
Correlations of PTEN and ERG Immunoexpression in Prostate Carcinoma and Lesions Related to Its Natural History: Clinical Perspectives
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Material Collection and Characterization
2.2. Immunohistochemistry Procedure and Evaluation
2.3. Statistical Analysis
3. Results
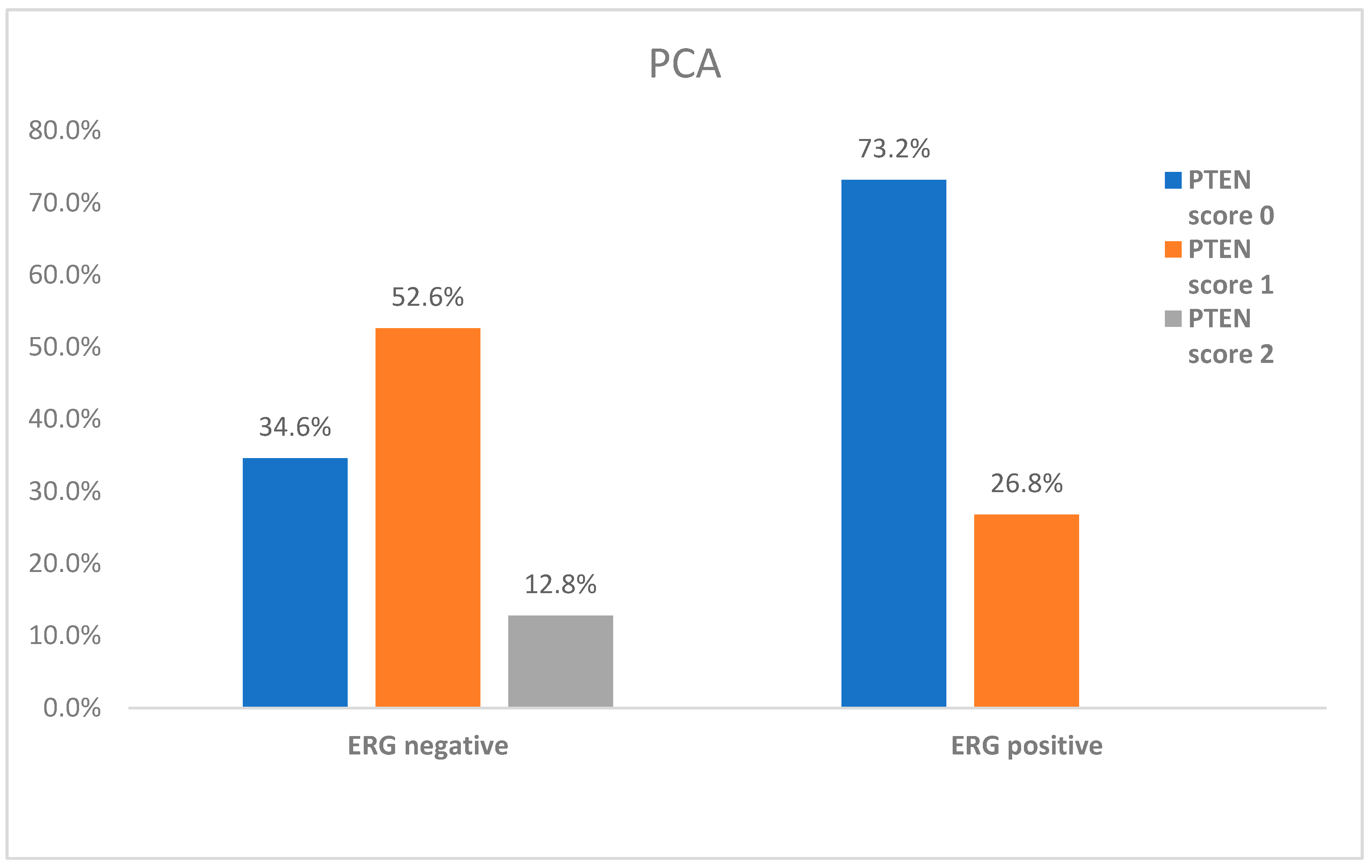
3.1. ERG and PTEN Associations in Prostate Carcinoma
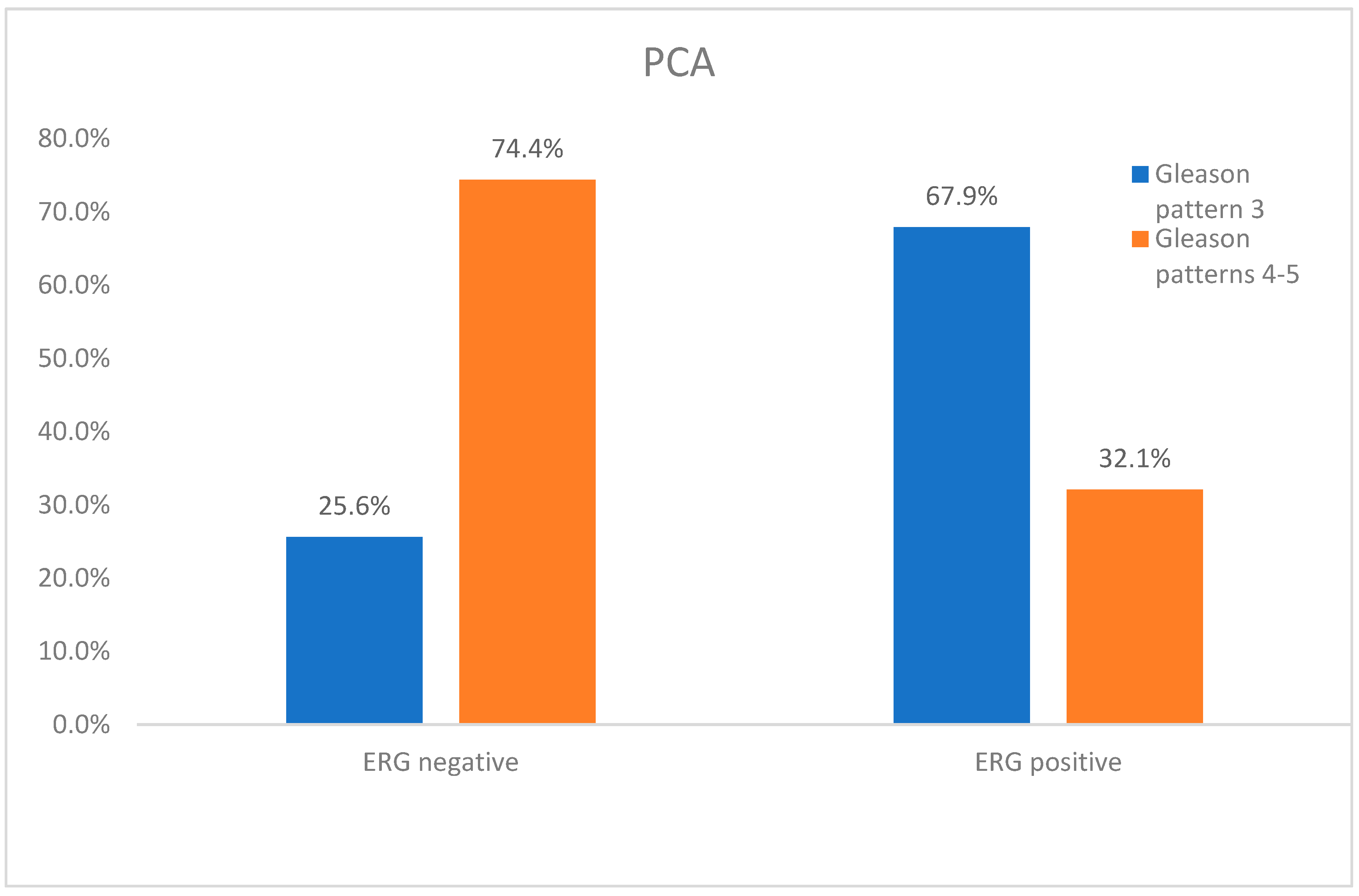
3.2. Association of ERG Expression with Gleason Grade Pattern in Prostate Cancer
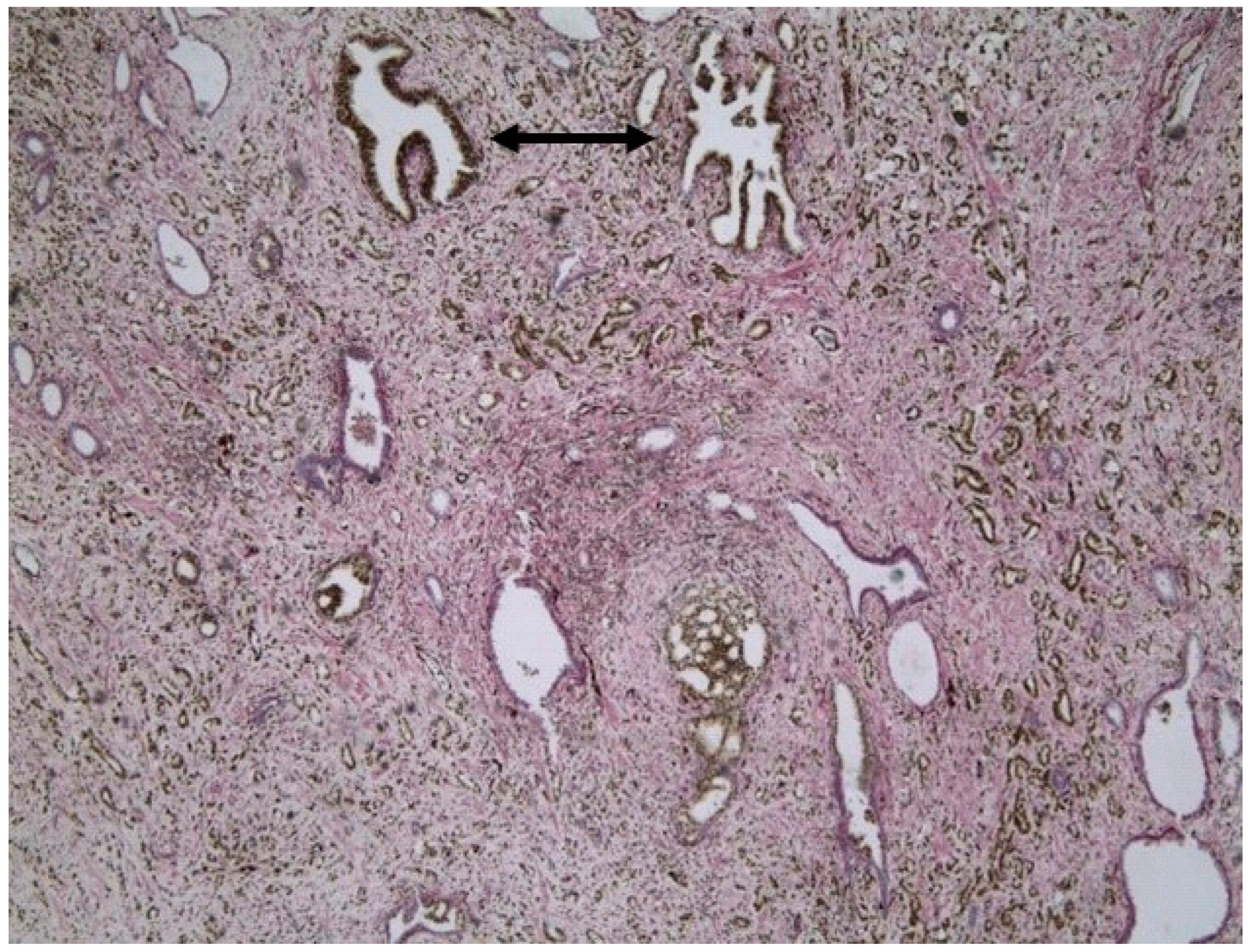
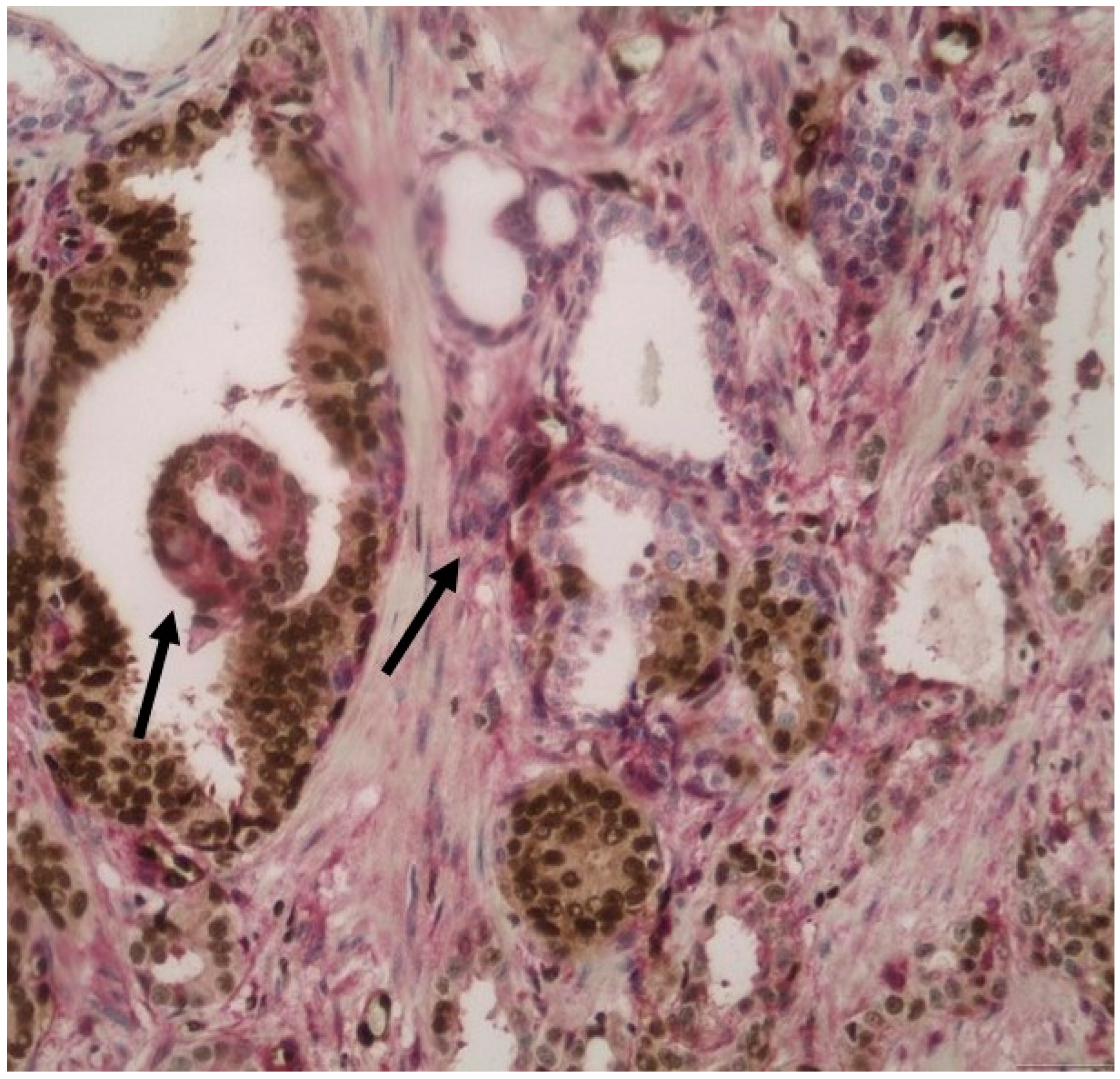
3.3. PTEN Expression in HGPIN and Its Association with the Adjacent Invasive Prostate Cancer
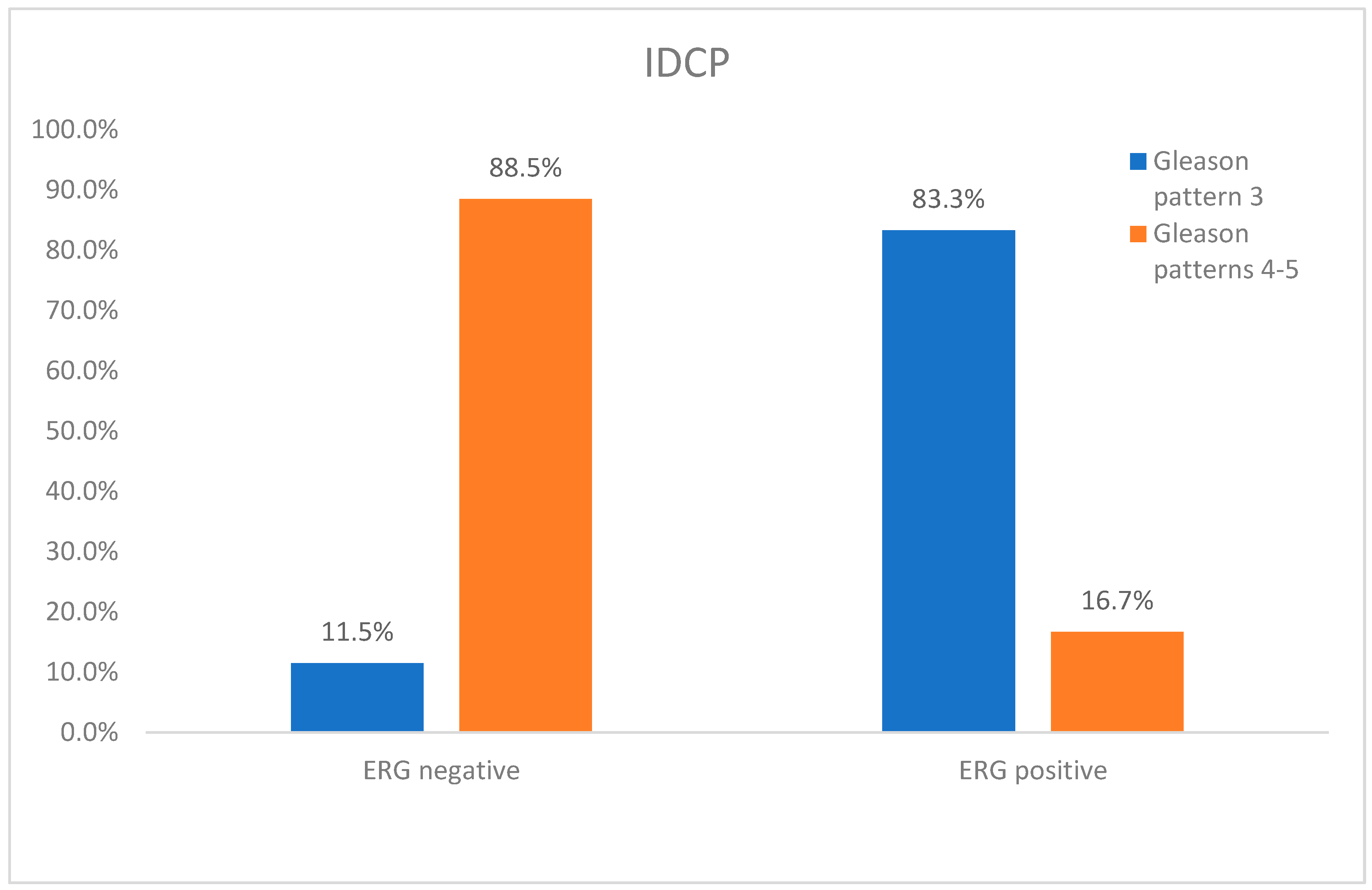
3.4. ERG Expression in IDCP and Its Association with the Adjacent Invasive Prostate Carcinoma
3.5. AMACR Expression in Prostate Cancer and Its Association with PTEN
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Center, M.M.; Jemal, A.; Lortet-Tieulent, J.; Ward, E.; Ferlay, J.; Brawley, O.; Bray, F. International Variation in Prostate Cancer Incidence and Mortality Rates. Eur. Urol. 2012, 61, 1079–1092. [Google Scholar] [CrossRef]
- Destouni, M.; Lazaris, A.C.; Tzelepi, V. Cribriform Patterned Lesions in the Prostate Gland with Emphasis on Differential Diagnosis and Clinical Significance. Cancers 2022, 14, 3041. [Google Scholar] [CrossRef] [PubMed]
- van Leenders, G.J.; van der Kwast, T.H.; Grignon, D.J.; Evans, A.J.; Kristiansen, G.; Kweldam, C.F.; Litjens, G.; McKenney, J.K.; Melamed, J.; Mottet, N.; et al. The 2019 International Society of Urological Pathology (ISUP) Consensus Conference on Grading of Prostatic Carcinoma. Am. J. Surg. Pathol. 2020, 44, e87–e99. [Google Scholar] [CrossRef] [PubMed]
- Boström, P.J.; Bjartell, A.S.; Catto, J.W.; Eggener, S.E.; Lilja, H.; Loeb, S.; Schalken, J.; Schlomm, T.; Cooperberg, M.R. Genomic Predictors of Outcome in Prostate Cancer. Eur. Urol. 2015, 68, 1033–1044. [Google Scholar] [CrossRef]
- Zhao, L.; Yu, N.; Guo, T.; Hou, Y.; Zeng, Z.; Yang, X.; Hu, P.; Tang, X.; Wang, J.; Liu, M. Tissue Biomarkers for Prognosis of Prostate Cancer: A Systematic Review and Meta-analysis. Cancer Epidemiol. Biomark. Prev. 2014, 23, 1047–1054. [Google Scholar] [CrossRef]
- Mithal, P.; Allott, E.; Gerber, L.; Reid, J.; Welbourn, W.; Tikishvili, E.; Park, J.; Younus, A.; Sangale, Z.; Lanchbury, J.S.; et al. PTEN loss in biopsy tissue predicts poor clinical outcomes in prostate cancer. Int. J. Urol. 2014, 21, 1209–1214. [Google Scholar] [CrossRef]
- Fontugne, J.; Lee, D.; Cantaloni, C.; Barbieri, C.; Caffo, O.; Hanspeter, E.; Mazzoleni, G.; Palma, P.D.; Rubin, M.; Fellin, G.; et al. MP24-13 Withdrawn: Recurrent Prostate Cancer Genomic Alterations Predict Response to Brachytherapy Treatment. J. Urol. 2014, 191, e264. [Google Scholar] [CrossRef]
- Krohn, A.; Diedler, T.; Burkhardt, L.; Mayer, P.-S.; De Silva, C.; Meyer-Kornblum, M.; Kötschau, D.; Tennstedt, P.; Huang, J.; Gerhäuser, C.; et al. Genomic Deletion of PTEN Is Associated with Tumor Progression and Early PSA Recurrence in ERG Fusion-Positive and Fusion-Negative Prostate Cancer. Am. J. Pathol. 2012, 181, 401–412. [Google Scholar] [CrossRef]
- Shah, R.B.; Bentley, J.; Jeffery, Z.; DeMarzo, A.M. Heterogeneity of PTEN and ERG expression in prostate cancer on core needle biopsies: Implications for cancer risk stratification and biomarker sampling. Hum. Pathol. 2015, 46, 698–706. [Google Scholar] [CrossRef] [PubMed]
- Krohn, A.; Freudenthaler, F.; Harasimowicz, S.; Kluth, M.; Fuchs, S.; Burkhardt, L.; Stahl, P.; Tsourlakis, M.C.; Bauer, M.; Tennstedt, P.; et al. Heterogeneity and chronology of PTEN deletion and ERG fusion in prostate cancer. Mod. Pathol. 2014, 27, 1612–1620. [Google Scholar] [CrossRef]
- Tomlins, S.A.; Rhodes, D.R.; Perner, S. Recurrent fusion of TMPRSS2 and ETS transcription factor genes in prostate cancer. Science 2005, 310, 644–648. [Google Scholar] [CrossRef] [PubMed]
- Chaux, A.; Peskoe, S.B.; Gonzalez-Roibon, N.; Schultz, L.; Albadine, R.; Hicks, J.; De Marzo, A.M.; A Platz, E.; Netto, G.J. Loss of PTEN expression is associated with increased risk of recurrence after prostatectomy for clinically localized prostate cancer. Mod. Pathol. 2012, 25, 1543–1549. [Google Scholar] [CrossRef] [PubMed]
- Lotan, T.L.; Gurel, B.; Sutcliffe, S.; Esopi, D.; Liu, W.; Xu, J.; Hicks, J.L.; Park, B.H.; Humphreys, E.; Partin, A.W.; et al. PTEN Protein Loss by Immunostaining: Analytic Validation and Prognostic Indicator for a High Risk Surgical Cohort of Prostate Cancer Patients. Clin. Cancer Res. 2011, 17, 6563–6573. [Google Scholar] [CrossRef] [PubMed]
- Pettersson, A.; Graff, R.E.; Bauer, S.R. The TMPRSS2:ERG rearrangement, ERG expression, and prostate cancer outcomes: A cohort study and meta-analysis. Cancer Epidemiol. Biomark. Prev. 2012, 21, 1497–1509. [Google Scholar] [CrossRef]
- Minner, S.; Enodien, M.; Sirma, H.; Luebke, A.M.; Krohn, A.; Mayer, P.S.; Simon, R.; Tennstedt, P.; Müller, J.; Scholz, L.; et al. ERG Status Is Unrelated to PSA Recurrence in Radically Operated Prostate Cancer in the Absence of Antihormonal Therapy. Clin. Cancer Res. 2011, 17, 5878–5888. [Google Scholar] [CrossRef]
- Yoshimoto, M.; Joshua, A.M.; Cunha, I.W.; A Coudry, R.; Fonseca, F.P.; Ludkovski, O.; Zielenska, M.; A Soares, F.; A Squire, J. Absence of TMPRSS2:ERG fusions and PTEN losses in prostate cancer is associated with a favorable outcome. Mod. Pathol. 2008, 21, 1451–1460. [Google Scholar] [CrossRef]
- Leinonen, K.A.; Saramäki, O.R.; Furusato, B.; Kimura, T.; Takahashi, H.; Egawa, S.; Suzuki, H.; Keiger, K.; Hahm, S.H.; Isaacs, W.B.; et al. Loss of PTEN Is Associated with Aggressive Behavior in ERG-Positive Prostate Cancer. Cancer Epidemiol. Biomark. Prev. 2013, 22, 2333–2344. [Google Scholar] [CrossRef]
- Gumuskaya, B.; Gurel, B.; Fedor, H.L.; Tan, H.-L.; Weier, C.A.; Hicks, J.L.; Haffner, M.C.; Lotan, T.; De Marzo, A.M. Assessing the order of critical alterations in prostate cancer development and progression by IHC: Further evidence that PTEN loss occurs subsequent to ERG gene fusion. Prostate Cancer Prostatic Dis. 2013, 16, 209–215. [Google Scholar] [CrossRef]
- Carver, B.S.; Tran, J.; Gopalan, A.; Chen, Z.; Shaikh, S.; Carracedo, A.; Alimonti, A.; Nardella, C.; Varmeh, S.; Scardino, P.T.; et al. Aberrant ERG expression cooperates with loss of PTEN to promote cancer progression in the prostate. Nat. Genet. 2009, 41, 619–624. [Google Scholar] [CrossRef]
- Hoogland, A.M.; Jenster, G.; van Weerden, W.M.; Trapman, J.; van der Kwast, T.; Roobol, M.J.; Schröder, F.H.; Wildhagen, M.F.; van Leenders, G.J. ERG immunohistochemistry is not predictive for PSA recurrence, local recurrence or overall survival after radical prostatectomy for prostate cancer. Mod. Pathol. 2012, 25, 471–479. [Google Scholar] [CrossRef]
- Xu, B.; Chevarie-Davis, M.; Chevalier, S.; Scarlata, E.; Zeizafoun, N.; Dragomir, A.; Tanguay, S.; Kassouf, W.; Aprikian, A.; Brimo, F. The prognostic role of ERG immunopositivity in prostatic acinar adenocarcinoma: A study including 454 cases and review of the literature. Hum. Pathol. 2014, 45, 488–497. [Google Scholar] [CrossRef] [PubMed]
- Cuzick, J.; on behalf of the Transatlantic Prostate Group; Yang, Z.H.; Fisher, G.; Tikishvili, E.; Stone, S.; Lanchbury, J.S.; Camacho, N.; Merson, S.; Brewer, D.; et al. Prognostic value of PTEN loss in men with conservatively managed localised prostate cancer. Br. J. Cancer 2013, 108, 2582–2589. [Google Scholar] [CrossRef] [PubMed]
- Barnett, C.M.; Heinrich, M.C.; Lim, J.; Nelson, D.; Beadling, C.; Warrick, A.; Neff, T.; Higano, C.S.; Garzotto, M.; Qian, D.; et al. Genetic Profiling to Determine Risk of Relapse-Free Survival in High-Risk Localized Prostate Cancer. Clin. Cancer Res. 2014, 20, 1306–1312. [Google Scholar] [CrossRef] [PubMed]
- Reid, A.H.M.; on behalf of the Transatlantic Prostate Group; Attard, G.; Ambroisine, L.; Fisher, G.; Kovacs, G.; Brewer, D.; Clark, J.; Flohr, P.; Edwards, S.; et al. Molecular characterisation of ERG, ETV1 and PTEN gene loci identifies patients at low and high risk of death from prostate cancer. Br. J. Cancer 2010, 102, 678–684. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Chi, P.; Rockowitz, S.; Iaquinta, P.J.; Shamu, T.; Shukla, S.; Gao, D.; Sirota, I.; Carver, B.S.; Wongvipat, J.; et al. ETS factors reprogram the androgen receptor cistrome and prime prostate tumorigenesis in response to PTEN loss. Nat. Med. 2013, 19, 1023–1029. [Google Scholar] [CrossRef]
- Grupp, K.; Kohl, S.; Sirma, H.; Simon, R.; Steurer, S.; Becker, A.; Adam, M.; Izbicki, J.; Sauter, G.; Minner, S.; et al. Cysteine-rich secretory protein 3 overexpression is linked to a subset of PTEN-deleted ERG fusion-positive prostate cancers with early biochemical recurrence. Mod. Pathol. 2013, 26, 733–742. [Google Scholar] [CrossRef]
- Sowalsky, A.G.; Ye, H.; Bubley, G.J.; Balk, S.P. Clonal Progression of Prostate Cancers from Gleason Grade 3 to Grade 4. Cancer Res. 2013, 73, 1050–1055. [Google Scholar] [CrossRef]
- Han, B.; Mehra, R.; Lonigro, R.J.; Wang, L.; Suleman, K.; Menon, A.; Palanisamy, N.; A Tomlins, S.; Chinnaiyan, A.M.; Shah, R.B. Fluorescence in situ hybridization study shows association of PTEN deletion with ERG rearrangement during prostate cancer progression. Mod. Pathol. 2009, 22, 1083–1093. [Google Scholar] [CrossRef]
- Morais, C.; Gurgel, D.; Teixeira, A.; Mattos, T.A.; Da Silva, A.A.; Tavora, F. Prevalence of ERG expression and PTEN loss in a Brazilian prostate cancer cohort. Braz. J. Med. Biol. Res. 2019, 52, e8483. [Google Scholar] [CrossRef]
- Yoshimoto, M.; Ding, K.; Sweet, J.M.; Ludkovski, O.; Trottier, G.; Song, K.S.; Joshua, A.M.; E Fleshner, N.; A Squire, J.; Evans, A.J. PTEN losses exhibit heterogeneity in multifocal prostatic adenocarcinoma and are associated with higher Gleason grade. Mod. Pathol. 2013, 26, 435–447. [Google Scholar] [CrossRef]
- Bismar, T.A.; Yoshimoto, M.; Vollmer, R.T.; Duan, Q.; Firszt, M.; Corcos, J.; Squire, J.A. PTEN genomic deletion is an early event associated with ERG gene rearrangements in prostate cancer. BJU Int. 2010, 107, 477–485. [Google Scholar] [CrossRef] [PubMed]
- Bhalla, R.; Kunju, L.P.; A Tomlins, S.; Christopherson, K.; Cortez, C.; Carskadon, S.; Siddiqui, J.; Park, K.; Mosquera, J.M.; A Pestano, G.; et al. Novel dual-color immunohistochemical methods for detecting ERG–PTEN and ERG–SPINK1 status in prostate carcinoma. Mod. Pathol. 2013, 26, 835–848. [Google Scholar] [CrossRef] [PubMed]
- Albero-González, R.; Hernández-Llodrà, S.; Juanpere, N. Immunohistochemical expression of mismatch repair proteins (MSH2, MSH6, MLH1, and PMS2) in prostate cancer: Correlation with grade groups (WHO 2016) and ERG and PTEN status. Virchows Arch. 2019, 475, 223–231. [Google Scholar] [CrossRef] [PubMed]
- Fragkoulis, C.; Glykas, I.; Tzelves, L. Clinical impact of ERG and PTEN status in prostate cancer patients underwent radical prostatectomy. Arch. Ital. Urol. Androl. 2022, 94, 390–395. [Google Scholar] [CrossRef]
- Haney, N.M.; Faisal, F.A.; Lu, J.; Guedes, L.B.; Reuter, V.E.; Scher, H.I.; Eastham, J.A.; Marchionni, L.; Joshu, C.; Gopalan, A.; et al. PTEN Loss with ERG Negative Status is Associated with Lethal Disease after Radical Prostatectomy. J. Urol. 2020, 203, 344–350. [Google Scholar] [CrossRef]
- Haffner, M.C.; Zwart, W.; Roudier, M.P.; True, L.D.; Nelson, W.G.; Epstein, J.I.; De Marzo, A.M.; Nelson, P.S.; Yegnasubramanian, S. Genomic and phenotypic heterogeneity in prostate cancer. Nat. Rev. Urol. 2020, 18, 79–92. [Google Scholar] [CrossRef]
- Schneider, T.M.; Osunkoya, A. ERG expression in intraductal carcinoma of the prostate: Comparison with adjacent invasive prostatic adenocarcinoma. Mod. Pathol. 2014, 27, 1174–1178. [Google Scholar] [CrossRef]
- Sengupta, P.; Hospital, C.C.C.; Taur, N.; Ranjan, R.; Vardhan, R. Study of Serum PSA, AMACR, P63 And PTEN in Prostatic Adenocarcinoma. Ann. Pathol. Lab. Med. 2019, 6, A506–A514. [Google Scholar] [CrossRef]
- Fu, P.; Bu, C.; Cui, B.; Li, N.; Wu, J. Screening of differentially expressed genes and identification of AMACR as a prognostic marker in prostate cancer. Andrologia 2021, 53, e14067. [Google Scholar] [CrossRef] [PubMed]
- Prostate Cancer: Statistics|Cancer.Net. Available online: https://www.cancer.net/cancer-types/prostate-cancer/statistics (accessed on 27 February 2023).










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of Cases | % | ||
|---|---|---|---|
| Grade | 3 | 61 | 45.5% |
| 4, 5 | 73 | 54.5% | |
| Total | 134 | 100.0% | |
| Prostate Carcinoma | Number of Cases | % | |
|---|---|---|---|
| P63 | Negative | 134 | 100% |
| AMACR | Negative | 6 | 4.5% |
| Positive | 128 | 95.5% | |
| PTEN (Pca) | Score 0 | 68 | 50.7% |
| Score 1 | 56 | 41.8% | |
| Score 2 | 10 | 7.5% | |
| ERG (Pca) | Negative | 78 | 58.2% |
| Positive | 56 | 41.8% | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Voulgari, O.; Goutas, D.; Pergaris, A.; Belogiannis, K.; Thymara, E.; Kavantzas, N.; Lazaris, A.C. Correlations of PTEN and ERG Immunoexpression in Prostate Carcinoma and Lesions Related to Its Natural History: Clinical Perspectives. Curr. Issues Mol. Biol. 2023, 45, 2767-2780. https://doi.org/10.3390/cimb45040181
Voulgari O, Goutas D, Pergaris A, Belogiannis K, Thymara E, Kavantzas N, Lazaris AC. Correlations of PTEN and ERG Immunoexpression in Prostate Carcinoma and Lesions Related to Its Natural History: Clinical Perspectives. Current Issues in Molecular Biology. 2023; 45(4):2767-2780. https://doi.org/10.3390/cimb45040181
Chicago/Turabian StyleVoulgari, Olga, Dimitrios Goutas, Alexandros Pergaris, Konstantinos Belogiannis, Eirini Thymara, Nikolaos Kavantzas, and Andreas C. Lazaris. 2023. "Correlations of PTEN and ERG Immunoexpression in Prostate Carcinoma and Lesions Related to Its Natural History: Clinical Perspectives" Current Issues in Molecular Biology 45, no. 4: 2767-2780. https://doi.org/10.3390/cimb45040181
APA StyleVoulgari, O., Goutas, D., Pergaris, A., Belogiannis, K., Thymara, E., Kavantzas, N., & Lazaris, A. C. (2023). Correlations of PTEN and ERG Immunoexpression in Prostate Carcinoma and Lesions Related to Its Natural History: Clinical Perspectives. Current Issues in Molecular Biology, 45(4), 2767-2780. https://doi.org/10.3390/cimb45040181