
Dental Implant Navigation System Based on Trinocular Stereo Vision




Abstract
:1. Introduction
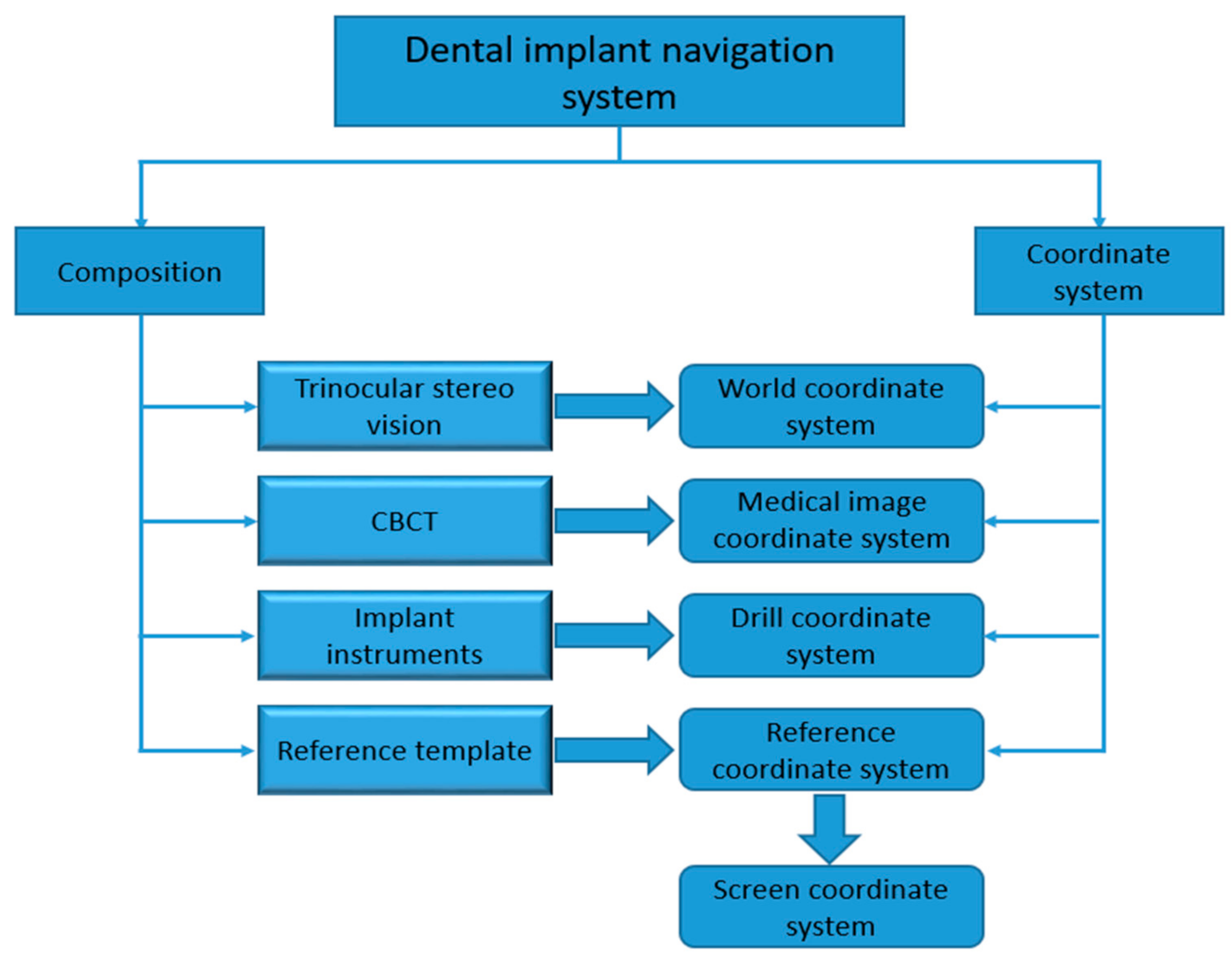
2. System Setup and Principal
2.1. Trinocular Stereo Vision
2.1.1. Trinocular Stereo Vision Calibration
2.1.2. Feature Point Matching
2.2. Medical Image Data
2.3. Implant Instruments Calibration
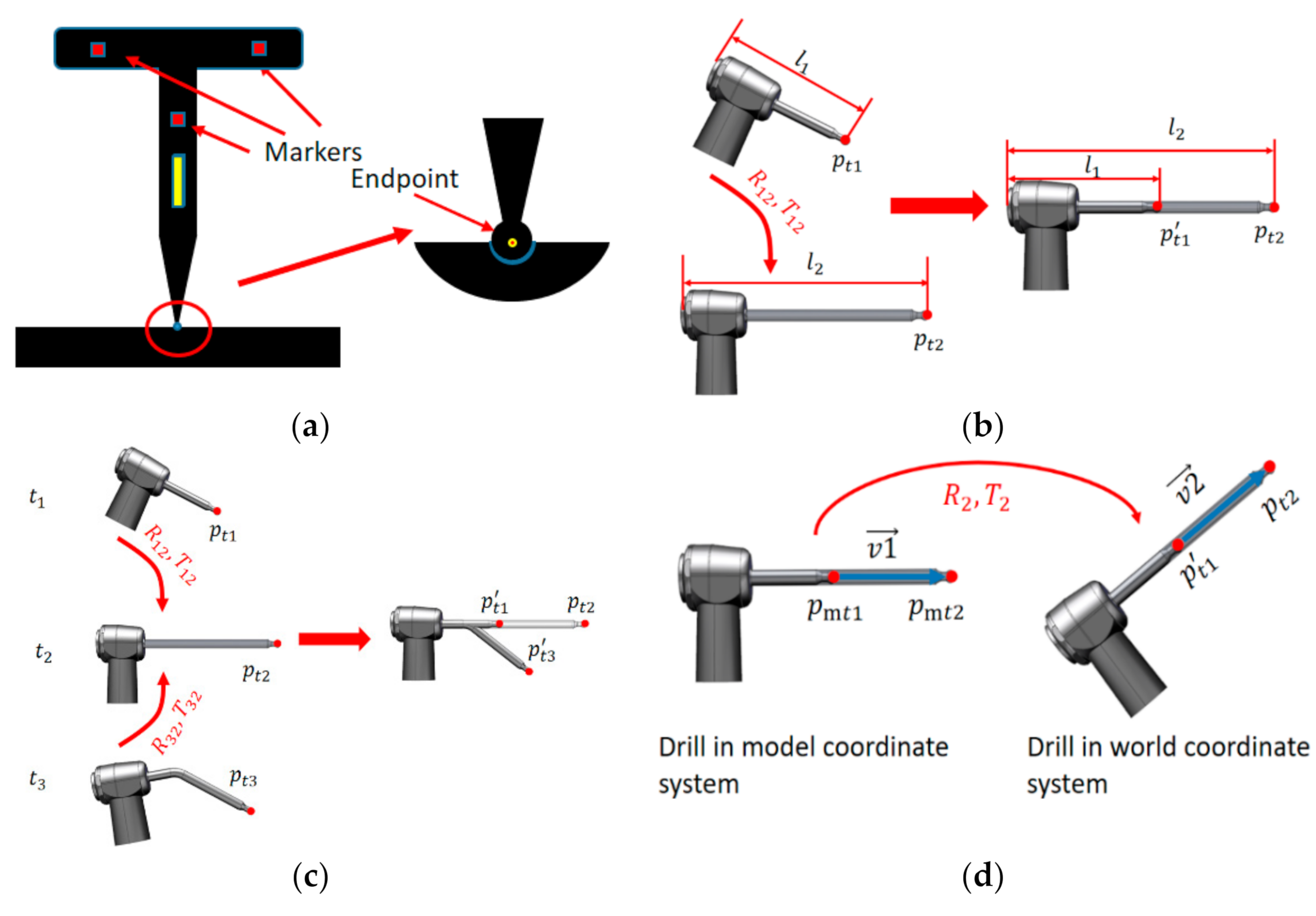
2.3.1. Endpoint Calibration
2.3.2. Axis Calibration
- (1)
- A short ball drill is installed on the self-designed implant instrument, and the effective length of the drill is recorded. The first calibration is completed by using the calibration method in Section 2.3.1. Recorded data include endpoint coordinate and marker coordinates at time .
- (2)
- A long ball drill is installed on the self-designed implant instrument, and the effective length of the drill is recorded. The second calibration is also completed by using the calibration method in Section 2.3.1. Recorded data include endpoint coordinate and marker coordinates at time .
2.3.3. Drill Calibration
2.4. Reference Template
3. Implant Hole Preparation Experiment and Result
- (1)
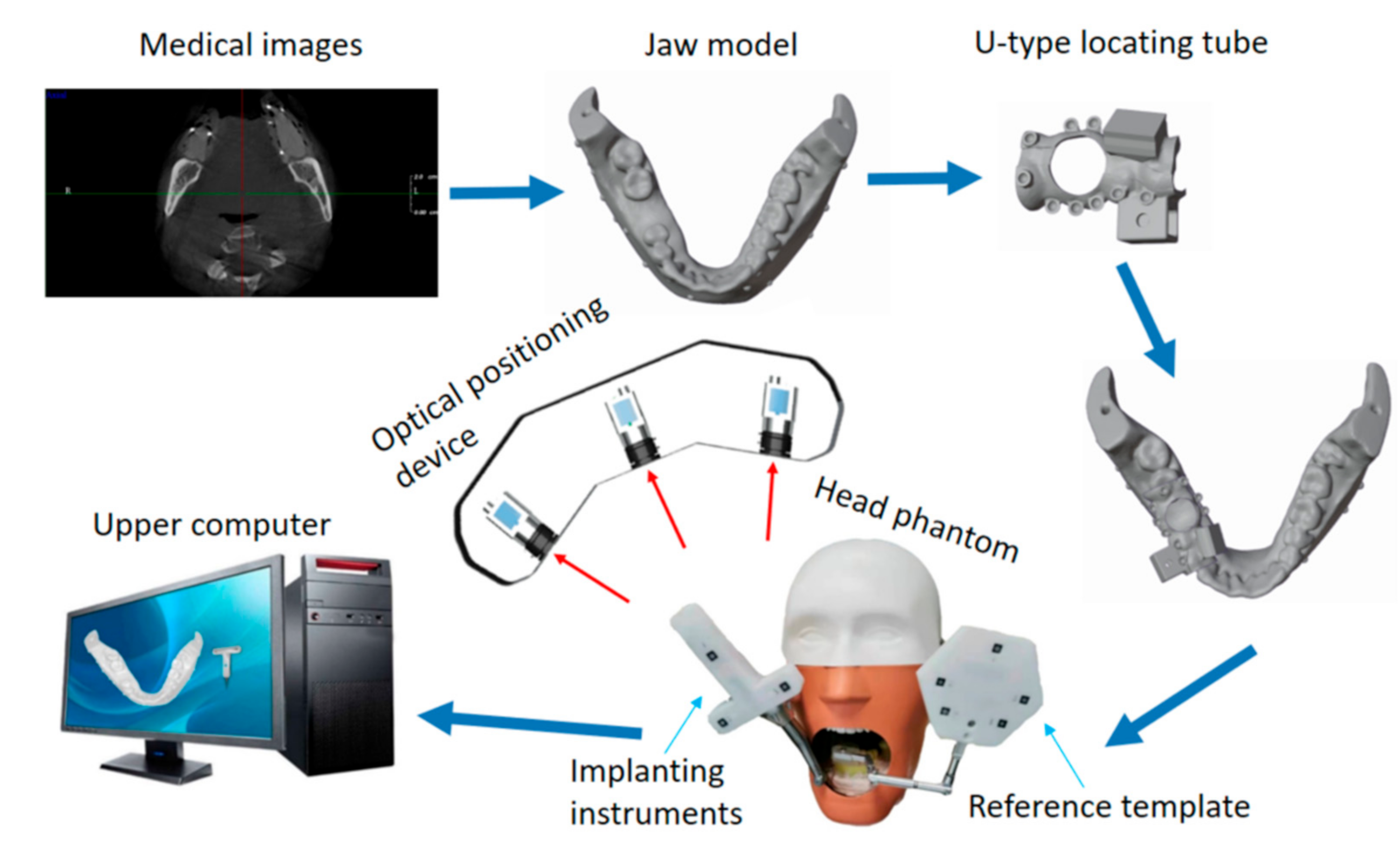
- CBCT data of dental is used to prepare a jaw model, along with the use of partly edentulous lower jaws with missing molars 46.
- (2)
- The U-type locating tube with development points is fixed in the model. The image data of the model are obtained by CBCT. The ideal planting axis was designed with self-designed software, and the coordinates of developing points in the image coordinate system are extracted, as shown in Figure 9a.
- (3)
- The jaw model is installed in the head phantom and is adjusted and fixed in the appropriate position. The reference template is clamped on the jaw model by a connecting rod, as shown in Figure 7, and the template is adjusted to the appropriate position and angle to suit the TSV measurement field of view.
- (4)
- The endpoint, axis, and drill are calculated based on the algorithm in Section 2.3. After calibration, the position and posture of the drill can be displayed in real time on the upper computer.
- (5)
- The markers on the U-type locating tube are clicked in a certain order to complete image registration.
- (6)
- The drill is replaced and the implant instrument is adjusted to drill under the guidance of the navigation software, as shown in Figure 10.
- (7)
- Boreholes are measured to obtain the deviation between the actual planting axis and the ideal planting axis.
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Van Oosterom, M.N.; den Houting, D.A.; van de Velde, C.J.; van Leeuwen, F.W. Navigating surgical fluorescence cameras using near-infrared optical tracking. J. Biomed. Opt. 2018, 23, 056003. [Google Scholar] [CrossRef] [PubMed]
- Clark, D.; Barbu, H.; Lorean, A.; Mijiritsky, E.; Levin, L. Incidental findings of implant complications on postimplantation CBCTs: A cross-sectional study. Clin. Implant. Dent. Relat. Res. 2017, 19, 776–782. [Google Scholar] [CrossRef] [PubMed]
- Cheng, K.J.; Kan, T.S.; Liu, Y.F.; Zhu, W.D.; Zhu, F.D.; Wang, W.B.; Jiang, X.F.; Dong, X.T. Accuracy of dental implant surgery with robotic position feedback and registration algorithm: An in-vitro study. Comput. Biol. Med. 2021, 129, 104153. [Google Scholar] [CrossRef] [PubMed]
- Bover-Ramos, F.; Viña-Almunia, J.; Cervera-Ballester, J.; Peñarrocha-Diago, M.; García-Mira, B. Accuracy of implant placement with computer-guided surgery: A systematic review and meta-analysis comparing cadaver, clinical, and in vitro studies. Int. J. Oral Maxillofac. Implant. 2018, 33, 101–115. [Google Scholar] [CrossRef]
- Sun, T.M.; Lee, H.E.; Lan, T.H. The influence of dental experience on a dental implant navigation system. BMC Oral Health 2019, 19, 222. [Google Scholar] [CrossRef] [Green Version]
- Jacobs, R.; Salmon, B.; Codari, M.; Hassan, B.; Bornstein, M.M. Cone beam computed tomography in implant dentistry: Recommendations for clinical use. BMC Oral Health 2018, 18, 88. [Google Scholar] [CrossRef] [Green Version]
- Wu, Y.; Wang, F.; Tao, B.; Lan, K. Real-time navigation system in implant dentistry. Comput.-Aided Oral Maxillofac. Surg. 2021, 223–253. [Google Scholar] [CrossRef]
- Fang, J.; Sun, Y.; Sun, X.L.; Wang, H.C.; Lyu, H.X.; Zhou, Y.M. Application of navigation system for dental implant in crossing-over the inferior alveolar nerve: A case report. Chin. J. Stomatol. 2021, 56, 377–379. [Google Scholar]
- Zhang, T.; Hu, J. Research progress on the application of surgical template and dynamic navigation system in implant dentistry. Int. J. Stomatol. 2019, 46, 99–104. [Google Scholar]
- Roberts, D.W.; Strohbehn, J.W.; Hatch, J.F.; Murray, W.; Kettenberger, H. A frameless stereotaxic integration of computerized tomographic imaging and the operating microscope. J. Neurosurg. 1986, 65, 545–549. [Google Scholar] [CrossRef]
- Mezger, U.; Jendrewski, C.; Bartels, M. Navigation in surgery. Langenbeck’s Arch. Surg. 2013, 398, 501–514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’haese, J.; Ackhurst, J.; Wismeijer, D.; De Bruyn, H.; Tahmaseb, A. Current state of the art of computer-guided implant surgery. Periodontology 2017, 73, 121–133. [Google Scholar] [CrossRef] [PubMed]
- Sießegger, M.; Schneider, B.T.; Mischkowski, R.A.; Lazar, F.; Krug, B.; Klesper, B.; Zöller, J.E. Use of an image-guided navigation system in dental implant surgery in anatomically complex operation sites. J. Craniomaxillofac. Surg. 2001, 29, 276–281. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Wang, F.; Fan, S.; Chow, J.K.F. Robotics in dental implantology. Oral Macillofac. Surg. Clin. 2019, 31, 513–518. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; Fan, J.; Tao, B.; Wang, S.; Mo, J.; Wu, Y.; Liang, Q.; Chen, X. An image-guided hybrid robot system for dental implant surgery. Int. J. Comput.-Assist. Radiol. Surg. 2021, 17, 15–26. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z. A flexible new technique for camera calibration. IEEE Trans. Pattern Anal. Mach. Intell. 2000, 22, 1330–1334. [Google Scholar] [CrossRef] [Green Version]
- Rueß, D.; Reulke, R. Ellipse constraints for improved wide-baseline feature matching and reconstruction. In Proceedings of the International Workshop on Combinatorial Image Analysis, Madrid, Spain, 23–25 May 2011. [Google Scholar]
- Lin, Q.; Yang, R.; Zhang, Z.; Cai, K.; Wang, Z.; Huang, M.; Huang, J.; Zhan, Y.; Zhuang, J. Robust stereo-match algorithm for infrared markers in image-guided optical tracking system. IEEE Access 2018, 6, 52421–52433. [Google Scholar] [CrossRef]
- Fan, B.; Wu, F.; Hu, Z. Robust line matching through line–point invariants. Pattern Recogn. 2012, 45, 794–805. [Google Scholar] [CrossRef]
- Duan, K.R.; Liu, X.Y. Research on coded reference point detection in photogrammetry. Transducer Microsyst. Technol. 2010, 29, 74. [Google Scholar]
- Bao, Y.; Shang, Y.; Sun, X.; Zhou, J. A robust recognition and accurate locating method for circular coded diagonal target. In Proceedings of the AOPC 2017: 3D Measurement Technology for Intelligent Manufacturing, Beijing, China, 4–6 June 2017; International Society for Optics and Photonics: Bellingham, WA, USA, 2017. [Google Scholar]
- Hung, K.; Huang, W.; Wang, F.; Wu, Y. Real-time surgical navigation system for the placement of zygomatic Implant. with severe bone deficiency. Int. J. Oral Maxillofac. Implant. 2016, 31, 1444–1449. [Google Scholar] [CrossRef] [Green Version]
- Beretta, M.; Poli, P.P.; Maiorana, C. Accuracy of computer-aided template-guided oral implant placement: A prospective clinical study. J. Periodontal. Implant. Sci. 2014, 44, 184–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Block, M.S.; Emery, R.W.; Lank, K.; Ryan, J. Implant placement accuracy using dynamic navigation. Int. J. Oral Maxillofac. Implant. 2017, 32, 92–99. [Google Scholar] [CrossRef] [PubMed]
- Tahmaseb, A.; Wismeijer, D.; Coucke, W.; Derksen, W. Computer technology applications in surgical implant dentistry: A systematic review. Int. J. Oral Maxillofac. Implant. 2014, 29, 25–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stefanelli, L.V.; DeGroot, B.S.; Lipton, D.I.; Mandelaris, G.A. Accuracy of a dynamic dental implant navigation system in a private practice. Int. J. Oral Maxillofac. Implant. 2019, 34, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Bi, S.; Gu, Y.; Zou, J.; Wang, L.; Zhai, C.; Gong, M. High precision optical tracking system based on near infrared trinocular stereo vision. Sensors 2021, 21, 2528. [Google Scholar] [CrossRef]
- Zhao, X.Z.; Xu, W.H.; Tang, Z.H.; Wu, M.J.; Zhu, J.; Chen, S. Accuracy of computer-guided implant surgery by a CAD/CAM and laser scanning technique. Chin. J. Dent. Res. 2014, 17, 31–36. [Google Scholar]
- Li, Y.; Hu, J.; Tao, B.; Yu, D.; Shen, Y.; Fan, S.; Wu, Y.; Chen, X. Automatic robot-world calibration in an optical-navigated surgical robot system and its application for oral implant placement. Int. J. Comput.-Assist. Radiol. Surg. 2020, 15, 1685–1692. [Google Scholar] [CrossRef]
- Qin, C.; Cao, Z.; Fan, S.; Wu, Y.; Sun, Y.; Politis, C.; Wang, C.; Chen, X. An oral and maxillofacial navigation system for implant placement with automatic identification of fiducial points. Int. J. Comput.-Assist. Radiol. Surg. 2019, 14, 281–289. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Groups | Entry Deviation (mm) | Exit Deviation (mm) | Angle Deviation (degree) |
|---|---|---|---|
| 1 | 0.459 | 0.734 | 1.58 |
| 2 | 0.561 | 1.070 | 2.91 |
| 3 | 0.825 | 1.447 | 3.56 |
| 4 | 0.149 | 0.561 | 2.36 |
| 5 | 0.731 | 0.578 | 0.88 |
| 6 | 0.614 | 0.813 | 1.14 |
| 7 | 0.760 | 1.404 | 3.68 |
| 8 | 0.312 | 0.803 | 2.81 |
| 9 | 0.432 | 0.859 | 2.45 |
| 10 | 0.682 | 0.514 | 0.96 |
| Mean | 0.553 | 0.878 | 2.23 |
| Std | 0.203 | 0.315 | 0.989 |
| Method | Entry Deviation (mm) | Exit Deviation (mm) | Angle Deviation (degree) |
|---|---|---|---|
| Manual operation [11] | 1.67 | 2.51 | 7.69 |
| Block et al. [24] | 1.37 | 1.56 | 3.62 |
| Tahmaseb et al. [25] | 1.45 | 2.99 | 4.00 |
| Stefanelli et al. [26] | 0.71 | 1.00 | 2.26 |
| Proposed | 0.55 | 0.88 | 2.23 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bi, S.; Wang, M.; Zou, J.; Gu, Y.; Zhai, C.; Gong, M. Dental Implant Navigation System Based on Trinocular Stereo Vision. Sensors 2022, 22, 2571. https://doi.org/10.3390/s22072571
Bi S, Wang M, Zou J, Gu Y, Zhai C, Gong M. Dental Implant Navigation System Based on Trinocular Stereo Vision. Sensors. 2022; 22(7):2571. https://doi.org/10.3390/s22072571
Chicago/Turabian StyleBi, Songlin, Menghao Wang, Jiaqi Zou, Yonggang Gu, Chao Zhai, and Ming Gong. 2022. "Dental Implant Navigation System Based on Trinocular Stereo Vision" Sensors 22, no. 7: 2571. https://doi.org/10.3390/s22072571
APA StyleBi, S., Wang, M., Zou, J., Gu, Y., Zhai, C., & Gong, M. (2022). Dental Implant Navigation System Based on Trinocular Stereo Vision. Sensors, 22(7), 2571. https://doi.org/10.3390/s22072571