

Trunk Posture from Randomly Oriented Accelerometers

Abstract
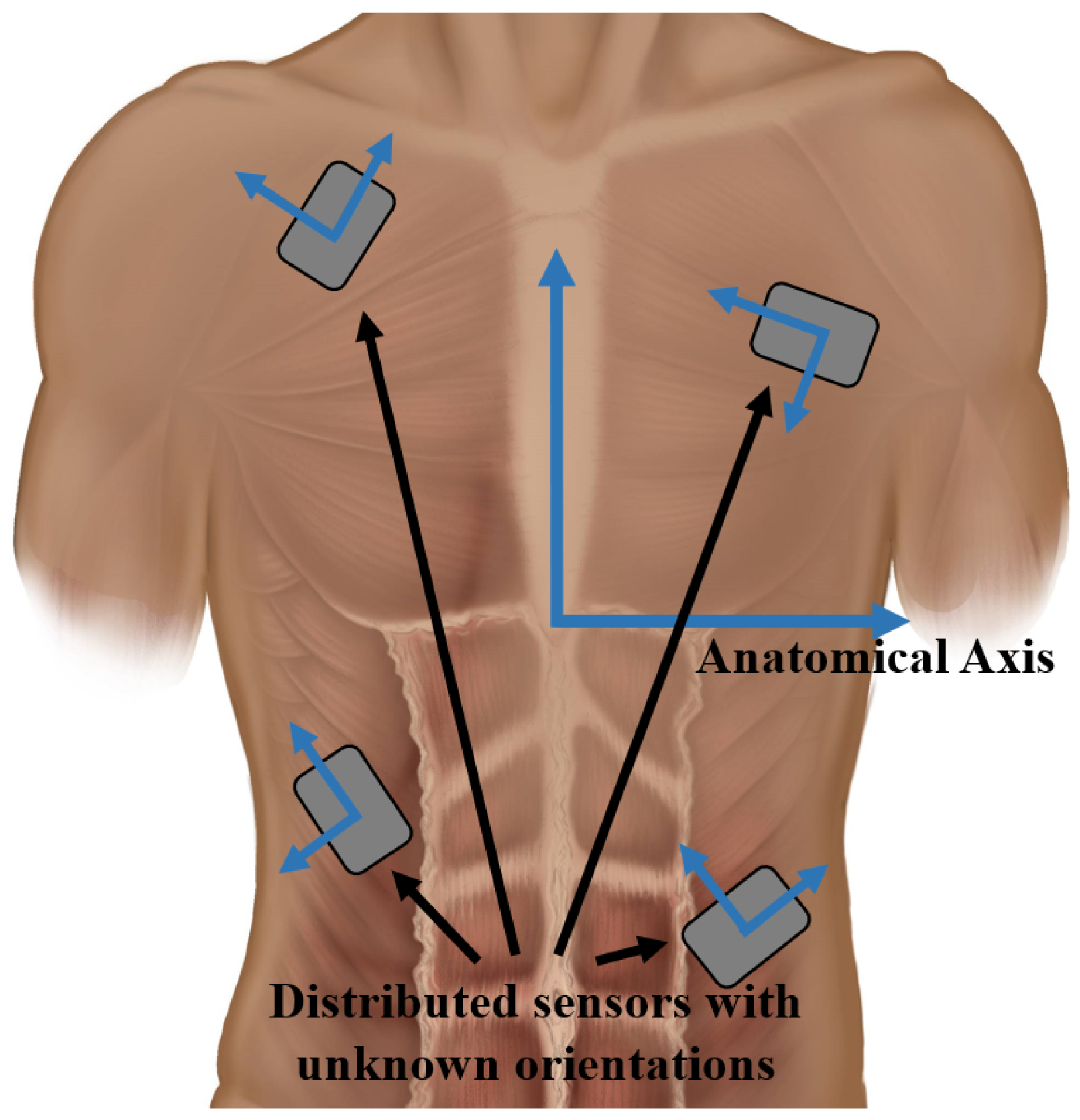
:1. Introduction
2. Materials and Methods
2.1. Participants
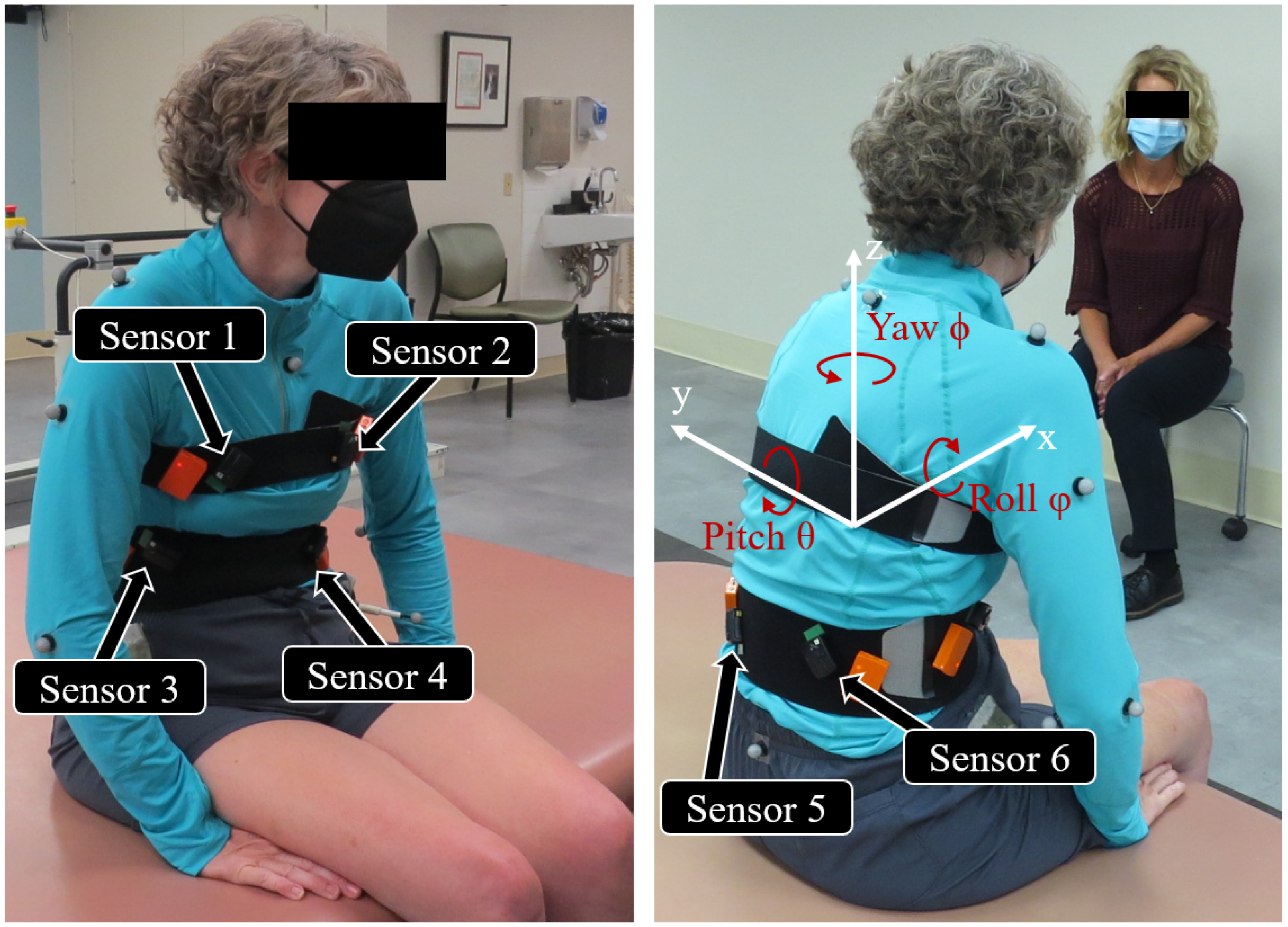
2.2. Experiment Setup
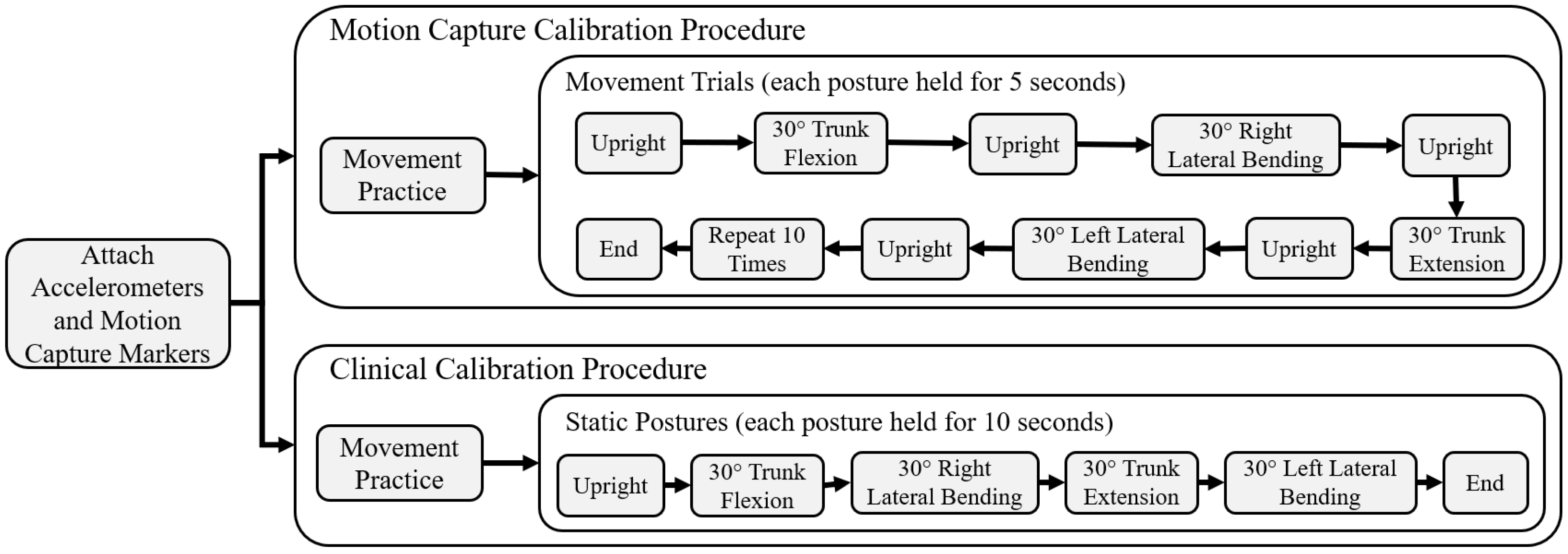
2.3. Motion Capture Calibration
2.4. Clinical Calibration
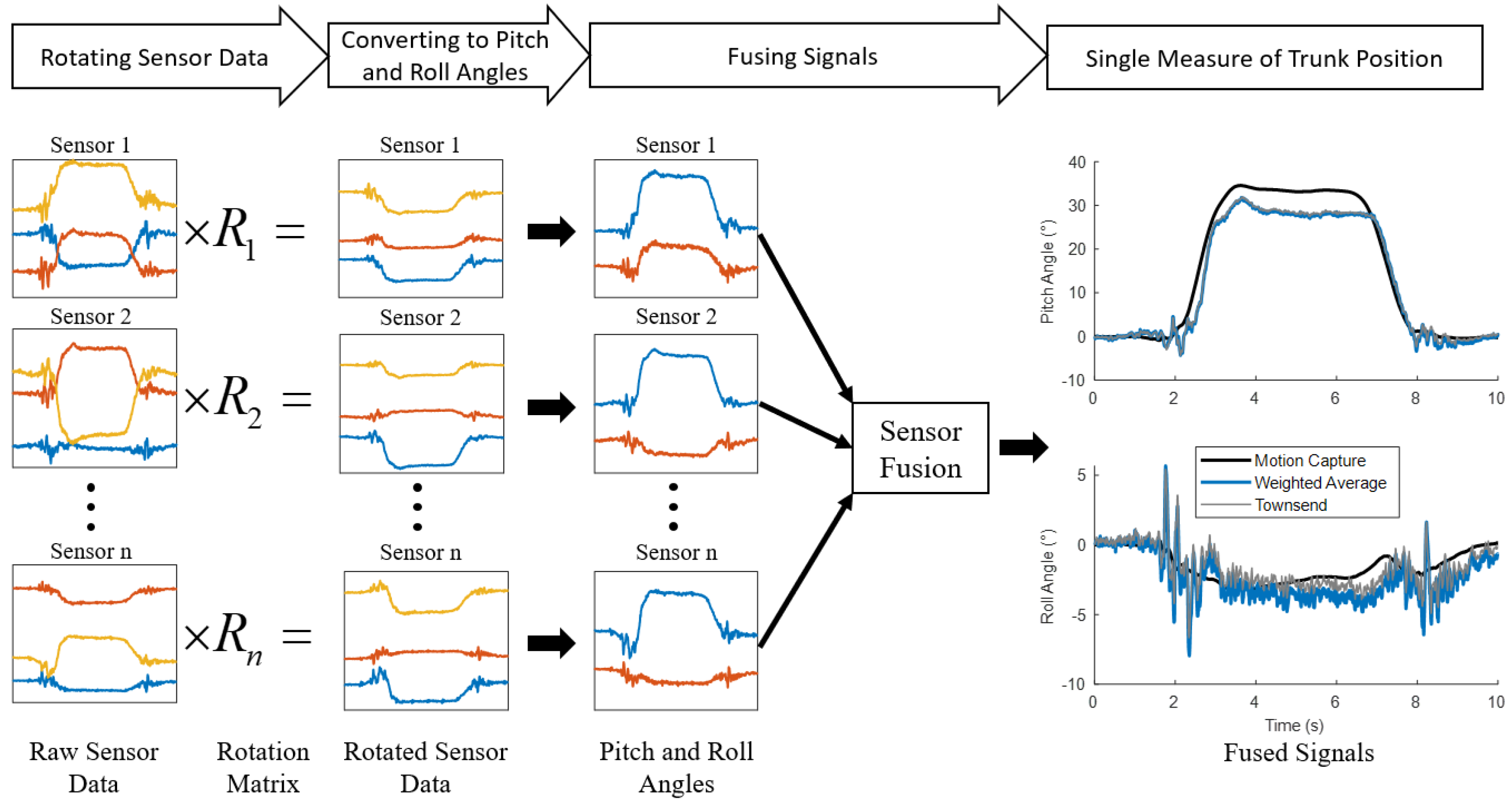
2.5. Experiment Data Analysis and Statistics
3. Results
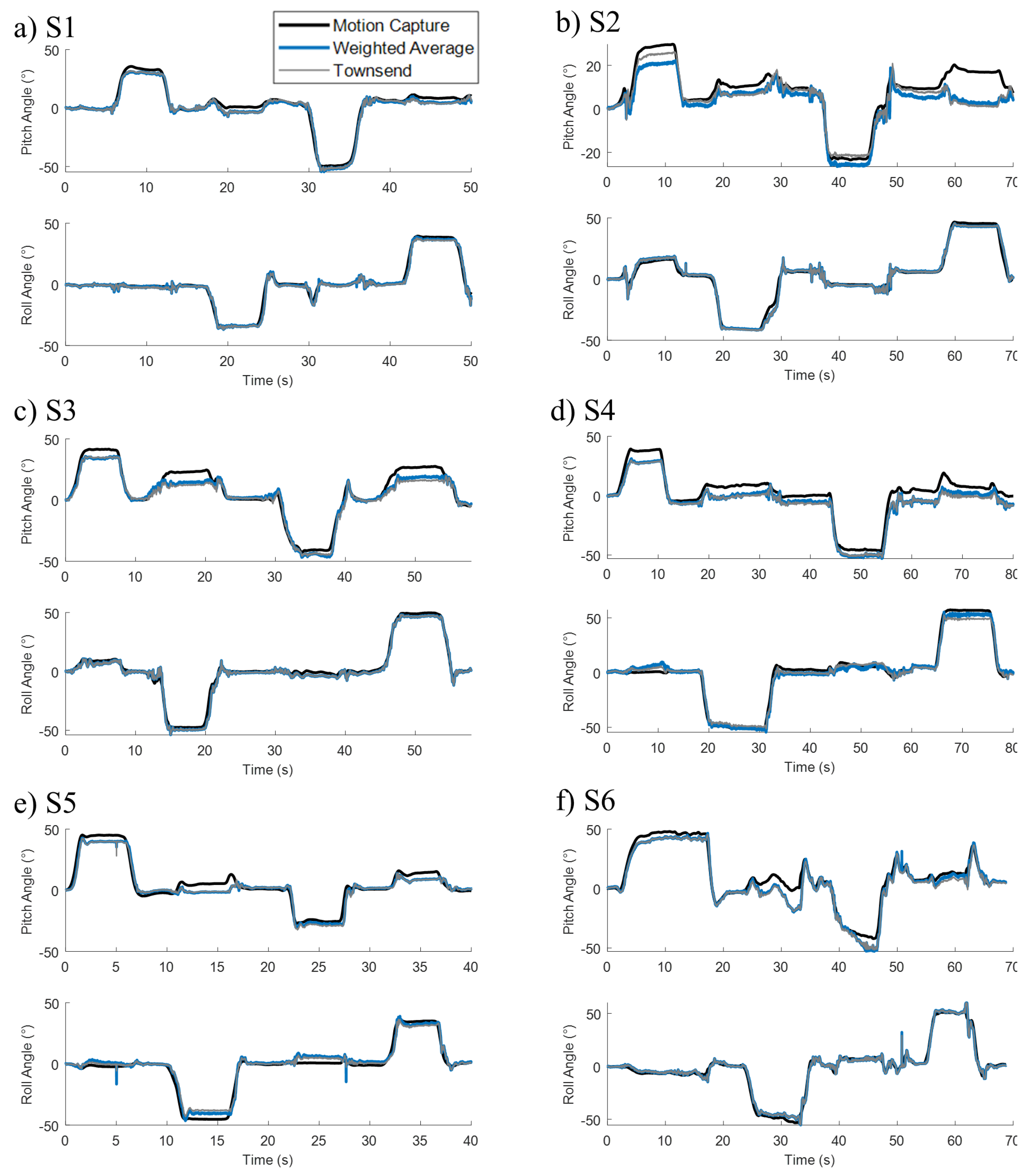
3.1. Motion Capture Calibration
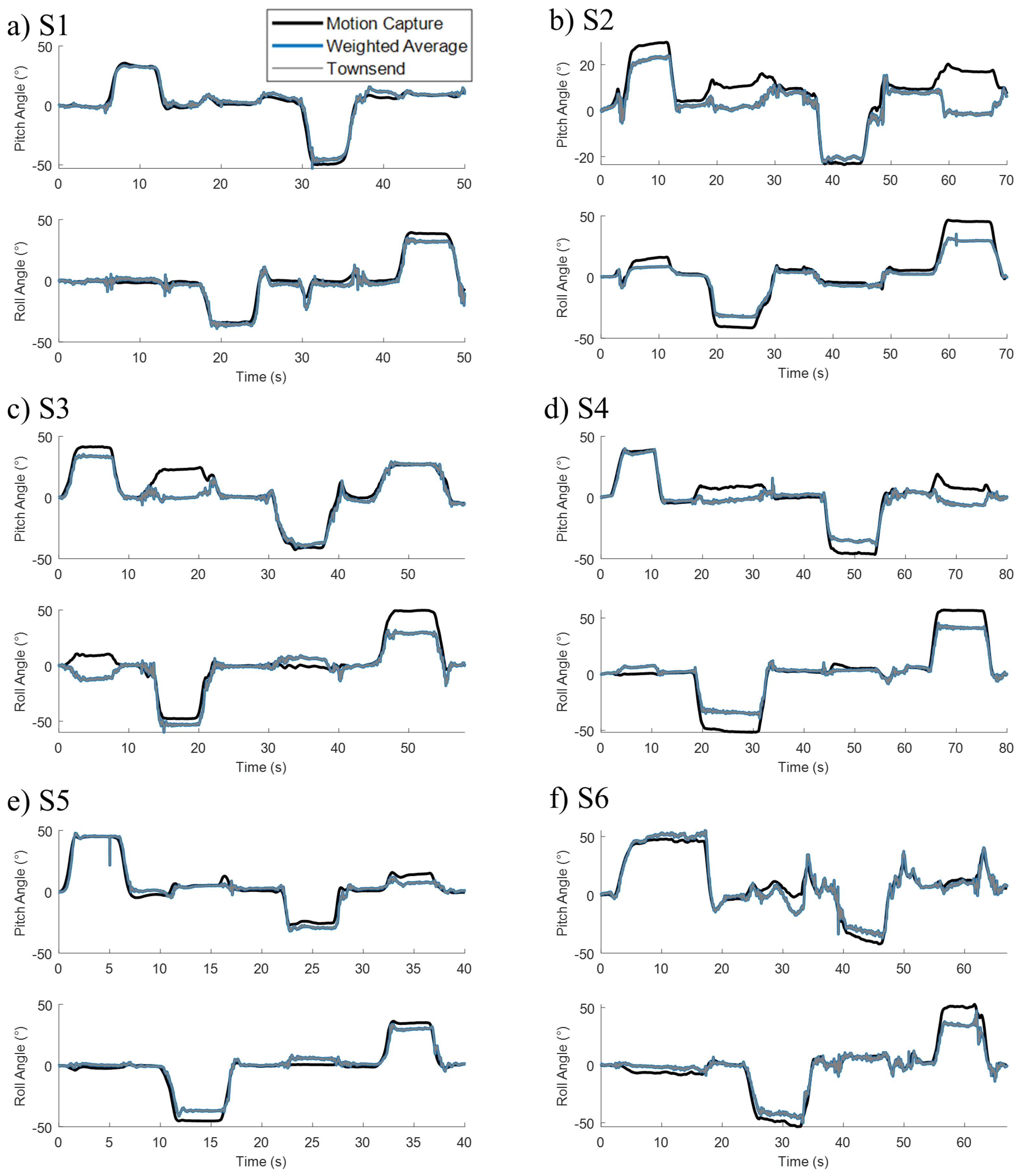
3.2. Clinical Calibration
4. Discussion
Limitations and Future Work
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| FNS | Functional Neuromuscular Stimulation |
| SCI | Spinal Cord Injury |
| AIS | American Spinal Injury Association Impairment Score |
| NNP | Networked Neuroprosthesis |
| IMU | Inertial Measurement Unit |
| RMSE | Root Mean Squared Error |
| r | Correlation Coefficient |
References
- Hardin, E.; Kobetic, R.; Murray, L.; Corado-Ahmed, M.; Pinault, G.; Sakai, J.; Bailey, S.N.; Ho, C.; Triolo, R.J. Walking after incomplete spinal cord injury using an implanted FES system: A case report. J. Rehabil. Res. Dev. 2007, 44, 333. [Google Scholar] [CrossRef] [PubMed]
- Thrasher, T.A.; Popovic, M.R. Functional electrical stimulation of walking: Function, exercise and rehabilitation. In Annales de Réadaptation et de Médecine Physique; Elsevier Masson: Paris, France, 2008; Volume 51, pp. 452–460. [Google Scholar]
- Hasnan, N.; Ektas, N.; Tanhoffer, A.; Tanhoffer, R.; Fornusek, C.; Middleton, J.W.; Husain, R.; Davis, G.M. Exercise responses during functional electrical stimulation cycling in individuals with spinal cord injury. Med. Sci. Sports Exerc. 2013, 45, 1131–1138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gelenitis, K.; Foglyano, K.; Lombardo, L.; Triolo, R. Selective neural stimulation methods improve cycling exercise performance after spinal cord injury: A case series. J. Neuroeng. Rehabil. 2021, 18, 1–14. [Google Scholar] [CrossRef]
- Andrews, B.; Gibbons, R.; Wheeler, G. Development of functional electrical stimulation rowing: The Rowstim series. Artif. Organs 2017, 41, E203–E212. [Google Scholar] [CrossRef] [PubMed]
- Triolo, R.J.; Bailey, S.N.; Miller, M.E.; Lombardo, L.M.; Audu, M.L. Effects of stimulating hip and trunk muscles on seated stability, posture, and reach after spinal cord injury. Arch. Phys. Med. Rehabil. 2013, 94, 1766–1775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schearer, E.M.; Liao, Y.W.; Perreault, E.J.; Tresch, M.C.; Memberg, W.D.; Kirsch, R.F.; Lynch, K.M. Multi-muscle FES force control of the human arm for arbitrary goals. IEEE Trans. Neural Syst. Rehabil. Eng. 2013, 22, 654–663. [Google Scholar] [CrossRef] [Green Version]
- Kapadia, N.M.; Bagher, S.; Popovic, M.R. Influence of different rehabilitation therapy models on patient outcomes: Hand function therapy in individuals with incomplete SCI. J. Spinal Cord Med. 2014, 37, 734–743. [Google Scholar] [CrossRef] [Green Version]
- Karamian, B.A.; Siegel, N.; Nourie, B.; Serruya, M.D.; Heary, R.F.; Harrop, J.S.; Vaccaro, A.R. The role of electrical stimulation for rehabilitation and regeneration after spinal cord injury. J. Orthop. Traumatol. 2022, 23, 1–17. [Google Scholar] [CrossRef]
- Marquez-Chin, C.; Popovic, M.R. Functional electrical stimulation therapy for restoration of motor function after spinal cord injury and stroke: A review. Biomed. Eng. Online 2020, 19, 1–25. [Google Scholar] [CrossRef]
- McDaniel, J.; Lombardo, L.M.; Foglyano, K.M.; Marasco, P.D.; Triolo, R.J. Setting the pace: Insights and advancements gained while preparing for an FES bike race. J. Neuroeng. Rehabil. 2017, 14, 1–8. [Google Scholar] [CrossRef]
- Anderson, K.D. Targeting recovery: Priorities of the spinal cord-injured population. J. Neurotrauma 2004, 21, 1371–1383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collinger, J.L.; Boninger, M.L.; Bruns, T.M.; Curley, K.; Wang, W.; Weber, D.J. Functional priorities, assistive technology, and brain-computer interfaces after spinal cord injury. J. Rehabil. Res. Dev. 2013, 50, 145. [Google Scholar] [CrossRef] [PubMed]
- Huh, S.; Ko, H.Y. Recovery target priorities of people with spinal cord injuries in Korea compared with other countries: A survey. Spinal Cord 2020, 58, 998–1003. [Google Scholar] [CrossRef] [PubMed]
- Kukke, S.N.; Triolo, R.J. The effects of trunk stimulation on bimanual seated workspace. IEEE Trans. Neural Syst. Rehabil. Eng. 2004, 12, 177–185. [Google Scholar] [CrossRef]
- Triolo, R.J.; Bailey, S.N.; Lombardo, L.M.; Miller, M.E.; Foglyano, K.; Audu, M.L. Effects of intramuscular trunk stimulation on manual wheelchair propulsion mechanics in 6 subjects with spinal cord injury. Arch. Phys. Med. Rehabil. 2013, 94, 1997–2005. [Google Scholar] [CrossRef] [Green Version]
- Vanoncini, M.; Holderbaum, W.; Andrews, B.J. Electrical stimulation for trunk control in paraplegia: A feasibility study. Control. Eng. Pract. 2012, 20, 1247–1258. [Google Scholar] [CrossRef]
- Audu, M.L.; Lombardo, L.M.; Schnellenberger, J.R.; Foglyano, K.M.; Miller, M.E.; Triolo, R.J. A neuroprosthesis for control of seated balance after spinal cord injury. J. Neuroeng. Rehabil. 2015, 12, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Friederich, A.R.; Bao, X.; Triolo, R.J.; Audu, M.L. Feedback Control of Upright Seating with Functional Neuromuscular Stimulation during a Functional Task after Spinal Cord Injury: A Case Study. In Proceedings of the 2021 43rd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Virtual, 1–5 November 2021; pp. 5719–5722. [Google Scholar]
- Lambrecht, J.M.; Kirsch, R.F. Miniature low-power inertial sensors: Promising technology for implantable motion capture systems. IEEE Trans. Neural Syst. Rehabil. Eng. 2014, 22, 1138–1147. [Google Scholar] [CrossRef]
- Roetenberg, D.; Luinge, H.J.; Baten, C.T.; Veltink, P.H. Compensation of magnetic disturbances improves inertial and magnetic sensing of human body segment orientation. IEEE Trans. Neural Syst. Rehabil. Eng. 2005, 13, 395–405. [Google Scholar] [CrossRef] [Green Version]
- Xing, H.; Hou, B.; Lin, Z.; Guo, M. Modeling and compensation of random drift of MEMS gyroscopes based on least squares support vector machine optimized by chaotic particle swarm optimization. Sensors 2017, 17, 2335. [Google Scholar] [CrossRef]
- De Vries, W.; Veeger, H.; Baten, C.; Van Der Helm, F. Magnetic distortion in motion labs, implications for validating inertial magnetic sensors. Gait Posture 2009, 29, 535–541. [Google Scholar] [CrossRef] [PubMed]
- Bheemreddy, A.; Lombardo, L.M.; Miller, M.E.; Foglyano, K.M.; Nogan-Bailey, S.; Triolo, R.J.; Audu, M.L. A closed-loop self-righting controller for seated balance in the coronal and diagonal planes following spinal cord injury. Med. Eng. Phys. 2020, 86, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Smith, B.; Crish, T.; Buckett, J.; Kilgore, K.; Peckham, P. Development of an implantable networked neuroprosthesis. In Proceedings of the 2nd International IEEE EMBS Conference on Neural Engineering, Arlington, VA, USA, 16–20 March 2005; pp. 454–457. [Google Scholar]
- Makowski, N.S.; Campean, A.; Lambrecht, J.M.; Buckett, J.R.; Coburn, J.D.; Hart, R.L.; Miller, M.E.; Montague, F.W.; Crish, T.; Fu, M.J.; et al. Design and testing of stimulation and myoelectric recording modules in an implanted distributed neuroprosthetic system. IEEE Trans. Biomed. Circuits Syst. 2021, 15, 281–293. [Google Scholar] [CrossRef] [PubMed]
- Castillo-Escario, Y.; Kumru, H.; Valls-Solé, J.; García-Alen, L.; Jané, R.; Vidal, J. Quantitative evaluation of trunk function and the StartReact effect during reaching in patients with cervical and thoracic spinal cord injury. J. Neural Eng. 2021, 18, 0460d2. [Google Scholar] [CrossRef] [PubMed]
- Armandei, M.; Saberi, H.; Derakhshanrad, N.; Yekaninejad, M. Pivotal role of cervical rotation for rehabilitation outcomes in patients with subaxial cervical spinal cord injury. Neurochirurgie 2020, 66, 247–251. [Google Scholar] [CrossRef]
- Field-Fote, E.C.; Ray, S.S. Seated reach distance and trunk excursion accurately reflect dynamic postural control in individuals with motor-incomplete spinal cord injury. Spinal Cord 2010, 48, 745–749. [Google Scholar] [CrossRef] [Green Version]
- Grimpampi, E.; Bonnet, V.; Taviani, A.; Mazzà, C. Estimate of lower trunk angles in pathological gaits using gyroscope data. Gait Posture 2013, 38, 523–527. [Google Scholar] [CrossRef]
- Mazza, C.; Donati, M.; McCamley, J.; Picerno, P.; Cappozzo, A. An optimized Kalman filter for the estimate of trunk orientation from inertial sensors data during treadmill walking. Gait Posture 2012, 35, 138–142. [Google Scholar] [CrossRef]
- Punchihewa, N.G.; Miyazaki, S.; Chosa, E.; Yamako, G. Efficacy of Inertial Measurement Units in the Evaluation of Trunk and Hand Kinematics in Baseball Hitting. Sensors 2020, 20, 7331. [Google Scholar] [CrossRef]
- Luinge, H.J.; Veltink, P.H. Measuring orientation of human body segments using miniature gyroscopes and accelerometers. Med. Biol. Eng. Comput. 2005, 43, 273–282. [Google Scholar] [CrossRef]
- Luinge, H.J.; Veltink, P.H. Inclination measurement of human movement using a 3-D accelerometer with autocalibration. IEEE Trans. Neural Syst. Rehabil. Eng. 2004, 12, 112–121. [Google Scholar] [CrossRef] [PubMed]
- Brouwer, N.P.; Yeung, T.; Bobbert, M.F.; Besier, T.F. 3D trunk orientation measured using inertial measurement units during anatomical and dynamic sports motions. Scand. J. Med. Sci. Sport. 2021, 31, 358–370. [Google Scholar] [CrossRef]
- Audu, M.L.; Triolo, R.J. Intrinsic and extrinsic contributions to seated balance in the sagittal and coronal planes: Implications for trunk control after spinal cord injury. J. Appl. Biomech. 2015, 31, 221–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leardini, A.; Biagi, F.; Belvedere, C.; Benedetti, M.G. Quantitative comparison of current models for trunk motion in human movement analysis. Clin. Biomech. 2009, 24, 542–550. [Google Scholar] [CrossRef]
- Ugray, Z.; Lasdon, L.; Plummer, J.; Glover, F.; Kelly, J.; Martí, R. Scatter search and local NLP solvers: A multistart framework for global optimization. INFORMS J. Comput. 2007, 19, 328–340. [Google Scholar] [CrossRef]
- Li, Q.; Mark, R.G.; Clifford, G.D. Robust heart rate estimation from multiple asynchronous noisy sources using signal quality indices and a Kalman filter. Physiol. Meas. 2007, 29, 15. [Google Scholar] [CrossRef] [Green Version]
- Crago, P.E.; Chizeck, H.J.; Neuman, M.R.; Hambrecht, F.T. Sensors for use with functional neuromuscular stimulation. IEEE Trans. Biomed. Eng. 1986, BME-33, 256–268. [Google Scholar] [CrossRef]
- Ernst, M.J.; Rast, F.M.; Bauer, C.M.; Marcar, V.L.; Kool, J. Determination of thoracic and lumbar spinal processes by their percentage position between C7 and the PSIS level. BMC Res. Notes 2013, 6, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Al Borno, M.; O’Day, J.; Ibarra, V.; Dunne, J.; Seth, A.; Habib, A.; Ong, C.; Hicks, J.; Uhlrich, S.; Delp, S. OpenSense: An open-source toolbox for Inertial-Measurement-Unit-based measurement of lower extremity kinematics over long durations. J. Neuroeng. Rehabil. 2022, 19, 1–11. [Google Scholar] [CrossRef]
- El-Diasty, M.; El-Rabbany, A.; Pagiatakis, S. Temperature variation effects on stochastic characteristics for low-cost MEMS-based inertial sensor error. Meas. Sci. Technol. 2007, 18, 3321. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject | Age (y) | Gender | Height (cm) | Weight (kg) | Injury Level | AIS * Grade | Time Post Injury (y) |
|---|---|---|---|---|---|---|---|
| S1 | 50 | F | 168 | 58.5 | C7 | B | 24 |
| S2 | 69 | M | 168 | 77.1 | T5 | D | 5 |
| S3 | 59 | F | 173 | 84.9 | C4–C7 | C | 4 |
| S4 | 46 | F | 173 | 84.9 | T4 | A | 10 |
| S5 | 62 | M | 191 | 93.8 | T11 | B | 12 |
| S6 | 31 | M | 188 | 66.2 | C5 | C | 10 |
| Subject | Correlation Coefficient (r) | RMSE (°) | ||||||
|---|---|---|---|---|---|---|---|---|
| Pitch | Roll | Pitch | Roll | |||||
| Weighted | Townsend | Weighted | Townsend | Weighted | Townsend | Weighted | Townsend | |
| S1 | 0.991 | 0.991 | 0.994 | 0.993 | 2.69 | 2.73 | 2.12 | 2.16 |
| S2 | 0.958 | 0.940 | 0.993 | 0.993 | 4.13 | 4.96 | 2.46 | 2.50 |
| S3 | 0.983 | 0.981 | 0.996 | 0.996 | 4.26 | 4.52 | 2.25 | 2.25 |
| S4 | 0.984 | 0.983 | 0.993 | 0.992 | 3.81 | 3.99 | 3.44 | 3.88 |
| S5 | 0.959 | 0.959 | 0.983 | 0.986 | 5.10 | 5.12 | 3.98 | 3.91 |
| S6 | 0.984 | 0.983 | 0.990 | 0.991 | 4.04 | 4.26 | 3.52 | 3.50 |
| Average | 0.976 | 0.973 | 0.991 | 0.992 | 4.01 | 4.26 | 2.96 | 3.03 |
| STD | 0.014 | 0.019 | 0.004 | 0.003 | 0.78 | 0.86 | 0.78 | 0.82 |
| Subject | Correlation Coefficient (r) | RMSE (°) | ||||||
|---|---|---|---|---|---|---|---|---|
| Pitch | Roll | Pitch | Roll | |||||
| Weighted | Townsend | Weighted | Townsend | Weighted | Townsend | Weighted | Townsend | |
| S1 | 0.972 | 0.972 | 0.984 | 0.984 | 4.83 | 4.83 | 3.63 | 3.63 |
| S2 | 0.847 | 0.847 | 0.968 | 0.968 | 8.25 | 8.25 | 7.26 | 7.26 |
| S3 | 0.931 | 0.931 | 0.925 | 0.925 | 8.89 | 8.89 | 9.57 | 9.57 |
| S4 | 0.931 | 0.938 | 0.995 | 0.995 | 8.02 | 8.06 | 8.11 | 8.11 |
| S5 | 0.959 | 0.959 | 0.979 | 0.979 | 5.52 | 5.53 | 5.12 | 5.12 |
| S6 | 0.957 | 0.957 | 0.981 | 0.981 | 7.35 | 7.35 | 7.49 | 7.49 |
| Average | 0.934 | 0.934 | 0.972 | 0.972 | 7.14 | 7.15 | 6.86 | 6.86 |
| STD | 0.045 | 0.045 | 0.024 | 0.024 | 1.62 | 1.62 | 2.14 | 2.14 |
| Source | Activity | Population | Sensor | r | RMSE (°) |
|---|---|---|---|---|---|
| Motion Capture Calibration | Leaning | Individuals with SCI | Six 3-axis accelerometers | 0.97 | 5 |
| Clinical Calibration | Leaning | Individuals with SCI | Six 3-axis accelerometers | 0.93 | 7 |
| Mazza et al. [31] | Walking | Able-bodied | 9-axis IMU | 0.91 | 1 |
| Punchihewa et al. [32] | Baseball hitting | Able-bodied | Two 9-axis IMU | 0.95 | 5 |
| Grimpampi et al. [30] | Walking | Individuals with hemiplegia or Parkinson’s | 3-axis gyroscope | 0.74 | 1.3 plus a 2 offset |
| Luinge et al. [33] | Lifting crates | Able-bodied | 6-axis IMU | N/A | 3 |
| Luinge et al. [34] | Lifting crates | Able-bodied | 3-axis accelerometer | N/A | 2 |
| Brouwer et al. [35] | Dynamic sport motions | Able-bodied | Two 9-axis IMU | 0.85 | 5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Friederich, A.R.W.; Audu, M.L.; Triolo, R.J. Trunk Posture from Randomly Oriented Accelerometers. Sensors 2022, 22, 7690. https://doi.org/10.3390/s22197690
Friederich ARW, Audu ML, Triolo RJ. Trunk Posture from Randomly Oriented Accelerometers. Sensors. 2022; 22(19):7690. https://doi.org/10.3390/s22197690
Chicago/Turabian StyleFriederich, Aidan R. W., Musa L. Audu, and Ronald J. Triolo. 2022. "Trunk Posture from Randomly Oriented Accelerometers" Sensors 22, no. 19: 7690. https://doi.org/10.3390/s22197690
APA StyleFriederich, A. R. W., Audu, M. L., & Triolo, R. J. (2022). Trunk Posture from Randomly Oriented Accelerometers. Sensors, 22(19), 7690. https://doi.org/10.3390/s22197690