
Patient–Therapist Cooperative Hand Telerehabilitation through a Novel Framework Involving the Virtual Glove System

 ,
,  , , and
, , and 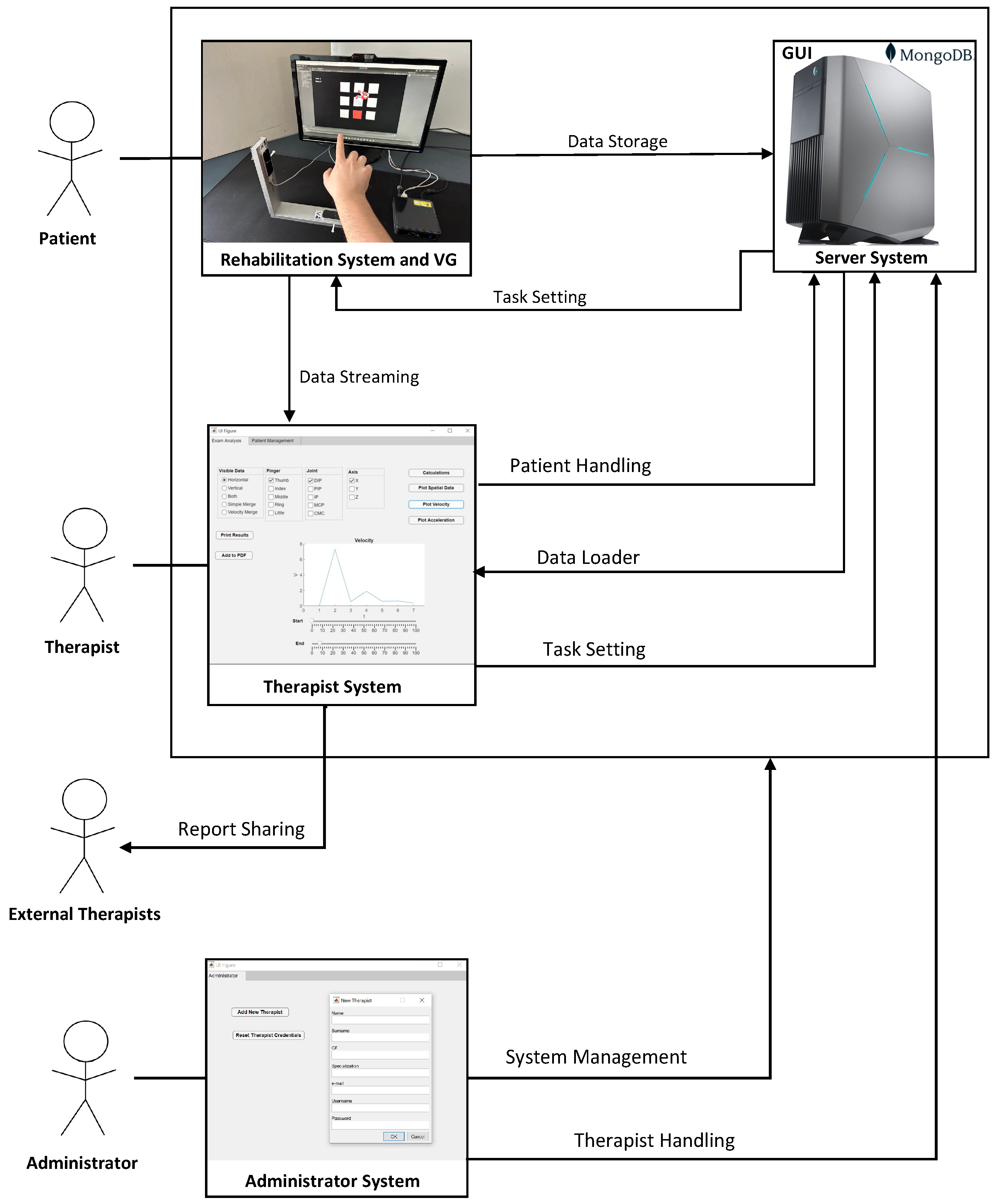{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
- support both supervised and unsupervised therapy;
- allow remote or “in-presence” therapy;
- support a client mode usage, robust in the case of a weak Internet connection;
- permit saving the history of the rehabilitation process of a person;
- provide an interface to the therapist for monitoring the rehabilitation progresses, managing patient and assigned rehabilitation tasks, data processing, and cooperating with other therapists by supporting data-sharing;
- recognize an administrator user that can manage the whole system.
2. The Cooperative Telerehabilitation Framework
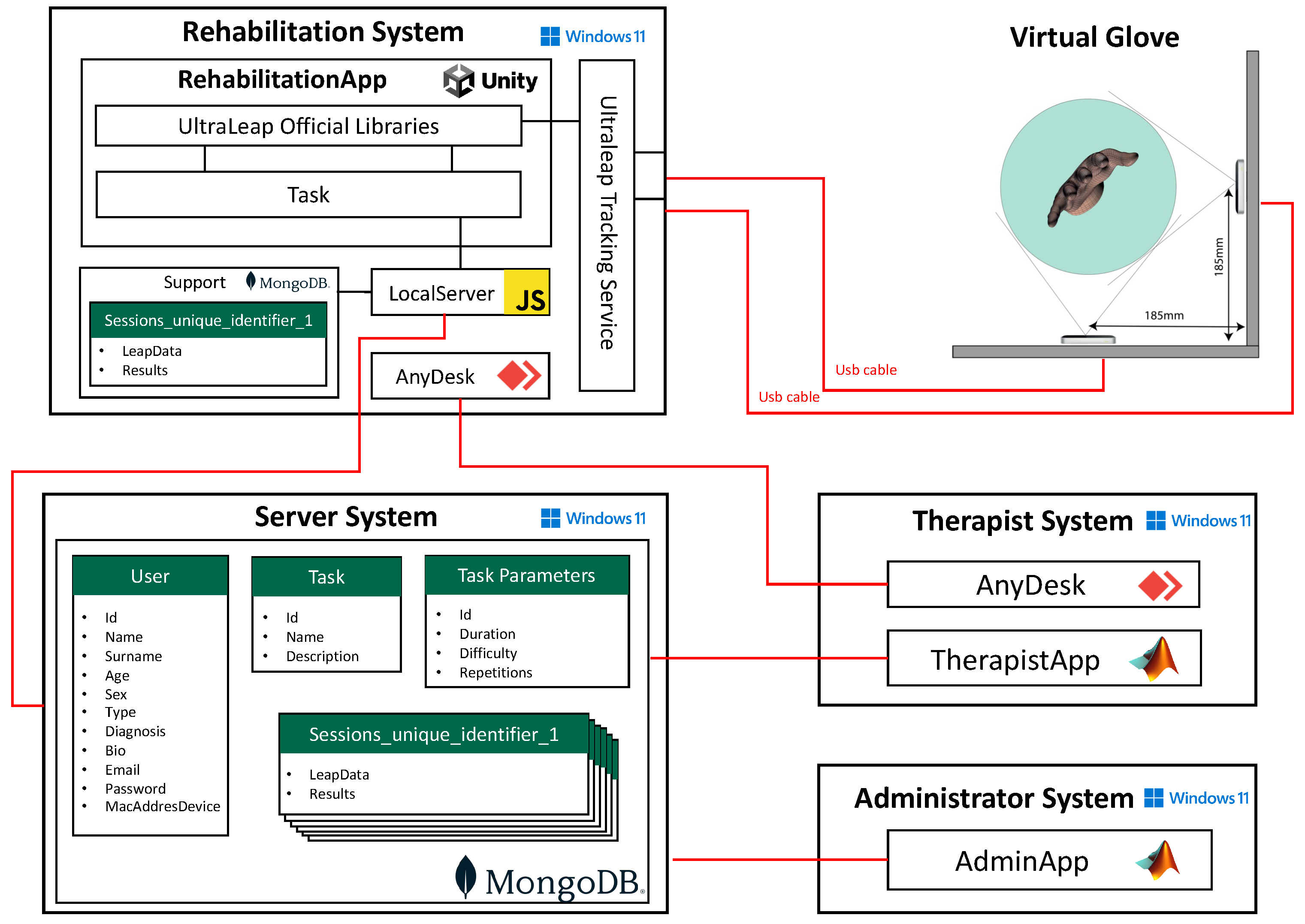
2.1. Hardware Architecture and Data Model
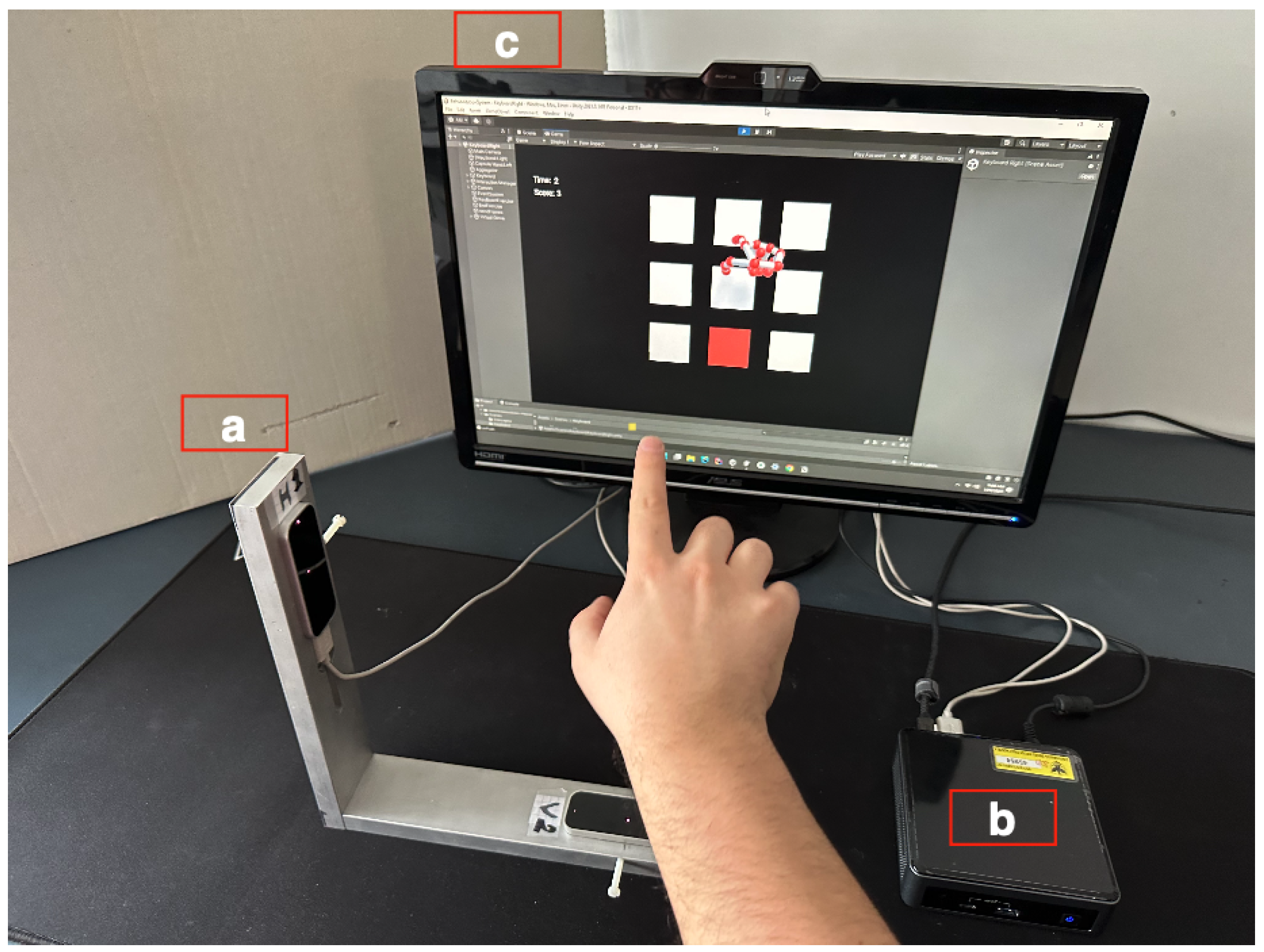
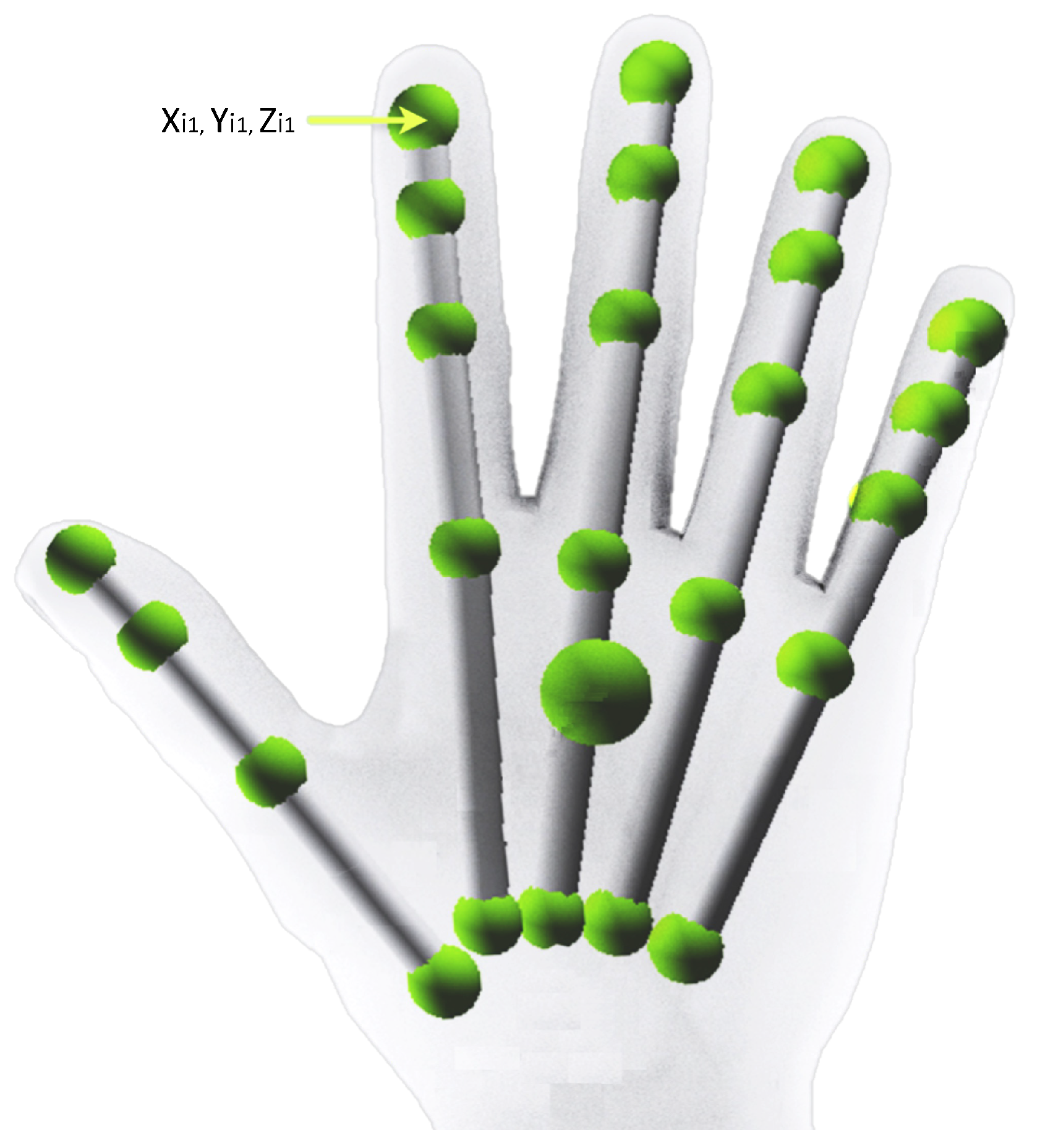
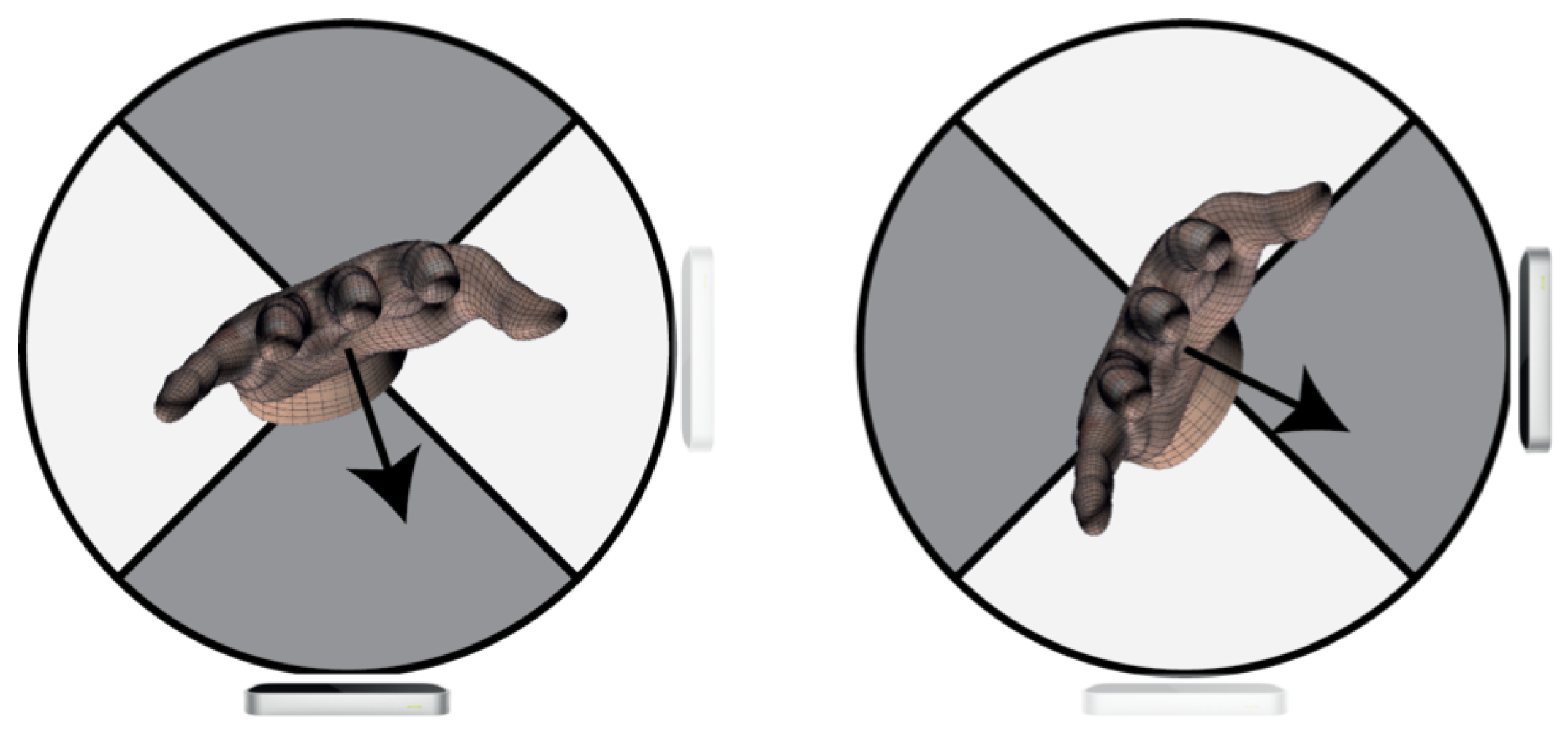
2.1.1. VG Architecture
2.1.2. Storage System
2.1.3. The Data Model
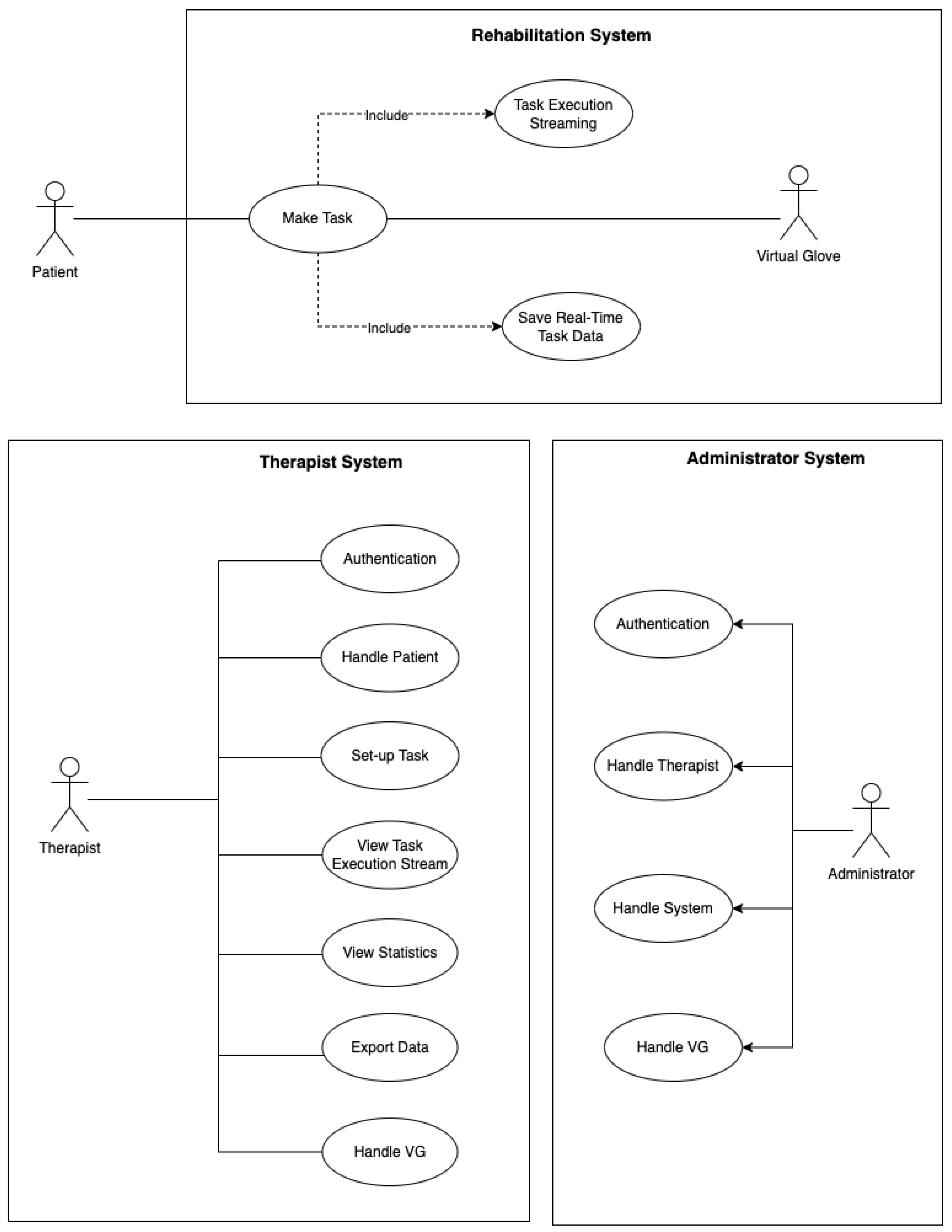
2.2. Use Cases and Software Architecture
2.2.1. Software Architecture
2.2.2. Rehabilitation System
2.2.3. The Server System
2.2.4. The Therapist System
2.2.5. Administrator System
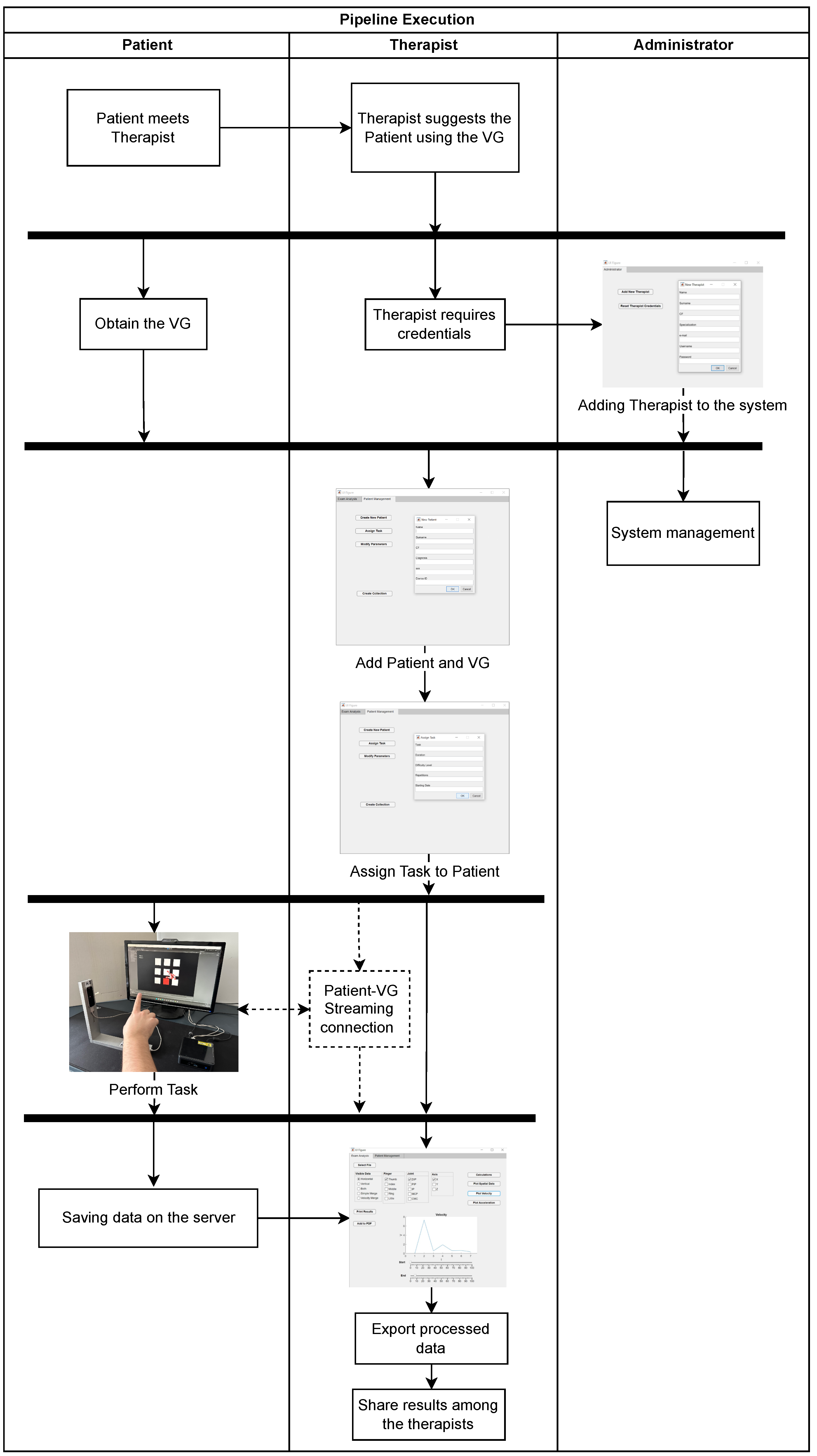
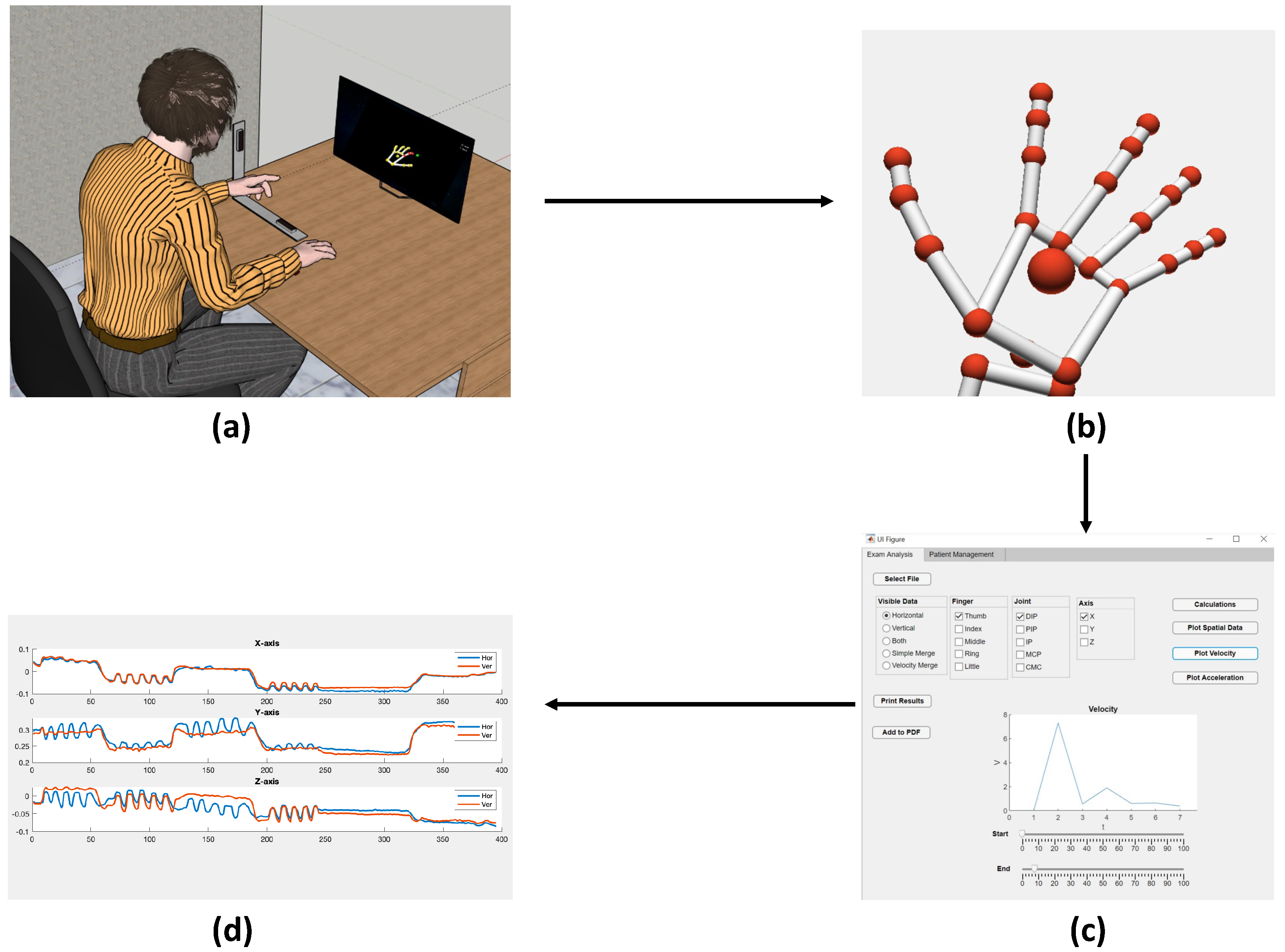
3. Execution Example
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Withers, H.G.; Glinsky, J.V.; Chu, J.; Jennings, M.D.; Hayes, A.J.; Starkey, I.J.; Palmer, B.A.; Szymanek, L.; Cruwys, J.J.; Wong, D.; et al. Face-to-face physiotherapy compared with a supported home exercise programme for the management of musculoskeletal conditions: Protocol of a multicentre, randomised controlled trial—The REFORM trial. BMJ Open 2021, 11, e041242. [Google Scholar] [CrossRef]
- Kwakkel, G. Intensity of practice after stroke: More is better. Power 2009, 7, 24. [Google Scholar]
- Kwakkel, G. Impact of intensity of practice after stroke: Issues for consideration. Disabil. Rehabil. 2006, 28, 823–830. [Google Scholar] [CrossRef] [PubMed]
- Standen, P.; Threapleton, K.; Richardson, A.; Connell, L.; Brown, D.; Battersby, S.; Platts, F.; Burton, A. A low cost virtual reality system for home based rehabilitation of the arm following stroke: A randomised controlled feasibility trial. Clin. Rehabil. 2016, 31, 340–350. [Google Scholar] [CrossRef] [PubMed]
- Nuara, A.; Fabbri-Destro, M.; Scalona, E.; Lenzi, S.E.; Rizzolatti, G.; Avanzini, P. Telerehabilitation in response to constrained physical distance: An opportunity to rethink neurorehabilitative routines. J. Neurol. 2022, 269, 627–638. [Google Scholar] [CrossRef]
- Sarfo, F.S.; Ulasavets, U.; Opare-Sem, O.K.; Ovbiagele, B. Tele-rehabilitation after stroke: An updated systematic review of the literature. J. Stroke Cerebrovasc. Dis. 2018, 27, 2306–2318. [Google Scholar] [CrossRef]
- Polsinelli, M.; Banchetti, P.A.; Cacchio, A.; Calvisi, V.; Marini, C.; Placidi, G.; Spezialetti, M.; Cinque, L. Hand movement parameters calculated by the LEAP based Virtual Glove. In Proceedings of the 2018 IEEE International Symposium on Medical Measurements and Applications (MeMeA), Rome, Italy, 11–13 June 2018. [Google Scholar] [CrossRef]
- Knepley, K.D.; Mao, J.Z.; Wieczorek, P.; Okoye, F.O.; Jain, A.P.; Harel, N.Y. Impact of telerehabilitation for stroke-related deficits. Telemed. E-Health 2021, 27, 239–246. [Google Scholar] [CrossRef]
- Gorman, C.; Gustafsson, L. The use of augmented reality for rehabilitation after stroke: A narrative review. Disabil. Rehabil. Assist. Technol. 2022, 17, 409–417. [Google Scholar] [CrossRef]
- Howard, M.C. A meta-analysis and systematic literature review of virtual reality rehabilitation programs. Comput. Hum. Behav. 2017, 70, 317–327. [Google Scholar] [CrossRef]
- Hao, J.; Pu, Y.; Chen, Z.; Siu, K.C. Effects of virtual reality-based telerehabilitation for stroke patients: A systematic review and meta-analysis of randomized controlled trials. J. Stroke Cerebrovasc. Dis. 2023, 32, 106960. [Google Scholar] [CrossRef] [PubMed]
- Pereira, M.F.; Prahm, C.; Kolbenschlag, J.; Oliveira, E.; Rodrigues, N.F. Application of AR and VR in hand rehabilitation: A systematic review. J. Biomed. Inform. 2020, 111, 103584. [Google Scholar] [CrossRef] [PubMed]
- Sheng, B.; Zhao, J.; Zhang, Y.; Xie, S.; Tao, J. Commercial device-based hand rehabilitation systems for stroke patients: State of the art and future prospects. Heliyon 2023, 9, e13588. [Google Scholar] [CrossRef] [PubMed]
- Demolder, C.; Molina, A.; Hammond, F.L., III; Yeo, W.H. Recent advances in wearable biosensing gloves and sensory feedback biosystems for enhancing rehabilitation, prostheses, healthcare, and virtual reality. Biosens. Bioelectron. 2021, 190, 113443. [Google Scholar] [CrossRef] [PubMed]
- Rashid, A.; Hasan, O. Wearable technologies for hand joints monitoring for rehabilitation: A survey. Microelectron. J. 2019, 88, 173–183. [Google Scholar] [CrossRef]
- Theodoridou, E.; Cinque, L.; Mignosi, F.; Placidi, G.; Polsinelli, M.; Tavares, J.M.R.; Spezialetti, M. Hand tracking and gesture recognition by multiple contactless sensors: A survey. IEEE Trans. Hum.-Mach. Syst. 2022, 53, 35–43. [Google Scholar] [CrossRef]
- Cortese, M.; Cempini, M.; de Almeida Ribeiro, P.R.; Soekadar, S.R.; Carrozza, M.C.; Vitiello, N. A mechatronic system for robot-mediated hand telerehabilitation. IEEE/ASME Trans. Mechatronics 2014, 20, 1753–1764. [Google Scholar] [CrossRef]
- Battaglia, E.; Bianchi, M.; Altobelli, A.; Grioli, G.; Catalano, M.G.; Serio, A.; Santello, M.; Bicchi, A. Thimblesense: A fingertip-wearable tactile sensor for grasp analysis. IEEE Trans. Haptics 2015, 9, 121–133. [Google Scholar] [CrossRef]
- Luzhnica, G.; Simon, J.; Lex, E.; Pammer, V. A sliding window approach to natural hand gesture recognition using a custom data glove. In Proceedings of the 2016 IEEE Symposium on 3D User Interfaces (3DUI), Greenville, SC, USA, 19–20 March 2016; pp. 81–90. [Google Scholar]
- Hadi, A.; Alipour, K.; Kazeminasab, S.; Elahinia, M. ASR glove: A wearable glove for hand assistance and rehabilitation using shape memory alloys. J. Intell. Mater. Syst. Struct. 2018, 29, 1575–1585. [Google Scholar] [CrossRef]
- Chen, X.; Gong, L.; Wei, L.; Yeh, S.C.; Da Xu, L.; Zheng, L.; Zou, Z. A wearable hand rehabilitation system with soft gloves. IEEE Trans. Ind. Inform. 2020, 17, 943–952. [Google Scholar] [CrossRef]
- Zhu, Y.; Gong, W.; Chu, K.; Wang, X.; Hu, Z.; Su, H. A Novel Wearable Soft Glove for Hand Rehabilitation and Assistive Grasping. Sensors 2022, 22, 6294. [Google Scholar] [CrossRef]
- Mouri, T.; Kawasaki, H.; Aoki, T.; Nishimoto, Y.; Ito, S.; Ueki, S. Telerehabilitation for fingers and wrist using a hand rehabilitation support system and robot hand. IFAC Proc. Vol. 2009, 42, 603–608. [Google Scholar] [CrossRef]
- Airò Farulla, G.; Pianu, D.; Cempini, M.; Cortese, M.; Russo, L.O.; Indaco, M.; Nerino, R.; Chimienti, A.; Oddo, C.M.; Vitiello, N. Vision-based pose estimation for robot-mediated hand telerehabilitation. Sensors 2016, 16, 208. [Google Scholar] [CrossRef] [Green Version]
- Ciorap, R.; Luca, C.; Andritoi, D.; Ciorap, M. Telerehabilitation Solution for Hand Therapy. In Proceedings of the 2020 International Conference and Exposition on Electrical Additionally, Power Engineering (EPE), Iasi, Romania, 22–23 October 2020; pp. 733–737. [Google Scholar]
- Golomb, M.R.; Warden, S.J.; Fess, E.; Rabin, B.; Yonkman, J.; Shirley, B.; Burdea, G.C. Maintained hand function and forearm bone health 14 months after an in-home virtual-reality videogame hand telerehabilitation intervention in an adolescent with hemiplegic cerebral palsy. J. Child Neurol. 2011, 26, 389–393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alamri, A.; Cha, J.; El Saddik, A. AR-REHAB: An augmented reality framework for poststroke-patient rehabilitation. IEEE Trans. Instrum. Meas. 2010, 59, 2554–2563. [Google Scholar] [CrossRef]
- Mousavi Hondori, H.; Khademi, M.; Dodakian, L.; Cramer, S.C.; Lopes, C.V. A spatial augmented reality rehab system for post-stroke hand rehabilitation. In Medicine Meets Virtual Reality 20; IOS Press: Amsterdam, The Netherlands, 2013; pp. 279–285. [Google Scholar]
- Placidi, G. A smart virtual glove for the hand telerehabilitation. Comput. Biol. Med. 2007, 37, 1100–1107. [Google Scholar] [CrossRef] [PubMed]
- Placidi, G.; Avola, D.; Iacoviello, D.; Cinque, L. Overall design and implementation of the virtual glove. Comput. Biol. Med. 2013, 43, 1927–1940. [Google Scholar] [CrossRef] [PubMed]
- Placidi, G.; Cinque, L.; Petracca, A.; Polsinelli, M.; Spezialetti, M. A Virtual Glove System for the Hand Rehabilitation based on Two Orthogonal LEAP Motion Controllers. In Proceedings of the ICPRAM, Porto, Portugal, 24–26 February 2017; pp. 184–192. [Google Scholar]
- Placidi, G.; Cinque, L.; Polsinelli, M.; Spezialetti, M. Measurements by a LEAP-based virtual glove for the hand rehabilitation. Sensors 2018, 18, 834. [Google Scholar] [CrossRef] [Green Version]
- Placidi, G.; Di Matteo, A.; Mignosi, F.; Polsinelli, M.; Spezialetti, M. Compact, Accurate and Low-cost Hand Tracking System based on LEAP Motion Controllers and Raspberry Pi. In Proceedings of the ICPRAM, Online, 3–5 February 2022; pp. 652–659. [Google Scholar]
- Ovur, S.E.; Su, H.; Qi, W.; De Momi, E.; Ferrigno, G. Novel Adaptive Sensor Fusion Methodology for Hand Pose Estimation With Multileap Motion. IEEE Trans. Instrum. Meas. 2021, 70, 9507108. [Google Scholar] [CrossRef]
- Houston, A.; Walters, V.; Corbett, T.; Coppack, R. Evaluation of a multi-sensor Leap Motion setup for biomechanical motion capture of the hand. J. Biomech. 2021, 127, 110713. [Google Scholar] [CrossRef]
- Novacek, T.; Marty, C.; Jirina, M. Project MultiLeap: Fusing Data from Multiple Leap Motion Sensors. In Proceedings of the 2021 IEEE 7th International Conference on Virtual Reality (ICVR), Foshan, China, 20–22 May 2021; pp. 19–25. [Google Scholar]
- Guna, J.; Jakus, G.; Pogačnik, M.; Tomažič, S.; Sodnik, J. An analysis of the precision and reliability of the leap motion sensor and its suitability for static and dynamic tracking. Sensors 2014, 14, 3702–3720. [Google Scholar] [CrossRef] [Green Version]
- Tarakci, E.; Arman, N.; Tarakci, D.; Kasapcopur, O. Leap Motion Controller–based training for upper extremity rehabilitation in children and adolescents with physical disabilities: A randomized controlled trial. J. Hand Ther. 2020, 33, 220–228. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.; Saini, R.; Roy, P.P.; Pal, U. A lexicon-free approach for 3D handwriting recognition using classifier combination. Pattern Recognit. Lett. 2018, 103, 1–7. [Google Scholar] [CrossRef]
- Nizamis, K.; Rijken, N.; Mendes, A.; Janssen, M.; Bergsma, A.; Koopman, B. A Novel Setup and Protocol to Measure the Range of Motion of the Wrist and the Hand. Sensors 2018, 18, 3230. [Google Scholar] [CrossRef] [Green Version]
- Gonçalves, R.S.; de Souza, M.R.S.B.; Carbone, G. Analysis of the Leap Motion Controller’s Performance in Measuring Wrist Rehabilitation Tasks Using an Industrial Robot Arm Reference. Sensors 2022, 22, 4880. [Google Scholar] [CrossRef]
- Bachmann, D.; Weichert, F.; Rinkenauer, G. Evaluation of the leap motion controller as a new contact-free pointing device. Sensors 2014, 15, 214–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Placidi, G.; Avola, D.; Cinque, L.; Polsinelli, M.; Theodoridou, E.; Tavares, J.M.R. Data integration by two-sensors in a LEAP-based Virtual Glove for human-system interaction. Multimed. Tools Appl. 2021, 80, 18263–18277. [Google Scholar] [CrossRef]
- Avola, D.; Spezialetti, M.; Placidi, G. Design of an efficient framework for fast prototyping of customized human–computer interfaces and virtual environments for rehabilitation. Comput. Methods Programs Biomed. 2013, 110, 490–502. [Google Scholar] [CrossRef]
- Petracca, A.; Carrieri, M.; Avola, D.; Moro, S.B.; Brigadoi, S.; Lancia, S.; Spezialetti, M.; Ferrari, M.; Quaresima, V.; Placidi, G. A virtual ball task driven by forearm movements for neuro-rehabilitation. In Proceedings of the 2015 International Conference on Virtual Rehabilitation (ICVR), Valencia, Spain, 9–12 June 2015. [Google Scholar] [CrossRef]








Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Placidi, G.; Di Matteo, A.; Lozzi, D.; Polsinelli, M.; Theodoridou, E. Patient–Therapist Cooperative Hand Telerehabilitation through a Novel Framework Involving the Virtual Glove System. Sensors 2023, 23, 3463. https://doi.org/10.3390/s23073463
Placidi G, Di Matteo A, Lozzi D, Polsinelli M, Theodoridou E. Patient–Therapist Cooperative Hand Telerehabilitation through a Novel Framework Involving the Virtual Glove System. Sensors. 2023; 23(7):3463. https://doi.org/10.3390/s23073463
Chicago/Turabian StylePlacidi, Giuseppe, Alessandro Di Matteo, Daniele Lozzi, Matteo Polsinelli, and Eleni Theodoridou. 2023. "Patient–Therapist Cooperative Hand Telerehabilitation through a Novel Framework Involving the Virtual Glove System" Sensors 23, no. 7: 3463. https://doi.org/10.3390/s23073463
APA StylePlacidi, G., Di Matteo, A., Lozzi, D., Polsinelli, M., & Theodoridou, E. (2023). Patient–Therapist Cooperative Hand Telerehabilitation through a Novel Framework Involving the Virtual Glove System. Sensors, 23(7), 3463. https://doi.org/10.3390/s23073463