
Potential Diagnostic Biomarker Detection for Prostate Cancer Using Untargeted and Targeted Metabolomic Profiling

 ,
,  , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Subjects and Clinical Data
2.2. Sample Preparation
2.3. UHPLC-QTOF-ESI+-MS Analysis
2.4. Data Processing and Statistical Analysis
- -
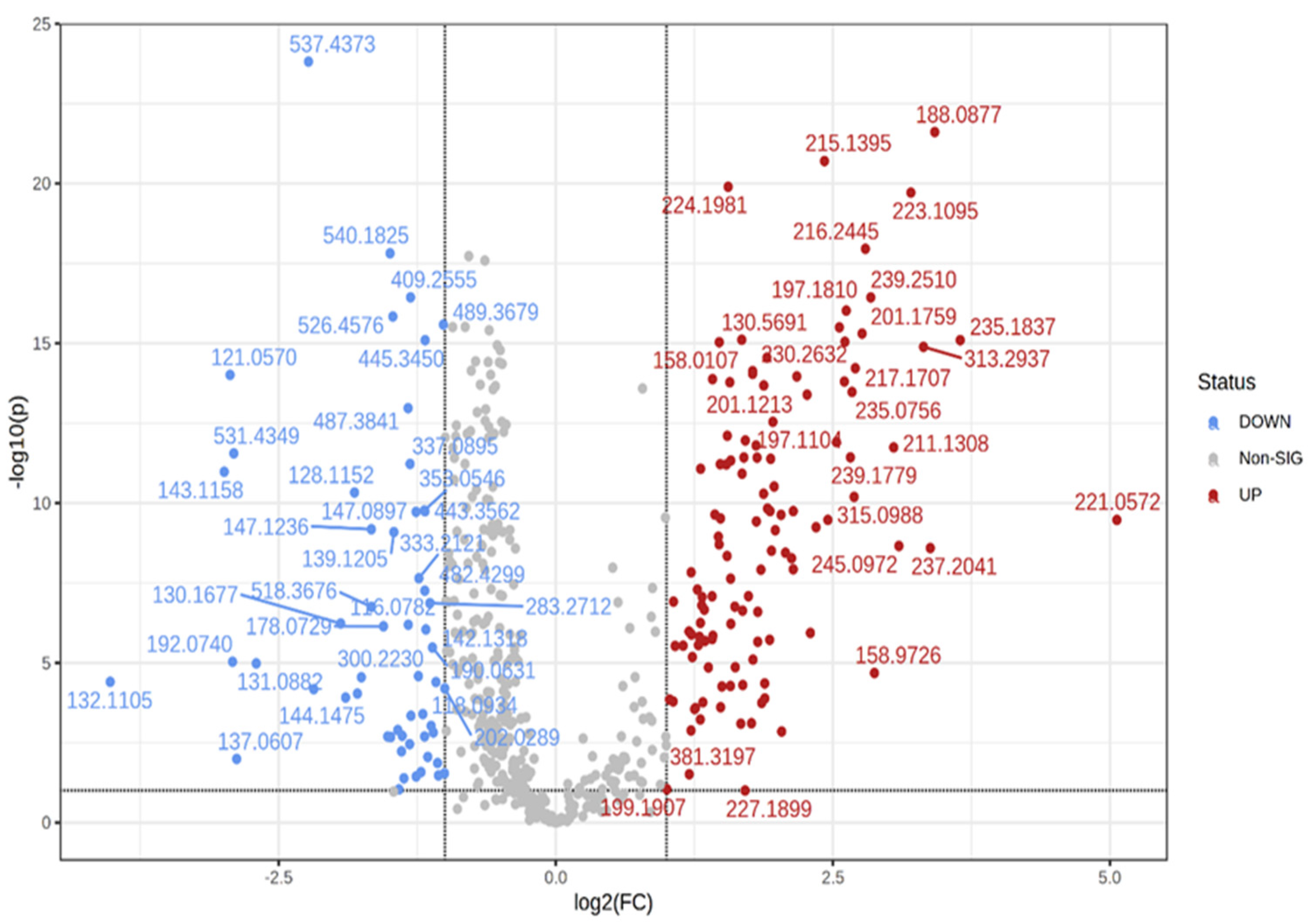
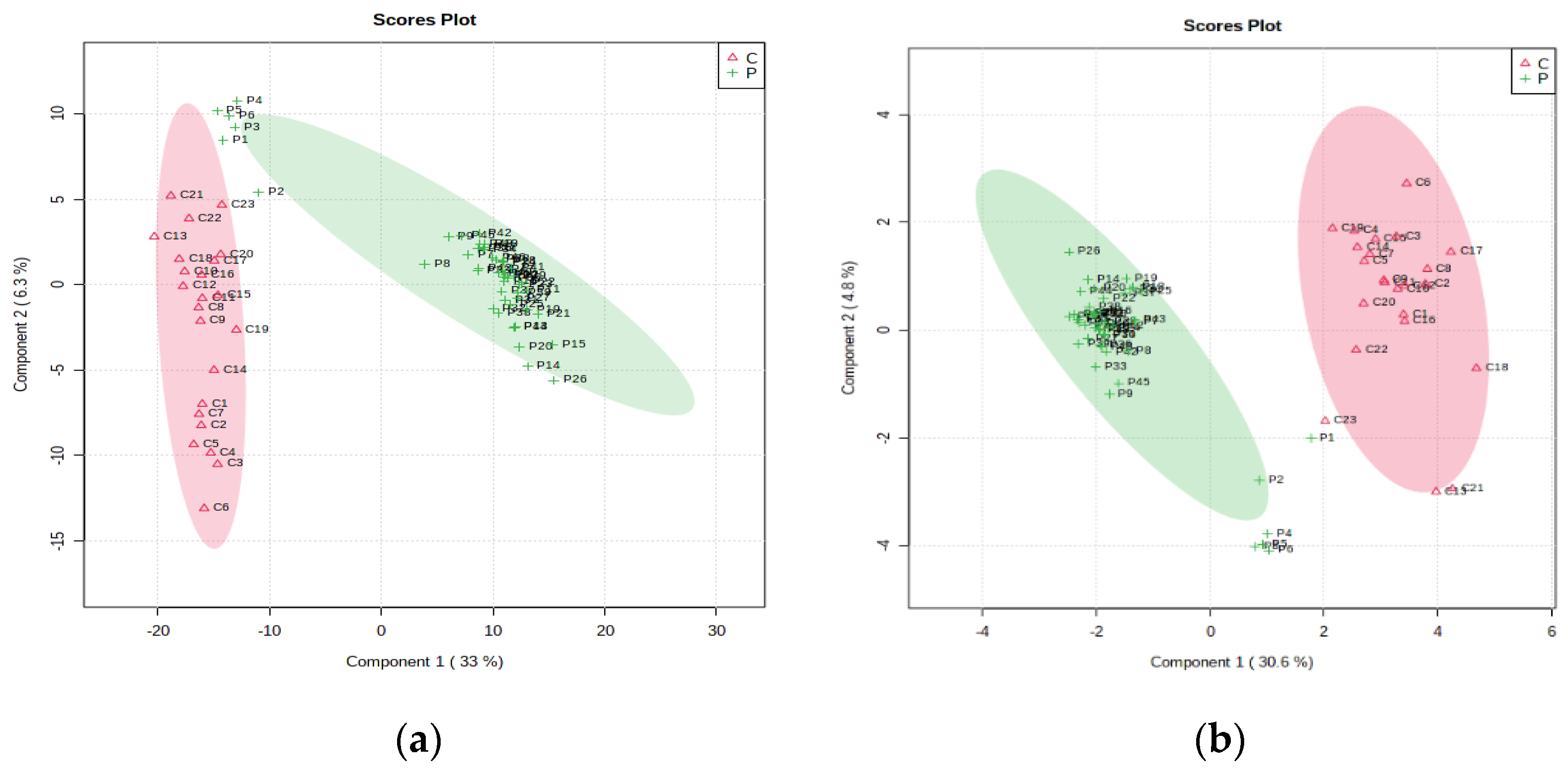
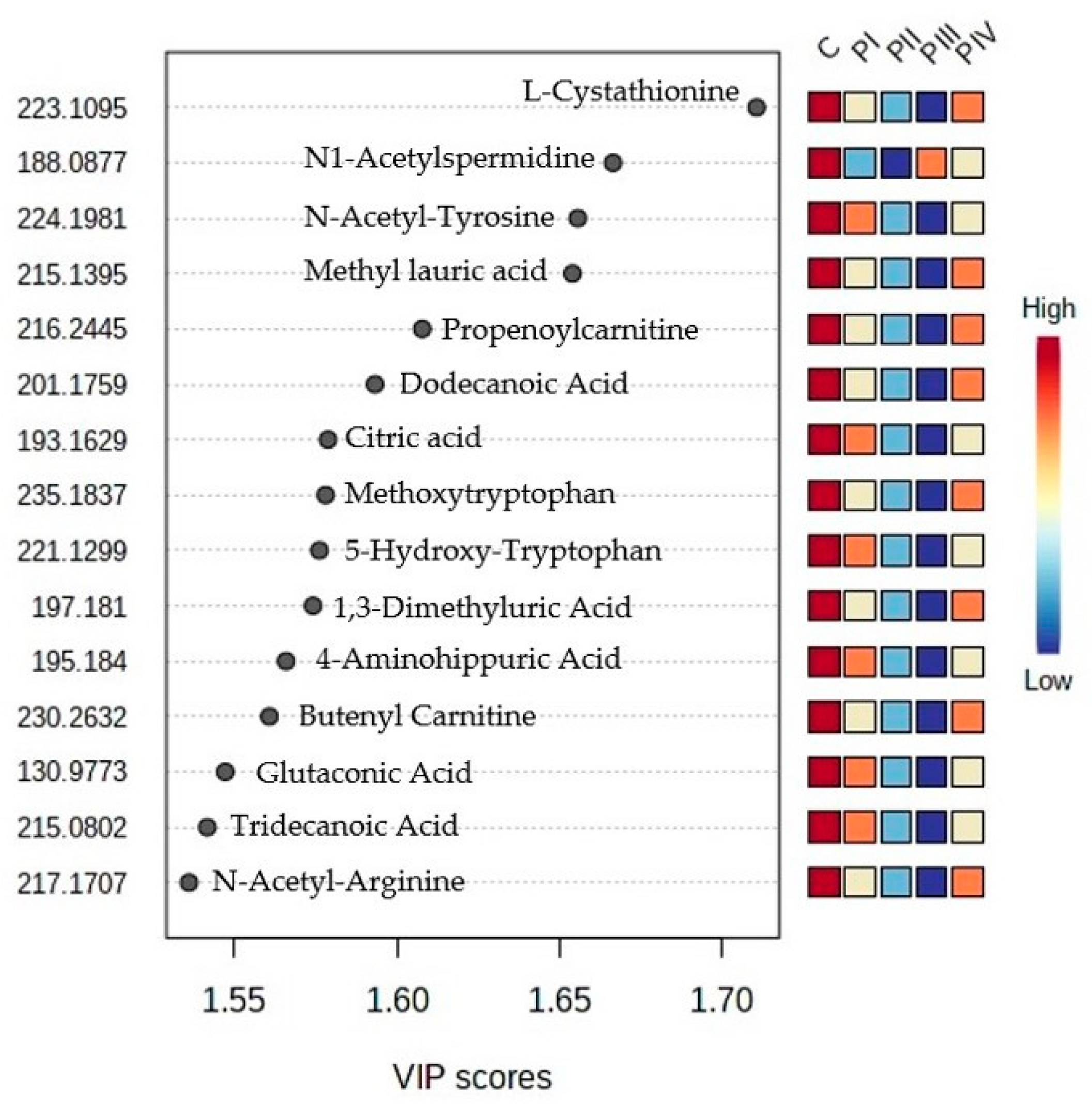
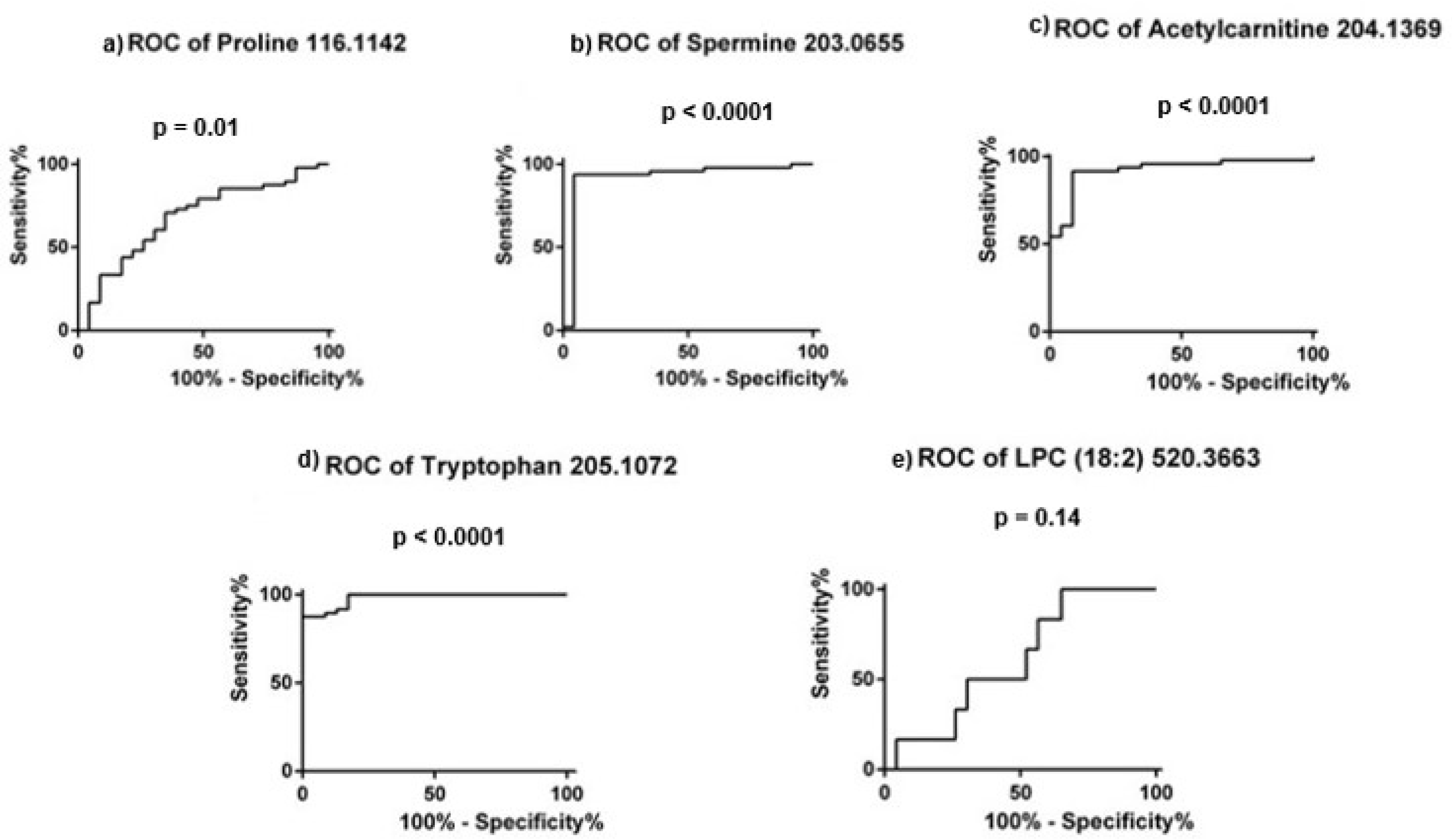
- Multivariate analysis comparing the control group with the whole patients’ group, based on the final matrix.csv for each type of sample. Discriminations between these two groups were represented by the fold change, volcano test, PatternHunter analysis, partial least squares discriminant analysis (PLS-DA), sparse PLSDA (sPLS-DA) and variable importance in the projection (VIP) values including cross-validation parameters. Then, the random forest-based prediction test was applied, and the calculations of p-values were performed by t-tests. The heat maps of correlations were also built. Finally, using the biomarker analysis, the receiver operating curves (ROCs) and the values of the areas under the ROC curves (AUCs) were obtained, and the m/z values were ranked according to their sensitivity/specificity.
- -
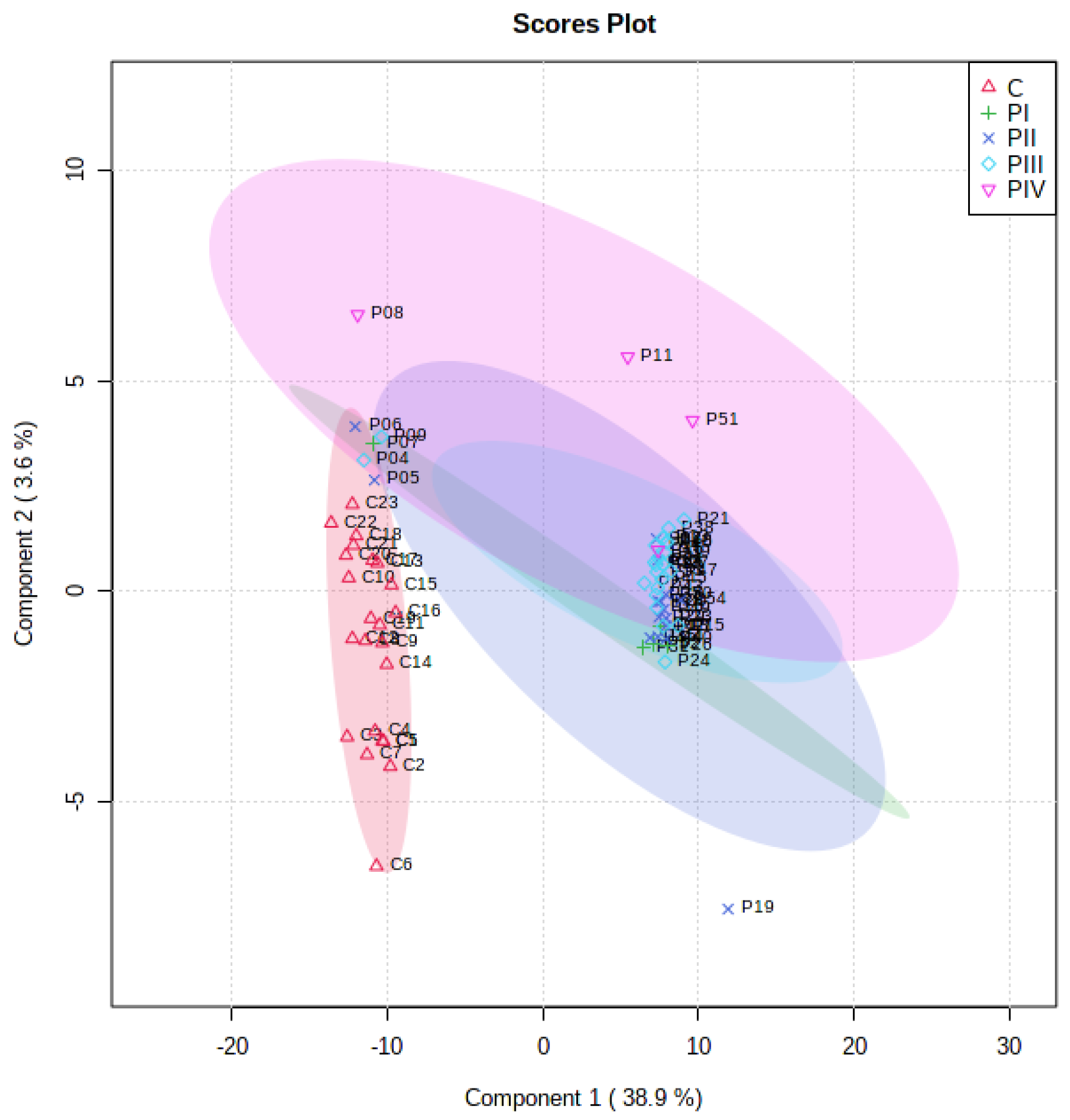
- Univariate analysis, which allowed us to compare the subgroups P1-P4 with the control group. The statistical analysis was conducted for each type of sample using one-way ANOVA, PLS-DA and sPLS-DA score analysis, PatternHunter, random forest and heat maps.
2.5. Quantitative Evaluation
2.5.1. Preparation of Calibration Solution and Quality Control (QC) Samples
2.5.2. Method Validation
2.5.3. Limit of Detection (LOD) and Limit of Quantification (LOQ)
2.6. Chemical Reagents
- -
- L-proline (from Amino Acid Standard H product #20088, Thermo Scientific, Waltham, MA, USA). MW = 115.
- -
- spermine (>97% product S3256, Sigma-Aldrich Chemie GmbH, St. Louis, MO, USA). MW = 202.
- -
- o-acetyl-L-carnitine hydrochloride (J6153606; Alfa Aesar by Thermo Scientific, Waltham, MA, USA). MW = 203.
- -
- L-tryptophan (>98.5% (T) (HPLC) (T0541;TCI Chemicals, Portland, OR, USA). MW = 204.
- -
- lyso L-α-Lysophosphatidylcholine-LPC(18:2) from bovine brain (CAS nr. 9008-30-4) Sigma-Aldrich Chemie GmbH, St. Louis, MO, USA. MW = 519.
3. Results
3.1. Subjects’ Clinicopathological Data
3.2. Untargeted Metabolomic Profiling
3.2.1. Metabolite Identification
3.2.2. Multivariate Untargeted Metabolomics Statistical Analysis of the 71 Plasma Samples
3.3. Targeted Metabolomic Profiling
3.3.1. Calibrations and Validation Parameters
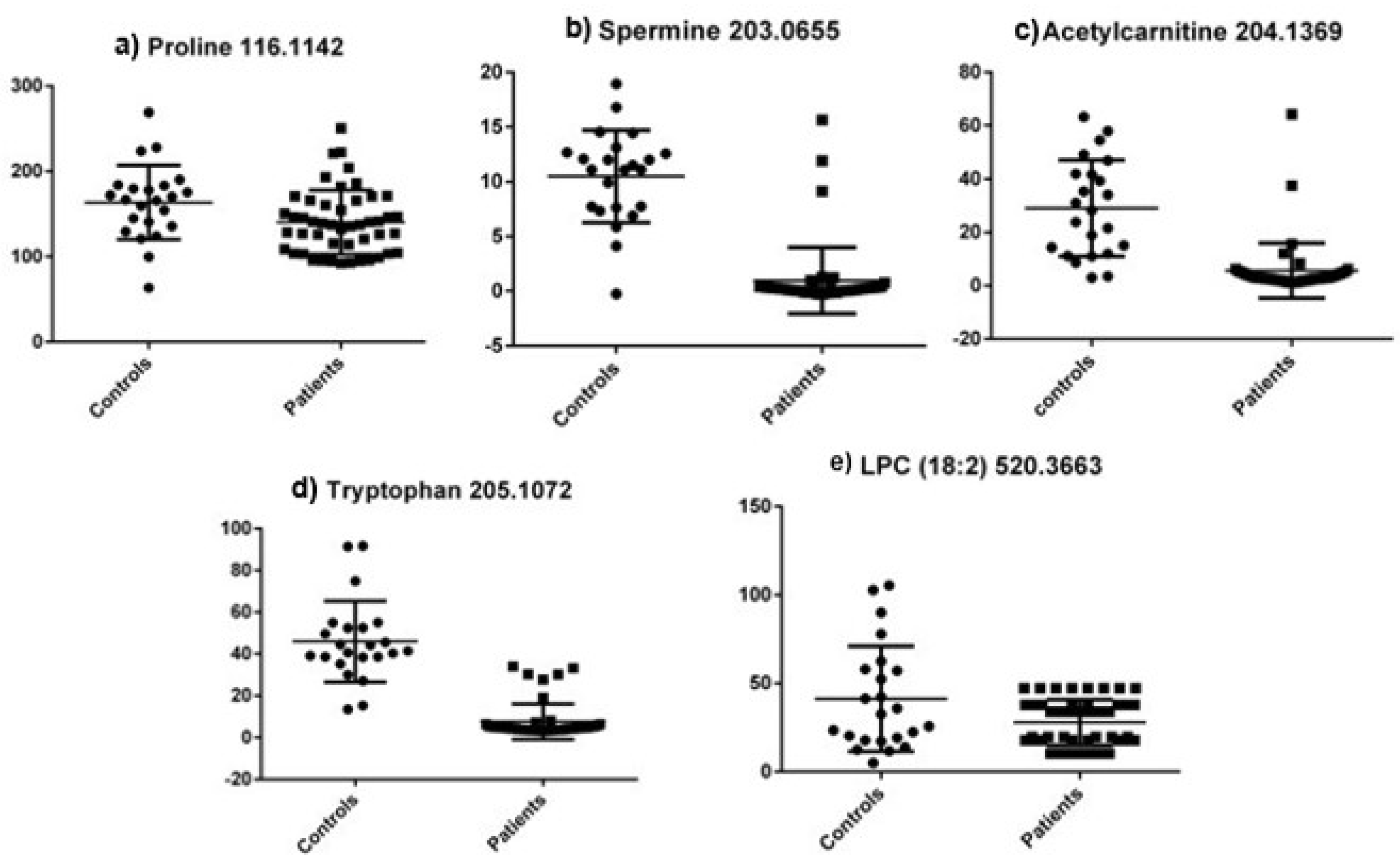
3.3.2. Quantitative Determination
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sekhoacha, M.; Riet, K.; Motloung, P.; Gumenku, L.; Adegoke, A.; Mashele, S. Prostate Cancer Review: Genetics, Diagnosis, Treatment Options, and Alternative Approaches. Molecules 2022, 27, 5730. [Google Scholar] [CrossRef] [PubMed]
- Cancer Stat Facts: Prostate Cancer. Available online: https://seer.cancer.gov/statfacts/html/prost.html (accessed on 5 January 2023).
- American Cancer Sociecty (ACS). Prostate Cancer Risk Factors. Available online: https://www.cancer.org/cancer/prostate-cancer/causes-risks-prevention/risk-factors.html (accessed on 5 January 2023).
- Rodriguez, J.F.; Eggener, S.E. Prostate Cancer and the Evolving Role of Biomarkers in Screening and Diagnosis. Radiol. Clin. N. Am. 2018, 56, 187–196. [Google Scholar] [CrossRef] [PubMed]
- Ortner, G.; Tzanaki, E.; Rai, B.P.; Nagele, U.; Tokas, T. Transperineal prostate biopsy: The modern gold standard to prostate cancer diagnosis. Turk. J. Urol. 2021, 47 (Suppl. S1), S19–S26. [Google Scholar] [CrossRef] [PubMed]
- Bach, C.; Pisipati, S.; Daneshwar, D.; Wright, M.; Rowe, E.; Gillatt, D.; Persad, R.; Koupparis, A. The status of surgery in the management of high-risk prostate cancer. Nat. Rev. Urol. 2014, 11, 342–351. [Google Scholar] [CrossRef]
- Velonas, V.M.; Woo, H.H.; dos Remedios, C.G.; Assinder, S.J. Current status of biomarkers for prostate cancer. Int. J. Mol. Sci. 2013, 14, 11034–11060. [Google Scholar] [CrossRef] [Green Version]
- Spratlin, J.L.; Serkova, N.J.; Eckhardt, S.G. Clinical applications of metabolomics in oncology: A review. Clin. Cancer Res. 2009, 15, 431–440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sreekumar, A.; Poisson, L.M.; Rajendiran, T.M.; Khan, A.P.; Cao, Q.; Yu, J.; Laxman, B.; Mehra, R.; Lonigro, R.J.; Li, Y.; et al. Metabolomic profiles delineate potential role for sarcosine in prostate cancer progression. Nature 2009, 457, 910–914. [Google Scholar] [CrossRef] [Green Version]
- Trock, B.J. Application of metabolomics to prostate cancer. Urol Oncol. 2011, 29, 572–581. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.; Kislinger, T. Novel approaches for the identification of biomarkers of aggressive prostate cancer. Genome Med. 2013, 5, 56. [Google Scholar] [CrossRef] [Green Version]
- Rigau, M.; Olivan, M.; Garcia, M.; Sequeiros, T.; Montes, M.; Colás, E.; Llauradó, M.; Planas, J.; de Torres, I.; Morote, J.; et al. The Present and Future of Prostate Cancer Urine Biomarkers. Int. J. Mol. Sci. 2013, 14, 12620–12649. [Google Scholar] [CrossRef] [Green Version]
- Idle, J.R.; Gonzalez, F.J. Metabolomics. Cell Metab. 2007, 6, 348–351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, A.; Sun, H.; Yan, G.; Wang, P.; Wang, X. Mass spectrometry-based metabolomics: Applications to biomarker and metabolic pathway research. Biomed. Chromatogr. 2016, 30, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Watson, D.G.; Wang, L.; Abbas, M.; Murdoch, L.; Bashford, L.; Ahmad, I.; Lam, N.-Y.; Ng, N.C.F.; Leung, H.Y. Application of Holistic Liquid Chromatography-High Resolution Mass Spectrometry Based Urinary Metabolomics for Prostate Cancer Detection and Biomarker Discovery. PLoS ONE 2013, 8, e65880. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alonso, A.; Marsal, S.; Julià, A. Analytical methods in untargeted metabolomics: State of the art in 2015. Front. Bioeng. Biotechnol. 2015, 3, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmad, F.; Cherukuri, M.K.; Choyke, P.L. Metabolic reprogramming in prostate cancer. Br. J. Cancer 2021, 125, 1185–1196. [Google Scholar] [CrossRef]
- Thapar, R.; Titus, M.A. Recent Advances in Metabolic Profiling And Imaging of Prostate Cancer. Curr. Metab. 2014, 2, 53–69. [Google Scholar] [CrossRef] [Green Version]
- Lima, A.R.; Pinto, J.; Amaro, F.; Bastos, M.L.; Carvalho, M.; Guedes de Pinho, P. Advances and Perspectives in Prostate Cancer Biomarker Discovery in the Last 5 Years through Tissue and Urine Metabolomics. Metabolites 2021, 11, 181. [Google Scholar] [CrossRef]
- Kdadra, M.; Höckner, S.; Leung, H.; Kremer, W.; Schiffer, E. Metabolomics Biomarkers of Prostate Cancer: A Systematic Review. Diagnostics 2019, 9, 21. [Google Scholar] [CrossRef] [Green Version]
- Sartori, D.A.; Chan, D.W. Biomarkers in prostate cancer: What’s new? Curr. Opin. Oncol. 2014, 26, 259–264. [Google Scholar] [CrossRef] [Green Version]
- Bentrad, V.V.; Gogol, S.V.; Zaletok, S.P.; Vitruk, Y.V.; Stakhovskyi, E.O.; Grechko, B.O. Urinary spermine level as novel additional diagnostic marker of prostate cancer. Ann. Oncol. 2019, 30, 123. [Google Scholar] [CrossRef]
- Giskeødegård, G.F.; Bertilsson, H.; Selnæs, K.M.; Wright, A.J.; Bathen, T.F.; Viset, T.; Halgunset, J.; Angelsen, A.; Gribbestad, I.S.; Tessem, M.-B. Spermine and Citrate as Metabolic Biomarkers for Assessing Prostate Cancer Aggressiveness. PLoS ONE 2013, 8, e62375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baci, D.; Bruno, A.; Cascini, C.; Gallazzi, M.; Mortara, L.; Sessa, F.; Pelosi, G.; Albini, A.; Noonan, D.M. Acetyl-L-Carnitine downregulates invasion (CXCR4/CXCL12, MMP-9) and angiogenesis (VEGF, CXCL8) pathways in prostate cancer cells: Rationale for prevention and interception strategies. J. Exp. Clin. Cancer Res. 2019, 38, 464. [Google Scholar] [CrossRef] [PubMed]
- Akbari, Z.; Dijojin, R.T.; Zamani, Z.; Hosseini, R.H.; Arjmand, M. Aromatic amino acids play a harmonizing role in prostate cancer: A metabolomics-based cross-sectional study. Int. J. Reprod. Biomed. 2021, 19, 741–750. [Google Scholar] [CrossRef] [PubMed]
- Hong, X.; Mao, L.; Xu, L.; Hu, Q.; Jia, R. Prostate-specific membrane antigen modulates the progression of prostate cancer by regulating the synthesis of arginine and proline and the expression of androgen receptors and Fos proto-oncogenes. Bioengineered 2022, 13, 995–1012. [Google Scholar] [CrossRef]
- Li, X.; Nakayama, K.; Goto, T.; Kimura, H.; Akamatsu, S.; Hayashi, Y.; Fujita, K.; Kobayashi, T.; Shimizu, K.; Nonomura, N.; et al. High level of phosphatidylcholines/lysophosphatidylcholine ratio in urine is associated with prostate cancer. Cancer Sci. 2021, 112, 4292–4302. [Google Scholar] [CrossRef]
- Zhou, X.; Lawrence, T.J.; He, Z.; Pound, C.R.; Mao, J.; Bigler, S.A. The expression level of lysophosphatidylcholine acyltransferase 1 (LPCAT1) correlates to the progression of prostate cancer. Exp. Mol. Pathol. 2012, 92, 105–110. [Google Scholar] [CrossRef] [Green Version]
- Buszewska-Forajta, M.; Pomastowski, P.; Monedeiro, F.; Walczak-Skierska, J.; Markuszewski, M.; Matuszewski, M.; Markuszewski, M.J.; Buszewski, B. Lipidomics as a Diagnostic Tool for Prostate Cancer. Cancers 2021, 13, 2000. [Google Scholar] [CrossRef]
- Geng, P.; Qin, W.; Xu, G. Proline metabolism in cancer. Amino Acids 2021, 53, 1769–1777. [Google Scholar] [CrossRef]
- Phang, J.M.; Liu, W.; Hancock, C.N.; Fischer, J.W. Proline metabolism and cancer: Emerging links to glutamine and collagen. Curr. Opin. Clin. Nutr. Metab. Care 2015, 18, 71–77. [Google Scholar] [CrossRef] [Green Version]
- Platten, M.; Nollen, E.A.A.; Röhrig, U.F.; Fallarino, F.; Opitz, C.A. Tryptophan metabolism as a common therapeutic target in cancer, neurodegeneration and beyond. Nat. Rev. Drug. Discov. 2019, 18, 379–401. [Google Scholar] [CrossRef]
- Dambrova, M.; Makrecka-Kuka, M.; Kuka, J.; Vilskersts, R.; Nordberg, D.; Attwood, M.M.; Smesny, S.; Sen, Z.D.; Guo, A.C.; Oler, E.; et al. Acylcarnitines: Nomenclature, Biomarkers, Therapeutic Potential, Drug Targets, and Clinical Trials. Pharmacol. Rev. 2022, 74, 506–551. [Google Scholar] [CrossRef] [PubMed]
- Law, S.H.; Chan, M.L.; Marathe, G.K.; Parveen, F.; Chen, C.H.; Ke, L.Y. An Updated Review of Lysophosphatidylcholine Metabolism in Human Diseases. Int. J. Mol. Sci. 2019, 6, 1149. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | N = 48 (Patients) | % | N = 23 (Controls) | % |
|---|---|---|---|---|
| Age (mean ± SD) | 63 (±5.49) | 54 (±1.29) | ||
| Prostate-specific antigen—PSA (ng/mL) | ||||
| <4 | 0 | 0.00 | 23 | 100.00 |
| 4–10 | 28 | 58.33 | 0 | 0.00 |
| >10 | 20 | 41.66 | 0 | 0.00 |
| Prostatic volume (mL) mean ± SD | 44 (±19.83) | |||
| PSA density (ng/mL2) mean ± SD | 0.28 (±0.15) | |||
| Gleason score | ||||
| 6 | 14 | 29.17 | ||
| 7–8 | 32 | 66.67 | ||
| 9 | 2 | 4.16 | ||
| AJCC stage | ||||
| I | 5 | 4.16 | ||
| II-III | 39 | 87.5 | ||
| IV | 4 | 8.33 | ||
| m/z | AUC | p-Value | Identification |
|---|---|---|---|
| 188.0877 | 0.9973 | 2.43 × 10−22 | N1-Acetylspermidine |
| 537.4373 | 0.9955 | 1.52 × 10−24 | Stearyl Stearate & Isomers |
| 335.298 | 0.9873 | 3.07 × 10−16 | Docosatrienoic Acid C22:3 |
| 326.301 | 0.9846 | 1.86 × 10−18 | N-Myristoyl Proline |
| 215.1395 | 0.9828 | 1.973 × 10−21 | Methyl lauric acid |
| 540.1825 | 0.9828 | 1.525 × 10−18 | Hexacosanoyl Carnitine |
| 223.1095 | 0.9792 | 1.92 × 10−20 | L-Cystathionine |
| 489.3679 | 0.9792 | 2.59 × 10−16 | Cytidine 5’-Diphosphocholine |
| 331.0208 | 0.9774 | 2.56 × 10−18 | Deoxycorticosterone |
| 300.223 | 0.9765 | 2.66 × 10−5 | D-Sphingosine |
| 526.4576 | 0.9728 | 1.45 × 10−16 | LPS(18:0) |
| 239.251 | 0.9701 | 3.66 × 10−17 | 5-Oxo-Tetradecadienoic Acid (C14:2) |
| 409.2555 | 0.9701 | 3.64 × 10−17 | Ursocholic/Muricholic Acid Acid |
| 205.1072 | 0.9692 | 3.16 × 10−16 | L-Tryptophan |
| 227.1899 | 0.9692 | 0.099 | Carnosine |
| 419.2139 | 0.9683 | 7.21 × 10−15 | Palmitoyl Glucuronide |
| 181.9605 | 0.9674 | 3.11 × 10−16 | Tyrosine |
| 224.1981 | 0.9674 | 1.26 × 10−20 | N-Acetyl-Tyrosine |
| Molecule (m/z) | Linear Range μM | Curve Equation | R2 | LOD μM | LOQ μM |
|---|---|---|---|---|---|
| L-proline (116.1142) | 10–100 | y = 11290x − 119623 | 0.898 | 4.0 | 5.5 |
| Spermine (203.0655) | 0.5–5 | y = 498406x + 51799 | 0.997 | 0.1 | 0.3 |
| Acetylcarnitine (204.1369) | 1–5 | y = 36813x − 3879.2 | 0.994 | 0.2 | 0.8 |
| L-tryptophan (205.1072) | 4–40 | y = 19944x − 7756 | 0.998 | 0.8 | 1.0 |
| LPC 18:2 (520.3663) | 1–10 | y = 172161x + 91874 | 0.965 | 0.3 | 0.9 |
| Metabolite | Initial Concentration (mM) | Measured Concentration (mM) | Recovery (%) |
|---|---|---|---|
| L-proline | 20 | 17.5 | 87.5 |
| Spermine | 2 | 1.82 | 91.0 |
| Acetylcarnitine | 2 | 1.88 | 94.0 |
| L-tryptophan | 8 | 7.55 | 94.3 |
| LPC(18:2) | 2 | 1.85 | 92.5 |
| IS (DOXO) | 1.4 | 1.25 | 89.3 |
| Metabolite | m/z | AUC Value | 95% CI | p Value |
|---|---|---|---|---|
| L-proline | 116.1142 | 0.682 | 0.548–0.816 | 0.01 |
| Spermine | 203.0655 | 0.922 | 0.832–1.01 | <0.0001 |
| Acetylcarnitine | 204.1369 | 0.923 | 0.855–0.991 | <0.0001 |
| L-tryptophan | 205.1072 | 0.981 | 0.957–1.005 | <0.0001 |
| LPC (18:2) | 520.3663 | 0.608 | 0.453–0.764 | 0.140 |
| Molecule | Controls | Patients (All Stages) | PI | PII | PIII | PIV | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean (μM) | SD (%) | Mean (μM) | SD (%) | Mean (μM) | SD (%) | Mean (μM) | SD (%) | Mean (μM) | SD (%) | Mean (μM) | SD (%) | |
| L-proline | 163.580 | 43.45 | 140.36 | 37.57 | 152.08 | 24.57 | 134.93 | 30.98 | 140.36 | 45.68 | 147.46 | 27.59 |
| Spermine | 10.484 | 4.22 | 0.98 | 3.04 | 3.05 | 7.05 | 0.06 | 0.37 | 1.19 | 2.99 | 0.87 | 0.10 |
| Acetylcarnitine | 29.020 | 18.03 | 5.65 | 10.27 | 4.10 | 4.56 | 3.49 | 1.69 | 6.29 | 12.98 | 12.53 | 16.70 |
| L-tryptophan | 45.908 | 19.39 | 7.63 | 8.45 | 9.67 | 11.58 | 7.60 | 9.45 | 6.16 | 5.67 | 13.68 | 13.65 |
| LPC (18:2) | 41.274 | 29.77 | 27.93 | 12.93 | 28.18 | 12.34 | 28.34 | 13.95 | 27.09 | 12.90 | 30.77 | 14.24 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nitusca, D.; Socaciu, C.; Socaciu, A.I.; Sirbu, I.O.; Bardan, R.; Cumpanas, A.A.; Seclaman, E.; Marian, C. Potential Diagnostic Biomarker Detection for Prostate Cancer Using Untargeted and Targeted Metabolomic Profiling. Curr. Issues Mol. Biol. 2023, 45, 5036-5051. https://doi.org/10.3390/cimb45060320
Nitusca D, Socaciu C, Socaciu AI, Sirbu IO, Bardan R, Cumpanas AA, Seclaman E, Marian C. Potential Diagnostic Biomarker Detection for Prostate Cancer Using Untargeted and Targeted Metabolomic Profiling. Current Issues in Molecular Biology. 2023; 45(6):5036-5051. https://doi.org/10.3390/cimb45060320
Chicago/Turabian StyleNitusca, Diana, Carmen Socaciu, Andreea Iulia Socaciu, Ioan Ovidiu Sirbu, Razvan Bardan, Alin Adrian Cumpanas, Edward Seclaman, and Catalin Marian. 2023. "Potential Diagnostic Biomarker Detection for Prostate Cancer Using Untargeted and Targeted Metabolomic Profiling" Current Issues in Molecular Biology 45, no. 6: 5036-5051. https://doi.org/10.3390/cimb45060320
APA StyleNitusca, D., Socaciu, C., Socaciu, A. I., Sirbu, I. O., Bardan, R., Cumpanas, A. A., Seclaman, E., & Marian, C. (2023). Potential Diagnostic Biomarker Detection for Prostate Cancer Using Untargeted and Targeted Metabolomic Profiling. Current Issues in Molecular Biology, 45(6), 5036-5051. https://doi.org/10.3390/cimb45060320