–675. [Google Scholar] [CrossRef] [PubMed]
- Martini, C.H.; Boon, M.; Broens, S.J.L.; Hekkelman, E.F.; Oudhoff, L.A.; Buddeke, A.W.; Dahan, A. Ability of the Nociception Level, a multiparameter composite of autonomic signals, to detect noxious stimuli during propofol–remifentanil anesthesia. Anesthesiology 2015, 123, 524–534. [Google Scholar] [CrossRef]
- Ledowski, T. Objective monitoring of nociception: A review of current commercial solutions. Br. J. Anaesth. 2019, 123, e312–e321. [Google Scholar] [CrossRef]
- Farhang, B.; Mathews, D.M. Pain monitor: Reality or fantasy in ambulatory patients. Curr. Opin. Anesthesiol. 2019, 32, 727–734. [Google Scholar] [CrossRef]
- Gruenewald, M.; Dempfle, A. Analgesia/nociception monitoring for opioid guidance: Meta-analysis of randomized clinical trials. Minerva Anestesiol. 2017, 83, 200–213. [Google Scholar] [CrossRef]
- Copot, D.; Ionescu, C.M. Models for nociception stimulation and memory effects in awake and aware healthy individuals. IEEE Trans. Biomed. Eng. 2019, 66, 718–726. [Google Scholar] [CrossRef]
- Ghita, M.; Ghita, M.; Copot, D.; Neckebroek, M.; Ionescu, C.M. Experimental Measurement of Pain Stimulus Effects in Skin Impedance. In Proceedings of the 22nd International Conference on Control Systems and Computer Science (CSCS), Bucharest, Romania, 28–30 May 2019; pp. 507–514. [Google Scholar] [CrossRef]
- Neckebroek, M.; Ghita, M.; Ghita, M.; Copot, D.; Ionescu, C.M. Pain detection with bioimpedance methodology from 3-dimensional exploration of nociception in a postoperative observational trial. J. Clin. Med. 2020, 9, 684. [Google Scholar] [CrossRef] [Green Version]
- Harder, R.; Diedrich, A.; Whitfield, J.S.; Buchowski, M.S.; Pietsch, J.B.; Baudenbacher, F.J. Smart multi-frequency bioelectrical impedance spectrometer for BIA and BIVA Applications. IEEE Trans. Biomed. Circuits Syst. 2016, 10, 912–919. [Google Scholar] [CrossRef] [Green Version]
- Kassanos, P.; Constantinou, L.; Triantis, I.F.; Demosthenos, A. An integrated analog readout for multi-frequency bioimpedance measurements. IEEE Sens. J. 2014, 14, 2792–2800. [Google Scholar] [CrossRef]
- Braun, R.; Mangana, J.; Goldinger, S.; French, L.; Dummer, R.; Marghoob, A. Electrical impedance spectroscopy in skin cancer diagnosis. Dermatol. Clin. 2017, 35, 489–493. [Google Scholar] [CrossRef] [PubMed]
- Grimnes, S.; Martinsen, Ø.G. Bioimpedance & Bioelectricity Basics, 3rd ed.; Elsevier Science Publishing Co. Inc.: London, UK, 2015. [Google Scholar]
- Freeborn, T.J.; Elwakil, A.S.; Maundy, B. Variability of Cole-model bioimpedance parameters using magnitude-only measurements of apples from a two-electrode configuration. Int. J. Food Prop. 2017, 20, S507–S519. [Google Scholar] [CrossRef]
- Abdulwadood, A.; Al-AliBrent, J.; Elwakil, S. Design and Implementation of Portable Impedance Analyzers, 1st ed.; Springer: Berlin/Heidelberg, Germany, 2019. [Google Scholar]
- Pintelon, R.; Schoukens, J. System Identification: A Frequency Domain Approach, 2nd ed.; John Wiley & Sons Inc.: Hoboken, NJ, USA, 2012. [Google Scholar]
- Talagas, M.; Lebonvallet, N.; Berthod, F.; Misery, L. Cutaneous nociception: Role of keratinocytes. Exp. Dermatol. 2019, 28, 1466–1469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamlih, A.; Freitas, P.; Belhaj, M.M.; Salles, J.; Kerzérho, V.; Soulier, F.; Bernard, S.; Rouyer, T.; Bonhommeau, S. A hybrid bioimpedance spectroscopy architecture for a wide frequency exploration of tissue electrical properties. In Proceedings of the IFIP/IEEE International Conference on Very Large Scale Integration (VLSI-SoC), Verona, Italy, 8–10 October 2018; pp. 168–171. [Google Scholar] [CrossRef] [Green Version]
- Hsiao, C.S.; Yang, Y.T.; Ching, T.S. Diagnosis of muscle properties in low-back-pain with electrical bioimpedance methodology. In Proceedings of the 3rd International Conference on Intelligent Technologies and Engineering Systems (ICITES2014); Springer: Cham, Switzerland, 2016; Volume 345, pp. 25–34. [Google Scholar] [CrossRef]
- Gabriel, C.; Peyman, A.; Grant, E. Electrical conductivity of tissue at frequencies below 1 MHZ. Phys. Med. Biol. 2009, 54, 4863–4867. [Google Scholar] [CrossRef]
- Mansor, M.A.; Takeuchi, M.; Nakajima, M.; Hasegawa, Y.; Ahmad, M.R. Electrical impedance spectroscopy for detection of cells in suspensions using microfluidic device with integrated microneedles. Appl. Sci. 2017, 7, 170. [Google Scholar] [CrossRef]
- Ho, J.S.; Lowb, J.H.; Simb, L.N.; Webstera, R.D.; Rice, S.A.; Fane, A.G.; Coster, H.G.L. In-situ monitoring of biofouling on reverse osmosis membranes: Detection and mechanistic study using electrical impedance spectroscopy. J. Membr. Sci. 2016, 518, 229–242. [Google Scholar] [CrossRef]
- Wang, Y.; Freedman, L.; Buck, M.; Bohorquez, J.; Rutkove, S.B.; Keel, J. Electrical impedance myography for assessing paraspinal muscles of patients with low back pain. J. Electr. Bioimpedance 2019, 10, 103–109. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Ma, R.; Wang, X.; Jin, J.; Wang, H.; Liu, Z.; Yin, T. Tissue coefficient as a novel index in bioelectric impedance analysis researches and applications. Biocybern. Biomed. Eng. 2020, 40, 950–964. [Google Scholar] [CrossRef]
- Ciumanghel, A.; Grigoras, I.; Siriopol, D.; Blaj, M.; Rusu, D.; Grigoras, G.R.; Igna, A.R.; Duca, O.; Siriopol, I.; Covic, A. Bio electrical impedance analysis for perioperative fluid evaluation in open major abdominal surgery. J. Clin. Monit. Comput. 2019, 34, 421–432. [Google Scholar] [CrossRef] [Green Version]
- Santoso, D.R.; Pitaloka, B.; Widodo, C.S.; Juswono, U.P. Low-cost, compact, and rapid bio-impedance spectrometer with real-time Bode and Nyquist plots. Appl. Sci. 2020, 10, 878. [Google Scholar] [CrossRef] [Green Version]
- de Castro, J.A.C.; de Lima, T.R.; Silva, D.A.S. Body composition estimation in children and adolescents by bioelectrical impedance analysis: A systematic review. J. Bodyw. Mov. Ther. 2018, 22, 134–136. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, B.; Pacheck, A.; Rutkovev, S.B. Guidelines to electrode positioning for human and animal electrical impedance myography research. Sci. Rep. 2016, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ionescu, C.M. Phase constancy in a ladder model neural dynamics. IEEE Trans. Syst. Man Cybern. 2012, 42, 1543–1551. [Google Scholar] [CrossRef]
- Ionescu, C.M.; Keyser, R.D.; Sabatier, J.; Oustaloup, A.; Levron, F. Low-frequency constant-phase behavior in the respiratory impedance. Biomed. Signal Process. Control 2011, 6, 197–208. [Google Scholar] [CrossRef]
- Jiang, Y.; Zhang, B.; Shu, X.; Wei, Z. Fractional-order autonomous circuits with order larger than one. J. Adv. Res. 2020, 25, 217–225. [Google Scholar] [CrossRef]
- Fu, B.; Freeborn, T.J. Cole-impedance parameters representing biceps tissue bioimpedance in healthy adults and their alterations following eccentric exercise. J. Adv. Res. 2020, 25, 285–293. [Google Scholar] [CrossRef]
- Shu, X.; Zhang, B.; Rong, C.; Jiang, Y. Frequency bifurcation in a series-series compensated fractional-order inductive power transfer system. J. Adv. Res. 2020, 25, 235–242. [Google Scholar] [CrossRef]
- Zhang, G.; Ou, Z.; Qu, L. A Fractional-Order Element (FOE)-based approach to wireless power transmission for frequency reduction and output power quality improvement. Electronics 2019, 8, 1029. [Google Scholar] [CrossRef] [Green Version]
- Ionescu, C.M. A memory-based model for blood viscosity. Commun. Nonlinear Sci. Numer. Simul. 2017, 45, 29–34. [Google Scholar] [CrossRef]
- Ionescu, C.M.; Kelly, J.F. Fractional calculus for respiratory mechanics: Power law impedance, viscoelasticity, and tissue heterogeneity. Chaos Solitons Fractals 2017, 102, 433–440. [Google Scholar] [CrossRef]
- Copot, D.; de Keyser, R.; Juchem, J.; Ionescu, C. Fractional order impedance model to estimate glucose concentration: In vitro analysis. Acta Politech. Hung. 2017, 14, 207–220. [Google Scholar]
- Niculescu, A.B.; Le-Niculescu, H.; Levey, D.F.; Roseberry, K.; Soe, K.C.; Rogers, J.; Khan, F.; Jones, T.; Judd, S.; McCormick, M.A.; et al. Towards precision medicine for pain: Diagnostic biomarkers and repurposed drugs. Mol. Psychiatry 2019, 24, 501–522. [Google Scholar] [CrossRef] [PubMed]
- Bear, M.F.; Connors, B.W.; Paradiso, M.A. Neuroscience. Exploring the Brain, 4th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2016. [Google Scholar]
- Geršak, G.; Drnovšek, J. Electrodermal activity patient simulator. PLoS ONE 2020, 15, e0228949. [Google Scholar] [CrossRef]
- Ionescu, C.M.; Lopes, A.; Copot, D.; Machado, J.A.T.; Bates, J.H.T. The role of fractional calculus in modelling biological phenomena: A review. Commun. Nonlinear Sci. Numer. Simul. 2017, 51, 141–159. [Google Scholar] [CrossRef]
- Ionescu, C.M.; Birs, I.R.; Copot, D.; Muresan, C.I.; Caponetto, R. Mathematical modelling with experimental validation of viscoelastic properties in non-Newtonian fluids. Philos. Trans. R. Soc. 2020, 378. [Google Scholar] [CrossRef]
- Copot, D. Automated Drug Delivery in Anesthesia, 1st ed.; Elsevier: London, UK, 2020. [Google Scholar]
- Zhou, Y.; Ionescu, C.; Tenreiro-Machado, J.A. Fractional dynamics and its applications. Nonlinear Dyn. 2015, 80, 1661–1664. [Google Scholar] [CrossRef] [Green Version]
- Ortigueira, M.D.; Ionescu, C.M.; Tenreiro-Machado, J.A.; Trujillo, J.J. Fractional signal processing and applications. Signal Process. 2015, 107, 197. [Google Scholar] [CrossRef]
- Ching, C.T.S.; Chen, Y.C.; Lu, L.H.; Hsieh, P.F.; Hsiao, C.S.; Sun, T.P.; Shieh, H.L.; Chang, K.M. Characterization of the muscle electrical properties in low back pain patients by electrical impedance myography. PLoS ONE 2013, 8, e61639. [Google Scholar] [CrossRef] [Green Version]
- Johnson, M.I.; Tabasam, G. An investigation in to the analgesic effects of different frequencies of the amplitude-modulated wave of interferential current therapy on cold-induced pain in normal subjects. Arch. Phys. Med. Rehabil. 2003, 84, 1387–1394. [Google Scholar] [CrossRef]
- Forouzanfar, T.; Kessels, A.G.H.; van Kleef, M.; Weber, W.; van Kreel, B.K. Multi-frequency bioelectrical impedance measurement in complex regional pain syndrome type I. Pilot study of 28 patients. Pain Clin. 2001, 31, 211–221. [Google Scholar] [CrossRef]
- Pliquett, U.; Prausnitz, M.R. Electrical impedance spectroscopy for rapid and noninvasive analysis of skin electroporation. In Electrochemotherapy, Electrogenetherapy, and Transdermal Drug Delivery; Series: Methods in Molecular Medicine; Jaroszeski, M.J., Heller, R., Gilbert, R., Eds.; Humana Press, Inc.: Totowa, NJ, USA, 2000; pp. 377–406. [Google Scholar] [CrossRef]
- Kenworthy, P.; Grisbrook, T.L.; Phillips, M.; Gittings, P.; Wooda, F.M.; Gibson, W.; Edgar, D.W. Bioimpedance spectroscopy: A technique to monitor interventions for swelling in minor burns. Burns 2017, 43, 1725–1735. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Zhang, F.; Tao, K.; Wang, L.; Wen, H.; Teng, Z. Multi-frequency simultaneous measurement of bioimpedance spectroscopy based on a low crest factor multisine excitation. Physiol. Meas. 2015, 36, 489–501. [Google Scholar] [CrossRef] [PubMed]
- European Commission—Health Technology and Cosmetics. MEDDEV 2.7/1 Revision 4: Guidelines on Medical Devices, 2016. Clinical Evaluation: A Guide for Manufacturers and Notified Bodies under Directives 93/42/EEC and 90/385/EEC. Available online: https://ec.europa.eu/docsroom/documents/17522/attachments/1/translations/en/renditions/native (accessed on 25 January 2017).
















| # Volunteer | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Gender | M | F | F | M | F | M | M | F | F | M | M | M | M |
| Age (Year) | 24 | 22 | 40 | 24 | 24 | 22 | 24 | 27 | 27 | 25 | 33 | 23 | 23 |
| Weight (kg) | 57 | 110 | 102 | 55 | 53 | 65 | 67 | 71 | 68 | 63 | 65 | 70 | 76 |
| Height (cm) | 164 | 160 | 174 | 160 | 165 | 170 | 173 | 180 | 178 | 180 | 165 | 175 | 196 |
| Fat (%) | 14.75 | 51.22 | 44.22 | 15.10 | 23.48 | 15.84 | 16.18 | 27.1 | 26.56 | 20.04 | 19.44 | 16.51 | 12.83 |
| BMI | 21.19 | 42.96 | 33.69 | 21.48 | 19.46 | 22.49 | 22.38 | 21.91 | 21.46 | 19.44 | 23.87 | 22.85 | 19.78 |
| Interval | L | C | ||||
|---|---|---|---|---|---|---|
| P1 | 0.099 | 0.008 | 0.430 | 29.075 | 0.062 | 131.7889 |
| NP2 | 0.155 | 0.002 | 0.527 | 102.276 | 2904.545 | 0.0009 |
| Interval | R | ||
|---|---|---|---|
| P1 | 2.683 × 10 | 23.732 | 0.279 |
| NP2 | 5.437 × 10 | 53.857 | 0.356 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghita, M.; Neckebroek, M.; Juchem, J.; Copot, D.; Muresan, C.I.; Ionescu, C.M. Bioimpedance Sensor and Methodology for Acute Pain Monitoring. Sensors 2020, 20, 6765. https://doi.org/10.3390/s20236765
Ghita M, Neckebroek M, Juchem J, Copot D, Muresan CI, Ionescu CM. Bioimpedance Sensor and Methodology for Acute Pain Monitoring. Sensors. 2020; 20(23):6765. https://doi.org/10.3390/s20236765
Chicago/Turabian StyleGhita, Mihaela, Martine Neckebroek, Jasper Juchem, Dana Copot, Cristina I. Muresan, and Clara M. Ionescu. 2020. "Bioimpedance Sensor and Methodology for Acute Pain Monitoring" Sensors 20, no. 23: 6765. https://doi.org/10.3390/s20236765
APA StyleGhita, M., Neckebroek, M., Juchem, J., Copot, D., Muresan, C. I., & Ionescu, C. M. (2020). Bioimpedance Sensor and Methodology for Acute Pain Monitoring. Sensors, 20(23), 6765. https://doi.org/10.3390/s20236765