

The Validity and Reliability of Self-Reported Adherence to Using Offloading Treatment in People with Diabetes-Related Foot Ulcers
 , , ,
, , , 
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Settings
2.2. Participants
2.3. Variables Collected
2.4. Outcome Measures
2.4.1. Self-Reported Adherence
2.4.2. Objective Adherence (Criterion Measure)
2.5. Procedure
2.6. Statistical Analysis
3. Results
3.1. Characteristics
3.2. Adherence
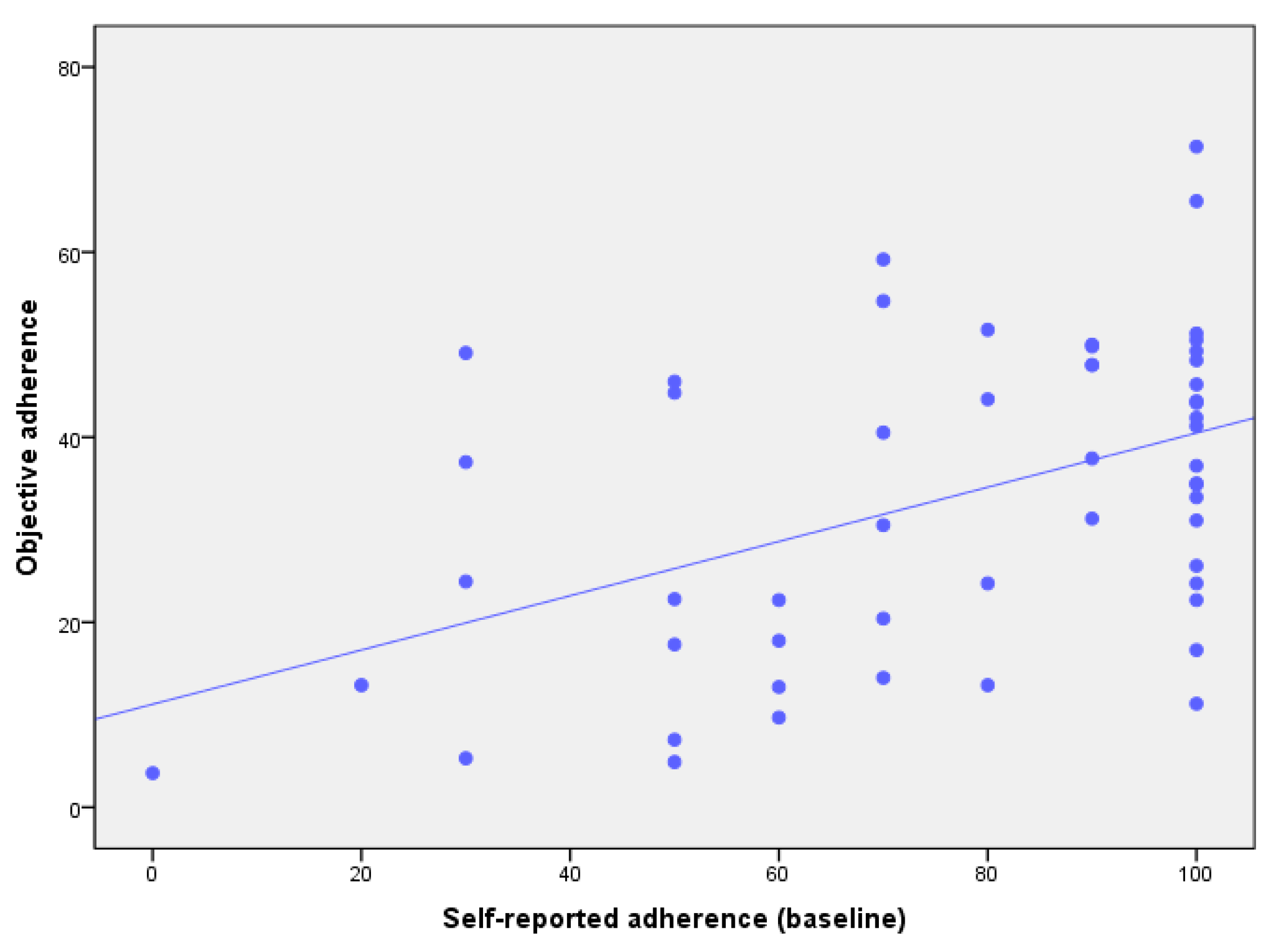
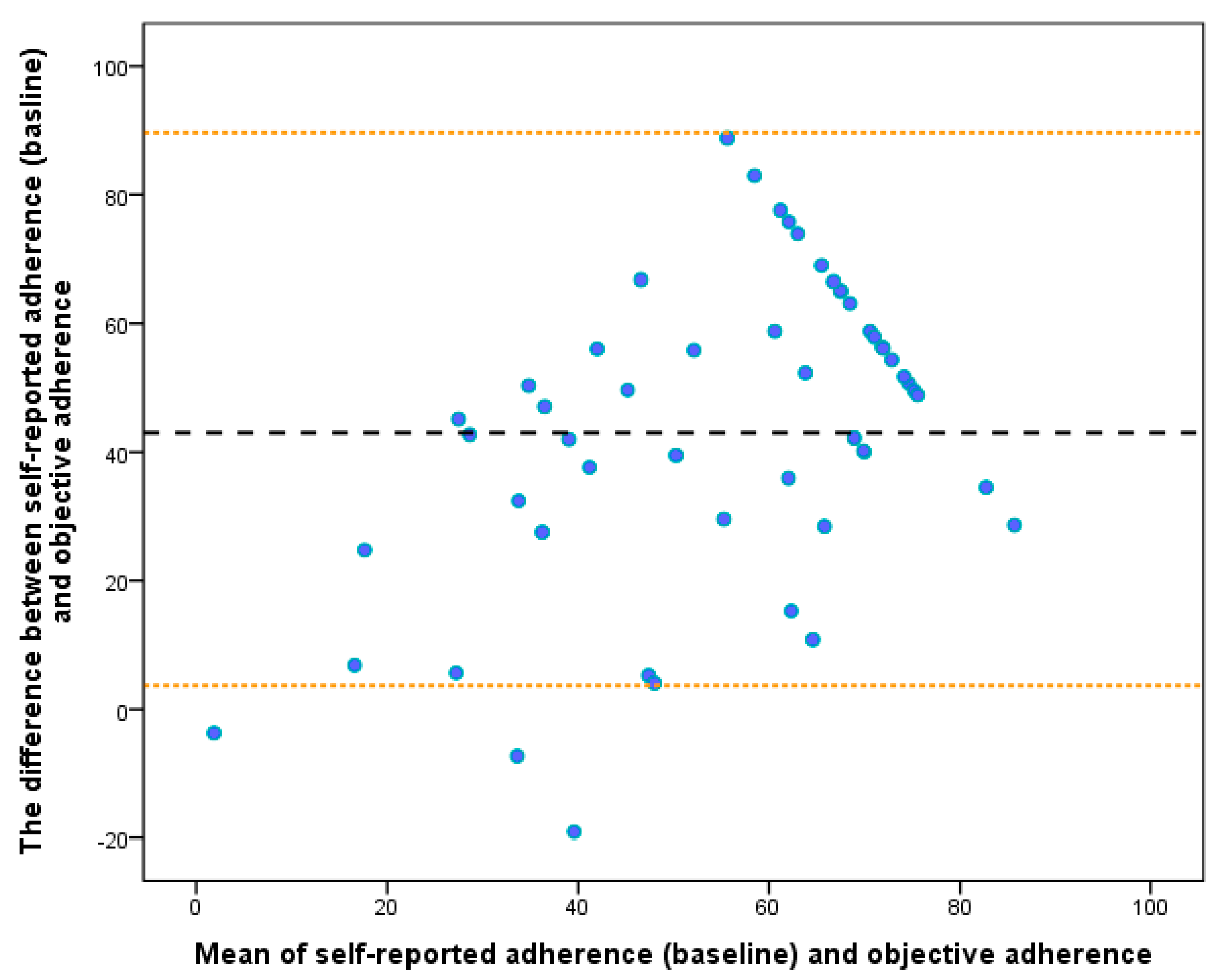
3.3. Validity
3.4. Reliability
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhang, Y.; Lazzarini, P.A.; McPhail, S.M.; van Netten, J.J.; Armstrong, D.G.; Pacella, R.E. Global disability burdens of diabetes-related lower-extremity complications in 1990 and 2016. Diabetes Care 2020, 43, 964–974. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, D.G.; Boulton, A.J.; Bus, S.A. Diabetic foot ulcers and their recurrence. N. Engl. J. Med. 2017, 376, 2367–2375. [Google Scholar] [CrossRef] [PubMed]
- Quigley, M.; Morton, J.I.; Lazzarini, P.A.; Zoungas, S.; Shaw, J.E.; Magliano, D.J. Trends in diabetes-related foot disease hospitalizations and amputations in Australia, 2010 to 2019. Diabetes Res. Clin. Pract. 2022, 194, 110189. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, D.G.; Swerdlow, M.A.; Armstrong, A.A.; Conte, M.S.; Padula, W.V.; Bus, S.A. Five year mortality and direct costs of care for people with diabetic foot complications are comparable to cancer. J. Foot Ankle Res. 2020, 13, 16. [Google Scholar] [CrossRef] [PubMed]
- Lazzarini, P.A.; Cramb, S.M.; Golledge, J.; Morton, J.I.; Magliano, D.J.; Van Netten, J.J. Global trends in the incidence of hospital admissions for diabetes-related foot disease and amputations: A review of national rates in the 21st century. Diabetologia 2022, 66, 267–287. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Carter, H.E.; Lazzarini, P.A.; Cramb, S.; Pacella, R.; van Netten, J.J.; Cheng, Q.; Derhy, P.H.; Kinnear, E.M.; McPhail, S.M. Cost-effectiveness of guideline-based care provision for patients with diabetes-related foot ulcers: A modelled analysis using discrete event simulation. Diabet. Med. 2023, 40, e14961. [Google Scholar] [CrossRef]
- Bus, S.A.; Armstrong, D.G.; Gooday, C.; Jarl, G.; Caravaggi, C.; Viswanathan, V.; Lazzarini, P.A. Guidelines on offloading foot ulcers in persons with diabetes (IWGDF 2019 update). Diabetes/Metab. Res. Rev. 2020, 36 (Suppl. 1), e3274. [Google Scholar] [CrossRef]
- Lazzarini Jarl, G.; Gooday, C.; Viswanathan, V.; Caravaggi, C.F.; Armstrong, D.G.; Bus, S.A. Effectiveness of offloading interventions to heal foot ulcers in persons with diabetes: A systematic review. Diabetes/Metab. Res. Rev. 2020, 36 (Suppl. 1), e3275. [Google Scholar] [CrossRef]
- Boulton, A.; Armstrong, D.; Krisner, R.; Attinger, C.; Lavery, L.; Lipsky, B.; Mills, J.; Steinberg, J. Diagnosis and Management of Diabetic Foot Complications. ADA Clin. Compend. 2018, 2018, 1–20. [Google Scholar] [CrossRef]
- Fife, C.E.; Carter, M.J.; Walker, D.; Thomson, B.; Eckert, K.A. Diabetic foot ulcer off-loading: The gap between evidence and practice. Data from the US Wound Registry. Adv. Skin Wound Care 2014, 27, 310–316. [Google Scholar] [CrossRef]
- Wu, S.C.; Jensen, J.L.; Weber, A.K.; Robinson, D.E.; Armstrong, D.G. Use of pressure offloading devices in diabetic foot ulcers: Do we practice what we preach? Diabetes Care 2008, 31, 2118–2119. [Google Scholar] [CrossRef] [PubMed]
- Raspovic, A.; Landorf, K.B. A survey of offloading practices for diabetes-related plantar neuropathic foot ulcers. J. Foot Ankle Res. 2014, 7, 35. [Google Scholar] [CrossRef] [PubMed]
- Quinton, T.R.; Lazzarini, P.A.; Boyle, F.M.; Russell, A.W.; Armstrong, D.G. How do Australian podiatrists manage patients with diabetes? The Australian diabetic foot management survey. J. Foot Ankle Res. 2015, 8, 16. [Google Scholar] [CrossRef] [PubMed]
- Bus, S.A.; Van Netten, J.J.; Kottink, A.I.; Manning, E.A.; Spraul, M.; Woittiez, A.-J.; Van Baal, J.G. The efficacy of removable devices to offload and heal neuropathic plantar forefoot ulcers in people with diabetes: A single-blinded multicentre randomised controlled trial. Int. Wound J. 2017, 15, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Crews Shen, B.-J.; Campbell, L.; Lamont, P.J.; Boulton, A.J.; Peyrot, M.; Kirsner, R.S.; Vileikyte, L. Role and determinants of adherence to off-loading in diabetic foot ulcer healing: A prospective investigation. Diabetes Care 2016, 39, 1371–1377. [Google Scholar] [CrossRef]
- Ababneh, A.; Finlayson, K.; Edwards, H.; Lazzarini, P.A. Factors associated with adherence to using removable cast walker treatment among patients with diabetes-related foot ulcers. BMJ Open Diabetes Res. Care 2022, 10, e002640. [Google Scholar] [CrossRef]
- Lazzarini, P.A.; Crews, R.T.; van Netten, J.J.; Bus, S.A.; Fernando, M.E.; Chadwick, P.J.; Najafi, B. Measuring Plantar Tissue Stress in People With Diabetic Peripheral Neuropathy: A Critical Concept in Diabetic Foot Management. J. Diabetes Sci. Technol. 2019, 13, 869–880. [Google Scholar] [CrossRef]
- Park, C.; Mishra, R.; Vigano, D.; Macagno, M.; Rossotti, S.; D’huyvetter, K.; Garcia, J.; Armstrong, D.G.; Najafi, B. Smart Offloading Boot System for Remote Patient Monitoring: Toward Adherence Reinforcement and Proper Physical Activity Prescription for Diabetic Foot Ulcer Patients. J. Diabetes Sci. Technol. 2022, 17, 42–51. [Google Scholar] [CrossRef]
- Bus, S.A.; Waaijman, R.; Nollet, F. New Monitoring Technology to Objectively Assess Adherence to Prescribed Footwear and Assistive Devices During Ambulatory Activity. Arch. Phys. Med. Rehabil. 2012, 93, 2075–2079. [Google Scholar] [CrossRef]
- Crews, R.T.; Armstrong, D.G.; Boulton, A.J. A method for assessing off-loading compliance. J. Am. Podiatr. Med. Assoc. 2009, 99, 100–103. [Google Scholar] [CrossRef]
- Crews, R.T.; Bowling, F.L.; Boulton, A.J. Controversies in off-loading: Should big brother be watching? Curr. Diabetes Rep. 2009, 9, 417–419. [Google Scholar] [CrossRef] [PubMed]
- Jarl, G.; Alnemo, J.; Tranberg, R.; Lundqvist, L.-O. Gender differences in attitudes and attributes of people using therapeutic shoes for diabetic foot complications. J. Foot Ankle Res. 2019, 12, 21. [Google Scholar] [CrossRef] [PubMed]
- Jarl, G. Methodological considerations of investigating adherence to using offloading devices among people with diabetes. Patient Prefer. Adherence 2018, 12, 1767–1775. [Google Scholar] [CrossRef] [PubMed]
- Stirratt, M.J.; Dunbar-Jacob, J.; Crane, H.M.; Simoni, J.M.; Czajkowski, S.; Hilliard, M.E.; Aikens, J.E.; Hunter, C.M.; Velligan, D.I.; Huntley, K.; et al. Self-report measures of medication adherence behavior: Recommendations on optimal use. Transl. Behav. Med. 2015, 5, 470–482. [Google Scholar] [CrossRef] [PubMed]
- Sangiorgio, S.N.; Ho, N.C.; Morgan, R.D.; Ebramzadeh, E.; Zionts, L.E. The objective measurement of brace-use adherence in the treatment of idiopathic clubfoot. JBJS 2016, 98, 1598–1605. [Google Scholar] [CrossRef]
- Morton, A.; Riddle, R.; Buchanan, R.; Katz, D.; Birch, J. Accuracy in the prediction and estimation of adherence to bracewear before and during treatment of adolescent idiopathic scoliosis. J. Pediatr. Orthop. 2008, 28, 336–341. [Google Scholar] [CrossRef]
- Nicolson, P.J.; Hinman, R.S.; Wrigley, T.V.; Stratford, P.W.; Bennell, K.L. Self-reported home exercise adherence: A validity and reliability study using concealed accelerometers. J. Orthop. Sport. Phys. Ther. 2018, 48, 943–950. [Google Scholar] [CrossRef]
- Van Netten, J.J.; Bus, S.A.; Apelqvist, J.; Lipsky, B.A.; Hinchliffe, R.J.; Game, F.; Rayman, G.; Lazzarini, P.A.; Forsythe, R.O.; Peters, E.J.G.; et al. Definitions and criteria for diabetic foot disease. Diabetes/Metab. Res. Rev. 2019, 36 (Suppl. 1), e3268. [Google Scholar] [CrossRef]
- Najafi, B.; Grewal, G.S.; Bharara, M.; Menzies, R.; Talal, T.K.; Armstrong, D.G. Can’t stand the pressure: The association between unprotected standing, walking, and wound healing in people with diabetes. J. Diabetes Sci. Technol. 2016, 11, 657–667. [Google Scholar] [CrossRef]
- Ababneh, A.N. Adherence to Wearing Removable Cast Walkers in Patients with Diabetes-Related Foot Ulcers: A Mixed Methods Investigation; Queensland University of Technology: Brisbane City, Australia, 2021. [Google Scholar]
- Blackman, N.J.M.; Koval, J.J. Interval estimation for Cohen’s kappa as a measure of agreement. Stat. Med. 2000, 19, 723–741. [Google Scholar] [CrossRef]
- Jeffcoate, W.J.; Bus, S.A.; Game, F.L.; Hinchliffe, R.J.; Price, P.E.; Schaper, N.C. Reporting standards of studies and papers on the prevention and management of foot ulcers in diabetes: Required details and markers of good quality. Lancet Diabetes Endocrinol. 2016, 4, 781–788. [Google Scholar] [CrossRef] [PubMed]
- Ababneh, A.; Bakri, F.G.; Khader, Y.; Lazzarini, P.; Ajlouni, K. Prevalence and Associates of Foot Deformities among Patients with Diabetes in Jordan. Curr. Diabetes Rev. 2020, 16, 471–482. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, D.G.; Lavery, L.A.; Harkless, L.B. Validation of a diabetic wound classification system: The contribution of depth, infection, and ischemia to risk of amputation. Diabetes Care 1998, 21, 855–859. [Google Scholar] [CrossRef]
- Wewers, M.E.; Lowe, N.K. A critical review of visual analogue scales in the measurement of clinical phenomena. Res. Nurs. Health 1990, 13, 227–236. [Google Scholar] [CrossRef]
- Erb, S.; Letang, E.; Glass, T.; Natamatungiro, A.; Mnzava, D.; Mapesi, H.; Haschke, M.; Duthaler, U.; Berger, B.; Muri, L.; et al. A Simple Visual Analog Scale is a Valuable Tool to Assess Self-Reported Adherence in HIV-Infected Patients on Antiretroviral Treatment in a Resource-Limited Setting. J. AIDS Clin. Res. 2017, 8, 731. [Google Scholar] [CrossRef]
- Smith, J.D.; Guerra, G.; Burkholder, B.G. The validity and accuracy of wrist-worn activity monitors in lower-limb prosthesis users. Disabil. Rehabil. 2019, 42, 3182–3188. [Google Scholar] [CrossRef] [PubMed]
- Burton, E.; Hill, K.D.; Lautenschlager, N.T.; Thogersen-Ntoumani, C.; Lewin, G.; Boyle, E.; Howie, E. Reliability and validity of two fitness tracker devices in the laboratory and home environment for older community-dwelling people. BMC Geriatr. 2018, 18, 103. [Google Scholar] [CrossRef]
- Kooiman, T.J.; Dontje, M.L.; Sprenger, S.R.; Krijnen, W.P.; van der Schans, C.P.; de Groot, M. Reliability and validity of ten consumer activity trackers. BMC Sport. Sci. Med. Rehabil. 2015, 7, 24. [Google Scholar] [CrossRef]
- Diaz, K.M.; Krupka, D.J.; Chang, M.J.; Peacock, J.; Ma, Y.; Goldsmith, J.; Schwartz, J.E.; Davidson, K.W. Fitbit(R): An accurate and reliable device for wireless physical activity tracking. Int. J. Cardiol. 2015, 185, 138–140. [Google Scholar] [CrossRef]
- Armstrong, D.G.; Lavery, L.A.; Kimbriel, H.R.; Nixon, B.P.; Boulton, A.J. Activity patterns of patients with diabetic foot ulceration: Patients with active ulceration may not adhere to a standard pressure off-loading regimen. Diabetes Care 2003, 26, 2595–2597. [Google Scholar] [CrossRef]
- Portney, L.G.; Watkins, M.P. Foundations of Clinical Research: Applications to Practice; Pearson/Prentice Hall: Upper Saddle River, NJ, USA, 2009. [Google Scholar]
- Bland, J.M.; Altman, D.G. Measuring agreement in method comparison studies. Stat. Methods Med. Res. 1999, 8, 135–160. [Google Scholar] [CrossRef] [PubMed]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Oates, G.R.; Stepanikova, I.; Rowe, S.M.; Gamble, S.; Gutierrez, H.H.; Harris, W.T. Objective versus self-reported adherence to airway clearance therapy in cystic fibrosis. Respir. Care 2019, 64, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Daniels, T.; Goodacre, L.; Sutton, C.; Pollard, K.; Conway, S.; Peckham, D. Accurate assessment of adherence: Self-report and clinician report vs electronic monitoring of nebulizers. Chest 2011, 140, 425–432. [Google Scholar] [CrossRef] [PubMed]
- Vik, S.A.; Maxwell, C.J.; Hogan, D.B. Measurement, correlates, and health outcomes of medication adherence among seniors. Ann. Pharmacother. 2004, 38, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Wagner, G.; Miller, L.G. Is the influence of social desirability on patients’ self-reported adherence overrated? JAIDS J. Acquir. Immune Defic. Syndr. 2004, 35, 203–204. [Google Scholar] [CrossRef]
- Heo, S.; Kim, J.; Shim, J.L.; Barbe, T.; Black, V.; Lee, M.O. Experiences of and factors associated with dietary sodium adherence in heart failure from patients’ and their caregivers’ perspectives: A qualitative study. Geriatr. Nurs. 2021, 42, 1190–1197. [Google Scholar] [CrossRef]
- Coffey, L.; Mahon, C.; Gallagher, P. Perceptions and experiences of diabetic foot ulceration and foot care in people with diabetes: A qualitative meta-synthesis. Int. Wound J. 2019, 16, 183–210. [Google Scholar] [CrossRef]
- Armstrong, D.G.; Abu-Rumman, P.L.; Nixon, B.P.; Boulton, A.J. Continuous activity monitoring in persons at high risk for diabetes-related lower-extremity amputation. J. Am. Podiatr. Med. Assoc. 2001, 91, 451–455. [Google Scholar] [CrossRef]
- Mignault, D.; St-Onge, M.; Karelis, A.D.; Allison, D.B.; Rabasa-Lhoret, R. Evaluation of the Portable HealthWear Armband: A device to measure total daily energy expenditure in free-living type 2 diabetic individuals. Diabetes Care 2005, 28, 225–227. [Google Scholar] [CrossRef]
- Van Remoortel, H.; Raste, Y.; Louvaris, Z.; Giavedoni, S.; Burtin, C.; Langer, D.; Wilson, F.; Rabinovich, R.; Vogiatzis, I.; Hopkinson, N.S. Validity of six activity monitors in chronic obstructive pulmonary disease: A comparison with indirect calorimetry. PLoS ONE 2012, 7, e39198. [Google Scholar] [CrossRef] [PubMed]
- van Schooten, K.S.; Rispens, S.M.; Elders, P.J.; Lips, P.; van Dieën, J.H.; Pijnappels, M. Assessing physical activity in older adults: Required days of trunk accelerometer measurements for reliable estimation. J. Aging Phys. Act. 2015, 23, 9–17. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Total |
|---|---|
| Numbers | 53 |
| Age (years) | 55.3 (9.9) |
| Males | 41 (77.4%) |
| Living with family | 49 (92.5%) |
| Secondary school education | 24 (45.3%) |
| Retired | 17 (32.1%) |
| Family income (JD) ^ | 400 (300–712.5) |
| Type 2 DM | 50 (94.3%) |
| Duration of diabetes (years) | 17.7 (7.0) |
| HbA1c (%, mmol/L) | 8.9 (2.1) |
| BMI | 31 (6.5) |
| Daily steps (wrist activity monitor) ^ | 2758.4 (1729–4676) |
| Neuropathy | 48 (90.6%) |
| PAD | 14 (26.4%) |
| Foot deformities | 38 (71.7%) |
| Minor amputations | 16 (30.2%) |
| Major amputations | 0 (0%) |
| History of previous ulceration | 35 (67.3%) |
| Duration of ulcer (weeks) ^ | 16 (5.0–38) |
| Ulcer size (cm2) ^ | 1.5 (0.5–6.0) |
| Deep ulcer (UTWCS Grade 2 or 3) | 22 (41.5%) |
| Ulcer infection | 27 (50.9%) |
| Duration of RCW (weeks) ^ | 12 (4.0–32.0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ababneh, A.; Finlayson, K.; Edwards, H.; Armstrong, D.G.; Najafi, B.; van Netten, J.J.; Lazzarini, P.A. The Validity and Reliability of Self-Reported Adherence to Using Offloading Treatment in People with Diabetes-Related Foot Ulcers. Sensors 2023, 23, 4423. https://doi.org/10.3390/s23094423
Ababneh A, Finlayson K, Edwards H, Armstrong DG, Najafi B, van Netten JJ, Lazzarini PA. The Validity and Reliability of Self-Reported Adherence to Using Offloading Treatment in People with Diabetes-Related Foot Ulcers. Sensors. 2023; 23(9):4423. https://doi.org/10.3390/s23094423
Chicago/Turabian StyleAbabneh, Anas, Kathleen Finlayson, Helen Edwards, David G. Armstrong, Bijan Najafi, Jaap J. van Netten, and Peter A. Lazzarini. 2023. "The Validity and Reliability of Self-Reported Adherence to Using Offloading Treatment in People with Diabetes-Related Foot Ulcers" Sensors 23, no. 9: 4423. https://doi.org/10.3390/s23094423
APA StyleAbabneh, A., Finlayson, K., Edwards, H., Armstrong, D. G., Najafi, B., van Netten, J. J., & Lazzarini, P. A. (2023). The Validity and Reliability of Self-Reported Adherence to Using Offloading Treatment in People with Diabetes-Related Foot Ulcers. Sensors, 23(9), 4423. https://doi.org/10.3390/s23094423