
Achieving Targeted Delivery of Chemotherapeutic Particles to Small Airway Tumors via Pulmonary Route Using Endotracheal Catheters: A CFPD Study



Abstract
:1. Introduction
2. Results and Discussion
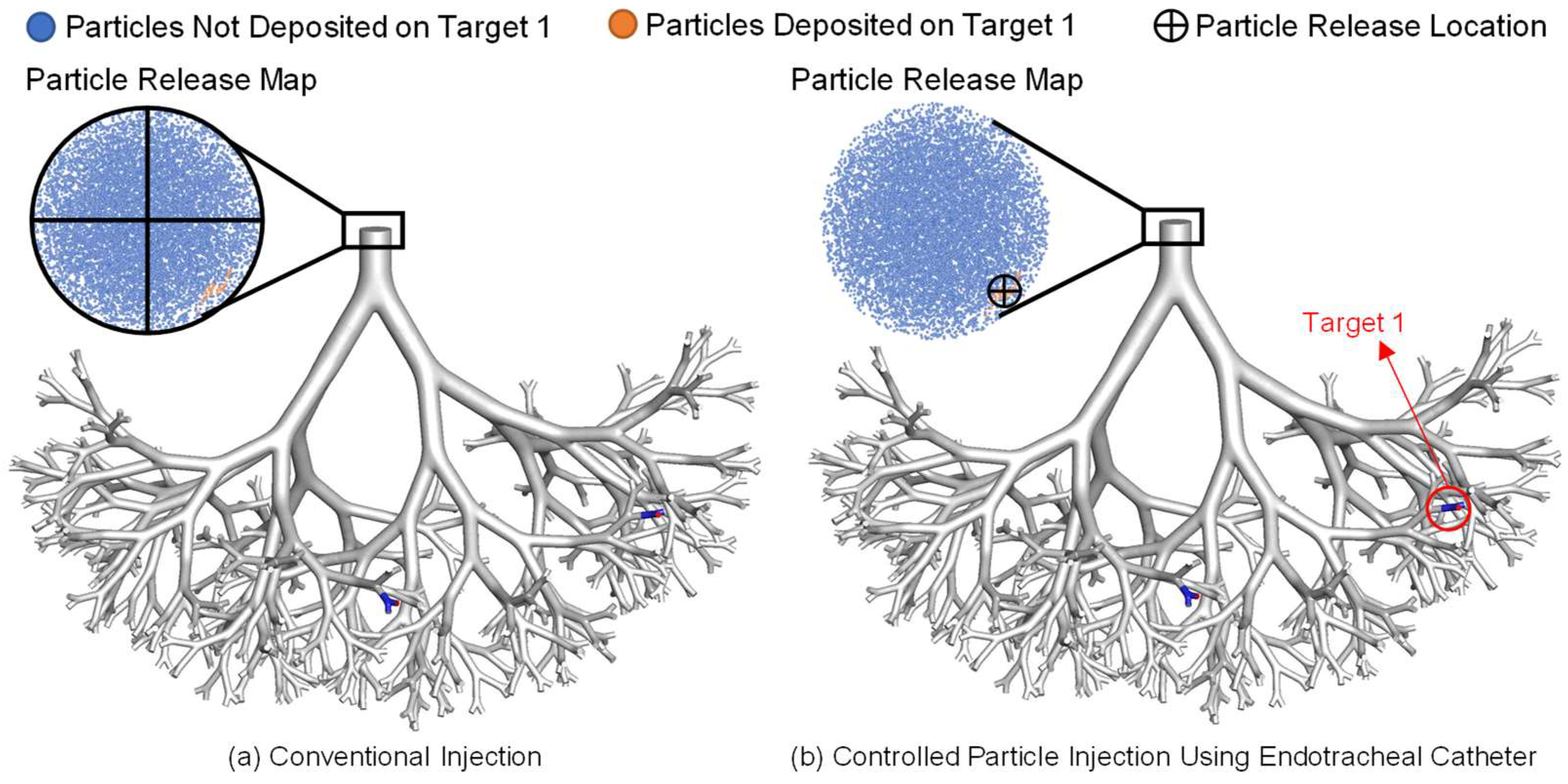
2.1. Conventional Injection vs. Controlled Particle Injection Using Endotracheal Catheters
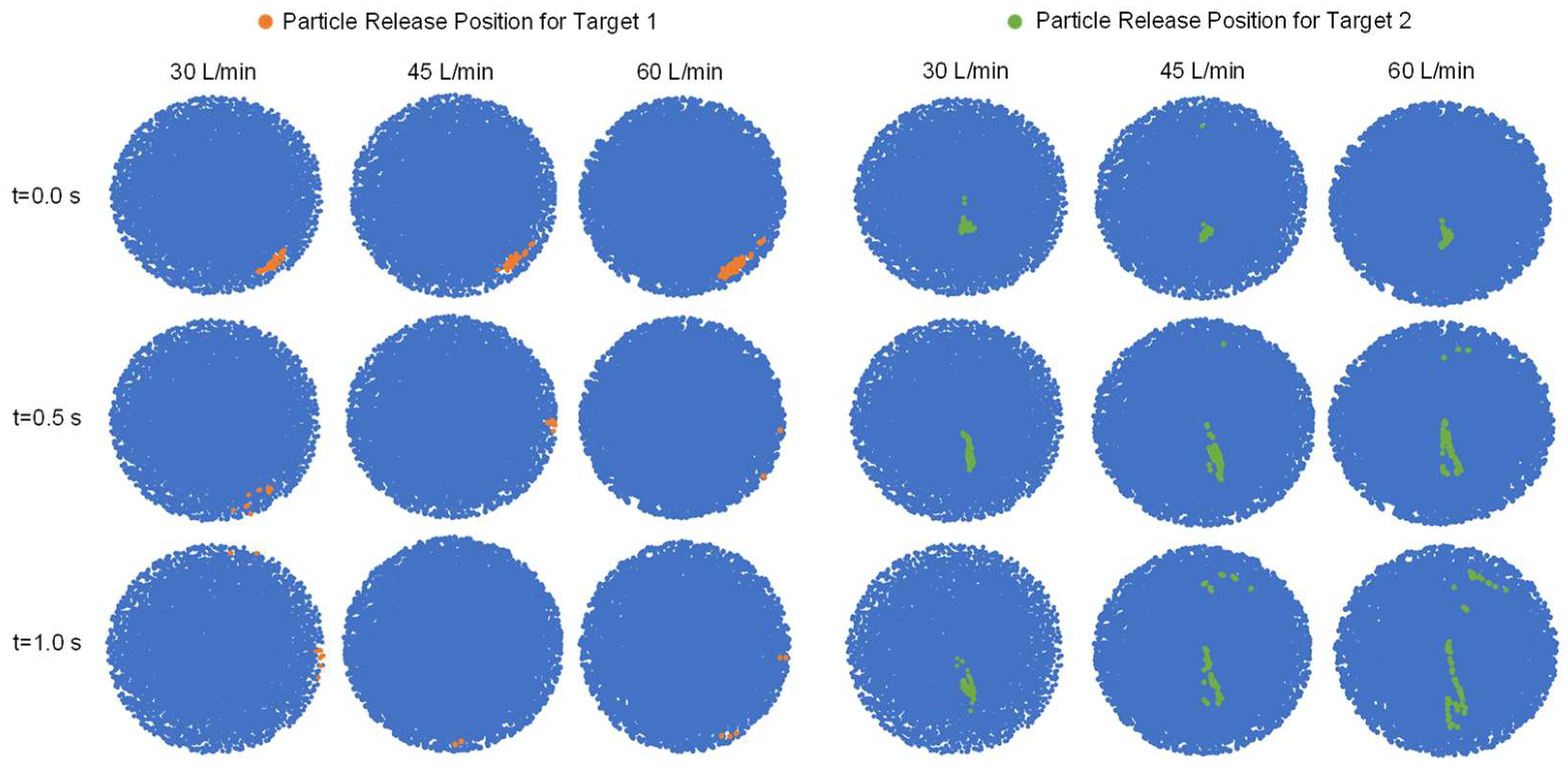
2.2. Particle Release Maps vs. Average Inhalation Flow Rate and Particle Release Time
2.3. Targeted Particle DE vs. Average Inhalation Flow Rate and Particle Release Time
2.4. Targeted Particle DE vs. Catheter Diameter
2.5. Particle Transport Dynamics with Controlled Injection Using Endotracheal Catheters
3. Materials and Methods
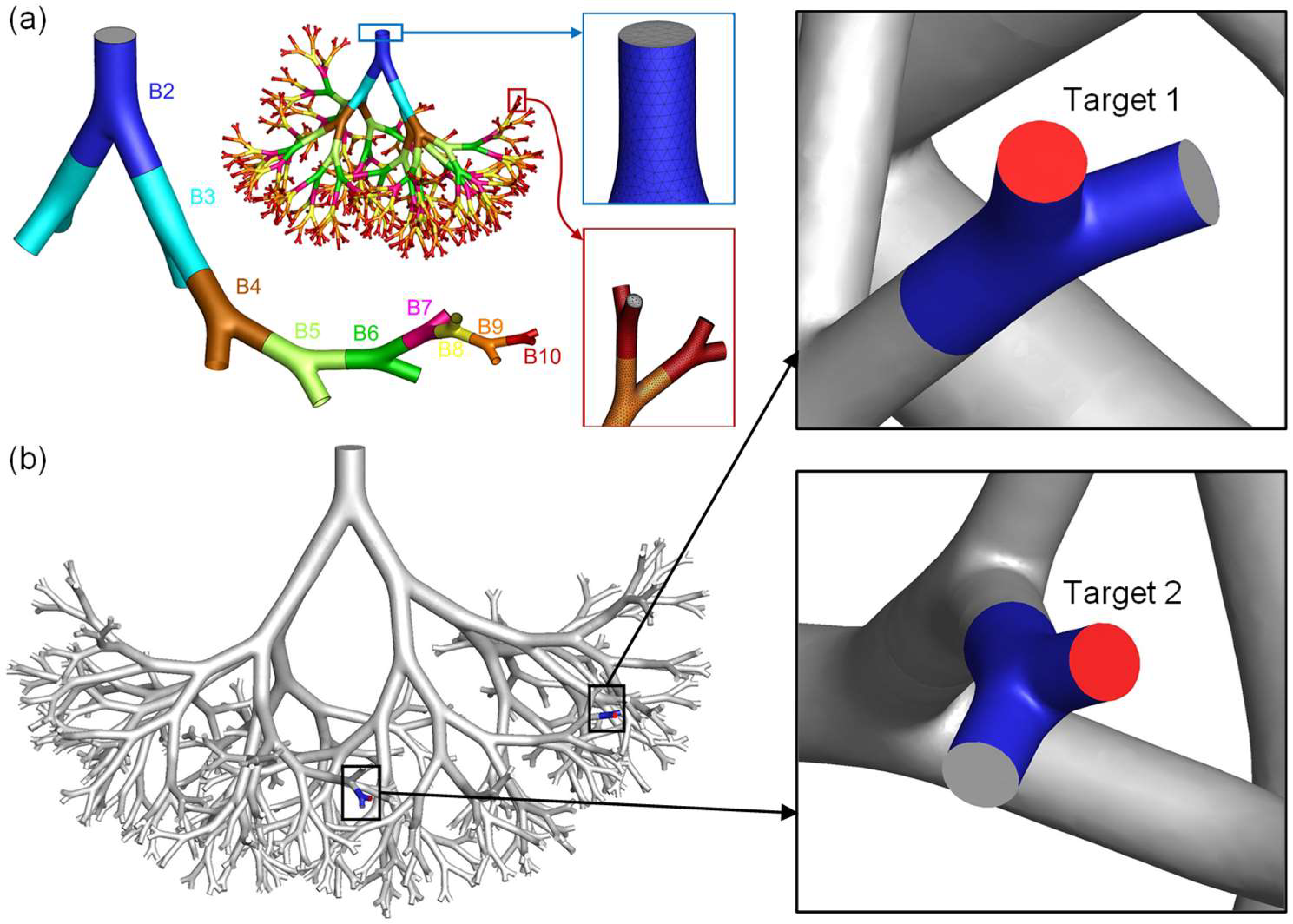
3.1. Geometry and Mesh
3.2. Governing Equations
3.3. Initial and Boundary Conditions
3.4. Particle Targeted Delivery Efficiency (DE)
3.5. Numerical Setup
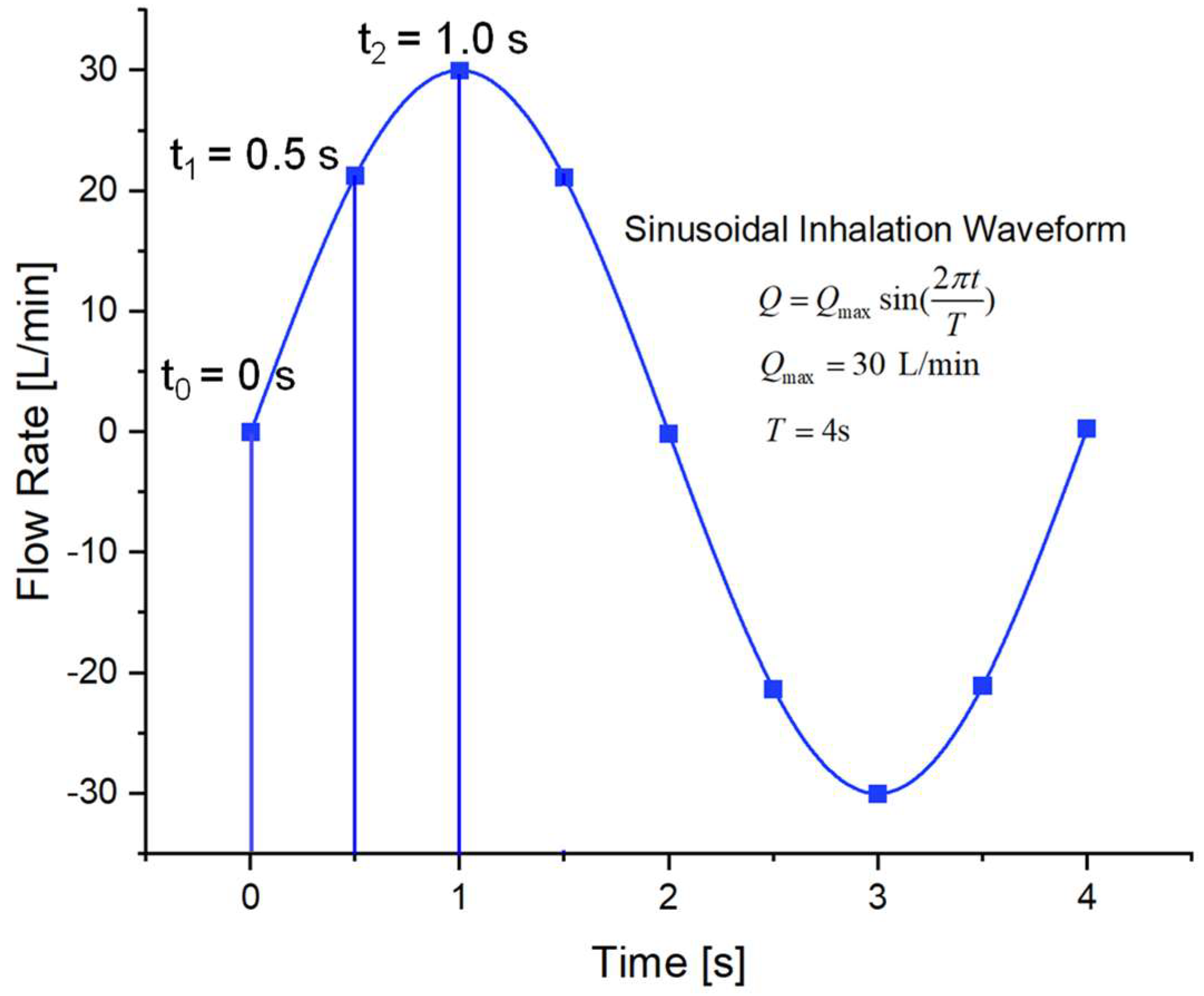
- Defining the transient sinusoidal inhalation waveforms (see Figure 9);
- Defining the DPM time-step;
- Defining the DPM drag coefficient; and
- Output of post-processing particle deposition data in the lung airway.
3.6. Model Validations
- The Transition Shear-Stress Transport (SST) model employed in this study to predict laminar-to-turbulence flow regime has been validated in a previous study [43]. Specifically, comparisons of airflow velocity magnitude and iso-surfaces show good matches between the employed SST k-ω transition model, and the experimental measurements [44] were performed in the same subject-specific human airway model.
- The CFPD model used in the current study was also employed to predict the discrete-phase transport and deposition, as can be seen in Figure S2 in the supplemental material of a previously published work [45]. The predicted regional deposition efficiencies (RDEs) were then compared to benchmark the experimental data obtained from physical models of lung airways, with inhalation flow rates ranging from 15 to 60 L/min. The comparisons revealed a high level of agreement between the results obtained from the numerical and experimental studies.
4. Conclusions
- The conventional injection method can only deliver less than 1% of the chemotherapeutic particles to the designated tumor sites, which indicates a strong side effect will be caused due to the high percentage of particle depositions on healthy tissues from G2 to G10. In contrast, a controlled particle injection method was proposed using a 0.1 mm endotracheal catheter, which can improve the particle DEs on Target 1 and Target 2 to 74% and 100%, respectively.
- Both average inhalation flow rate and particle release time had an influence on the topology of particle release maps. With the increase in local airflow velocities surrounding the particle release (i.e., increase in average inhalation flow rate or increase the particle release time during the sinusoidal inhalation phase before reaching the peak flow rate), the available regions for particle release for achieved targeted delivery to both tumors became more scattered, due to the enhanced turbulence dispersion effect.
- Both average inhalation flow rates and particle release time had an impact on the particle DEs on both tumors. However, the influences were different between Target 1 and Target 2, which were highly dependent on tumor locations. Therefore, the targeted delivery strategy is dependent on tumor locations.
- With the decrease in catheter diameter, the targeted particle DEs on both tumors increased.
- For seeking the optimal average inhalation flow rate and particle release time for the controlled particle injection method using endotracheal catheters, two criteria were used, that is, (1) highest particle DEs, and (2) largest areas of available regions for particle release position to aim for the tumor. For Target 1, 60 L/min and a 0.0 s particle release time were employed. For Target 2, 30 L/min and a 0.0 s particle release time were selected.
5. Limitations of this Study and Future Work
- The small lung airway model used in the study is stationary and does not take into account any lung movement;
- The study did not consider the effects of cilia-driven mucus motion on medication clearance; and
- The dynamics of medication perfusion into tumor cells following deposition were not modeled in the study.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| 5-FU | 5-Fluorouracil |
| B | Bifurcation |
| CFD | Computational Fluid Dynamics |
| CFPD | Computational Fluid Particle Dynamics |
| COVID-19 | Coronavirus Disease 2019 |
| CRA | Cryoablation |
| CPRT | Controlled Particle Release and Targeting |
| DF | Deposition Fraction |
| DE | Delivery Efficiency |
| DPI | Dry Powder Inhaler |
| DPM | Discrete Phase Model |
| FSI | Fluid-Structure Interaction |
| G | Generation |
| IL-2 | Interleukin-2 |
| MWA | Microwave Ablation |
| PDT | Photodynamic Therapy |
| PVC | Polyvinyl Chloride |
| RDE | Regional Deposition Efficiency |
| RFA | Route Radiofrequency Ablation |
| SST | Shear Stress Transport |
| TB | Tracheobronchial |
| VOF | Volume of Fluid |
References
- Siegel, R.; Ma, J.; Zou, Z.; Jemal, A. Cancer statistics, 2014. CA: A Cancer J. Clin. 2014, 64, 9–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, C.M.; Goo, J.M.; Lee, H.J.; Kim, M.A.; Lee, C.H.; Kang, M.-J. Tumors in the tracheobronchial tree: CT and FDG PET features. Radiographics 2009, 29, 55–71. [Google Scholar] [CrossRef] [PubMed]
- Macchiarini, P. Primary tracheal tumours. Lancet Oncol. 2006, 7, 83–91. [Google Scholar] [CrossRef]
- Konoglou, M.; Cheva, A.; Zarogoulidis, P.; Porpodis, K.; Pataka, A.; Mpaliaka, A.; Papaiwannou, A.; Zarogoulidis, K.; Kontakiotis, T.; Karaiskos, T. Epithelial-myoepithelial carcinoma of the trachea—A rare entity case report. J. Thorac. Dis. 2014, 6, S194. [Google Scholar] [PubMed]
- Patil, P.S.; Mahajan, H.S. Lung Cancer: How Well We Have Fared? Indo Glob. J. Pharm. Sci. 2022, 12, 82–91. [Google Scholar] [CrossRef]
- Spiro, S.; Rudd, R.; Souhami, R.; Brown, J.; Fairlamb, D.; Gower, N.; Maslove, L.; Milroy, R.; Napp, V.; Parmar, M. Chemotherapy versus supportive care in advanced non-small cell lung cancer: Improved survival without detriment to quality of life. Thorax 2004, 59, 828–836. [Google Scholar] [CrossRef] [Green Version]
- Bunn, P.A., Jr.; Kelly, K. New chemotherapeutic agents prolong survival and improve quality of life in non-small cell lung cancer: A review of the literature and future directions. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 1998, 4, 1087–1100. [Google Scholar]
- Tatsumura, T.; Koyama, S.; Tsujimoto, M.; Kitagawa, M.; Kagamimori, S. Further study of nebulisation chemotherapy, a new chemotherapeutic method in the treatment of lung carcinomas: Fundamental and clinical. Br. J. Cancer 1993, 68, 1146–1149. [Google Scholar] [CrossRef]
- Tatsumura, T.; Yamamoto, K.; Murakami, A.; Tsuda, M.; Sugiyama, S. New chemotherapeutic method for the treatment of tracheal and bronchial cancers--nebulization chemotherapy. Gan No Rinsho. Jpn. J. Cancer Clin. 1983, 29, 765–770. [Google Scholar]
- Huland, E.; Heinzer, H.; Huland, H. Inhaled interleukin-2 in combination with low-dose systemic interleukin-2 and interferon α in patients with pulmonary metastatic renal-cell carcinoma: Effectiveness and toxicity of mainly local treatment. J. Cancer Res. Clin. Oncol. 1994, 120, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Otterson, G.A.; Villalona-Calero, M.A.; Sharma, S.; Kris, M.G.; Imondi, A.; Gerber, M.; White, D.A.; Ratain, M.J.; Schiller, J.H.; Sandler, A. Phase I study of inhaled Doxorubicin for patients with metastatic tumors to the lungs. Clin. Cancer Res. 2007, 13, 1246–1252. [Google Scholar] [CrossRef] [Green Version]
- Taratula, O.; Garbuzenko, O.B.; Chen, A.M.; Minko, T. Innovative strategy for treatment of lung cancer: Targeted nanotechnology-based inhalation co-delivery of anticancer drugs and siRNA. J. Drug Target. 2011, 19, 900–914. [Google Scholar] [CrossRef] [PubMed]
- Roa, W.H.; Azarmi, S.; Al-Hallak, M.H.D.K.; Finlay, W.H.; Magliocco, A.M.; Löbenberg, R. Inhalable nanoparticles, a non-invasive approach to treat lung cancer in a mouse model. J. Control. Release 2011, 150, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; Chen, X.; Yang, M. An in Silico Investigation of a Lobe-Specific Targeted Pulmonary Drug Delivery Method. In Proceedings of the Frontiers in Biomedical Devices, Washingtong, DC, USA, 15 March 2018; p. V001T008A011. [Google Scholar]
- Laube, B.L.; Janssens, H.M.; de Jongh, F.H.C.; Devadason, S.G.; Dhand, R.; Diot, P.; Everard, M.L.; Horvath, I.; Navalesi, P.; Voshaar, T.; et al. What the pulmonary specialist should know about the new inhalation therapies. Eur. Respir. J. 2011, 37, 1308–1417. [Google Scholar] [CrossRef] [Green Version]
- Tena, A.F.; Clarà, P.C. Deposition of inhaled particles in the lungs. Arch. De Bronconeumol. 2012, 48, 240–246. [Google Scholar] [CrossRef]
- Geller, D.E.; Weers, J.; Heuerding, S. Development of an inhaled dry-powder formulation of tobramycin using PulmoSphere™ technology. J. Aerosol Med. Pulm. Drug Deliv. 2011, 24, 175–182. [Google Scholar] [CrossRef]
- Yang, M.Y.; Chan, J.G.Y.; Chan, H.-K. Pulmonary drug delivery by powder aerosols. J. Control. Release 2014, 193, 228–240. [Google Scholar] [CrossRef]
- Gürzing, S.; Thiebes, A.L.; Cornelissen, C.G.; Jockenhoevel, S.; Reddemann, M.A. Suitability of Bronchoscopic Spraying for Fluid Deposition in Lower Airway Regions: Fluorescence Analysis on a Transparent In Vitro Airway Model. J. Aerosol Med. Pulm. Drug Deliv. 2022, 35, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Lai, Y.; Wang, X.; Zhou, K.; Su, J.; Che, G. The feasibility and safety of no placement of urinary catheter following lung cancer surgery: A retrospective cohort study with 2,495 cases. J. Investig. Surg. 2021, 34, 568–574. [Google Scholar] [CrossRef]
- Kang, J.R.; Long, L.H.; Yan, S.W.; Wei, W.W.; Jun, H.Z.; Chen, W. Peripherally Inserted Central Catheter-Related Vein Thrombosis in Patients with Lung Cancer. Clin. Appl. Thromb. Hemost. 2017, 23, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.-R.; Lau, R.W.; Ng, C.S. Catheter-based alternative treatment for early-stage lung cancer with a high-risk for morbidity. J. Thorac. Dis. 2018, 10, S1864. [Google Scholar] [CrossRef] [PubMed]
- Kleinstreuer, C.; Zhang, Z. Airflow and particle transport in the human respiratory system. Annu. Rev. Fluid Mech. 2010, 42, 301–334. [Google Scholar] [CrossRef]
- Kleinstreuer, C.; Zhang, Z. Targeted drug aeroso deposition analysis for a four-generation lung airway model with hemispherical tumors. J. Biomech. Eng. 2003, 125, 197–206. [Google Scholar] [CrossRef]
- Plank, C. Nanomagnetosols: Magnetism opens up new perspectives for targeted aerosol delivery to the lung. Trends Biotechnol. 2008, 26, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Kenjereš, S.; Tjin, J.L. Numerical simulations of targeted delivery of magnetic drug aerosols in the human upper and central respiratory system: A validation study. R. Soc. Open Sci. 2017, 4, 170873. [Google Scholar] [CrossRef] [Green Version]
- Ghosh, A.; Islam, M.S.; Saha, S.C. Targeted drug delivery of magnetic nano-particle in the specific lung region. Computation 2020, 8, 10. [Google Scholar] [CrossRef] [Green Version]
- Ostrovski, Y.; Hofemeier, P.; Sznitman, J. Augmenting regional and targeted delivery in the pulmonary acinus using magnetic particles. Int. J. Nanomed. 2016, 11, 3385. [Google Scholar]
- Ostrovski, Y.; Dorfman, S.; Mezhericher, M.; Kassinos, S.; Sznitman, J. Targeted drug delivery to upper airways using a pulsed aerosol bolus and inhaled volume tracking method. Flow Turbul. Combust. 2019, 102, 73–87. [Google Scholar] [CrossRef] [PubMed]
- Martonen, T.B.; Guan, X. Effects of tumors on inhaled pharmacologic drugs. Cell Biochem. Biophys. 2001, 35, 233–243. [Google Scholar] [CrossRef] [PubMed]
- Srivastav, V.; Kumar, A.; Shukla, S.; Paul, A.; Bhatt, A.; Jain, A. Airflow and aerosol-drug delivery in a CT scan based human respiratory tract with tumor using CFD. J. Appl. Fluid Mech. 2014, 7, 345–356. [Google Scholar]
- Feng, Y.; Zhao, J.; Kleinstreuer, C.; Wang, Q.; Wang, J.; Wu, D.H.; Lin, J. An in silico Inter-subject Variability Study of Extra-thoracic Morphology Effects on Inhaled Particle Transport and Deposition. J. Aerosol Sci. 2018, 123, 185–207. [Google Scholar] [CrossRef]
- Thakur, A.K.; Kaundle, B.; Singh, I. Mucoadhesive Drug Delivery Systems in Respiratory Diseases. In Targeting Chronic Inflammatory Lung Diseases Using Advanced Drug Delivery Systems; Elsevier: Amsterdam, The Netherlands, 2020; pp. 475–491. [Google Scholar]
- Smith, H. Human Respiratory Tract Model for Radiological Protection. Ann. ICRP 1994, 24, 1–3. [Google Scholar]
- Feng, Y.; Zhao, J.; Hayati, H.; Sperry, T.; Yi, H. Tutorial: Understanding the transport, deposition, and translocation of particles in human respiratory systems using Computational Fluid-Particle Dynamics and Physiologically Based Toxicokinetic models. J. Aerosol Sci. 2021, 151, 105672. [Google Scholar]
- Chen, X.; Feng, Y.; Zhong, W.; Sun, B.; Tao, F. Numerical investigation of particle deposition in a triple bifurcation airway due to gravitational sedimentation and inertial impaction. Powder Technol. 2018, 323, 284–293. [Google Scholar] [CrossRef]
- Morsi, S.; Alexander, A. An investigation of particle trajectories in two-phase flow systems. J. Fluid Mech. 1972, 55, 193–208. [Google Scholar] [CrossRef]
- Allen, M.D.; Raabe, O.G. Slip correction measurements of spherical solid aerosol particles in an improved Millikan apparatus. Aerosol Sci. Technol. 1985, 4, 269–286. [Google Scholar] [CrossRef]
- Barnas, G.M.; Harinath, P.; Green, M.D.; Suki, B.; Kaczka, D.W.; Lutchen, K.R. Influence of waveform and analysis technique on lung and chest wall properties. Respir. Physiol. 1994, 96, 331–344. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Feng, Y.; Zhong, W.; Kleinstreuer, C. Numerical investigation of the interaction, transport and deposition of multicomponent droplets in a simple mouth-throat model. J. Aerosol Sci. 2017, 105, 108–127. [Google Scholar] [CrossRef]
- Haghnegahdar, A.; Zhao, J.; Feng, Y. Lung aerosol dynamics of airborne influenza A virus-laden droplets and the resultant immune system responses: An in silico study. J. Aerosol Sci. 2019, 134, 21. [Google Scholar] [CrossRef]
- Zhao, J.; Feng, Y.; Bezerra, M.; Wang, J.; Sperry, T. Numerical simulation of welding fume lung dosimetry. J. Aerosol Sci. 2019, 135, 16. [Google Scholar] [CrossRef]
- Feng, Y.; Kleinstreuer, C.; Castro, N.; Rostami, A. Computational transport, phase change and deposition analysis of inhaled multicomponent droplet--vapor mixtures in an idealized human upper lung model. J. Aerosol Sci. 2016, 96, 96–123. [Google Scholar] [CrossRef] [Green Version]
- Banko, A.; Coletti, F.; Schiavazzi, D.; Elkins, C.; Eaton, J. Three-dimensional inspiratory flow in the upper and central human airways. Exp. Fluids 2015, 56, 117. [Google Scholar] [CrossRef]
- Haghnegahdar, A.; Feng, Y.; Chen, X.; Lin, J. Computational analysis of deposition and translocation of inhaled nicotine and acrolein in the human body with e-cigarette puffing topographies. Aerosol Sci. Technol. 2018, 52, 483–493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, J.; Feng, Y.; Koshiyama, K.; Wu, H. Prediction of airway deformation effect on pulmonary air-particle dynamics: A numerical study. Phys. Fluids 2021, 33, 101906. [Google Scholar] [CrossRef]
- Zhao, J.L.L.; Fromen, C.; Feng, Y. Predicting Transport and Deposition of Inhaled Microparticles in an Elastic Lung Model. In Proceedings of the BMES/FDA Frontiers in Medical Devices Conferences, College Park, MD, USA, 13 May 2019. [Google Scholar]
- Yi, H.; Wang, Q.; Feng, Y. Computational analysis of obstructive disease and cough intensity effects on the mucus transport and clearance in an idealized upper airway model using the volume of fluid method. Phys. Fluids 2021, 33, 021903. [Google Scholar] [CrossRef]
- Zhao, J.F.Y.; Hjaghnegahdar, A.; Sarkar, S.; Bharadwaj, R. Numerical Investigation of Particle Shape and Actuation Flow Rate Effects on Lactose Carrier Delivery Efficiency through a Dry Powder Inhaler (DPI) Using CFD-DEM. In Proceedings of the 2020 Virtual AIChE Annual Meeting, Online, 13–20 November 2020. [Google Scholar]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mesh No. | Nodes | Faces | Cells | Near-Wall Prism Layers |
|---|---|---|---|---|
| 1 | 2,817,233 | 15,052,480 | 6,059,303 | 5 |
| 2 (Final) | 4,428,041 | 25,530,968 | 10,641,093 | 5 |
| 3 | 4,962,751 | 29,349,686 | 12,357,045 | 5 |
| 4 | 5,493,502 | 33,328,366 | 14,168,216 | 5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Islam, M.R.; Feng, Y. Achieving Targeted Delivery of Chemotherapeutic Particles to Small Airway Tumors via Pulmonary Route Using Endotracheal Catheters: A CFPD Study. Pharmaceuticals 2023, 16, 158. https://doi.org/10.3390/ph16020158
Islam MR, Feng Y. Achieving Targeted Delivery of Chemotherapeutic Particles to Small Airway Tumors via Pulmonary Route Using Endotracheal Catheters: A CFPD Study. Pharmaceuticals. 2023; 16(2):158. https://doi.org/10.3390/ph16020158
Chicago/Turabian StyleIslam, Mohammad Rashedul, and Yu Feng. 2023. "Achieving Targeted Delivery of Chemotherapeutic Particles to Small Airway Tumors via Pulmonary Route Using Endotracheal Catheters: A CFPD Study" Pharmaceuticals 16, no. 2: 158. https://doi.org/10.3390/ph16020158
APA StyleIslam, M. R., & Feng, Y. (2023). Achieving Targeted Delivery of Chemotherapeutic Particles to Small Airway Tumors via Pulmonary Route Using Endotracheal Catheters: A CFPD Study. Pharmaceuticals, 16(2), 158. https://doi.org/10.3390/ph16020158