Which Are the Central Aspects of Infant Sleep? The Dynamics of Sleep Composites across Infancy


Abstract
:1. Introduction
- The goal of this study was to first extend the approach of Staples et al. to an infant dataset and to, secondly, facilitate variable selection for future sleep studies;
- We therefore included 48 single sleep variables, which thoroughly characterize the diverse dimensions of sleep, and then performed a component analysis to identify the core infant sleep composites;
- We then examined the evolution of the sleep composites across repeated assessments throughout the first year of life and also tested for sex differences in the sleep composites. Additionally, we explored the stability of composites as well as the stability of the single sleep variables;
- Finally, to evaluate the relevance of sleep for development and to identify maturational markers, we linked sleep composites to infant behavioral developmental scores.
2. Materials and Methods
2.1. Participants
2.2. Experimental Design
2.3. Behavioral Development
2.4. Sleep Analysis
2.4.1. Sleep–Wake-Behavior
2.4.2. Handling of Missing Data
2.4.3. Calculation of Sleep Variables
2.4.4. Data Imputation
2.4.5. Sleep Composites
3. Results
3.1. Five Principal Components Express All Infant Sleep Variables: Infant Sleep Composites
- Sleep Activity—Larger values reflect more movements and more awakenings during the night as well as less regularity of awakenings. The most representative (i.e., with highest loading) single variable were Sleep Efficiency (negative) or Longest Nocturnal Wake (positive);
- Sleep Timing—Larger values reflect later clock time of bed times and sleep times. The most representative single variable was Sleep Offset;
- Sleep Night—Larger values reflect longer nighttime sleep opportunity and longer nighttime sleep duration. The most representative single variable was Sleep Period;
- Sleep Day—Larger values reflect longer daytime sleep duration, more daytime naps, and lower regularity in daytime sleep. The most representative variables were Longest Wake (negatively) or Nap Counter (positively);
- Sleep Variability—Larger values reflect higher variability between measurement days (standard deviation) within Sleep Timing and Sleep Night. The most representative single variable was Variability of Sleep Opportunity.
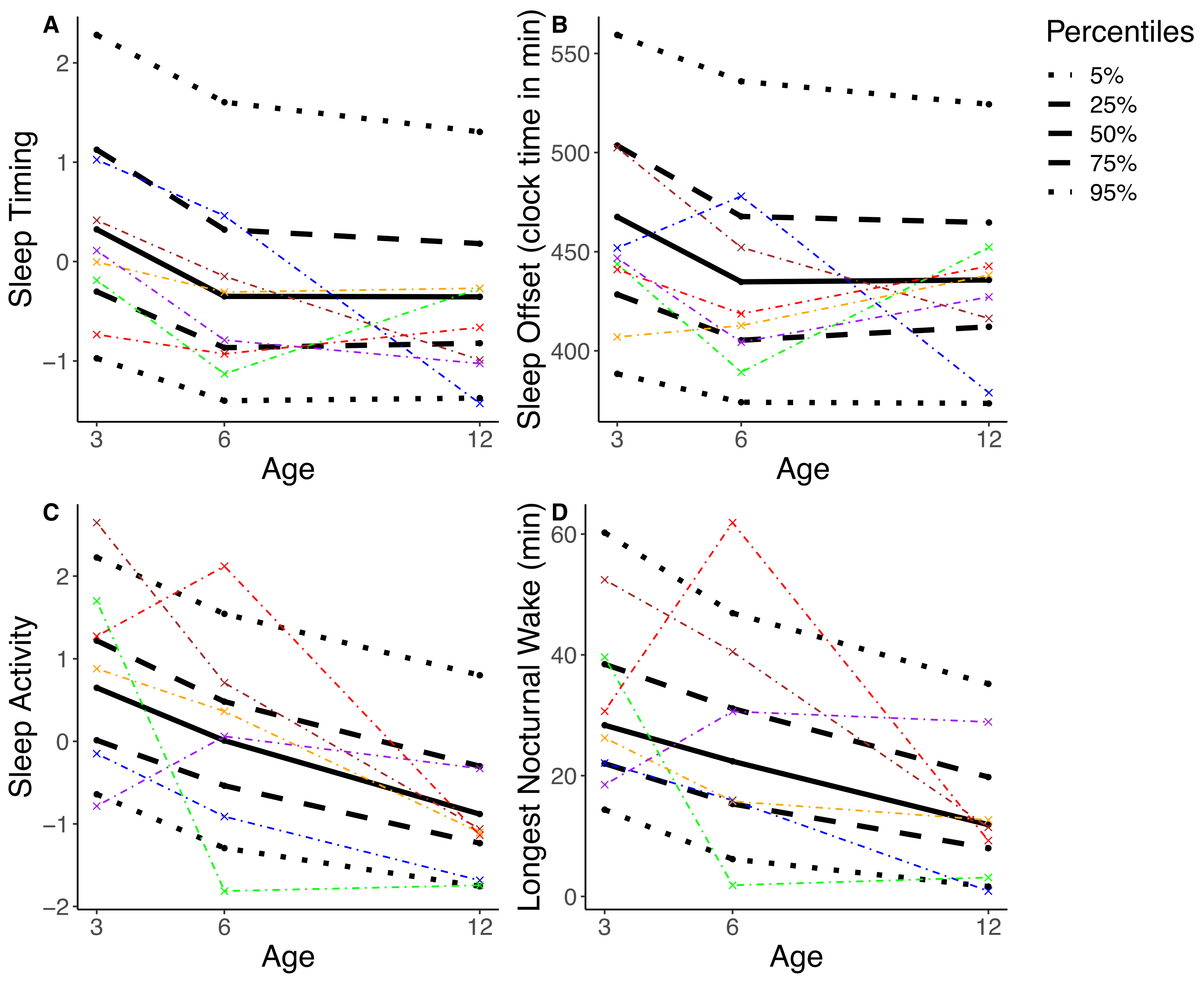
3.2. Sleep Composites Accurately Reflect Sleep Maturation Across Infancy
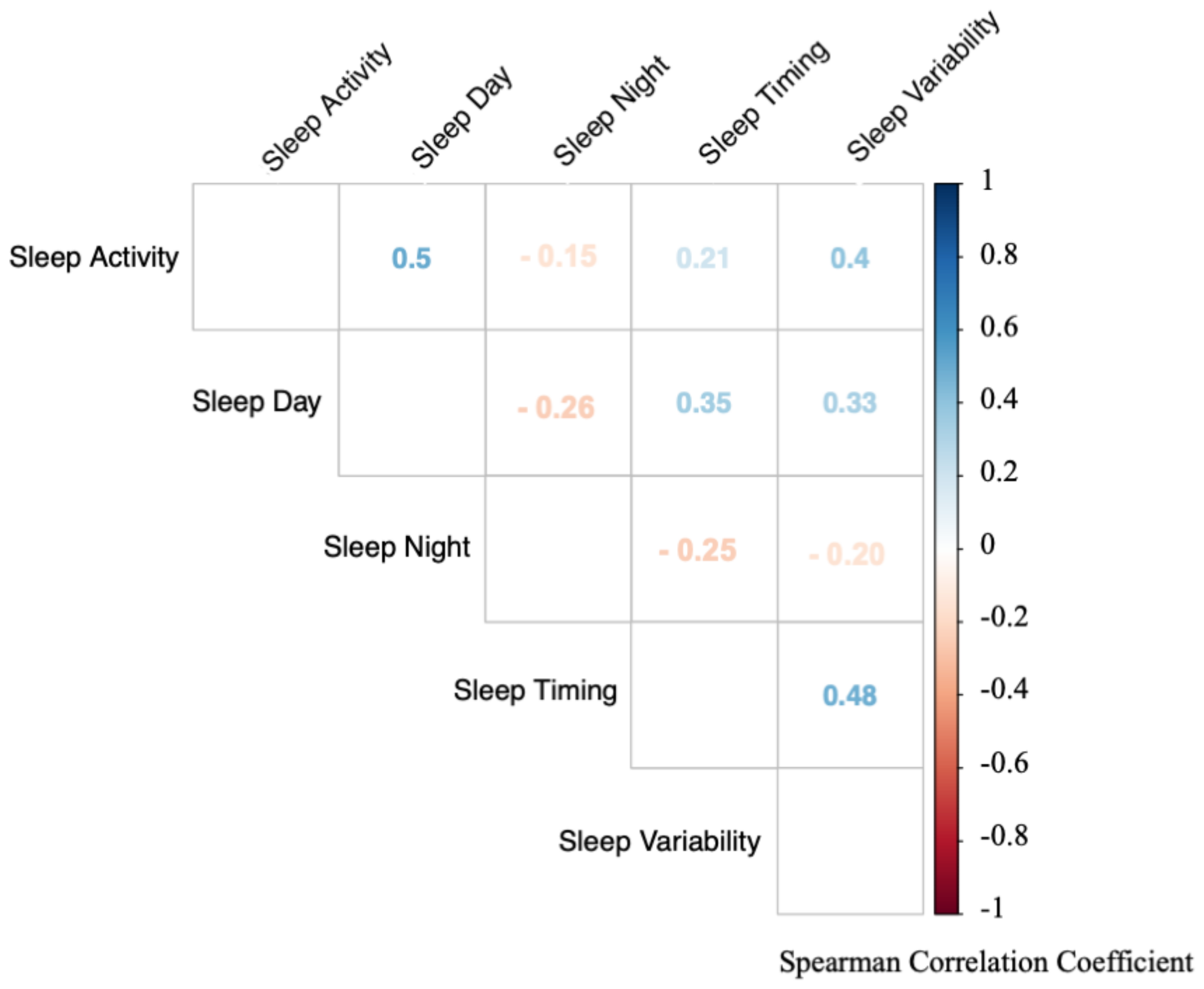
3.3. Strong Correlations between the Sleep Composites
3.4. Stability of Sleep Composites
3.5. Stability of Sleep Composites vs. Single Sleep Variables
3.6. Association of Sleep Composite with Behavioral Development
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
References
- Iglowstein, I.; Jenni, O.G.; Molinari, L.; Largo, R.H. Sleep Duration from Infancy to Adolescence: Reference Values and Generational Trends. Pediatrics 2003, 111, 302–307. [Google Scholar] [CrossRef]
- Kurth, S.; Ringli, M.; Geiger, A.; LeBourgeois, M.; Jenni, O.G.; Huber, R. Mapping of Cortical Activity in the First Two Decades of Life: A High-Density Sleep Electroencephalogram Study. J. Neurosci. 2010, 30, 13211–13219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feinberg, I.; Campbell, I.G. Sleep EEG changes during adolescence: An index of a fundamental brain reorganization. Brain Cogn. 2010, 72, 56–65. [Google Scholar] [CrossRef]
- Cao, J.; Herman, A.B.; West, G.B.; Poe, G.R.; Savage, V.M. Unraveling why we sleep: Quantitative analysis reveals abrupt transition from neural reorganization to repair in early development. Sci. Adv. 2020, 6, eaba0398. [Google Scholar] [CrossRef] [PubMed]
- Friedrich, M.; Mölle, M.; Friederici, A.D.; Born, J. Sleep-dependent memory consolidation in infants protects new episodic memories from existing semantic memories. Nat. Commun. 2020, 11, 1298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peiffer, A.; Brichet, M.; De Tiège, X.; Peigneux, P.; Urbain, C. The power of children’s sleep—Improved declarative memory consolidation in children compared with adults. Sci. Rep. 2020, 10, 9979. [Google Scholar] [CrossRef] [PubMed]
- El-Sheikh, M.; Sadeh, A.I. Sleep and development: Introduction to the monograph. Monogr. Soc. Res. Child Dev. 2015, 80, 1–14. [Google Scholar] [CrossRef]
- Lam, P.; Hiscock, H.; Wake, M. Outcomes of infant sleep problems: A longitudinal study of sleep, behavior, and maternal well-being. Pediatrics 2003, 111, e203–e207. [Google Scholar] [CrossRef] [Green Version]
- Martin, J.; Hiscock, H.; Hardy, P.; Davey, B.; Wake, M. Adverse Associations of Infant and Child Sleep Problems and Parent Health: An Australian Population Study. Pediatrics 2007, 119, 947–955. [Google Scholar] [CrossRef]
- Kurth, S.; Lassonde, J.M.; Pierpoint, L.A.; Rusterholz, T.; Jenni, O.G.; McClain, I.J.; Achermann, P.; LeBourgeois, M.K. Development of nap neurophysiology: Preliminary insights into sleep regulation in early childhood. J. Sleep Res. 2016, 25, 646–654. [Google Scholar] [CrossRef] [Green Version]
- Scher, A.; Epstein, R.; Tirosh, E. Stability and changes in sleep regulation: A longitudinal study from 3 months to 3 years. Int. J. Behav. Dev. 2004, 28, 268–274. [Google Scholar] [CrossRef]
- Galland, B.C.; Taylor, B.J.; Elder, D.E.; Herbison, P. Normal sleep patterns in infants and children: A systematic review of observational studies. Sleep Med. Rev. 2012, 16, 213–222. [Google Scholar] [CrossRef] [PubMed]
- Louis, J.; Zhang, J.; Revol, M.; Debilly, G.; Challamel, M. Ontogenesis of nocturnal organization of sleep spindles: A longitudinal study during the first 6 months of life. Electroencephalogr. Clin. Neurophysiol. 1992, 83, 289–296. [Google Scholar] [CrossRef]
- Jenni, O.G.; Borbély, A.A.; Achermann, P. Development of the nocturnal sleep electroencephalogram in human infants. Am. J. Physiol. Integr. Comp. Physiol. 2004, 286, R528–R538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parmelee, A.H. Sleep Patterns in Infancy A Study of One Idant from Birth to Eight Months of Age. Acta Paediatr. 1961, 50, 160–170. [Google Scholar] [CrossRef] [PubMed]
- Sadeh, A.; Lavie, P.; Scher, A.; Tirosh, E.; Epstein, R. Actigraphic home-monitoring sleep-disturbed and control infants and young children: A new method for pediatric assessment of sleep-wake patterns. Pediatrics 1991, 87, 494–499. [Google Scholar]
- Anders, T.F.; Keener, M. Developmental Course of Nighttime Sleep-Wake Patterns in Full-Term and Premature Infants during the First Year of Life. I. Sleep 1985, 8, 173–192. [Google Scholar] [CrossRef]
- Hagne, I. Development of the Sleep EEG in Normal Infants during the First Year of Life. Acta Paediatr. 1972, 61, 25–53. [Google Scholar] [CrossRef]
- Sadeh, A., III. Sleep assessment methods. Monogr. Soc. Res. Child Dev. 2015, 80, 33–48. [Google Scholar] [CrossRef]
- Camerota, M.; Tully, K.P.; Grimes, M.; Gueron-Sela, N.; Propper, C.B. Assessment of infant sleep: How well do multiple methods compare? Sleep 2018, 41. [Google Scholar] [CrossRef]
- Werner, H.; Molinari, L.; Guyer, C.; Jenni, O. Agreement Rates between Actigraphy, Diary, and Questionnaire for Children’s Sleep Patterns. Arch. Pediatr. Adolesc. Med. 2008, 162, 350–358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meltzer, L.J.; Montgomery-Downs, H.E.; Insana, S.P.; Walsh, C.M. Use of actigraphy for assessment in pediatric sleep research. Sleep Med. Rev. 2012, 16, 463–475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schoch, S.F.; Kurth, S.; Werner, H. Actigraphy in sleep research with infants and young children: Current practices and future benefits of standardized reporting. J. Sleep Res. 2020, e13134. [Google Scholar] [CrossRef]
- Schoch, S.F.; Jenni, O.G.; Kohler, M.; Kurth, S. Actimetry in infant sleep research: An approach to facilitate comparability. Sleep 2019, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alamian, A.; Wang, L.; Hall, A.M.; Pitts, M.; Ikekwere, J. Infant sleep problems and childhood overweight: Effects of three definitions of sleep problems. Prev. Med. Rep. 2016, 4, 463–468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaffer, J.P. Multiple Hypothesis Testing. Annu. Rev. Psychol. 1995, 46, 561–584. [Google Scholar] [CrossRef]
- Staples, A.D.; Bates, J.E.; Petersen, I.T.; McQuillan, M.E.; Hoyniak, C. Measuring sleep in young children and their mothers: Identifying actigraphic sleep composites. Int. J. Behav. Dev. 2019, 43, 278–285. [Google Scholar] [CrossRef]
- Acebo, C.; Sadeh, A.; Seifer, R.; Tzischinsky, O.; Wolfson, A.R.; Hafer, A.; Carskadon, M.A. Estimating Sleep Patterns with Activity Monitoring in Children and Adolescents: How Many Nights Are Necessary for Reliable Measures? Sleep 1999, 22, 95–103. [Google Scholar] [CrossRef]
- Squires, J.; Potter, L.; Bricker, D. The ASQ User’s Guide for the Ages & Stages Questionnaires: A Parent-Completed, Child-Monitoring System; Paul H Brookes Publishing: Baltimore, MD, USA, 1995; ISBN 978-1-55766-179-1. [Google Scholar]
- Gollenberg, A.L.; Lynch, C.; Jackson, L.W.; McGuinness, B.M.; Msall, M.E. Concurrent validity of the parent-completed Ages and Stages Questionnaires, 2nd Ed. with the Bayley Scales of Infant Development II in a low-risk sample. Child Care Health Dev. 2009, 36, 485–490. [Google Scholar] [CrossRef]
- Valla, L.; Wentzel-Larsen, T.; Hofoss, D.; Slinning, K. Prevalence of suspected developmental delays in early infancy: Results from a regional population-based longitudinal study. BMC Pediatr. 2015, 15, 215. [Google Scholar] [CrossRef] [Green Version]
- Lindert, B.H.W.T.; Van Someren, E.J.W. Sleep Estimates Using Microelectromechanical Systems (MEMS). Sleep 2013, 36, 781–789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sadeh, A.; Acebo, C.; Seifer, R.; Aytur, S.; Carskadon, M.A. Activity-based assessment of sleep-wake patterns during the 1st year of life. Infant Behav. Dev. 1995, 18, 329–337. [Google Scholar] [CrossRef]
- Phillips, A.J.K.; Clerx, W.M.; O’Brien, C.S.; Sano, A.; Barger, L.K.; Picard, R.W.; Lockley, S.W.; Klerman, E.B.; Czeisler, C.A. Irregular sleep/wake patterns are associated with poorer academic performance and delayed circadian and sleep/wake timing. Sci. Rep. 2017, 7, 3216. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2013. [Google Scholar]
- RStudio Team. RStudio: Integrated Development for R; R Studio Inc.: Boston, MA, USA, 2015; Volume 42, p. 14. Available online: http://www.rstudio.com (accessed on 15 December 2020).
- Wickham, H.; Henry, L. Tidyr: Tidy Messy Data. R Package Version 1.02; R Package: Madison, WI, USA, 2019. [Google Scholar]
- Wei, T.; Simko, V. R Package “Corrplot”: Visualization of a Correlation Matrix (Version 0.84); R Package: Madison, WI, USA, 2017; Available online: https://github.com/taiyun/corrplot (accessed on 15 December 2020).
- Becker, J.P.; Knowles, J.E.; Knowles, M.J.E. Package ‘Eeptools’. Available online: https://cran.r-project.org/web/packages/eeptools/index.html2020 (accessed on 15 December 2020).
- Wickham, H. Reshaping data with the reshape package. J. Stat. Softw. 2007, 21, 1–20. [Google Scholar] [CrossRef]
- Wickham, H.; Francois, R.; Henry, L.; Müller, K. Dplyr: A Grammar of Data Manipulation; R Package: Madison, WI, USA, 2015. [Google Scholar]
- Wickham, H. ggplot2: Elegant graPhics for Data Analysis; Springer: Berlin/Heidelberg, Germany, 2016. [Google Scholar]
- Grolemund, G.; Wickham, H. Dates and times made easy with lubridate. J. Stat. Softw. 2011, 40, 1–25. [Google Scholar] [CrossRef]
- Sarkar, D. Lattice: Multivariate Data Visualization with R; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2008. [Google Scholar]
- McMurdie, P.J.; Holmes, S. phyloseq: An R Package for Reproducible Interactive Analysis and Graphics of Microbiome Census Data. PLoS ONE 2013, 8, e61217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kowarik, A.; Templ, M. Imputation with the R Package VIM. J. Stat. Softw. 2016, 74, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Bache, S.M.; Wickham, H. Magrittr: A Forward-Pipe Operator for R; R Package: Madison, WI, USA, 2014. [Google Scholar]
- James, D.; Hornik, K. Chron: Chronological Objects Which Can Handle Dates and Times; R Package: Madison, WI, USA, 2010. [Google Scholar]
- Tang, Y.; Horikoshi, M.; Li, W. Ggfortify: Unified Interface to Visualize Statistical Results of Popular R Packages. R J. 2015, 8, 474–485. [Google Scholar] [CrossRef] [Green Version]
- Lüdecke, D. Sjplot: Data Visualization for Statistics in Social Science; R Package: Madison, WI, USA, 2018. [Google Scholar]
- Zhu, H. KableExtra: Construct Complex Table with ’Kable’ and Pipe Syntax; R Package Version 0.90; R Package: Madison, WI, USA, 2018; Available online: https://cran.r-project.org/web/packages/kableExtra/index.html (accessed on 15 December 2020).
- Wilke, C.O. Cowplot: Streamlined Plot Theme and Plot Annotations for “ggplot2”; R Package Version 0.94; R Package: Madison, WI, USA, 2019. [Google Scholar]
- Xie, Y. Knitr: A General-Purpose Tool for Dynamic Report Generation in R; R Package: Madison, WI, USA, 2013. [Google Scholar]
- DeWitt, P. Qwraps2: Quick Wraps 2; R Package Version 0.3.0; R Package: Madison, WI, USA, 2018. [Google Scholar]
- Van Buuren, S.; Groothuis-Oudshoorn, K. Mice: Multivariate Imputation by Chained Equations inR. J. Stat. Softw. 2011, 45, 8. [Google Scholar] [CrossRef] [Green Version]
- Robitzsch, A.; Grund, S.; Henke, T.; Robitzsch, M.A. Package ‘Miceadds’; R Package: Madison, WI, USA, 2017. [Google Scholar]
- Audigier, V.; Resche-Rigon, M. Micemd: Multiple Imputation by Chained Equations with Multilevel Data; R Package: Madison, WI, USA, 2017. [Google Scholar]
- Kohl, M. MKmisc: Miscellaneous Functions from M. Kohl; R Package Version 0.94; R Package: Madison, WI, USA, 2013. [Google Scholar]
- Revelle, W.; Revelle, M.W. Package ‘Psych’. Compr. R Arch. Netw. 2015. Available online: https://cran.r-project.org/web/packages/psych/psych.pdf (accessed on 15 December 2020).
- Stevens, J. Applied Multivariate Statistics for the Social Sciences, 2nd ed.; Lawrence Erlbaum Associates, Inc.: Hillsdale, NJ, USA, 1992; ISBN 978-0-8058-1154-4. [Google Scholar]
- Bruni, O.; Baumgartner, E.; Sette, S.; Ancona, M.; Caso, G.; Di Cosimo, M.E.; Mannini, A.; Ometto, M.; Pasquini, A.; Ulliana, A.; et al. Longitudinal Study of Sleep Behavior in Normal Infants during the First Year of Life. J. Clin. Sleep Med. 2014, 10, 1119–1127. [Google Scholar] [CrossRef] [Green Version]
- Sadeh, A.; Sharkey, K.M.; Carskadon, M.A. Activity-Based Sleep-Wake Identification: An Empirical Test of Methodological Issues. Sleep 1994, 17, 201–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, R.W.; Williams, S.M.; Farmer, V.L.; Taylor, B.J. The Stability of Sleep Patterns in Children 3 to 7 Years of Age. J. Pediatr. 2015, 166, 697–702. [Google Scholar] [CrossRef] [PubMed]
- Jenni, O.; Molinari, L.; Caflisch, J.; Largo, R.H. Sleep Duration from Ages 1 to 10 Years: Variability and Stability in Comparison with Growth. Pediatrics 2007, 120, 769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akerstedt, T.; Kecklund, G. Stability of Day and Night Sleep-A Two-Year Follow-Up of EEG Parameters in Three-Shift Workers. Sleep 1991, 14, 507–510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knutson, K.; Rathouz, P.J.; Yan, L.L.; Liu, K.; Lauderdale, D.S. Intra-Individual Daily and Yearly Variability in Actigraphically Recorded Sleep Measures: The CARDIA Study. Sleep 2007, 30, 793–796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaines, J.; Vgontzas, A.N.; Fernandez-Mendoza, J.; Basta, M.; Pejovic, S.; He, F.; Bixler, E.O. Short- and Long-Term Sleep Stability in Insomniacs and Healthy Controls. Sleep 2015, 38, 1727–1734. [Google Scholar] [CrossRef] [Green Version]
- Druiven, S.J.M.; Hovenkamp-Hermelink, J.H.; Knapen, S.E.; Kamphuis, J.; Haarman, B.C.M.; Penninx, B.W.; Antypa, N.; Meesters, Y.; Schoevers, R.; Riese, H. Stability of chronotype over a 7-year follow-up period and its association with severity of depressive and anxiety symptoms. Depress. Anxiety 2020, 37, 466–474. [Google Scholar] [CrossRef]
- Ednick, M.; Cohen, A.P.; McPhail, G.L.; Beebe, D.; Simakajornboon, N.; Amin, R.S. A Review of the Effects of Sleep during the First Year of Life on Cognitive, Psychomotor, and Temperament Development. Sleep 2009, 32, 1449–1458. [Google Scholar] [CrossRef] [Green Version]
- Randler, C.; Faßl, C.; Kalb, N. From Lark to Owl: Developmental changes in morningness-eveningness from new-borns to early adulthood. Sci. Rep. 2017, 7, srep45874. [Google Scholar] [CrossRef]
- Tikotzky, L.; De Marcas, G.; Har-Toov, J.; Dollberg, S.; Bar-Haim, Y.; Sadeh, A. Sleep and physical growth in infants during the first 6 months. J. Sleep Res. 2010, 19, 103–110. [Google Scholar] [CrossRef]
- Sadeh, A.; Flint-Ofir, E.; Tirosh, T.; Tikotzky, L. Infant sleep and parental sleep-related cognitions. J. Fam. Psychol. 2007, 21, 74–87. [Google Scholar] [CrossRef] [PubMed]
- Kurina, L.M.; Thisted, R.A.; Chen, J.-H.; McClintock, M.K.; Waite, L.; Lauderdale, D.S. Actigraphic sleep characteristics among older Americans. Sleep Health 2015, 1, 285–292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berg, J.F.V.D.; Miedema, H.M.; Tulen, J.H.; Hofman, A.; Neven, A.K.; Tiemeier, H. Sex Differences in Subjective and Actigraphic Sleep Measures: A Population-Based Study of Elderly Persons. Sleep 2009, 32, 1367–1375. [Google Scholar] [CrossRef] [PubMed]
- Jean-Louis, G.; Mendlowicz, M.V.; Von Gizycki, H.; Zizi, F.; Nunes, J. Assessment of Physical Activity and Sleep by Actigraphy: Examination of Gender Differences. J. Women’s Health Gender Based Med. 1999, 8, 1113–1117. [Google Scholar] [CrossRef]
- Campbell, D.W.; Eaton, W.O. Sex differences in the activity level of infants. Infant Child Dev. 1999, 8, 1–17. [Google Scholar] [CrossRef]
- Bach, V.; Telliez, F.; Leke, A.; Libert, J.-P. Gender-related sleep differences in neonates in thermoneutral and cool environments. J. Sleep Res. 2000, 9, 249–254. [Google Scholar] [CrossRef]
- Spruyt, K.; Aitken, R.J.; So, K.; Charlton, M.; Adamson, T.M.; Horne, R.S. Relationship between sleep/wake patterns, temperament and overall development in term infants over the first year of life. Early Hum. Dev. 2008, 84, 289–296. [Google Scholar] [CrossRef]
- Hupbach, A.; Gomez, R.L.; Bootzin, R.R.; Nadel, L. Nap-dependent learning in infants. Dev. Sci. 2009, 12, 1007–1012. [Google Scholar] [CrossRef]
- Seehagen, S.; Konrad, C.; Herbert, J.S.; Schneider, S. Timely sleep facilitates declarative memory consolidation in infants. Proc. Natl. Acad. Sci. USA 2015, 112, 1625–1629. [Google Scholar] [CrossRef] [Green Version]
- Kurdziel, L.; Duclos, K.; Spencer, R.M.C. Sleep spindles in midday naps enhance learning in preschool children. Proc. Natl. Acad. Sci. USA 2013, 110, 17267–17272. [Google Scholar] [CrossRef] [Green Version]
- Lukowski, A.F.; Milojevich, H.M. Sleeping like a baby: Examining relations between habitual infant sleep, recall memory, and generalization across cues at 10 months. Infant Behav. Dev. 2013, 36, 369–376. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable Name | 3 Months | 6 Months | 12 Months |
|---|---|---|---|
| (1) Bedtime (clock time in min) Parent-reported time in the 24-h-diary of putting the child to bed. For missing values, the first minute of reported sleep was used. If bedtime exceeded midnight 1440 was added. | 21:14 ± 01:15 (18:56–01:19) 1273.71 ± 75.38 (1116–1479) | 20:27 ± 01:19 (18:25–00:21) 1226.59 ± 69.18 (1105–1420.8) | 20:21 ± 00:53 (18:40–00:16) 1220.78 ± 53.46 (1120–1416) |
| (2) Variability of Bedtime (SD) Standard deviation of Bedtime across recording days. | 00:44 ± 00:22 (0:00–01:58) 43.5 ± 21.64 (0–118.39) | 00:33 ± 00:18 (0:00–01:27) 32.6 ± 17.76 (0–87.13) | 00:29 ± 00:17 (0:03–01:31) 28.88 ± 16.83 (3.35–91.41) |
| (3) Get up Time (clock time in min) Parent reported time in the 24-h-diary of getting out of bed in the morning. For missing values, the last minute of reported sleep was used. | 07:53 ± 00:52 (06:02–10:12) 472.88 ± 52.06 (361.5–612) | 07:24 ± 00:49 (05:36–09:38) 443.84 ± 48.89 (335.5–577.7) | 07:18 ± 00:43 (05:23–10:25) 437.93 ± 43.41 (323.33–625) |
| (4) Variability of Get up Time (SD) Standard deviation of Get up Time across recording days. | 00:42 ± 00:17 (00:06–01:36) 42.02 ± 16.44 (6.35–96.17) | 00:36 ± 00:16 (0:00–01:49) 36.35 ± 16.26 (0–109.2) | 00:36 ± 00:17 (00:06–01:40) 35.8 ± 16.93 (6.12–99.82) |
| (5) Sleep Onset (clock time in min) Following Bedtime, the first minute asleep of at least 10 min of consecutive sleep. If asleep at Bedtime, the first minute asleep before Bedtime was chosen. | 20:58 ± 01:08 (18:47–00:33) 1257.94 ± 68.08 (1127.17–1473.3) | 20:29 ± 01:06 (18:47–00:09) 1228.59 ± 65.87 (1112.33–1449.4) | 18:49 ± 00:55 (18:46–23:24) 1228.74 ± 54.7 (1125.5–1423.6) |
| (6) Variability of Sleep Onset (SD) Standard deviation of Sleep Onset across recording days. | 00:52 ± 00:24 (00:08–02:37) 51.87 ± 23.83 (7.75–157.33) | 00:38 ± 00:19 (00:06–01:49) 37.79 ± 19.07 (6.33–109.24) | 00:34 ± 00:17 (00:05–01:20) 34.28 ± 17.2 (4.7–79.86) |
| (7) Sleep Latency (min) Duration in minutes between Bedtime and Sleep Onset, set to 0 if Sleep Onset is before Bedtime. | 7.79 ± 7.97 (0–42) | 11.29 ± 8.3 (0–45.5) | 10.94 ± 8.2 (0–38.38) |
| (8) Variability of Sleep Latency (SD) Standard deviation of Sleep Latency across recording days. | 10.29 ± 9.17 (0–56.64) | 11.43 ± 7.61 (0–44.91) | 10.26 ± 7.14 (0–40.27) |
| (9) Sleep Offset (clock time in min) Last minute asleep of at least 10 consecutive minutes asleep before Get up Time or if asleep at Get up Time last minute asleep after Get up Time. | 07:51 ± 00:53 (05:55–10:23) 470.93 ± 53.13 (354.8–622.86) | 07:18 ± 00:49 (05:25–09:43) 437.71 ± 49.41 (324.5–583.38) | 07:17 ± 00:47 (05:16–10:16) 437.96 ± 46.6 (316.67–615.5) |
| (10) Variability of Sleep Offset (SD) Standard deviation of Sleep Offset across recording days. | 00:48 ± 00:19 (00:16–01:54) 48.06 ± 18.51 (15.82–114.17) | 00:40 ± 00:17 (00:17–02:03) 39.74 ± 16.89 (16.51–123.17) | 00:39 ± 00:21 (00:12–02:45) 38.66 ± 20.5 (12.02–164.83) |
| (11) Midsleep (clock time in min) Midpoint between Sleep Onset and Sleep Offset. | 02:24 ± 00:53 (00:33–04:59) 143.93 ± 53.02 (32.65–298.7) | 01:53 ± 00:52 (00:14–04:53) 112.88 ± 51.71 (13.7–293.81) | 01:54 ± 00:46 (00:14–04:38) 114.03 ± 46.09 (13.5–278.2) |
| (12) Variability of Midsleep (SD) Standard Deviation of Midsleep across recording days. | 00:38 ± 00:14 (00:12–01:19) 37.62 ± 13.62 (11.95–78.54) | 00:28 ± 00:11 (00:09–01:04) 28.37 ± 11.24 (8.86–64.22) | 00:27 ± 00:13 (00:08–01:42) 27.33 ± 13.46 (7.7–101.79) |
| (13) Sleep Opportunity (min) Time between Bedtime and Get Up Time (unless asleep at either of these times, in which case Sleep Onset/Sleep Offset was used). | 662.46 ± 62.8 (494.2–840) | 670.89 ± 54.38 (558.11–820.67) | 666.4 ± 42.51 (578–738) |
| (14) Variability of Sleep Opportunity (SD) Standard deviation of Sleep Opportunity across recording days. | 62.85 ± 23.14 (16.83–124.55) | 47.29 ± 20.18 (12.31–129.93) | 45.32 ± 23.34 (14.51–163.62) |
| (15) Sleep Period (min) Time between Sleep Onset and Sleep Offset. | 651.87 ± 58.05 (488.9–796) | 651.52 ± 50.44 (543.56–821.78) | 650.94 ± 44.7 (547–735.75) |
| (16) Variability of Sleep Period (SD) Standard deviation of Sleep Period across recording days. | 67.09 ± 22.21 (21.19–127.12) | 51.83 ± 21.73 (16.36–144.75) | 49.85 ± 23.43 (11.27–163.32) |
| (17) Total Sleep Time (min) Minutes scored ‘Sleep’ within Sleep Period. | 573.63 ± 58.25 (421.33–709.44) | 605.23 ± 47.38 (492.44–728.75) | 627.3 ± 51.29 (488.5–717.1) |
| (18) Variability of Total Sleep Time (SD) Standard deviation of Total Sleep Time across recording days. | 53.47 ± 18.91 (18.62–108.3) | 45.98 ± 16.04 (10.15–91.2) | 46.33 ± 19.44 (11.61–140.08) |
| (19) Sleep Efficiency (%) (Total Sleep Time)/(Sleep Opportunity) × 100. | 87.83 ± 5.4 (69.37–99.5) | 90.67 ± 4.08 (80.55–99.21) | 94.25 ± 3.52 (84.06–99.64) |
| (20) Variability of Sleep Efficiency (SD) Standard deviation of Sleep Efficiency across recording days. | 5.46 ± 2.35 (1.84–18.22) | 4.59 ± 1.95 (1.57–11.97) | 3.57 ± 1.9 (0.45–12.94) |
| (21) Wake after Sleep Onset (min) Minutes scored ‘Wake’ in Sleep Period. | 69.04 ± 32.15 (13.7–197.75) | 44.73 ± 24.55 (1.86–121.17) | 22.31 ± 17.02 (0–78.22) |
| (22) Variability of Wake after Sleep Onset (SD) Standard deviation of Wake after Sleep Onset across recording days. | 32.72 ± 12.52 (11.3–79.02) | 26.63 ± 13.46 (4.26–86.03) | 18.8 ± 10.68 (1.9–57.17) |
| (23) Longest Nocturnal Wake (min) Longest period scored ‘Wake’ followed by at least 15 min scored ‘Sleep’ in Sleep Period. | 31.87 ± 14.5 (7.6–93.33) | 24.37 ± 13.19 (1.86–75.89) | 13.74 ± 9.65 (0–56.67) |
| (24) Variability of Longest Nocturnal Wake (SD) Standard deviation of Longest Nocturnal Wake across recording days. | 16.43 ± 7.32 (3.1–39.7) | 17.09 ± 10.2 (3.14–48.35) | 12.04 ± 8.78 (0–60.19) |
| (25) Nocturnal Wake Frequency per Hour (waking/hour) (Number of Nocturnal Wake Periods in Sleep Period)/Sleep Period. | 0.34 ± 0.11 (0.1–0.61) | 0.23 ± 0.1 (0.02–0.49) | 0.14 ± 0.09 (0–0.46) |
| (26) Variability of Nocturnal Wake Frequency per Hour (SD) Standard deviation of Nocturnal Wake Frequency per Hour across recording days. | 0.12 ± 0.04 (0.03–0.27) | 0.11 ± 0.04 (0.03–0.22) | 0.1 ± 0.04 (0–0.24) |
| (27) Variability of Activity level (SD) Standard deviation of activity per minute in Sleep Period. | 168.64 ± 61.51 (40.69–356.73) | 178.91 ± 79.21 (49.92–478.14) | 108.5 ± 50.86 (33.64–336.46) |
| (28) Percent Active Epochs (ratio) (Minutes of epochs with non-zero activity in Sleep Period)/Sleep Period. | 0.3 ± 0.05 (0.14–0.4) | 0.24 ± 0.04 (0.13–0.34) | 0.23 ± 0.03 (0.14–0.32) |
| (29) Variability Percent Active Epochs (SD) Standard deviation of Percent Active Epochs across recording days. | 0.04 ± 0.01 (0.02–0.09) | 0.04 ± 0.02 (0.01–0.1) | 0.04 ± 0.01 (0.01–0.12) |
| (30) Longest Sleep (min) Longest continuous period scored as ‘Sleep’. | 292.19 ± 90.16 (139–580.29) | 339.21 ± 99.18 (158.75–632.17) | 458.24 ± 126.82 (166.89–706.44) |
| (31) Variability of Longest Sleep (SD) Standard deviation of Longest Sleep across recording days. | 82.75 ± 36.25 (21.04–190.74) | 104.82 ± 39.39 (23.02–222.59) | 127.41 ± 50.7 (14.21–245.62) |
| (32) Longest Wake (min) Longest continuous period scored as ‘Wake’. | 162.44 ± 27.74 (101.11–292.29) | 212.13 ± 32.94 (139.33–348) | 293.14 ± 40.25 (195.33–402) |
| (33) Variability of Longest Wake (SD) Standard deviation of Longest Wake across recording days. | 40.07 ± 18 (11.65–111.57) | 50.11 ± 22.36 (9.07–109.98) | 65.91 ± 22.99 (18.63–150.2) |
| (34) Nap Counter Number of daytime sleep periods exceeding 20 min between Sleep Offset and Sleep Onset. | 4.06 ± 0.77 (2–6.25) | 3.2 ± 0.59 (1.38–4.56) | 2.07 ± 0.55 (0.67–3.57) |
| (35) Variability Nap counter (SD) Standard deviation of Nap counter across recording days. | 1.1 ± 0.31 (0.38–2.32) | 0.84 ± 0.3 (0–1.72) | 0.74 ± 0.27 (0–1.9) |
| (36) Sleep after Wake Onset (min) Minutes scored Sleep between Sleep Offset and Sleep Onset. | 247.56 ± 53.3 (123–382.88) | 179.03 ± 37.26 (95.6–298.43) | 142.54 ± 38.17 (70.5–282.63) |
| (37) Variability Sleep after Wake Onset (SD) Standard deviation of Sleep after Wake Onset across recording days. | 61.92 ± 20.6 (19.22–154.89) | 45.27 ± 16.89 (15.49–112.18) | 43.76 ± 17.8 (10.94–140.06) |
| (38) Sleep Duration 24 h (min) Minutes scored ‘Sleep’ across 24 h. | 822.19 ± 55.68 (672.86–975.44) | 783.15 ± 44.45 (654–922.33) | 767.64 ± 45.34 (609.67–867.43) |
| (39) Variability of Sleep Duration 24 h (SD) Standard deviation of Sleep Duration 24 h across recording days. | 66.34 ± 19.58 (28.03–123.61) | 58.77 ± 19.91 (24.73–121.56) | 54.17 ± 18.89 (20.77–127.09) |
| (40) Sleep Duration Day (min) Minutes scored ‘Sleep’ between 7 am to 7 pm. | 278.59 ± 44.98 (158.7–396) | 203.46 ± 39.66 (115.88–345.13) | 165.83 ± 41.31 (81.33–298.56) |
| (41) Variability Sleep Duration Day (SD) Standard deviation of Sleep Duration Day across recording days. | 53.42 ± 16.05 (17.33–125.21) | 43.44 ± 14.42 (15.79–83.25) | 43.2 ± 12.34 (21.21–76.36) |
| (42) Sleep Duration Night (min) Minutes scored ‘Sleep’ between 7 pm to 7 am. | 548.43 ± 45.54 (407.22–644.44) | 579.11 ± 49.17 (426.75–672.11) | 602.1 ± 47.78 (467.89–699.11) |
| (43) Variability of Sleep Duration Night (SD) Standard deviation of Sleep Duration Night across recording days. | 44.78 ± 16.37 (12.78–92.5) | 40.95 ± 14.53 (12.34–103.61) | 35.51 ± 13.72 (7.31–72.05) |
| (44) % Sleep Duration Night (ratio) (Sleep Duration Night)/(Sleep Duration 24 h). | 0.67 ± 0.05 (0.55–0.84) | 0.74 ± 0.05 (0.57–0.85) | 0.78 ± 0.05 (0.61–0.88) |
| (45) Variability % Sleep Duration Night (SD) Standard deviation of % Sleep Duration Night across recording days. | 0.05 ± 0.01 (0.02–0.09) | 0.05 ± 0.01 (0.02–0.11) | 0.05 ± 0.01 (0.02–0.1) |
| (46) Sleep Regularity Index Whole Day (ratio) The probability of being in the same state (Sleep or Wake) computed for each minute, averaged across one day, and then across all recording days. Represented with ratio (0–1) (‘Sleep’/’Wake), where 1 reflects the exact same rhythm every day. | 0.77 ± 0.03 (0.66–0.84) | 0.82 ± 0.03 (0.74–0.89) | 0.87 ± 0.03 (0.76–0.95) |
| (47) Sleep Regularity Index Day (ratio) Sleep Regularity Index for the clock times from 7 am to 7 pm. | 0.7 ± 0.04 (0.62–0.86) | 0.76 ± 0.04 (0.64–0.91) | 0.81 ± 0.04 (0.7–0.92) |
| (48) Sleep Regularity Index Night (ratio) Sleep Regularity Index for the clock times from 7 pm to 7 am. | 0.84 ± 0.05 (0.66–0.96) | 0.88 ± 0.05 (0.62–0.97) | 0.92 ± 0.04 (0.79–0.99) |
| Variables | Sleep Activity | Sleep Variability | Sleep Day | Sleep Timing | Sleep Night |
|---|---|---|---|---|---|
| (19) Sleep Efficiency (%) | −0.89 | 0.05 | 0.00 | −0.01 | −0.02 |
| (23) Longest Nocturnal Wake (min) | 0.88 | 0.04 | 0.05 | 0.02 | 0.19 |
| (21) Wake after Sleep Onset (min) | 0.86 | −0.01 | −0.11 | 0.00 | 0.16 |
| (25) Nocturnal Wake Frequency per Hour (wakings/hour) | 0.79 | −0.13 | −0.14 | 0.03 | −0.13 |
| (30) Longest Sleep (min) | −0.77 | 0.09 | 0.04 | −0.03 | 0.15 |
| (27) Variability of Activity level (SD) | 0.76 | −0.05 | 0.10 | 0.01 | 0.02 |
| (22) Variability of Wake after Sleep Onset (SD) | 0.72 | 0.09 | 0.10 | 0.01 | 0.05 |
| (24) Variability of Longest Nocturnal Wake (SD) | 0.70 | 0.07 | 0.28 | −0.05 | 0.02 |
| (48) Sleep Regularity Index Night (ratio) | −0.69 | −0.18 | 0.17 | 0.04 | 0.09 |
| (28) Percent Active Epochs (ratio) | 0.58 | −0.08 | −0.28 | 0.01 | 0.12 |
| (14) Variability of Sleep Opportunity (SD) | −0.05 | 0.87 | −0.07 | −0.08 | 0.04 |
| (16) Variability of Sleep Period (SD) | 0.04 | 0.86 | 0.03 | −0.11 | −0.07 |
| (18) Variability of Total Sleep Time (SD) | −0.06 | 0.73 | 0.10 | 0.00 | 0.00 |
| (10) Variability of Sleep Offset (SD) | −0.09 | 0.73 | −0.05 | 0.02 | 0.11 |
| (12) Variability of Midsleep (SD) | 0.00 | 0.73 | −0.08 | −0.01 | −0.05 |
| (4) Variability of Get up Time (SD) | −0.13 | 0.72 | 0.02 | 0.14 | 0.19 |
| (6) Variability of Sleep Onset (SD) | 0.10 | 0.64 | −0.04 | 0.06 | −0.10 |
| (2) Variability of Bedtime (SD) | 0.20 | 0.58 | 0.05 | −0.02 | −0.11 |
| (32) Longest Wake (min) | −0.10 | 0.04 | −0.92 | 0.11 | −0.17 |
| (34) Nap Counter | 0.03 | −0.06 | 0.86 | −0.12 | −0.14 |
| (36) Sleep after Wake Onset (min) | 0.00 | 0.01 | 0.82 | −0.11 | −0.26 |
| (47) Sleep Regularity Index Day (ratio) | −0.02 | −0.24 | −0.76 | 0.07 | −0.02 |
| (40) Sleep Duration Day (min) | −0.01 | 0.11 | 0.72 | 0.32 | 0.05 |
| (33) Variability of Longest Wake (SD) | 0.06 | 0.12 | −0.68 | 0.03 | −0.21 |
| (44) % Sleep Duration Night (ratio) | −0.12 | −0.05 | −0.56 | −0.39 | 0.12 |
| (9) Sleep Offset (clock time in min) | 0.03 | −0.01 | 0.03 | 1.01 | 0.32 |
| (3) Get up Time (clock time in min) | 0.08 | −0.03 | 0.01 | 0.97 | 0.37 |
| (11) Midsleep (clock time in min) | −0.02 | −0.01 | 0.08 | 0.93 | −0.18 |
| (5) Sleep Onset (clock time in min) | −0.05 | −0.04 | 0.08 | 0.76 | −0.52 |
| (1) Bedtime (clock time in min) | −0.07 | 0.00 | −0.04 | 0.68 | −0.49 |
| (15) Sleep Period (min) | 0.11 | 0.03 | −0.01 | 0.12 | 0.99 |
| (13) Sleep Opportunity (min) | 0.18 | 0.00 | 0.05 | 0.08 | 0.96 |
| (17) Total Sleep Time (min) | −0.40 | −0.03 | 0.04 | 0.06 | 0.78 |
| Proportion of Variance explained | 0.19 | 0.14 | 0.14 | 0.13 | 0.11 |
| Sleep Composite | Correlation 3 vs. 6 Months | Correlation 6 vs. 12 Months | Correlation 3 vs. 12 Months | |||
|---|---|---|---|---|---|---|
| rs | p | rs | p | rs | p | |
| Sleep Activity | 0.29 | <0.001 | 0.21 | 0.01 | 0.15 | 0.07 |
| Sleep Day | 0.25 | 0.004 | 0.29 | <0.001 | 0.11 | 0.21 |
| Sleep Night | 0.53 | <0.001 | 0.45 | <0.001 | 0.24 * | 0.004 |
| Sleep Timing | 0.68 | <0.001 | 0.58 | <0.001 | 0.55 | <0.001 |
| Sleep Variability | 0.28 | <0.001 | 0.38 | <0.001 | 0.23 * | 0.007 |
| Variable | Collective Score | Personal-Social | Gross Motor | |||
|---|---|---|---|---|---|---|
| b ± SE | p | b ± SE | p | b ± SE | p | |
| Intercept | 203.16 ± 6.58 | <0.001 | 42.17 ± 2.04 | <0.001 | 38.82 ± 2.21 | <0.001 |
| Sleep Activity | −0.91 ± 2.27 | 0.69 | −0.46 ± 0.73 | 0.53 | 1.05 ± 0.80 | 0.19 |
| Sleep Day | −6.65± 3.00 | 0.03 | −1.08 ± 0.98 | 0.27 | 1.12 ± 1.10 | 0.31 |
| Sleep Night | 0.84 ± 2.08 | 0.68 | 0.49 ± 0.62 | 0.43 | 0.68 ± 0.69 | 0.33 |
| Sleep Timing | −0.20 ± 2.41 | 0.94 | −0.40 ± 0.70 | 0.57 | 0.47 ± 0.78 | 0.55 |
| Sleep Variability | −2.52 ± 2.09 | 0.23 | 0.33 ± 0.67 | 0.62 | 0.55 ± 0.77 | 0.47 |
| Exact age | 0.21 ± 0.79 | 0.78 | −0.37 ± 0.27 | 0.17 | 0.14 ± 0.30 | 0.63 |
| Female sex | 9.49 ± 5.63 | 0.09 | 1.76 ± 1.35 | 0.19 | 0.90 ± 1.55 | 0.56 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schoch, S.F.; Huber, R.; Kohler, M.; Kurth, S. Which Are the Central Aspects of Infant Sleep? The Dynamics of Sleep Composites across Infancy. Sensors 2020, 20, 7188. https://doi.org/10.3390/s20247188
Schoch SF, Huber R, Kohler M, Kurth S. Which Are the Central Aspects of Infant Sleep? The Dynamics of Sleep Composites across Infancy. Sensors. 2020; 20(24):7188. https://doi.org/10.3390/s20247188
Chicago/Turabian StyleSchoch, Sarah F., Reto Huber, Malcolm Kohler, and Salome Kurth. 2020. "Which Are the Central Aspects of Infant Sleep? The Dynamics of Sleep Composites across Infancy" Sensors 20, no. 24: 7188. https://doi.org/10.3390/s20247188
APA StyleSchoch, S. F., Huber, R., Kohler, M., & Kurth, S. (2020). Which Are the Central Aspects of Infant Sleep? The Dynamics of Sleep Composites across Infancy. Sensors, 20(24), 7188. https://doi.org/10.3390/s20247188